
Abstract
Background. Children with unilateral spastic cerebral palsy (USCP) have strength, coordination, and balance deficits affecting gross motor skills, such as walking, running, and jumping. However, there is a paucity of evidence for effective treatments for lower-extremity (LE) function in children with USCP. Objective. To determine the effectiveness of LE intensive functional training (LIFT) compared with an attention control group receiving upper-extremity bimanual training (Hand-Arm Bimanual Intensive Therapy [H-HABIT]). Methods. A total of 24 children with USCP were randomized to receive 90 hours of LIFT (5.8 [2.3] years) or an equivalent dosage of H-HABIT (5.1 [2.6] years) delivered 2 h/d, 5 d/wk for 9 weeks. Caregivers were trained to administer the intervention in the home setting. Progress and skill progression were monitored, and supervision was provided via weekly telerehabilitation. The primary outcome was the 1-minute walk test (1MWT). Secondary outcomes included self-selected and fast walking speeds, ABILOCO-kids, 30-s chair rise test, and single-leg stance. Results. LIFT showed greater improvement for the 1MWT (P = .017) and ABILOCO-kids (P = .008) compared with controls. The other secondary outcomes were not different between groups. Conclusions. The administration of LE intensive interventions in the home setting by caregivers was shown to be an effective and novel mode of delivery for improving gait capacity and performance. LIFT delivered in the home setting using telerehabilitation for monitoring resulted in improvements in ambulation distance and overall walking ability as compared to an intervention of equal intensity and duration that also controlled for the increased social interaction and attention between caregiver and child.
Keywords
Introduction
Cerebral palsy (CP) describes a group of disorders of the development of movement and posture causing activity limitations that are attributed to nonprogressive disturbances that occurred in the developing fetal or infant brain. 1 Children with unilateral spastic CP (USCP) present with muscle weakness, spasticity, and limited selective voluntary control, resulting in gait and balance impairments.2,3 These gait abnormalities, including reduced gait speed, may affect a child’s daily activities, sports and leisure, quality of life, and social interactions.4-6 Although most children with USCP can walk without assistance, motor skill impairments should be addressed in order to improve gross motor function in everyday life.
Over the years, the paradigm has shifted from stand-alone treatment of impairments, such as strength and spasticity, to approaches focusing on improving motor function and activities of daily living. Lower-extremity (LE) strength training has been studied in children with USCP, and though it has shown to be effective in improving muscle strength, the effects of strength training alone on gross motor function, balance, and gait are questionable. 7 An evidence-based review of interventions designed for CP concluded that motor learning–based approaches emphasizing intensity are effective in improving function. 8 Although many intensive activity-based rehabilitation approaches targeting motor skill learning and motor function are available for the upper extremities in those with USCP, this evidence-based review highlighted the paucity of evidence for interventions targeting motor function in the lower extremities.8,9
Intensive training for the upper extremities in children with USCP has been reported to be effective when delivered as a 90-hour massed practice in a camp setting.10-13 Bleyenheuft et al 14 investigated 90 hours of intensive training for combined upper and lower extremities delivered in a one-to-one supervised camp model for children with USCP and reported improvements in both upper and LE function. 14 However, the appropriate dosage for isolated LE intensive training in children with USCP has not been investigated, without the confounding influences of upper-extremity training. Additionally, mode and location of delivery are also vital to an intervention. Camps can be logistically complex, expensive and difficult to access for many families. The principles of motor learning suggest that transfer of motor skill learning is optimal when the training environment simulates the actual setting. 15 Therefore, a distributed model where caregivers provide one-on-one training within the home setting is an alternative delivery option compared with an intensive day camp.
In designing the LE intensive functional training (LIFT) protocol, we integrated the principles of motor learning, such as intensive and structured practice, active participation, and skill/exercise progression. The aim of LIFT was to target strength, balance, and coordination deficits of the lower extremities, with an emphasis on the involved leg, in order to improve gait and LE functioning. Therefore, the purpose of this study was to test the effectiveness of 90 hours of distributed, LE intensive functional training (LIFT) on gait and LE function compared with a control intervention, Hand-Arm Bimanual Intensive Therapy (H-HABIT) of similar intensity and duration for the upper extremities. Both interventions were delivered in a home setting by the caregivers to optimize the transfer of motor skill learning while controlling for the increase in one-on-one social interaction between the caregiver and participant during the intervention. 16 We hypothesized that children in the LIFT group would demonstrate greater improvement in gait and LE function in comparison to children in the control group.
Methods
Design Overview
This was a randomized control trial (NCT02299284) reported according to CONSORT guidelines. 17 Participants were recruited from families attending a Children’s Hemiplegia and Stroke Association (CHASA) retreat, clinics in the New York City area, our website (http://www.tc.edu/centers/cit/), and clinicaltrials.gov. The Institutional Review Board of Teachers College, Columbia University and Louisiana State University Health Sciences Center, New Orleans, approved the study. The participating families signed the informed consent form. Children were assessed twice prior to the intervention (baseline 1 and baseline 2, assessed 1 week apart), immediately after the intervention (posttest), and at a 6-month follow-up. The investigators administered the first baseline assessment in person, and the caregivers administered second baseline in their home, which was supervised online by the supervisor. Caregivers were trained and then required to deliver either LIFT or H-HABIT control activities to their child for 2 h/d for 5 d/wk for a total of 9 weeks (90 hours). The 2 hours of training could be performed consecutively or broken into two 1-hour or four 30-minute sessions at different times of the day. Supervisors in each group telemonitored activities remotely once a week (1 hour) using Adobe Connect.
