
Abstract
Background. The relationship between structural and functional integrity of descending motor pathways can predict the potential for motor recovery after stroke. The authors examine the relationship between brain imaging biomarkers within contralesional and ipsilesional hemispheres and hand function in well-recovered patients after subcortical stroke at the level of the internal capsule. Objective. Measures of functional activation and integrity of the ipsilesional corticospinal tract might predict paretic hand function. Methods. A total of 14 patients in the chronic stable phase of motor recovery after subcortical stroke and 24 healthy age-matched individuals participated in the study. Functional MRI was used to examine BOLD contrast during passive wrist flexion–extension and paced or maximum-velocity active fist clenching. Functional integrity of the corticospinal pathway was assessed by transcranial magnetic stimulation to obtain motor-evoked potentials (MEPs) in the first dorsal interosseus muscle of the paretic and nonparetic hands. Fractional anisotropy and the proportion of traces between hemispheres in the posterior limb of both internal capsules were quantified using diffusion-weighted MRI. Results. Patients with smaller MEPs had a weaker paretic hand and more primary motor cortex activation in their affected hemisphere. Asymmetry between white matter tracts of either hemisphere was associated with reduced precision grip strength and increased BOLD activation within the contralesional dorsal premotor cortex for demanding hand tasks. Conclusion. There may be beneficial reorganization in contralesional secondary motor areas with increasing damage to the corticospinal tract after subcortical stroke. Associations between clinical, functional, and structural integrity measures in chronic stroke may lead to a better understanding of motor recovery processes.
Introduction
About 75% of those who experience stroke have lingering upper-limb impairment. 1 Based on clinical presentation alone, it is difficult to gauge which patients will recover upper-limb function several months later. 2 This study examines the relationship between neuroimaging parameters and upper-limb function months after stroke in well-recovered patients.
Experimentally, structural and functional cerebral parameters may indicate motor function at the chronic phase after stroke. With respect to functional magnetic resonance imaging (fMRI), increased activation in motor areas of both the damaged hemisphere (DAM-H) and the hemisphere contralateral to the affected one (CON-H) have been reported. 3 Greater chronic motor impairment is associated with an increase of fMRI activation in motor areas of both hemispheres during simple, repetitive hand movements. 4 In contrast, good motor-recovery is related to a near-normal DAM-H fMRI activation associated with movement execution of the affected hand. 5 The importance of CON-H activation is not completely understood but may be indicative of good outcomes for some patients.6,7
Clinical outcome after stroke may depend on residual functional integrity of the corticospinal pathways as assessed using transcranial magnetic stimulation (TMS).8-10 Greater motor impairment is associated with increased motor thresholds 11 and decreased motor recruitment. 12 An association between structural integrity of descending motor pathways and motor impairment in chronic stroke patients has been shown, 13 and this parameter is a stronger predictor for motor recovery than is BOLD response in motor areas in patients 3 to 5 months after stroke. 14 Stinear and colleagues 10 identified an association between corticospinal integrity and motor impairment in chronic stroke patients. They found that white matter integrity (asymmetry in fractional anisotropy [FA]) negatively predicted motor impairment score (Fugl-Meyer score) with an r2 = 0.67 as did the presence of TMS motor-evoked potentials (MEP; r2 = 0.58). However, most predictive for future outcome of motor performance after training was a combination of absent TMS MEPs and FA asymmetry (r2 = 0.71). 10 Conversely, although lateralization of cortical activation obtained with FMRI predicted the motor impairment score, it was not a predictor of change scores resulting from training.
In the present multimodal investigation, we investigate the functional role of increased BOLD signal activation within the CON-H and its association with corticospinal integrity within the DAM-H and hand motor function in 14 chronic subcortical stroke patients. We examined 2 hypotheses. First, following from previous studies, an increase in fMRI activation in the DAM-H for patients with greater motor impairment was expected. 4 Second, activation in contralesional primary and secondary motor areas was expected to correlate positively with ipsilesional pyramidal tract damage 13 and be greatest under conditions of highest demand. To examine this, we compared fMRI activations of paretic hand fist clenching at maximal rates versus a low-frequency paced condition. An understanding of these associations at the chronic stage after stroke might be helpful for selecting the most promising measurement method for predicting motor outcome in patients in the acute or subacute stage.
Methods
Participants
Patients were recruited from the Neurological Department of the University of Greifswald. All patients had been diagnosed with a first-ever subcortical ischemic stroke more than 5 months previously (mean = 14.2 ± 5.0 months). Exclusion criteria were epileptic seizures, neuropsychological or language impairment, or lasting paresis of the affected hand with a score greater than 4 of 5 (MRC [Medical Research Council] Scale). Furthermore, patients with cortical lesions and carotid artery stenosis of more than 70% were excluded. Overall, we investigated 14 patients (10 male/4 female; mean age = 58.0 ± 14.4 y; range = 29-75 years; 2 left handed and 12 right handed; average score of handedness 15 : 86.2 ± 23.9) with subcortical circumscribed lesions (Table 1, Supplementary Figure 1). The group had the same number of lesions in the dominant and nondominant hemispheres (right-handed: 6 left- and 6 right-hemispheric lesions; left-handed: 1 left- and 1 right-hemispheric lesion).
