
Abstract
Background. Objective measures of functional walking remain scarce for individuals with incomplete spinal cord injury (ISCI). Hence, the authors developed the Spinal Cord Injury Functional Ambulation Profile (SCI-FAP), which encompasses the timed performance of 7 tasks, such as walking and negotiating obstacles, doors, and stairs. Objective. To assess the reliability and validity of the SCI-FAP. Methods. A total of 32 individuals with ISCI attended 2 testing sessions separated by 1 to 2 weeks. At the first session, participants performed the SCI-FAP, the 10-m walk test (10MW), the 6-minute walk test (6MW), and the Walking Index for Spinal Cord Injury (WISCI II); 3 raters scored the participants’ performances on the SCI-FAP to assess interrater reliability. To establish convergent validity, SCI-FAP scores were compared with scores on the 10MW, 6MW, and WISCI II. At the second session, participants completed the SCI-FAP to assess test-retest reliability. To establish discriminative validity, SCI-FAP scores were compared between participants with ISCI and 60 able-bodied adults, who were scored on the SCI-FAP in a single session. Results. Internal consistency (α = .95), interrater reliability (intraclass correlation coefficient [ICC] = 1.00), and test-retest reliability (ICC = 0.98) of the SCI-FAP were high. SCI-FAP scores were moderately correlated with results from the 10MW (r = −0.59), 6MW (r = −0.59), and WISCI II (M = −0.68). Performance on the SCI-FAP was significantly poorer among participants with ISCI compared with their able-bodied counterparts (P = .002). Conclusions. The findings support the SCI-FAP as a valid and reliable measure of walking skill for individuals with ISCI.
Introduction
Regaining the ability to walk is important for individuals who have experienced an injury to the central nervous system. 1,2 More than half of individuals who sustain an incomplete spinal cord injury (ISCI) regain some walking ability. 3,4 Objective and comprehensive measures of walking are extremely important for quantifying the effect of gait interventions.
Currently, the 10-meter walk test (10MW) and the Walking Index for Spinal Cord Injury II (WISCI II) are considered the most useful measures of walking for individuals with ISCI. 5 Although these measures provide valuable information concerning walking speed and general walking function, respectively, they assess walking over smooth, level ground only. Measures of more challenging walking tasks have been developed, such as the Dynamic Gait Index, 6 Rivermead Mobility Index, 7 and several obstacle courses. 8-11 These measures, however, lack assessment of many of the tasks frequently encountered in daily walking, 12 and most include subjectivity in the scoring.
Functional walking involves the ability to walk on different surfaces (smooth, rough, uneven, sloped), carry objects, negotiate doors and obstacles, and ascend/descend curbs and stairs. 12 The most objective measure of functional walking is the Modified Emory Functional Ambulation Profile (mEFAP), which is a timed measure that quantifies mobility in stroke survivors. 13,14 Of the tasks comprising the mEFAP, 4 have been identified as walking tasks frequently encountered by able-bodied adults (walking on smooth and carpeted surfaces, negotiating obstacles and steps). 12 The fifth task, the Timed Up and Go, is generally regarded as a critical transition task needed for walking. 6 The scoring accounts for the devices, braces, and physical assistance needed to complete each task. It has excellent reliability and concurrent validity and is sensitive to change, 14 but it lacks several frequently encountered walking tasks. 12 To fill this gap, we modified the mEFAP, based on our earlier study 12 to create the Spinal Cord Injury Functional Ambulation Profile (SCI-FAP) (appendix), a measure of functional walking that assesses function at the activity level according to the International Classification of Functioning. 15
The objectives of the present study were to (1) develop a measure of functional walking for ISCI (the SCI-FAP), (2) assess the interrater and test-retest reliability of the SCI-FAP in individuals with ISCI, (3) evaluate the discriminative validity of the SCI-FAP by comparing performance on the measure between individuals with ISCI and age- and gender-matched, able-bodied adults, and (4) assess the SCI-FAP’s convergent validity by comparing, within the ISCI-group, the results obtained on the SCI-FAP, the 10MW, the 6-minute walk test (6MW), and the WISCI II.