Setting and Participants
Children with USCP between 2 and 13 years of age were invited to complete a screening. Inclusion criteria were the following: (1) Gross Motor Functional Classification System I and II, (2) ability to walk independently, (3) ability to follow 2-step instructions and complete testing, and (4) ability of caregiver to provide one-on-one attention to the child during daily activities. The investigators confirmed the child’s impairments using either a video-recorded or in-person screening. Exclusion criteria were the following: (1) cognitive delay preventing 2-step instructions, (2) health diagnoses not associated with USCP, (3) visual problems preventing performance of intervention/testing tasks, and (4) caregivers unable to commit to duration of intervention.
Randomization and Interventions
Randomization
Participants were recruited over multiple cohorts, where each cohort consisted of at least 4 children. For each cohort, children were matched into groups stratified by age. They were randomized to either LIFT or H-HABIT control using concealed allocation.18,19 An individual without any direct participation in the clinical aspects for the study performed the randomization, random number generation, and preparation of allocation materials off-site.
Interventions
LIFT
The goal of LIFT was to improve gait and LE gross motor function by targeting strength, balance, and coordination impairments of the lower extremities, with an emphasis on the involved leg. LIFT was based on principles of (1) motor learning, (2) intensive and structured practice, (3) skill or activity progression, and (4) resistance training. Thus, it was a hybrid of strengthening and motor learning–based principles, involving exercises and activities with dosing specific to the primary goal (ie, strength, balance, or coordination). Skill progression was used to make LIFT challenging and intensive enough to elicit changes in motor skills and function. The strengthening domain primarily involved LE exercises using body weight as resistance that targeted functional activities (eg, sit to stand, step ups, vertical jumping, stair climbing). Exercises targeting muscle groups important for gait were also included to a lesser extent with muscle-specific exercises (eg, bridges, clamshells, heel raises). The balance domain included activities such as tandem walking, one-leg standing, and balancing on unstable surfaces and balance beams. The coordination domain involved activities such as ball kicking, jumping jacks, hopping through squares (hopscotch), and galloping/skipping. Caregivers were asked to pick a minimum of 4 strengthening, 2 balance, and 2 coordination activities per day from a reference manual of activities. They were free to pick activities from any of the 3 domains once minimum requirements were met. (Protocol details are provided in supplemental material—LIFT description).
Control group
The H-HABIT control group performed bimanual activities, designed to improve reaching, grasping, releasing, in-hand manipulation, and movements related to using the affected hand as an assisting hand. Children performed activities designed as child-friendly games. The intervention involved specific bimanual activities, shaping of the environment to promote bimanual hand use, and grading of task demands.10,11,18,19
Caregivers in the LIFT group performed activities that involved only the lower extremities, and caregivers in H-HABIT control performed activities that involved only the upper extremities. Caregivers in both groups were instructed to avoid performing activities that involved the whole body during training. Supervisors monitored daily logs to ensure that there was no treatment overlap. Children were free to engage in activities without restriction outside the study’s daily 2 hours. All participants could receive usual and customary care during the study. We did not control what both LIFT and H-HABIT control groups did outside the training hours, and participants were free to continue their normal routines.
Caregiver training
Caregivers received 3 training sessions prior to the treatment. The first session was a group session where an experienced supervisor described the conception and development of LIFT and provided caregivers with a reference manual, which included illustrations and descriptions of intervention activities, strategies, and instructions for progression specific to each activity/exercise (see supplemental material). In the first one-on-one session, supervisors trained the caregivers using an instruction manual in the administration of the outcome measures, demonstrated the testing protocol with the participant, and then collected baseline 1 results. In the second one-on-one training session, all intervention activities from the manual were performed with the child, including progression of each activity. Caregivers then performed the activities with their child using feedback about performance as the supervisor modeled how to direct the LIFT activities. The last training session overlapped with the first hour of the 90-hour intervention, where the supervisor assisted caregivers with picking appropriate activities from the manual to begin and provided feedback. Following training, participants were monitored via webcam-based software (Adobe Connect) once per week while they performed the activities at home. The supervisor closely monitored activities by checking daily online logs.
Although caregivers were free to choose activities from the manual, the supervisor ensured that the structure of the intervention was maintained and that skill progression was followed, based on weekly remote sessions and logs. Strength progression was done by increasing the number of repetitions, sets, and load. Balance and coordination were progressed by increasing hold time, speed and accuracy demands, and complexity. Additional support via phone/email and assistance with decision making was provided as needed (see supplemental material).
