
Abstract
Background. This study tested in children with cerebral palsy (CP) whether motor habilitation resembles motor learning. Methods. Twelve children with hemiplegic CP ages 5 to 12 years with moderate to severe motor impairments underwent a 16-session robot-mediated planar therapy program to improve upper limb reach, with a focus on shoulder and elbow movements. Participants were trained to execute point-to-point movements (with robot assistance) with the affected arm and were evaluated (without robot assistance) in trained (point-to-point) and untrained (circle-drawing) conditions. Outcomes were measured at baseline, midpoint, immediately after the program, and 1 month postcompletion. Outcome measures were the Fugl-Meyer (FM), Quality of Upper Extremity Skills Test (QUEST), and Modified Ashworth Scale (MAS) scores; parent questionnaire; and robot-based kinematic metrics. To assess whether learning best characterizes motor habilitation in CP, the authors quantified (a) improvement on trained tasks at completion of training (acquisition) and 1 month following completion (retention) and (b) quantified generalization of improvement to untrained tasks. Results. After robotic intervention, the authors found significant gains in the FM, QUEST, and parent questionnaire. Robot-based evaluations demonstrated significant improvement in trained movements and that improvement was sustained at follow-up. Furthermore, children improved their performance in untrained movements indicating generalization. Conclusions. Motor habilitation in CP exhibits some traits of motor learning. Optimal treatment may not require an extensive repertoire of tasks but rather a select set to promote generalization.
Introduction
Motor neuroscience is increasingly incorporated into clinical practice, leading to new therapeutic approaches. Based on evidence supporting further testing of therapeutic robot-assistive training devices to lessen upper extremity impairment and disability after stroke,1-4 investigators are exploring the use of these devices as a technique for habilitation in cerebral palsy (CP). These studies can also improve our understanding of motor skill acquisition models in this population.5-7 Accordingly, several studies have suggested that motor recovery after stroke or motor habilitation in children with CP resembles some form of motor learning, 8 but the extent of this resemblance is not well understood.
From a cursory view point, models representing stroke recovery start out from the inherent premise that subjects had learned and perfected the neural network that drives and controls movement over the course of many repetitions of many variations of purposeful actions. After a stroke, this network is disrupted and rehabilitation efforts aim to reestablish the effectiveness of partially disrupted pathways or strengthen alternate neuromotor connections. On the contrary, neural networks of people with CP are still immature at the time of the lesion. Rather than reestablishing disrupted pathways as in stroke, we have to habilitate children as they mature and to teach them skills within the limits of the spared pathways, perhaps strengthen alternate neuromotor networks to maximize their potential, fully cognizant of the potential of malplasticity.
We have established that several aspects of motor recovery have similar traits as motor learning.8-10 Here we examine whether the same occurs with motor habilitation in CP. This study employs robot-based metrics to investigate whether the kinematics of unassisted movements can improve with training (acquisition of motor skills) and whether this improvement persists at follow-up (retention of motor skills gains). This study also examines whether there is some generalization of gains to untrained tasks. It is generally accepted that motor learning implies some retention of the gained ability independent of how much time elapses between acquisition and retention assessments,11,12 that is, there is no return to the original state, and motor learning allows some generalization to occur (presumably based on some form of newly acquired internal representation). We expect these results to shed some light on the effectiveness of current practices, which support a model that involves training an exhaustive set of tasks, versus a learning model, in which we may employ a sparser set of training tasks if we understand the limitations of generalization.
Methods
Participants
This study enrolled a sample of convenience of 12 children ages 5 to 12 years with hemiplegic CP and 1 child with traumatic brain injury. Inclusion criteria were discussed in a companion article 5 and are repeated here: (a) eligible children were between ages 4 and 12 years, (b) had diagnosis of CP or acquired brain injury at least 6 months prior to enrollment and presented with upper limb hemiplegia, (c) had no more than moderate spasticity in the upper limb, (d) had adequate range of motion to engage in the study, and (e) were able to follow instructions and maintain attention during therapy. Children were excluded if they had received botulinum toxin or phenol injections within 4 months of enrollment or were scheduled to receive injections prior to study completion.
Informed consent and assent were obtained from all guardians and study subjects. The study protocol was approved by the Committee on the Use of Human Experimental Subjects of the Massachusetts Institute of Technology and the Institutional Review Boards at Spaulding Rehabilitation Hospital and Franciscan Hospital for Children.