Demographic and Clinical Data of Stroke Patients
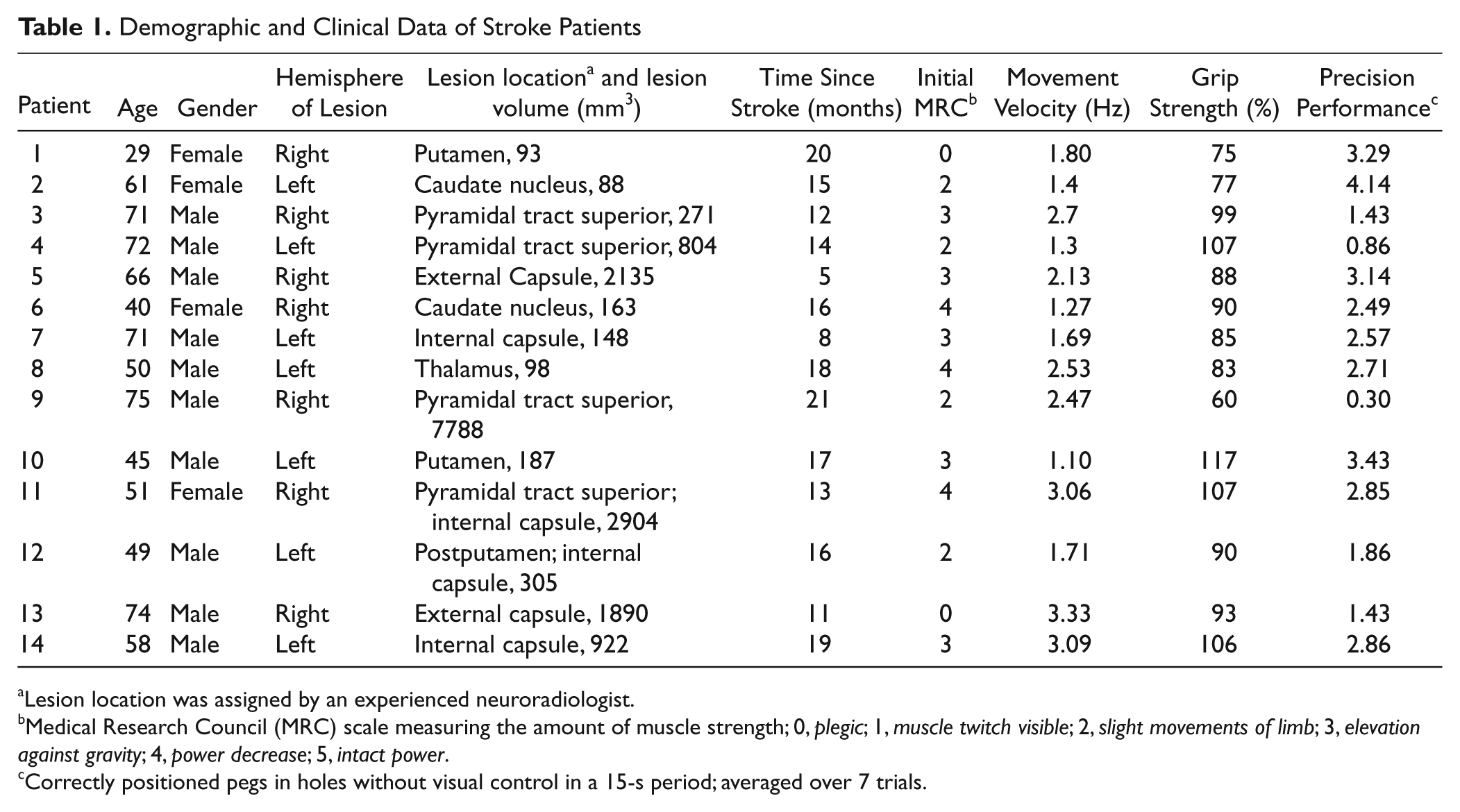
Lesion location was assigned by an experienced neuroradiologist.
Medical Research Council (MRC) scale measuring the amount of muscle strength; 0, plegic; 1, muscle twitch visible; 2, slight movements of limb; 3, elevation against gravity; 4, power decrease; 5, intact power.
Correctly positioned pegs in holes without visual control in a 15-s period; averaged over 7 trials.
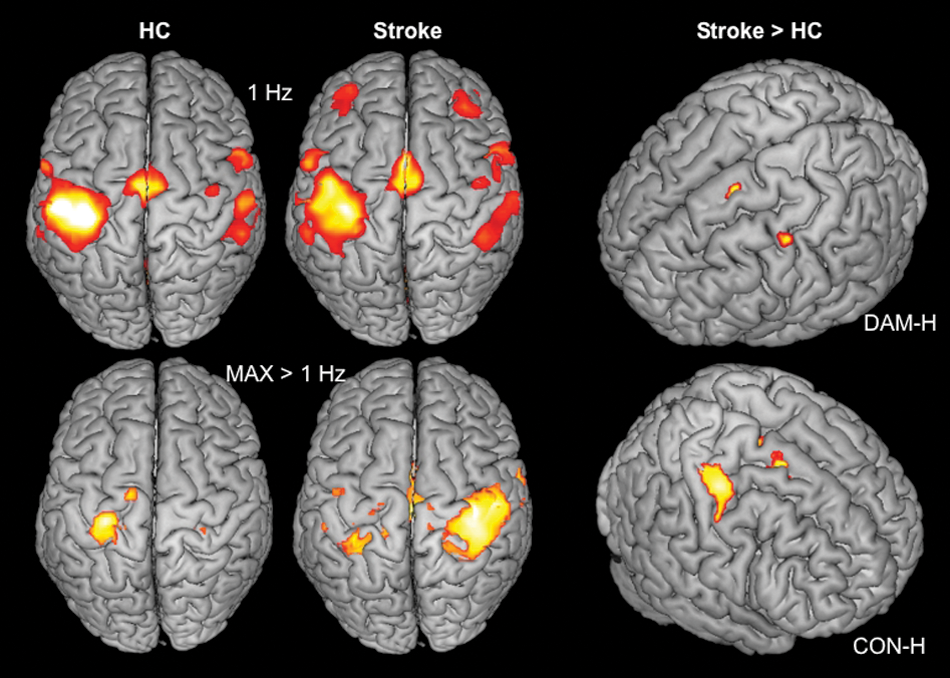
fMRI statistical parametric maps for within- (first column: HCs; second column stroke patients, stroke) and between-group effects (stroke > HC) for the fist clenching task: main effects (left row) were thresholded with P < .05 and FDR corrected; comparisons between groups (right column) were thresholded with P < .05 and FDR corrected for ROIs. Top row: active fist clenching at 1 Hz; patients showed increased activation in the inferior SMA, the medial cingulate gyrus, and PMC of the DAM-H. Bottom row: group contrast results for maximum > 1 Hz. Stroke patients showed increased activation in the SMA and the dPMC and M1 of the CON-H
Additionally, 24 age-matched healthy controls (HCs; 10 male/14 female: mean age = 59.5 ± 16.0 years; range = 28-67 years; all strongly right handed: score = 98.4 ± 5.0) without history of neurological or psychiatric disease participated in the diffusion tensor imaging (DTI) and the fMRI investigations only. Participants in both groups provided written informed consent, which was approved by the Ethics Committee of the Medical Faculty of the University of Greifswald.