Outcomes: Primary and Secondary Outcome Measures
The primary outcome measure was the 1-minute walk test (1MWT). 20 This measure was selected because the age of some participants may have resulted in decreased attention to task and ability to comprehend pacing required for 6 minutes. Because it is a fast walking test, it is a measure of walking capacity and can be completed in a short period. Secondary outcome measures were the 10-Meter Walk Test 21 (self-selected and fast gait speed), 30-s chair rise 22 (strength), single-leg stance on the affected side 23 (balance), and ABILOCO-kids 24 —a parent-reported measure of ambulatory function.
Statistical Analysis
Sample size calculations were based on estimates obtained from pilot data and the first cohort in this study. Calculations were performed using the “longpower” package in R (R Foundation 2017). 25 For the 1MWT, we specified a linear mixed-effects model that included the group by time interaction and a =0.05, 1 − b =0.8, δ =6.5, number of testing sessions =2, and the parameter of interest as the interaction between testing session and intervention group. Results indicated that 11.5 children (rounded up to 12) per group were required.
An intent-to-treat based analysis was performed, as specified by CONSORT guidelines. 26 All statistical analyses were performed using R (R Core Team, 2017). 25 Linear mixed-effects models were used to estimate interindividual variability and intraindividual patterns of change over time. Linear mixed-effects models permit flexibility in the underlying structure of the data and account well for missing data when observations are missing at random, which is useful for clinical studies.27,28 Separate models were fit for each outcome measure using maximum-likelihood estimation and an unstructured variance-covariance structure. Models were specified with fixed effect terms, including intervention group, test session, and the group by session interaction. Random effects included intercepts of participants and by-participant and by-session slopes. We compared how well separate models fit the data. We did this by starting with a simple model then adding effects (ie, parameters) that we were interested in comparing. We began with the most basic model (ie, null model), which does not include a session or group effect. Then, we examined a reduced model, which adds the session and group effect. Finally, a full model which contains the effects of group, session, and a Group × Session interaction was fit to the data. Likelihood ratio tests were used to compare models. Akaike information criterion (AIC) and Bayesian information criterion (BIC), measures of model goodness-of-fit, were also used to compare the models. Lower AIC or BIC values indicate a better fit for models estimated on the same data. Reproducible statistical code has been included as a supplementary file. Reliability between caregiver- and supervisor-administered assessments was examined using paired t-tests and intraclass correlation coefficients. An α level of .05 was considered statistically significant.
Results
Participant Flow
A total of 40 qualified participants were randomized into the 2 intervention groups, and 24 individuals (12/group) completed the intervention. The patient flow is provided in the CONSORT diagram (Figure 1). Table 1 describes participant characteristics. There were no baseline differences between the groups for any measure. Three children in the LIFT group did not complete the 6-month follow-up.
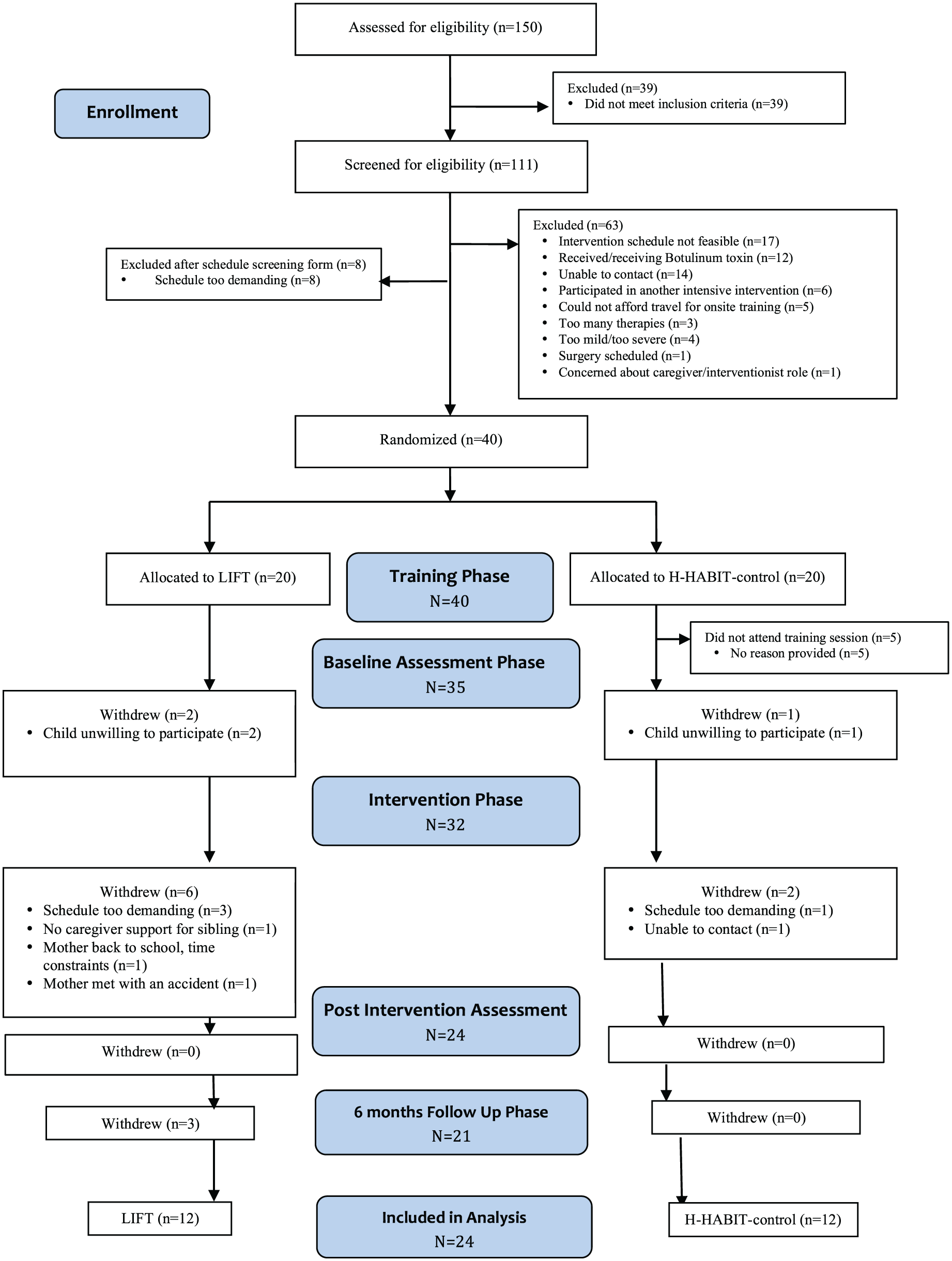
Participant flow through the study.