Methods
SCI-FAP Development
A small focus group developed the first version of the SCI-FAP, based on the mEFAP and 5 additional tasks known to be commonly encountered in daily walking. 2,12,16 The devices, braces, and physical assistance categories used in the mEFAP were retained, with slight modifications (eg, forearm crutches were added). This first version was tested on 2 individuals with ISCI. Based on their feedback and that of therapists who work with patients with ISCI, a second version was developed containing 9 tasks (5 from mEFAP and 4 new ones—walking while carrying a bag, negotiating a ramp, stepping up and down 1 step, and walking through a door).
The second version of the SCI-FAP was sent to 10 recognized experts in the area of SCI rehabilitation. Feedback was received from 6 of these experts. Overall they were positive about the new measure, stating that it included important walking skills, thus, supporting content validity. The grading of devices/braces and assistance level was identified as a problem. There was no rationale for the ordering of devices/braces. Moreover, selecting an assistance level was subjective. As a result, we simplified the rating of devices/assistance (henceforth abbreviated to assistance; see appendix available online) and had 12 physical therapists rank the assistance from greatest to least independence. Eleven of the 12 therapists ranked the levels in the order shown in the appendix.
The final revision was made after the data were obtained; 2 tasks (walking on smooth floor and on a ramp) were removed to reduce redundancy (see below). Thus, the current version of the SCI-FAP includes 7 tasks (appendix).
Scoring of the SCI-FAP
Scoring of the SCI-FAP is based on the time it takes a participant to complete each task at a comfortable walking pace and a multiplication factor to quantify the assistance needed for each task (appendix, “assistance”). The largest assistance level is given when a participant is “unable to complete” a task. This includes situations where participants cannot attempt the task and situations where they complete part of the task but are unable to finish.
Maximum times for each task, set at 50 times the mean from able-bodied participants, have been established to allow scoring of individuals who cannot complete a task (appendix). Fifty was chosen because the 2 lowest-functioning participants with ISCI who could complete all tasks took 10 to 50 times longer than the able-bodied participants. Participants who complete a task but take longer than the maximum time are assigned the maximum time for that task multiplied by the factor that reflects the assistance used. Participants who do not attempt or complete a task are assigned the maximum time for that task multiplied by a factor of 6 (ie, unable to complete).
To avoid the problem of one or more tasks dominating the scores because they take longer to complete or are more difficult, we normalized the scores by the mean able-bodied time for each task (appendix). Thus, the score for each task is as follows:

Because the SCI-FAP is a timed measure, a low score reflects better function. The highest total score on the SCI-FAP is 2100, composed of 300 for each task (ie, normalized score of 50 × 6).
Participants
Participants with ISCI were recruited from the University of Alberta (UA) and the University of British Columbia (UBC). To be included, they had to satisfy the following conditions: (1) at least 6 months postinjury; (2) able to walk at least 5 m with or without physical assistance of another person and/or walking aids; (3) free of any disease, injury, or condition other than their ISCI that affected walking ability; (4) not receiving rehabilitation services that included walking practice; (5) no change in medications that affect walking ability during the study; and (6) able to follow spoken commands in English.
Able-bodied participants, older than 18 years of age, were recruited at UA. To be included, able-bodied individuals must have (1) had ≤1 fall in the previous month (to exclude individuals with undiagnosed pathology in equilibrium); (2) been free of any disease, injury, condition, or medication that affected walking ability; and (3) been able to follow spoken commands in English. Written informed consent was obtained from all participants prior to participation in the study. Ethical approval was received from the Capital Health and UA Health Research Ethics Board and the UBC Clinical Research Ethics Board.