Motor Test Battery
Patient motor performance was assessed using the MRC Scale, differentiated for finger, wrist, elbow, and shoulder; NIH Stroke Scale 16 ; and maximal hand grip force (Newgen medicals, Tokyo, Japan), assessed as the average value of 10 trials for each hand and the percentage of strength of the affected with respect to the unaffected hand. We also used the 9-Hole Peg Test (9HPT), which shows a high test–retest reproducibility, 17 with eyes closed to examine sensorimotor integration by determining the number of pegs positioned correctly in 15 s, averaged over 7 consecutive trials. The final test measured the accuracy of following a line of a figure with a pencil, adopted from the “Wiener Testsystem.” 18 Mirror movements were monitored with video control of both hands for fist clenching around a rubber ball with the individual maximal velocity and for the 9HPT. None of the patients showed mirror movements.
Motor Tasks During fMRI
All tasks were trained outside of the scanner to ensure proper performance. During scanning, participants were supine and wore hearing protection. Both patients (using the affected hand) and HCs (using the right dominant hand) performed fist clenching around a rubber ball. One movement frequency was paced at 1 Hz via a metronome. The other was performed at the participant’s maximal frequency. Performance frequency was counted in 4 blocks and averaged over time during scanning. The performance amplitude was monitored online by a pressure detector connected to an electro-optical biosignal recorder (Varioport-b, Becker Meditec, Karlsruhe, Germany). The signals were recorded and stored for further off-line analysis using PhysioMeter software. The force was adjusted to about 30% of the maximal force by visual training with the pressure device prior to measurement. In a separate task, passive wrist flexion–extension were elicited by a nonmagnetic torque motor at 1 Hz 19 to assess possible differences in representation maps without any voluntary movement or effort contribution. All conditions were randomized with respect to their order. These signals were presented via a video projection controlled by the presentation software (Neurobehavioral Systems, Albany, NY) and triggered by the scanner.
MRI Scanning Parameters
MRI data were collected using a 1.5-T MRI scanner (Siemens Symphony) that was additionally equipped with an 8-channel head coil. Field homogeneity was optimized prior to each session using a shimming sequence. As a structural data set, we recorded a T1-weighted volume (MPrage; TR, 2.3 s; TE, 3.93 ms; 175 sagittal slices; voxel size, 1 × 1 × 1 mm3). During the performance tasks, 75 volumes with 33 slices each (3-mm thick, 0.75-mm gap) were acquired in the transverse direction, parallel to the AC-PC line, using echo-planar images (TR, 3000 ms; TE, 50 ms; flip angle, 90°; voxel size, 3 × 3 × 3 mm3). Each block therefore lasted for 3.75 minutes; active and resting blocks alternated all 15 s. Additionally, we measured a DTI sequence on a 3-T MRI scanner (Siemens Verio, Erlangen, Germany) equipped with a 32-channel head coil. For this, we performed 3 single measurements of 30 directions, 55 slices of 1.8 mm thickness with a 0.5-mm gap; pixel size 1.8 × 1.8 mm2; TE, 105 ms; TR, 10 400 ms, summing up to a DTI-measuring time of 15 minutes.
Analyses of Functional Imaging
The first 2 volumes of each scan were ignored. Preprocessing and statistical parametric mapping was performed with SPM5 (Wellcome Department of Neuroscience, London, UK) and Matlab version 7.4 (MathWorks Inc; Natick, MA). Each time series was realigned and resliced after unwarping in the phase encoding direction (anterior/posterior) to account for movement and susceptibility artifacts and were high-pass filtered (128 s). The realigned data were spatially normalized to the Montreal Neurological Institute (MNI) template by using the coregistered and segmented T1 image as a reference and resliced to 3 × 3 × 3 mm3. The images for the 6 patients with right-hemisphere lesion were flipped in the midsagittal plane before normalization and smoothed with a Gaussian filter of 9 mm (full width at half maximum). At the first level of analysis, a fixed-effect analysis was performed to obtain contrast images for each condition. These were entered into a second-level random-effects analysis. The main effects of each condition were modeled separately, and differences between maximal minus 1 Hz active fist clenching were calculated with significance thresholds for multiple comparison correction over the whole brain (adjusted P < .05; false discovery rate [FDR 20 ]). Comparisons between groups (2-sample unpaired t test) were restricted to regions known to show increased activation in patients in a chronic phase after stroke (M1 and dorsal premotor cortex [dPMC] of the DAM-H and CON-H; the supplementary motor area [SMA] and medial cingulate cortex [MCC]; and the anterior cerebellar hemispheres). For the regions of interest (ROIs) analysis within these areas, a threshold of P < .05 (FDR corrected) was used. ROIs were selected using cytoarchitectural probability masks from Anatomy toolbox 21 for M1 (BA 4ap) and dPMC (lateral to x = 30), and SMA (BA6) and Automated Anatomical Labeling (AAL) 22 for the cerebellar hemisphere and MCC. Highest β values during performance of maximal frequent voluntary movement in M1 and dPMC were correlated for linear regression analyses with recruitment curve (RC) and DTI data.