Participant Characteristics and Baseline Measurements.
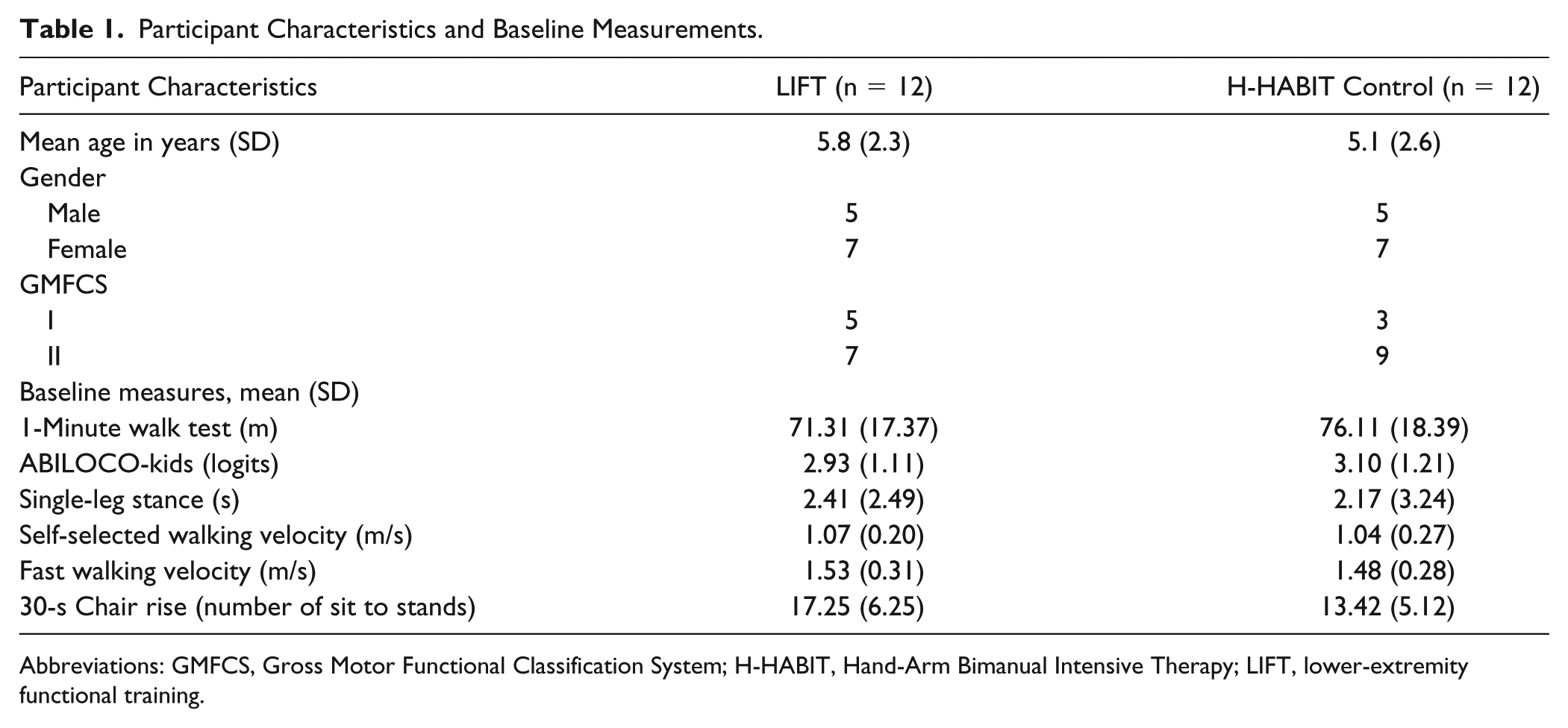
Abbreviations: GMFCS, Gross Motor Functional Classification System; H-HABIT, Hand-Arm Bimanual Intensive Therapy; LIFT, lower-extremity functional training.