Intervention
Participants received a therapist-supervised robot-mediated program with InMotion2 (Interactive Motion Technologies, Inc, Watertown, Massachusetts) during 1-hour therapy sessions twice per week for 8 weeks. The frequency and duration of the robotic therapy sessions were similar to that of conventional rehabilitation programs for children with hemiplegia and comparable with prior robot-assisted therapy protocols for adults with stroke. During each session, youngsters were seated on a chair and directed to make 2 blocks of 320 point-to-point movements (total 640 movements), ending as near as possible to the target location with the robot providing assistance-as-needed. 13 A center target and 8 targets equally spaced around a circle were displayed on a monitor, and visual feedback regarding the current position of the robot endpoint (subjects’ hand position) was provided (Figure 1). The center of the workspace was in front of the subject at the body midline with the shoulder elevation at 45° with the elbow slightly flexed. Youngsters moved from the center to each target (10 cm) in random order, stopped, then returned to the center, with the robot delivering performance-based training (active assist-as-needed). 13 Some children were able to perform all or part of a third block of 320 point-to-point movements during their 1-hour sessions. If a child was unable to maintain active grasp of the robot handle during therapy, the least restrictive assist (either a grasping mitt or foam strapping) was provided to safely secure the hand. Children who received community-based therapy continued their usual treatment during the robotic therapy pilot trial.
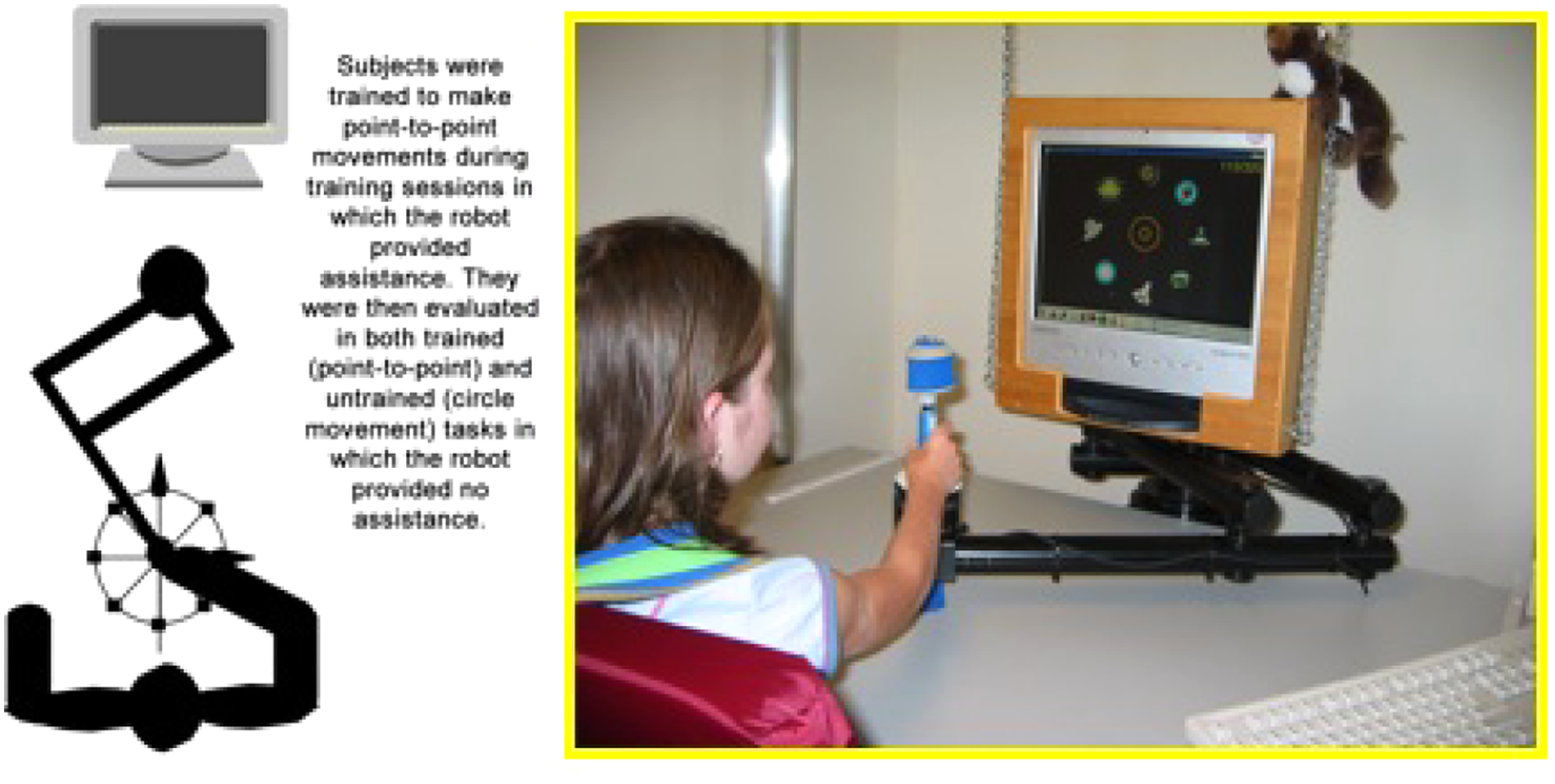
Configuration of trained and untrained motor tasks.