Lesion Volumes
Lesion volumes were calculated by manually drawing the border of the lesion in the high-spatial-resolution T1-weighted image for each slice and calculating the resulting volume (mm3) with MRIcron (http://www.sph.sc.edu/comd/rorden/mricron).
Evaluation of DTI Data
Evaluation of the diffusion-weighted data was performed using JavaDTI (Domin, University of Greifswald, Greifswald, Germany), which uses the FACT algorithm for fiber tracking. 23 Three single diffusion measurements were averaged and interpolated to an isometric voxel size of 1 mm3. Rectangular ROIs (15 × 12 mm2) were placed manually 2 mm above the anterior commissural plane and 6 mm higher as a seed for counting the number of traces (NTs) passing through the posterior limb of the internal capsule (PLIC) presumed to be connected to the primary motor, premotor, and primary somatosensory cortices. 24 DTI tracking determined the NTs passing through the PLIC. Parameters for tracking termination were 0.35 for FA and 45° for the angle between 2 contiguous eigenvectors. Fibers traversing the ROIs in both directions were counted within each hemisphere. Fibers passing predominantly in the z-axis can be assumed to cross both ROIs as described by Zarei and colleagues. 24 We calculated proportional NTs as (NTDAM/NTCON) × 100 and the proportional FA as (FADAM/FACON) × 100 as described previously.10,13 Comparison with HCs was performed for the same number of dominant and nondominant hemispheres to avoid a bias for a higher amount of NTs and FA values in the dominant hemisphere. 25
TMS Parameters and Resting Motor Threshold (RMT)
Participants were seated comfortably on a reclining chair. Focal TMS was delivered to the optimal scalp position for activation of the first dorsal interosseus muscle using a figure-of-eight coil connected to a Magstim 200 magnetic stimulator (Magstim, Whitland, Dyfed, UK). The coil was placed tangentially to the scalp with the handle pointing backward and rotated away from the midline by approximately 45°. The current induced in the brain was posterior–anterior approximately perpendicular to the line of the central sulcus. 26 The position was marked on the scalp to ensure identical coil placement throughout the experiment. The RMT and RCs were used as measures of corticomotor excitability. The latency and amplitude of the M- and F-waves were used as measures of α motoneuron excitability. MEPs were recorded from silver chloride surface electrodes overlying the first dorsal interosseus muscle of each hand. Relaxation was monitored by continuous visual feedback of the EMG signal amplified to 500 times. After amplification and bandpass filtering (20 to 500 Hz; CED 1902 Signal Conditioner, Cambridge Electronic Design, Cambridge, UK) the EMG signal was digitized at 1 kHz (CED micro 1401 mkII, CED) and stored on a laboratory computer for off-line analysis (Signal, CED). The RMT for each hand was defined as the minimum stimulus intensity that produced MEPs > 50 µV in at least 5 of 10 consecutive trials. 27 RCs were derived from the MEP amplitude obtained at 90%, 110%, 130%, and 150% of RMTs, from 10 stimuli per intensity. The MEP amplitude was measured peak to peak from single trials and subsequently averaged off-line. M-waves were elicited using supramaximal electrical stimulation of the ulnar nerve at the wrist. Individual trials were examined off-line, and any traces showing voluntary EMG activity were discarded. MEP amplitudes for the RC were normalized to M-wave amplitude for each muscle. 7 The slope of RC was determined from the line of best fit using least squares. The ratio of slope of the affected hand relative to the unaffected hand was determined for linear regression analysis with BOLD signal magnitude. Pearson partial correlations were calculated using SPSS (Statistical Package for the Social Sciences; PASW-Statistics; Version 17.0) for strength of the affected hand, ratio of slope of the affected hand relative to the unaffected hand, FA proportion, proportion of NTs, and β-weights from f MRI contrasts and corrected for age and time since stroke. We did not correct for multiple comparisons for significance thresholds of hypothesis-driven correlations based on previously reported observations (strength and TMS recruitment 7 ; strength and fMRI magnitude for conditions normalized to the individual maximal performance 4 ; and FA and complex motor performance 10 ). For correlations without prior observations (proportion of NTs and fMRI activation in M1 and dPMC of both hemispheres; TMS parameters of motor recruitment), we corrected for multiple comparisons using the modified Hochberg correction. 28 Partial correlation analyses were undertaken to control for possible confounding factors of age and time since stroke.
Results
Clinical and Behavioral Measures
All patients experienced almost complete recovery of motor function, with median scores of 1 according to the NIH Stroke Scale 29 and 5 according to the Medical Research Council Scale, indicating normal upper-limb function.
Age did not differ between patients and HCs (t36 = 0.30; NS). On average, patients had modest impairment of paretic hand grip strength (affected hand, 31.7 ± 8.5 kg; unaffected hand, 34.7 ± 9.4 kg; t13 = 2.13; P = .028; 1-tailed), indicating an excellent clinical recovery of strength. For more complex movement performance (precision grip), patients performed significantly worse than HCs (9HPT: average, 2.73 pegs for patients and 3.24 pegs for HCs; t36 = 4.24; P < .001; velocity to follow a line: average, 1.74 cm/s for patients and 2.35 cm/s for HCs; t36 = 3.53; P < .001). Overall, patients exhibited decreased motor performance with the paretic hand, especially evident during complex motor tasks.
Diffusion-Weighted and Functional MRI
DTI measurements revealed a proportional FA decrease of the DAM-H in patients (patients, 97.30% ± 4.41%; HCs, 100.85% ± 3.53%; t28 = 2.53; P < .05). There was a positive correlation between FA proportion and performance of the 9HPT (r = 0.55; P < .05) that was no more significant when controlling for age (r = 0.40; NS).
Performance during fMRI scanning was comparable between patients and HCs (maximal frequency of fist clen-ching: patients, 2.04 ± 0.93 Hz; HCs, 2.34 ± 0.88 Hz; t28 = 0.24; NS; force difference between patients and HCs, t16 = 0.35; NS).