Treatment Characteristics
Participants in the LIFT group completed 87.4 (7.8) hours, and those in the H-HABIT control group completed 82.9 (12.7) hours, on average, of home training, respectively. The LIFT group on average spent 46.2% of their total training time in strengthening activities, 21.3% in balance, and 32.4% in coordination activities. Of the 46.2% of total training time spent in the strengthening domain, 30.1% was spent performing functional strengthening activities and 16.1% performing muscle specific exercises. Two children in the LIFT group did not complete training logs; however, the caregivers verbally verified the activities and participated in weekly supervised sessions.
The H-HABIT control group on average spent 38% of the time in manipulative games and tasks, 16% in functional tasks, 6% in gross motor tasks, 11% in fine motor tasks, 9% in arts and crafts, 8% in card games, 1% in video games, and 10% in miscellaneous upper-limb activities.
Caregiver- and Supervisor-Administered Assessment Consistency
There were no statistically significant differences between the supervisor-administered baseline and caregiver-administered pretest for any measure (P > .05). The 1MWT and single-leg stance had moderate reliability, and the self-selected walking velocity, fast walking velocity, and 30-s chair rise had good reliability (Table 2). Therefore, caregiver-administered baseline assessments only were used as the pretest values in the analyses.
Comparison Between Supervisor and Caregiver-Administered Testing.
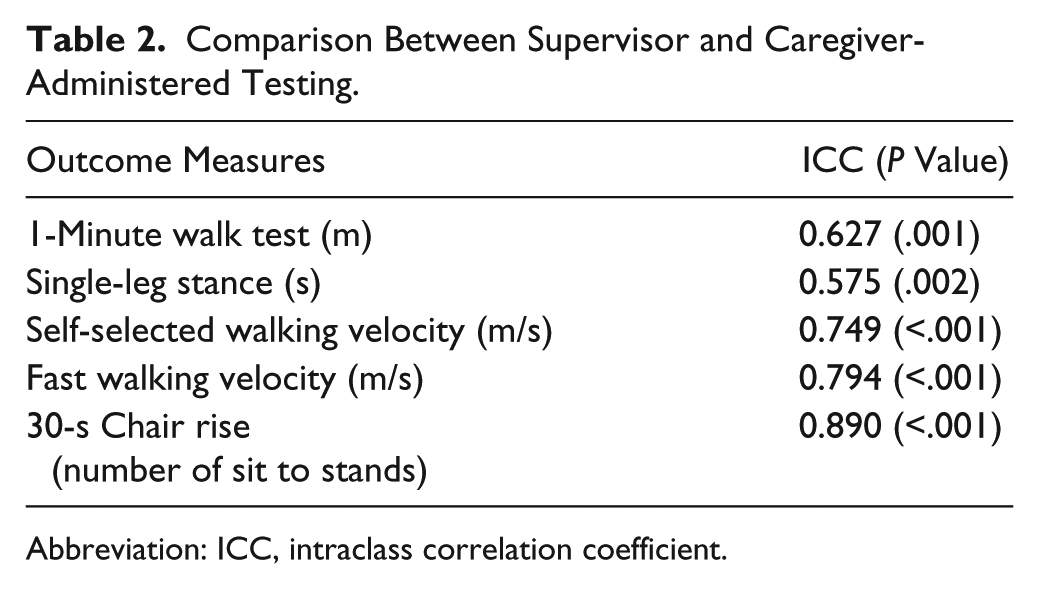
Abbreviation: ICC, intraclass correlation coefficient.
Primary Outcome Measure
Figure 2 displays the means and standard error for all measures across each time point. Children in the LIFT group made greater improvements in the 1MWT between the pretest and posttest relative to H-HABIT controls (Figure 2A). Comparisons between models with and without the Group × Session interaction supported this observation: χ(1) = 5.72; P = .017. Table 3 provides parameter estimates for the fitted models. The lower AIC and BIC values also suggest that the model with the interaction term fit the data better than the null or reduced model. Therefore, the LIFT group demonstrated a greater rate of improvement over testing sessions relative to H-HABIT control.