Clinical Assessment
Clinical outcomes were reported elsewhere in a companion article by Fasoli et al 5 and are repeated here. Measures included the impairment scores on the Fugl-Meyer Assessment—Upper Limb subtest (FM, max 66 points), 14 the Quality of Upper Extremity Skills Test (QUEST), 15 Modified Ashworth Scale, 16 and a parent questionnaire that rated the child’s functional use of the paretic arm in the home and community. 5 We evaluated children twice at baseline within a 2-week period, at midpoint (after 8th therapy session), at completion of the treatment protocol (after 16th therapy session), and at follow-up 1 month after treatment completion. We chose a relatively short 1-month follow-up period to be practical in our request that parents refrain from pursuing other forms of treatment (eg, regularly scheduled botulinum toxin injections to manage upper limb spasticity, hippotherapy, aquatic therapy, etc) during the research protocol.
Kinematic Acquisition and Analysis
Robot-based evaluations coincided with clinical testing to collect kinematic data that further quantified changes in motor performance. For these evaluation sessions, the robot was not in the active mode and acted instead as a very low friction passive measurement device that restricted subjects’ arm motion to a horizontal plane but allowed even weak movements of a child to be expressed. During each robot-based evaluation session, youngsters sat on a chair as described above and were asked to make (a) 80 point-to-point movements (40 outbound and 40 inbound to center target) similar to the training protocol and (b) 20 circle-drawing movements.
The circle-drawing task (not trained during the intervention sessions) was performed in the same workspace as the trained movements. Children were asked to draw a circle shown on the computer monitor by moving the end-effector of the robot in a horizontal plane in a terminated motion. Subjects drew 5 circles clockwise and 5 circles counterclockwise starting at 9 o’clock and also 5 circles clockwise and 5 circles counterclockwise starting at 3 o’clock.
Outcome measures extracted from participants’ kinematic data of the center-out, point-to-point movements evaluated changes in reaching performance (Figure 2). These included movement variables of aim, movement deviation from a straight line, mean speed, peak speed, duration, and 1 smoothness metric, 17 known as the speed shape (mean speed divided by peak speed). The beginning and end of movements were defined respectively as the instants when speed first became greater and again smaller (and remained below) than 2% of its peak. Outcome measures extracted from subjects’ movement kinematics during the circle-drawing movements included the axes ratio (ratio of the minor and major axes of the ellipse best-fitting the data 18 ). The axes ratio is a number between 0 and 1, with values closer to 1 indicating more circular shapes. During circle drawing, a child’s ability to draw a circular shape (with value closer to 1) is accompanied by improved interjoint coordination of shoulder and elbow movements. Together, these metrics quantify whether the movements become faster and smoother with recovery and whether the independent control of isolated shoulder and elbow movements improves.