Patients showed an increase in activation during 1-Hz fist clenching in the MCC, compared with HCs (t = 3.98; peak of activation 18, −27, 45), the SMA, and the dPMC of the CON-H (Table 2; Figure 1, top). The condition with individual maximal velocity showed no significant differences between groups but a trend for an increase for the patients in the SMA (t = 3.78; 0, 6, 48; FDR correction failed). The increase of activation for maximal compared with 1-Hz voluntary fist clenching was larger for the stroke patients than for HCs in the primary motor cortex (M1), the dPMC, and the SMA of the CON-H (Table 2; Figure 1, bottom). Activation maps during passive movements did not reveal significant differences between participant groups.
Comparison of the Statistical Parametric Mapping Results Between Participant Groups (P < .05; FDR Corrected)
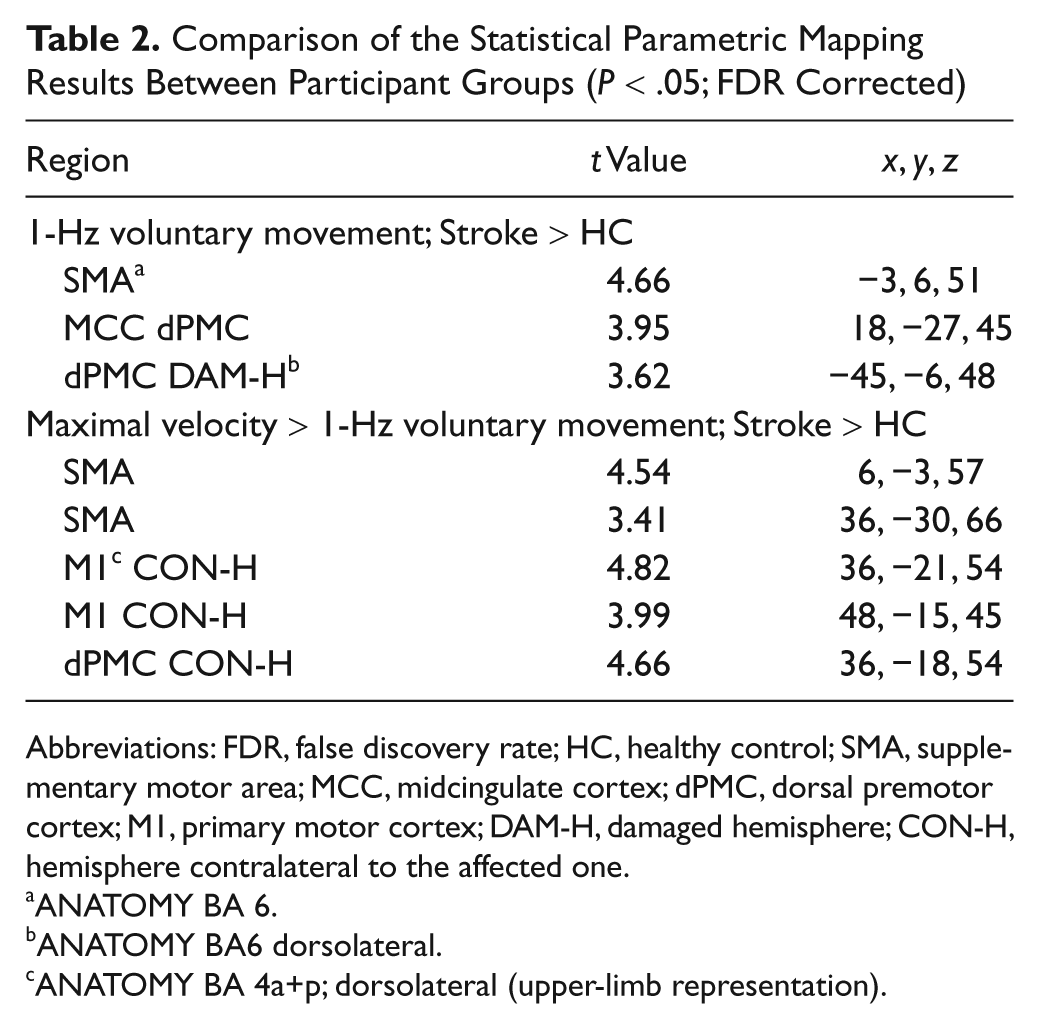
Abbreviations: FDR, false discovery rate; HC, healthy control; SMA, supplementary motor area; MCC, midcingulate cortex; dPMC, dorsal premotor cortex; M1, primary motor cortex; DAM-H, damaged hemisphere; CON-H, hemisphere contralateral to the affected one.
ANATOMY BA 6.
ANATOMY BA6 dorsolateral.
ANATOMY BA 4a+p; dorsolateral (upper-limb representation).
fMRI activation in the dPMC of the CON-H (r = −0.67; P c < .05) correlated negatively with the proportion of NTs (Figure 2C) and was not associated with age or time since stroke. Also, functional activation intensity in CON-M1, DAM-M1, and DAM-dPMC during maximal frequent movements with the affected hand was negatively correlated with the affected hand grip force. Complete linear regression statistics are shown in Table 3.