Parameter Estimates for Linear Mixed Models Fit to Outcome Measures. a
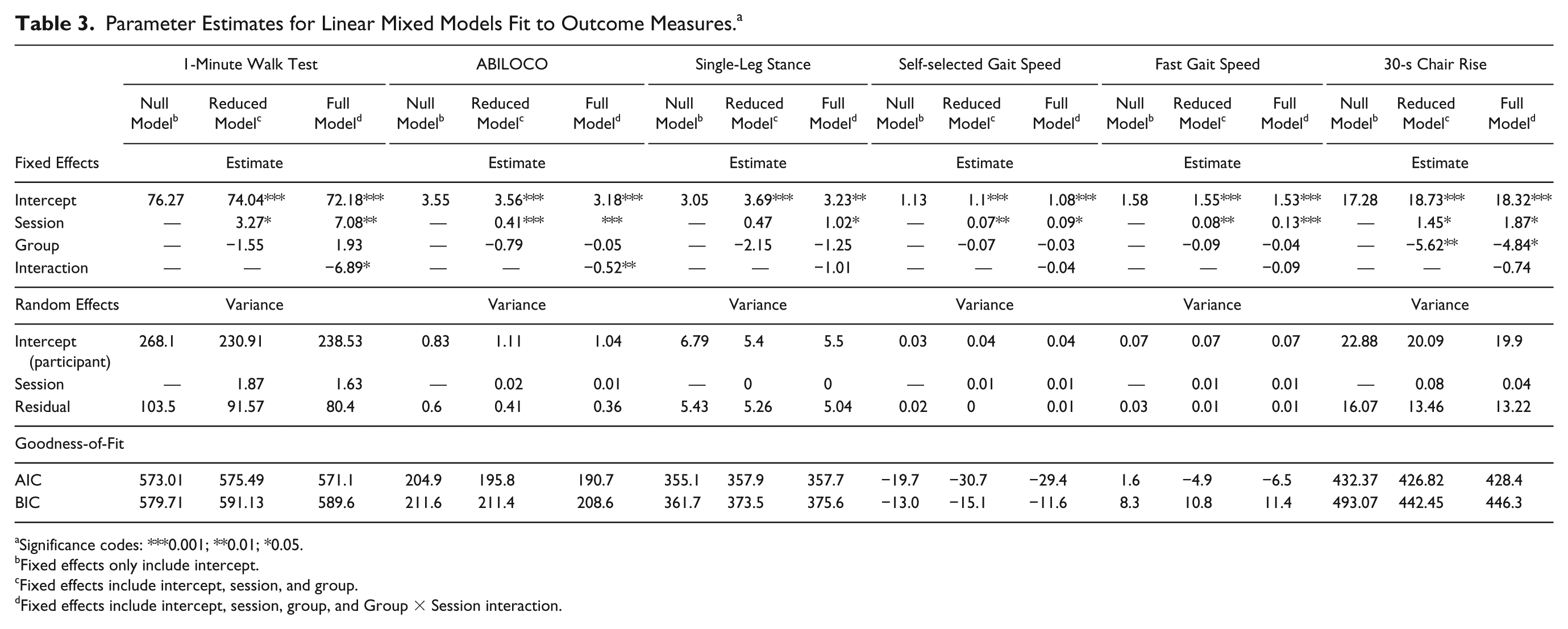
Significance codes: ***0.001; **0.01; *0.05.
Fixed effects only include intercept.
Fixed effects include intercept, session, and group.
Fixed effects include intercept, session, group, and Group × Session interaction.
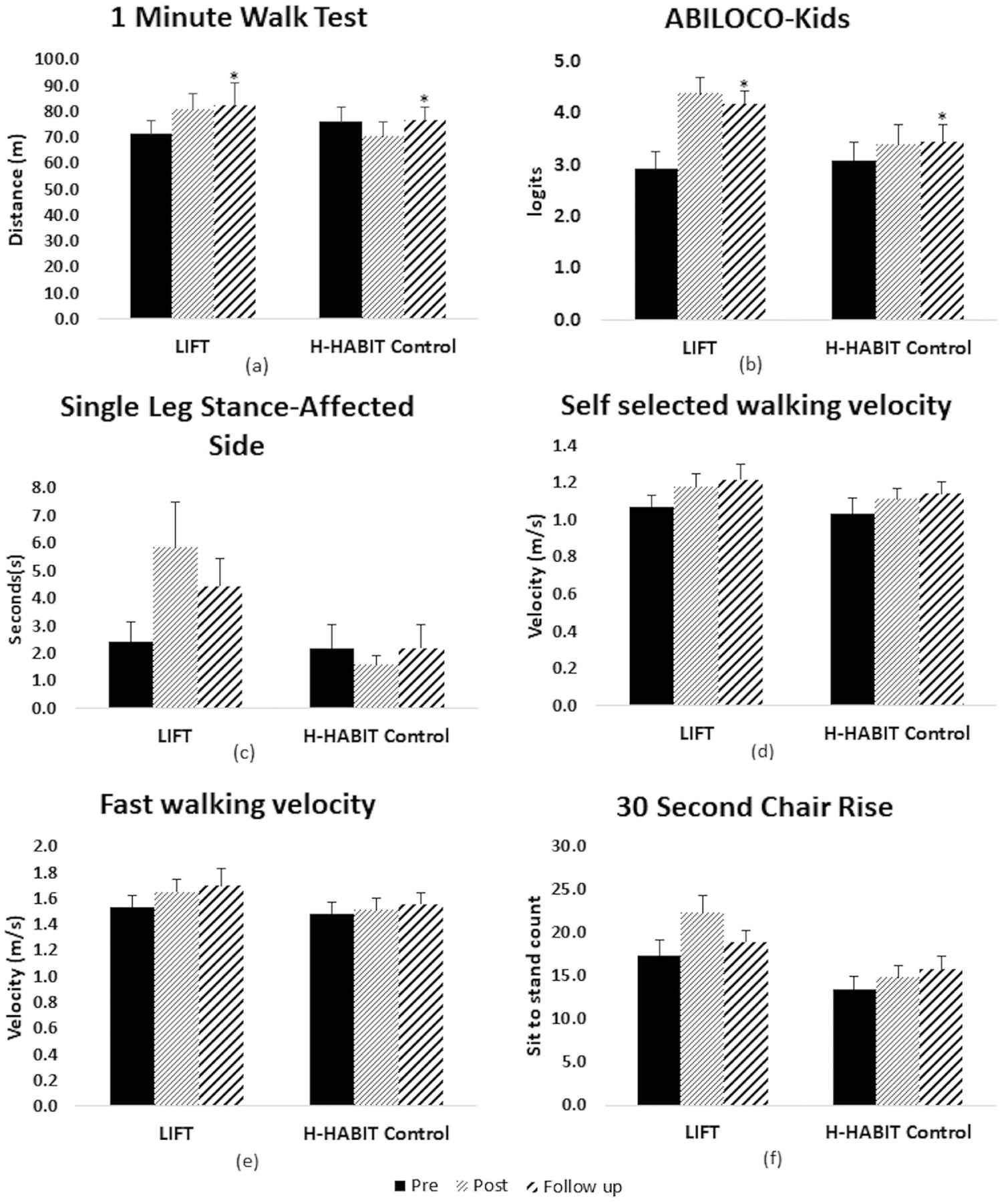
Mean and standard error across testing sessions for (A) 1-minute walk test, (B) ABILOCO-kids, (C) single-leg stance, (D) self-selected walking velocity, (E) fast walking velocity, and (F) 30-s chair rise.
Secondary Outcome Measures
Children in the LIFT group made greater improvements in the ABILOCO-kids between the pretest and posttest as compared with the H-HABIT control group (Figure 2B). One child in each group had a ceiling effect. Comparisons between models with and without the Group × Session interaction supported this observation: χ(1) = 7.08; P = .008. The lower AIC and BIC values also suggest that the model with the interaction term fit the data better than the null or reduced model.
Children in the LIFT group made greater improvements in the single-leg stance between the pretest and posttest relative to those in the H-HABIT control group (Figure 2C). However, comparisons between the full and reduced models suggested that the interactions were not significant: χ(1) = 2.14; P = .14. Parameter estimates (Table 3) suggest that there was a main effect for session.
There were no significant differences between LIFT and H-HABIT for self-selected walking velocity [χ (1) = 0.72; P = .39] for comparison between full and reduced models (Figure 2D). Parameter estimates (Table 3) suggest that there was a main effect for session. For fast walking velocity, children in the LIFT group reported greater improvements between the pretest and posttest (Figure 2E). Comparisons between the full and reduced models suggested that the interaction approached significance: χ(1) = 3.61; P = .06.
Children in the LIFT group reported greater improvements between pretest and posttest for 30-s chair rise (Figure 2F); however, comparisons between the full and reduced models suggested that the interaction was not significant: χ(1) = 0.42; P = .51.
Discussion