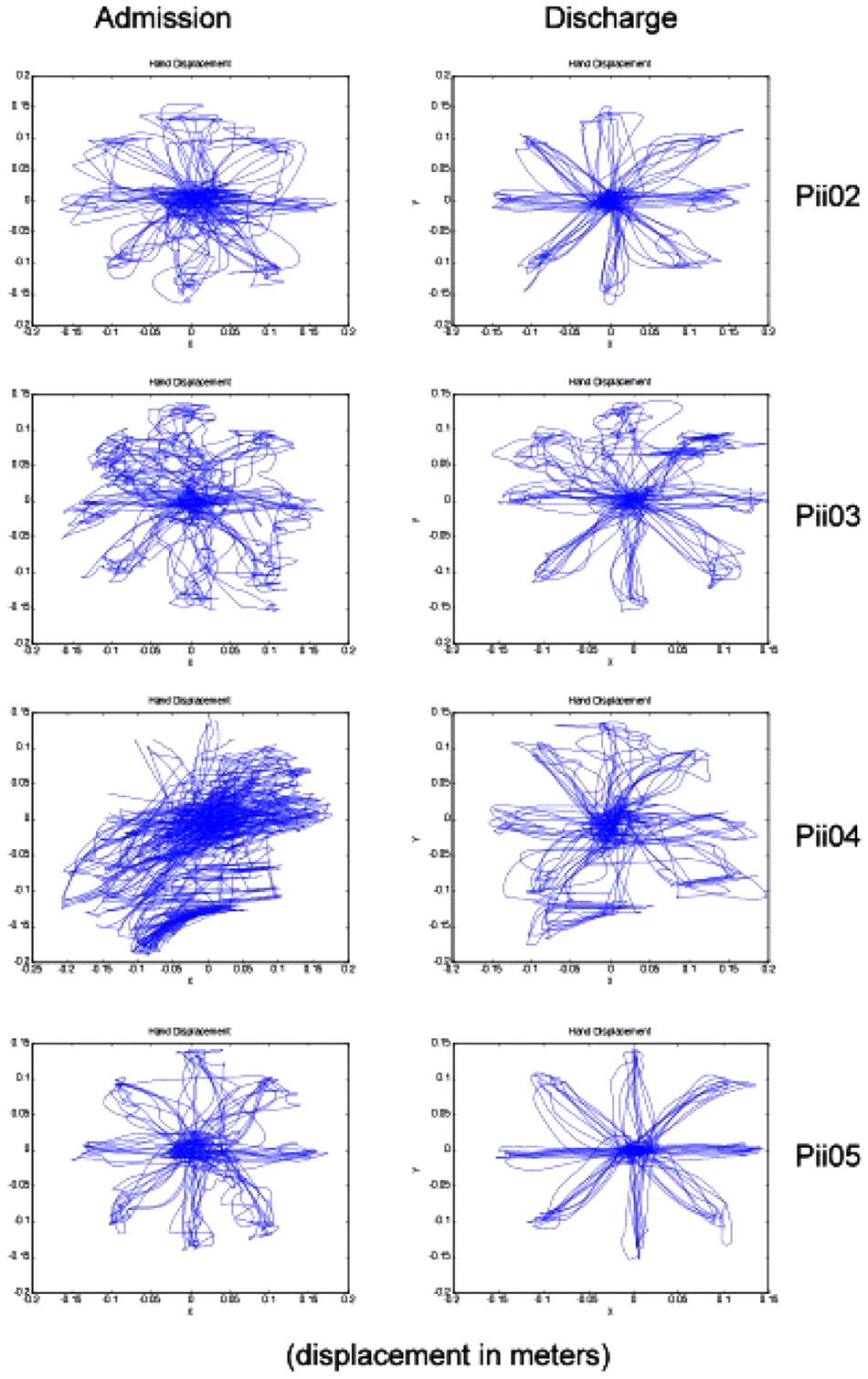
Representative example of children’s performance at baseline and completion of intervention on the trained (point-to-point) reaching task. We selected the attempts of the first 4 children enrolled in the study. Similar unassisted reaching attempts can be observed for all the children. Each child was asked to move to 8 targets equally distributed around the circle. Each target was presented 5 times.
Statistical Analysis
This feasibility study used a single-group, repeated-measures design to assess changes in upper limb motor impairment and function over the course of robotic therapy. Repeated-measures analyses of variance tested statistical significance for each clinical measure and robot metrics. A Bonferroni correction (0.05/4 = 0.0125) was applied to examine changes in kinematic metrics from baseline to follow-up. Two-tailed t tests compared kinematic outcome measures (average across trials for each subject) at baseline and at discharge, at discharge and at follow-up for point-to-point (trained) and for circle-drawing (untrained) movements.
Results
Participants
All children completed the training and evaluation sessions, except 2 children who missed the follow-up evaluation session.