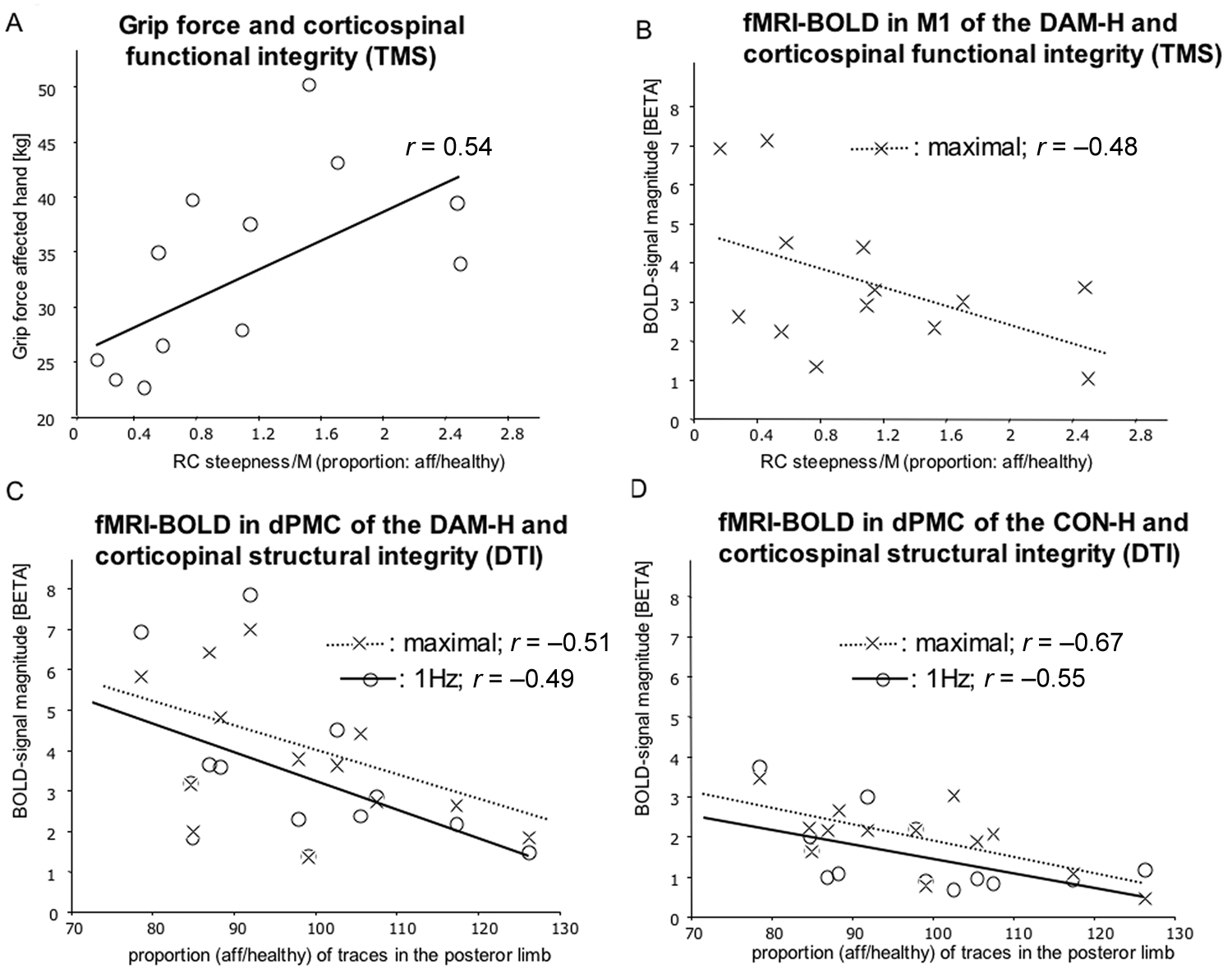
Regression analyses: A. The grip force of the affected hand correlated positively with corticospinal tract integrity (TMS; affected vs the unaffected hand) but was not significant after accounting for age. B. fMRI BOLD signal magnitude in M1 of the DAM-H during maximal voluntary movements correlated negatively with RC slope (TMS) of the affected hand but was not significant after accounting for age. fMRI BOLD signal magnitude in the dPMC of the DAM-H (C) and CON-H (D) during maximal frequent voluntary movements correlated negatively with the proportion of traces of the affected versus the unaffected hemisphere
Partial Correlation Between Motor Recruitment, fMRI Activation, and Grip Strength and Structural Integrity of the Corticospinal Tract After Accounting for Age and Time Since Stroke
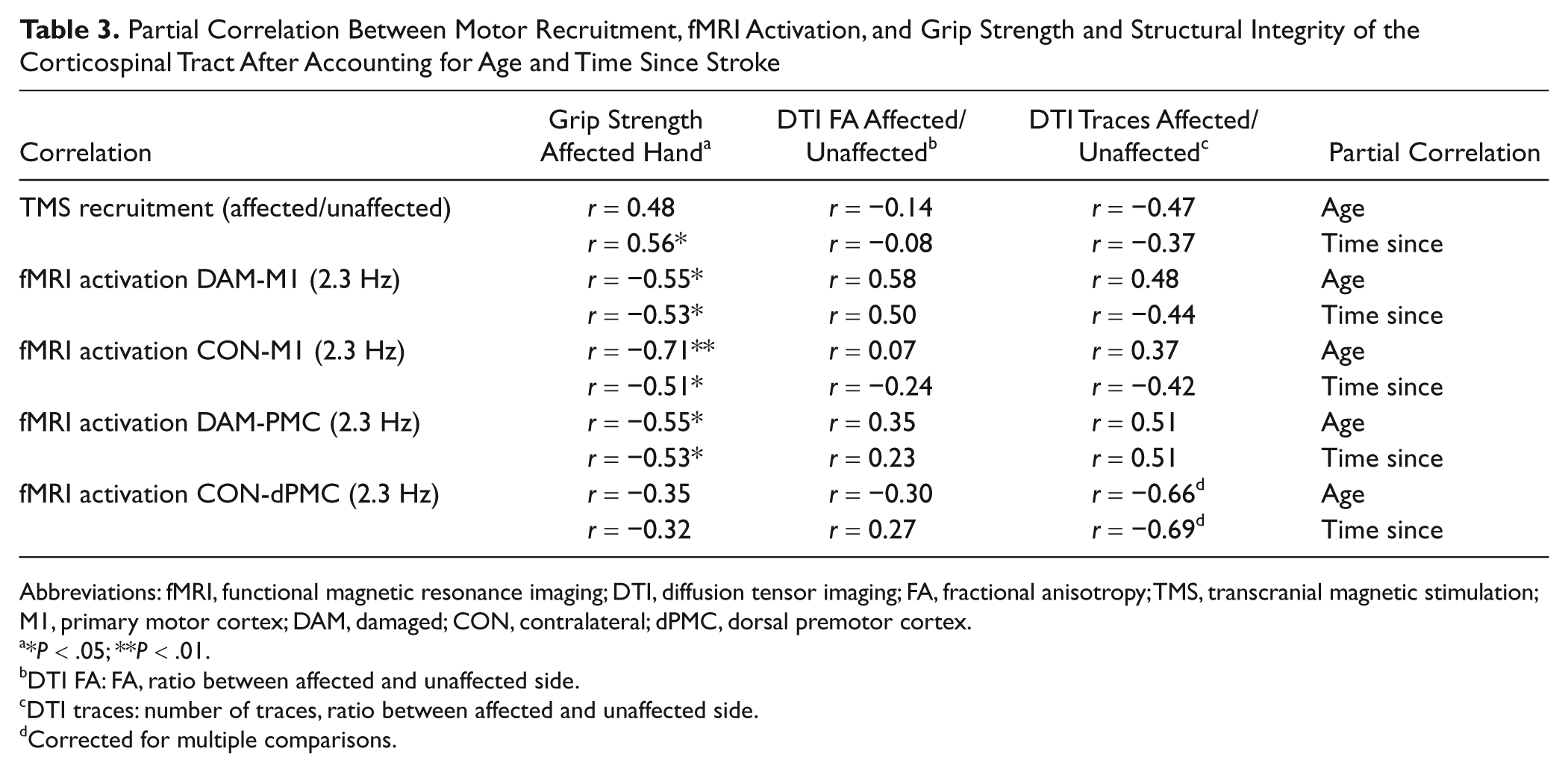
Abbreviations: fMRI, functional magnetic resonance imaging; DTI, diffusion tensor imaging; FA, fractional anisotropy; TMS, transcranial magnetic stimulation; M1, primary motor cortex; DAM, damaged; CON, contralateral; dPMC, dorsal premotor cortex.
*P < .05; **P < .01.
DTI FA: FA, ratio between affected and unaffected side.
DTI traces: number of traces, ratio between affected and unaffected side.
Corrected for multiple comparisons.
Neurophysiological Variables
One patient did not tolerate TMS RCs, and these analyses were limited to 13 patients. Neurophysiological measures (RMT, slope of RC, M-wave; see Supplementary Table 1) between the affected and the unaffected hand did not differ significantly. The proportion of RC-slope/M in the affected versus the unaffected hemisphere was positively related to the grip force of the affected hand (r = 0.54; P < .05; Figure 2A); however, the correlation was no more significant when performing a partial correlation with the variable age (r = 0.48; NS) but was not associated with time after stroke (r = −0.56; P < .05). We observed a positive correlation of FA proportion with sensorimotor performance (9HPT: r = 0.55; P < .05). This association was also dependent on age and not significant when performing a partial correlation with the variable age (r = 0.40; NS). Corticospinal integrity (TMS; RC slope) and fMRI activation in M1 of the DAM-H during affected hand movement correlated negatively (r = −0.48; P < .05; Figure 2B) but was not significant when accounting for age (r = −0.43; NS).
Discussion