This study examined the effectiveness of 90 hours of caregiver-administered LIFT on gait and LE function. To our knowledge, this was the first randomized controlled trial to examine the effectiveness of intensive LE training in children with USCP provided by caregivers in the home setting using telerehabilitation.
According to the activity domain of the World Health Organization’s International Classification of Functioning, Disability and Health (ICF), capacity is representative of what the person is capable of doing. Performance, on the other hand, represents what a person actually performs in everyday life. 29 Distance ambulated during a 1MWT represents a potential cost-effective and user-friendly method of assessing gait capacity in a clinical setting. Children in the LIFT group had greater improvements in gait capacity as demonstrated by increased distances, which exceeded the MCID for a large effect size. 30 This was corroborated by an increase in fast gait speed at both time points that approached significance and exceeded the MCID for the LIFT group only 31 (Figure 2E). There was a decrease in the 1MWT distance for the H-HABIT group posttraining. This may be a result of sitting for 2 hours per day. However, participants in both groups were free to walk, run, and perform regular physical activities outside the hours of training. Because we did not monitor what the children did outside of the 2 hours of training, we cannot rule out this as a possibility.
Parents’ perception of their child’s usual walking performance, as measured by ABILOCO-kids, improved significantly for the LIFT group. The ABILOCO-kids assesses an individual’s ability to move about effectively in their environment. Therefore, a significant increase in both measures post-LIFT reflects improvements in both walking capacity and performance under the ICF construct.
Inspection of the 30-s chair rise test (Figure 2F) revealed a larger increase in functional strength in the LIFT group; however, the difference between the groups was not significant. This was surprising given that a large percentage of the intervention was directed toward LE functional strengthening activities. However, the 30-s chair rise was often difficult to keep the youngest participants focused for the 30 seconds. Improvements in LE strength in both groups could also be attributed to developmental changes in gross motor function.