Clinical Scores
Clinical scores previously reported 5 showed a significant change from baseline to discharge in all scales. The FM improved from 18.92 (±7.43 standard deviation [SD]) to 26.92 (±9.76 SD), the QUEST total score from 58.63 (±9.12 SD) to 66.12 (±12.38 SD), and the Modified Ashworth Scale from 6.58 (±1.79 SD) to 5.08 (±1.87 SD) (lower score is better). The Parent Questionnaire scores improved from 9.75 (±6.54 SD) to 14.58 (±6.50 SD) for how much the paretic limb was used for daily tasks and from 7.67 (±5.98 SD) to 12.75 (±5.99 SD) for how well the limb was used functionally.
Analysis of Kinematic Data
Figure 3 summarizes the changes in values of the kinematic metrics at different stages of training. For the trained movements, movement duration, aim, deviation from the straight line, and smoothness all showed statistically significant changes from baseline to discharge (P < .05), with the aim improving, the deviation from the straight line decreasing, and movement smoothness increasing. Hence, changes we observed in the kinematic outcome measures occurred as children also improved on the clinical scales.
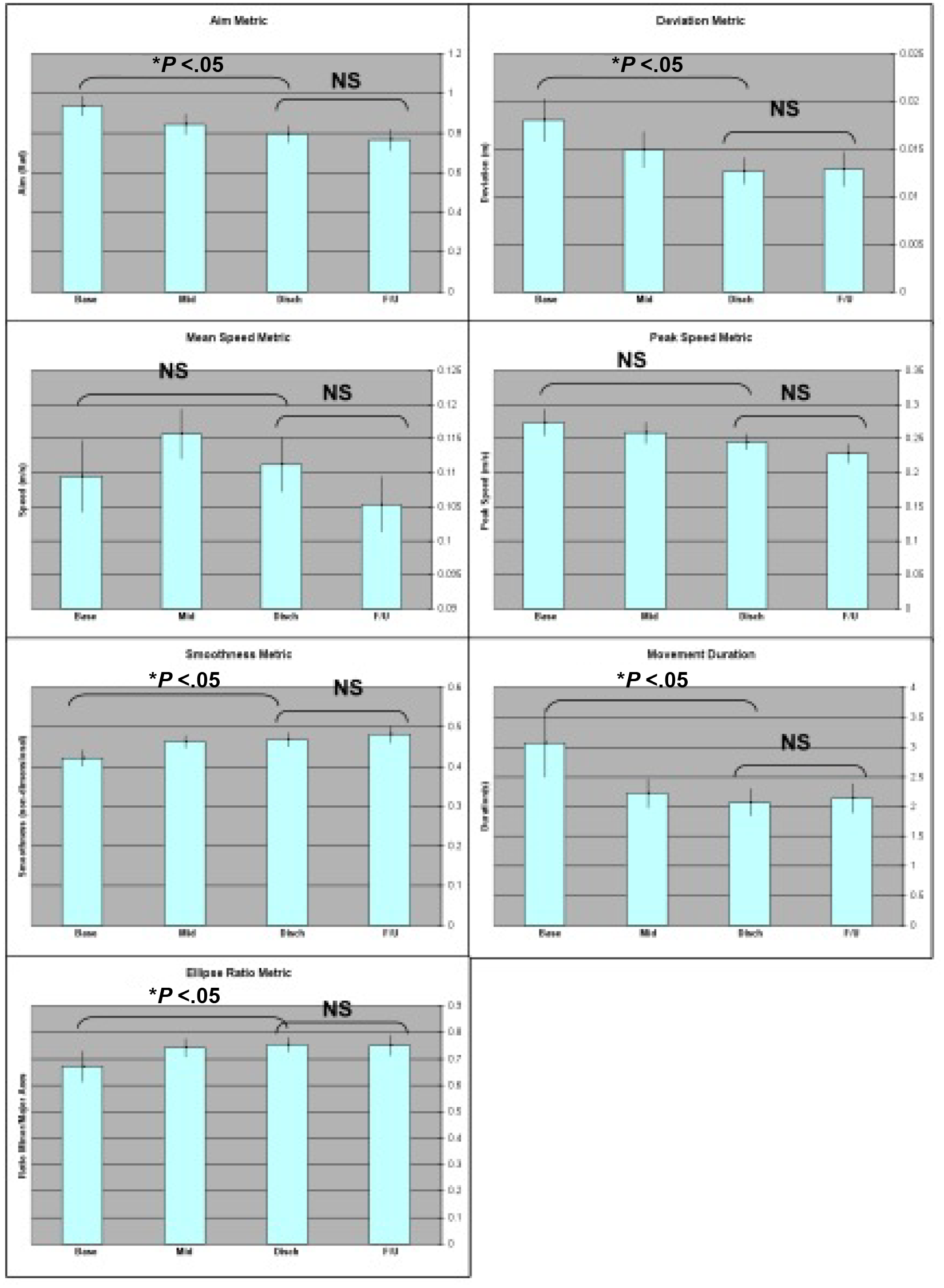
Mean and standard error of kinematic outcome metrics for trained point-to-point and untrained circle-drawing movements. Each plot shows whether changes from baseline to discharge and from discharge to follow-up were significant. *Indicates significance (P < .05).