In this novel investigation of well-recovered patients with focal subcortical damage, we observed only slight fMRI activation increases during motor tasks compared with HCs. In accordance with previous studies,4,6,30 we found increased activation in the dPMC of the DAM-H and the SMA/MCC, even during performance of low-frequency paced voluntary hand movements. More interestingly, however, an activation increase for maximal frequency movements was observed only in the CON-H as indicated by a significant negative correlation between activation in the contralesional dPMC and ipsilesional corticospinal tract integrity by diffusion-weighted MRI. This finding underscores the potential importance of contralesional dPMC for more demanding motor performance even in well-recovered patients with minimal damage.
Patients who had a lower proportion of NTs showed especially high dPMC activation in both hemispheres during the most demanding active motor task. This finding was independent of age. This observation points to the importance of both ipsilesional and contralesional dPMC for recovery of motor function, especially with damage to the pyramidal tract from a subcortical lesion. Finally, maximal grip force in the affected hand correlated negatively with fMRI activation in CON-M1 and DAM-dPMC pointing to possible insufficient recovery mechanisms in these areas. 4
Correlates of Motor Recruitment May Reflect Age not Function
Associations with TMS-based measures may have been related to age more than lesion characteristics. As observed previously, 7 grip force correlated negatively with motor recruitment evident from RC slopes, but this association was predominantly mediated by age. Talelli and colleagues 31 found a negative correlation between age and the area under the RC, supporting the current finding that RC slope varied predominantly as a function of age. In concordance with others, 32 there was no difference in RMT and the RC slope between affected and unaffected sides for these well-recovered chronic patients. However, the RC slope/M-wave was especially low for those patients who showed poorer motor outcomes, supporting previous observations of correlations with motor recruitment and maximal grip force 7 and correlations of an increase in RC amplitude in the subacute period after stroke with good outcome after rehabilitative therapy. 33 The present findings align well with a previous study showing an inverse correlation between TMS measures of functional integrity of the corticospinal pathway and magnitude of BOLD activation in M1 of the DAM-H, 7 but again, the association was dependent on age. Overall, the TMS parameters of motor recruitment for these well-recovered patients related mostly to age.