There was a difference in the outcomes of LIFT and H-HABIT for improving motor function in their respective groups. LIFT was able to elicit significant improvements in gait capacity and performance with remote supervision, whereas H-HABIT led to improvements in hand dexterity, but not bimanual hand function. This was attributed to the absence of in-person supervision because bimanual function involves more complex, fine motor skills as compared with LIFT. 19 The participation rate was slightly higher in the LIFT group compared with the H-HABIT control group. Most LIFT activities could be performed as play activities, before or after school, indoors or outdoors. This could have been more appealing for children and caregivers than seated bimanual activities. Differences between LIFT and H-HABIT were further influenced by the interaction between remote supervision and nature of intervention, caregiver role, and home setting.
Evidence suggests that if home programs are designed according to the best available evidence and parent preferences, parents are more likely to be adherent and implement it at a higher dose. 32 The LIFT protocol provided caregivers with an intensive structured training tool in their home setting. This saved multiple visits to the research center, allowed them to use resources readily available at home, and allowed them carry out training per their schedules. The majority of families who completed the study found it easy to schedule and execute the training sessions. They were able to implement the activities listed in the manual in different ways, indoors and outdoors. In contrast to a clinical setting, the caregivers had more control over the training aspects. The home-based setting did carry a risk of disturbing the psychosocial dynamics within the family, but to avoid this, we advised caregivers to separate training time from the rest of their daily routine. They were instructed to use the training materials and equipment only during the designated 2 hours per day. Although we did not measure how the intervention affected the parent-child relationship objectively, efforts were made to prevent the training from disrupting family dynamics.
In addition to providing the intensive training, caregivers administered the pretests and posttests under online supervision. Although it limited the number and complexity of the assessments, it spared the families from the expense and logistics of traveling to our research laboratory on multiple occasions. Our battery of assessments consisted of timed tests, which were simple and easy to perform, but decreased complexity of the outcome assessments may have prevented us from realizing quantitative changes in the children’s gait (eg, kinematics). However, the goal was to make the study more accessible for families. The lack of significant difference between the baseline measures administered by the caregivers and supervisor suggests that performing the testing and training in children’s natural environment is effective.
Limitations and Future Considerations
Although the LIFT design was based on previously established protocols, we faced high attrition. Of the 8 participants who did not complete the LIFT program, 2 participants dropped out before starting the training, and 4 participants dropped out at the end of the first week of training (Figure 1). Future studies could utilize detailed interviews and mock training sessions for families to experience the actual requirements of the training before they commit to participate. Furthermore, the LIFT dosage was modeled off bimanual training and HABIT-ILE studies, which have been extensively studied. However, the appropriate dosage for LE training in USCP has not been determined. It is plausible that a lower dosage would be equally effective in the LE. It is possible that fewer training hours are needed and that a frequency of 3 times per week may be more feasible and beneficial given resistance training guidelines that recommend 48 hours between sessions. 33
Another limitation was that we did not control what the participants did outside the training hours. Whereas this was done to prevent disruption of the psychosocial dynamics, monitoring the amount of physical activity outside the training could have provided useful information. In addition, an in-depth analysis of the relationship between the caregiver experience and motor improvements could provide important information about the applicability of such home-based intensive programs in clinical practice.
Additionally, while the overarching goal of LIFT was to improve gait and LE motor function, personalized functional goals were not defined. Goal-based intensive training has been found to be effective in improving gross motor function in children with CP practiced in a camp setting. 14 However, LIFT was distributed across 9 weeks and was delivered in a home setting by caregivers. This allowed us to include families from a wide geographical area but limited us to remote supervision. Goal-based training would have required massed practice and intensive supervision and possibly a combination of in-person and remote sessions to incorporate personalized functional goals and scaffolding of activities. Future studies would need to combine distributed practice and intensive supervision while incorporating functional goals in LIFT.
Conclusion
This randomized controlled trial utilized a novel design of delivering intensive LE training in a home-based setting, using telerehabilitation. The administration of a LE intensive intervention in the home setting by caregivers was shown to be an effective and novel mode of delivery for improving gait capacity and performance. The 90 hours of LIFT resulted in improvements in ambulation distance and overall walking ability as compared with an intervention of equal intensity and duration while controlling for the increased social interaction and attention between caregiver and child. Future dosing studies are needed to determine whether reduced training hours, an altered practice schedule, or including personalized functional goals would produce similar or greater improvements to those reported in the present study.
Supplemental Material
Supplemental_Material – Supplemental material for Effectiveness of Lower-Extremity Functional Training (LIFT) in Young Children With Unilateral Spastic Cerebral Palsy: A Randomized Controlled Trial
Supplemental material, Supplemental_Material for Effectiveness of Lower-Extremity Functional Training (LIFT) in Young Children With Unilateral Spastic Cerebral Palsy: A Randomized Controlled Trial by Bhavini K. Surana, Claudio L. Ferre, Ashley P. Dew, Marina Brandao, Andrew M. Gordon and Noelle G. Moreau in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We would like to thank the children and their families for participating.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
Authors’ Note
ClinicalTrials.gov identifier: NCT02299284.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by support from a Children’s Hemiplegia and Stroke Association (CHASA) grant.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.