Robot kinematic metrics showed a significant change from baseline to follow-up (P < .0125) for aiming, deviation from the straight line, peak speed, and smoothness. There were no significant changes for mean speed, duration, or axes ratio. There were no statistically significant differences between discharge and follow-up kinematic measures, which was consistent with the clinical outcomes. There were no statistically significant changes in mean or peak speed at baseline and at discharge or at discharge and at follow-up (although peak speed was significant from baseline to follow-up). For the untrained movements there was a statistically significant increase in the axes ratio over training from baseline to discharge. No statistical difference was found from discharge to follow-up (or from baseline to follow-up). As the axes ratio increased and became closer to 1 (more circular shape), children demonstrated improved interjoint coordination and less influence of abnormal synergy components during circle drawing. 18
Discussion
Habilitation Has Basic Traits of Motor Learning
We tested whether habilitation, that is, the ability of the child to acquire new skills within the spared network, exhibits characteristics similar to unimpaired subjects motor learning, namely, acquisition, retention, and generalization of motor skills. We found that motor habilitation for children with CP indeed has some traits of motor learning. Our study showed that children improved on clinical scales during robot-mediated training. Gains in trained movements, as seen by improved aim, deviation, smoothness, and duration, indicate motor learning in terms of skill acquisition. Retention was evidenced by the children’s ability to retain these gains at least 1 month following training completion. Generalization was seen by better performance of untrained circle-drawing movements (higher axes ratio). Generalization was also evident on gains in clinical measures over the course of robot-aided intervention. 5
Based on the observed changes during recovery, we hypothesize a motor controller consisting of adaptive forward and inverse models is implemented with a Locally Weighted Projection Regression algorithm, employing discrete rather than continuous motor commands. 19 Our model is similar in structure to that proposed by others, 20 especially in that it incorporates time delays. The model predicts that, given limited computational resources, motor performance would be maximized by initially improving the forward model, then refining the inverse model. The fact that aim, deviation from a straight line, and smoothness measures improved, all quantities closely associated with quality of the forward model, but not speed, suggests that the time course of training reflected in the data is consistent with our model. Training of the forward model first would allow the motor control system to predict the result of a move in process, based on sensory information. Tuning of the inverse model would follow and hence allow for faster movements to be made without increasing the endpoint error. One has to interpret this model with the appropriate caveats. Training must be extended beyond this pilot 16 sessions to allow us to investigate whether speed is optimized after aim, deviation from the straight line, and smoothness significantly improve. Such studies will also have to be compared with other strategies to enhance upper extremity function.21,22
Conclusion
While most descriptions of motor habilitation in CP are highly qualitative, we provided a quantitative, kinematic characterization for 12 subjects. The results of this pilot suggest that if motor habilitation is characterized by a model of motor learning, robot-mediated therapy for children with CP should consider testing of motor learning traits, such as generalization, interference, order-effect, saltation (ie, improvement is followed by an apparent period of stagnation, which is followed by further improvement), blending of submovements, and timelines of learning. Increased knowledge in this area could further advance the design of distinct robot-mediated interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs H. I. Krebs and N. Hogan are co-inventors of the Massachusetts Institute of Technology (MIT) held patent for the robotic device used in this work and hold equity positions in Interactive Motion Technologies, Inc, Watertown, Massachusetts, a company that manufactures this type of technology under license to MIT.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by National Institute of Child Health and Human Development Grant R01-HD-045343, the Veterans Administration Grant V512(P)P-521-02, the Cerebral Palsy International Research Foundation, and the Charles H. Hood Foundation, Boston, Massachusetts.