fMRI Activation Maps
Overall, there was increased fMRI activation in the dPMC of the DAM-H and the SMA together with the MCC for the voluntary movements. Differences in fMRI activation between lesioned and nonlesioned hemispheres were lower than previously described for affected hand movements in the chronic phase of stroke.6,30,34,35 This is likely because of the excellent motor recovery of the patients selected. Similar findings have been described previously.36,37 The lack of differences between groups during passive movement may also be explained by the amount of recovery of patients in the present study compared with differences observed between HCs and more impaired patients. 38
The increase of dPMC activation during active movement of the affected hand seems to be a robust parameter for altered functional activation in patients after motor stroke.30,34,39 Longitudinal studies demonstrated correlations between improved motor performance and increased dPMC activation in the DAM-H.40-42 It is interesting to note that our patients not only showed increased recruitment of M1 and the dPMC of the CON-H but also increased SMA and MCC activation, and increased reliance on the nonaffected hemisphere has been demonstrated previously. 26 Several studies point to the importance of M1 activation of the CON-H as a poor prognostic sign for motor outcome following motor training. 43 Recent electrophysiological 30 and fMRI findings 44 suggest increased effective connectivity of areas of the CON-H with the dPMC of the DAM-H in patients after subcortical stroke in order to facilitate movement of the recovered hand. In particular, the dPMC of DAM-H 45 and CON-H 46 can have functional significance for the performance of simple hand movements for patients with partial recovery after stroke. The dPMC has direct connection to the corticospinal tract. 47 Even after excellent restitution, an increase of dPMC activation seems to be associated with damage in the PLIC as indicated by negative correlations between the NTs of the DAM-H and dPMC activity.
Increased activation in the SMA during active movements has been described previously in chronic patients suffering from subcortical stroke. 42 The SMA is connected bilaterally and has direct connections to the spinal motor neurons, particularly those innervating the fingers and the wrist. 48 Our data confirm previous reports that both SMA and MCC may be important for restoring motor function after a lesion of the pyramidal tract. 49
Relating DTI and TMS-Based Measures of Corticospinal Tract Integrity
The DTI parameters of proportional NTs and proportional FA did not correlate with TMS measures of motor recruitment. TMS measures of motor recruitment reflect functional corticospinal tract projections originating from M1, modulating especially strength and speed of motor control. Conversely, DTI measures reflect white matter integrity of pathways passing through the PLIC, which include pathways from M1 as well as more anterior frontal regions. 47 Newton and colleagues found that more anterior traces in the internal capsule are connected with cortical areas of the dPMC and the SMA, whereas more posterior traces originate in M1. 50 Additionally, traces following the corticobulbar and the corticocerebellar tract pass the PLIC and might therefore contribute to the lack of association between the TMS and the DTI parameters. Indeed, associations between these measures and behavioral measures mirror this distinction. Whereas the TMS parameters of motor recruitment were correlated with grip strength of the affected hand, DTI measurements correlated with a measure of performance for complex motor tasks with higher affordances for sensorimotor integration (precision grip task). This notion is supported by the fact that very-well-recovered patients show behavioral deficits in more complex sensorimotor integration tasks,51,52 which, in addition to M1, necessitate greater incorporation of other parts of the motor network.
It is worth noting that all patients in the present study had observable MEPs from TMS, and their FA asymmetry range was between 0.008 and 0.06. Therefore, all were within range of good potential for recovery according to the criteria of Stinear et al. 10 Indeed, motor outcome was excellent. Although these patients exhibited a predominantly contralateral control of motor function of the affected limb as predicted, 10 they also exhibited an increase of ipsilateral dPMC activation during voluntary hand movement with maximal frequency, and this increase in activation was associated with a decrease of traces in the affected PLIC. Therefore, activation indices based on lateralization of activity alone are insensitive to such reorganization. Indeed, it has been suggested that while lateralization of activations may be sensitive to current upper-limb function, they may not be salient predictors of motor recovery. 7
Study Limitations
Some limitations of the study have to be mentioned. First, to balance performance between the patient and the control group, patients were selected who were able to perform the motor tasks investigated in a manner comparable to that of age-matched HCs. This homogeneity of patients with respect to performance weakens the correlation analysis. The same holds true for the location of the subcortical lesion: The lesions observed in the patients selected were not restricted to the internal capsule but also included damage of the basal ganglia and other subcortical structures (see Supplementary Figure 1). However, the homogeneity of lesion locations in the present study was comparable to that found by others investigating motor recovery in the chronic phase after stroke in the region of the internal capsule. 7 Second, this study focuses on differences between chronic stroke patients and HCs. It was not designed to allow comparisons between movements of the intact and the affected hand. Third, measures of force of the unaffected hand were not obtained and could not be modeled as nuisance events in the fMRI analysis. However, motor recovery was very good in our patients, and associated movements were excluded by visual inspection and video monitoring of both hands during all motor tasks. Fourth, patients were examined at different time frames. All patients recovered after this time, but compensatory functional activation might differ with respect to time after the damage has occurred. 53 Fifth, the modeling of different frequencies of movement performance in a block design can be problematic. 48 For future studies, use of an individual maximal frequency and modeling each movement as a single event may be warranted. Finally, there is limited predictive power in the current cross-sectional study. We specifically sought well-recovered patients at the chronic stage to explore the potential association between corticospinal tract damage and activation in nonprimary motor cortical areas. Further longitudinal studies might examine how these cortical reorganization profiles evolve from the subacute to the acute stage.53,54
In conclusion, negative correlations between TMS measurements of motor recruitment, grip force, and M1 activation in the DAM-H indicate compensation for decreased corticospinal integrity at the chronic stage after subcortical stroke. Although TMS parameters of motor recruitment were associated with patient age, correlates between dPMC activation and the proportional NTs, or dPMC activation in the DAM-H and hand grip force were independent of age. This might have implications for the specificity of these parameters for stroke-related changes associated with decreased motor performance and may offer potential prognostic utility for predicting the upper-limb recovery potential of patients at the subacute stage.
Footnotes
Acknowledgements
We thank B. Sehm for help with the selection of patients. This study was supported by the German Research Association (DFG; LO 795/7).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the German Research Association (DFG; LO 795/7).