Study Design
Participants with ISCI
Most participants with ISCI were tested at UA. These individuals attended 2 testing sessions. At session 1, participants completed the SCI-FAP, 10MW, 6MW, and WISCI II. At session 2, only the SCI-FAP was completed. The SCI-FAP tasks were performed in the same order on both days and across participants so that the testing conditions were consistent for the evaluation of test-retest reliability. The order was as follows: carpet, floor, up & go, obstacles, stairs, carry, step, ramp, and door. The 6MW, a measure of walking endurance, 17 was performed on a 25-m walkway. The score is the total distance (in meters) traveled in 6 minutes. The 10MW, a measure of comfortable walking speed, was performed over a 15-m walkway, with the middle 10 m timed. The WISCI II is a 21-point ordinal scale that rates an individual’s ability to walk 10 m based on the braces, devices, and assistance needed. 18 Self-selected and maximal WISCI II ratings were assessed. 19 The 10MW, 6MW, and WISCI II are valid and reliable measures for individuals with ISCI. 20,21
The SCI-FAP was assessed first, followed by the remaining 3 tests in a random order. The SCI-FAP was administered first to ensure the same testing conditions in sessions 1 and 2. The sessions were spaced 1 to 2 weeks apart to reduce the chance of practice effects and were scheduled at the same time of day for each participant. Three raters (authors KM, JY, KB) scored each participant simultaneously on the SCI-FAP at session 1. Each rater used a silent stopwatch and recorded the time to 1/10 of a second. All raters were trained as physical therapists, with 2 currently licensed (KM and KB). One rater, designated the lead rater (KM), provided verbal instructions to all participants. Only the lead rater scored the 6MW, 10MW, and WISCI II, and attended session 2.
For 5 participants with ISCI, the SCI-FAP was scored by a total of 5 raters (the 3 raters mentioned above plus 2 additional physical therapists) at session 1. This determined the interrater reliability beyond the original 3 raters, who were very familiar with the measure as they were involved in its development. The 2 additional therapists, unfamiliar with the SCI-FAP, spent ~15 minutes reviewing the instructions and scoring with the lead rater prior to testing.
Some participants with ISCI were tested at UBC. These participants attended 1 testing session where they completed the 6MW, 10MW, SCI-FAP, and WISCI II, in that order. One rater scored their performance on all measures. The SCI-FAP tasks were administered in the same order outlined above for the UA site. All equipment used for the SCI-FAP was identical in dimension to the equipment used at UA. The 6MW was tested on 1 of 2 circular loops that were 41.1 m and 51.8 m in circumference. The assessment of comfortable walking speed (ie, 10MW) was the same as that described above. The data from these individuals contributed to the assessment of validity (ie, discriminative and convergent).
Able-bodied participants
Data were collected from able-bodied adults in order to establish normative scores for the SCI-FAP and to assess its discriminative validity. Able-bodied adults attended 1 testing session at UA to complete the SCI-FAP. The lead rater administered the test to 23 of the able-bodied participants. A physical therapy student trained in administering the SCI-FAP assessed the remaining 37 participants. The student was trained by one of the authors, and pilot data were collected to ensure that the scoring was comparable.
Analysis
Mean values are reported with ±1 standard deviation. Significance was set at .05 for all statistical tests.
Able-bodied data
To determine whether performance on the SCI-FAP changed with age, SCI-FAP scores (total and task scores) were compared for 5 decades (20-29 years, 30-39 years, 40-49 years, 50-59 years, and 60-69 years). A 1-way ANOVA with the Bonferroni correction for post hoc analyses was used for this analysis.
Homogeneity
An exploratory factor analysis was performed to assess the dimensionality of the SCI-FAP. Intertask correlations and task–total correlations (ie, correlation of task A with total score minus task A) were performed using Pearson correlation coefficient (r). A total of 9 SCI-FAP tasks were included in these analyses. For the remaining analyses described below, 2 tasks (floor and ramp) were removed from the total SCI-FAP score based on the intertask correlations (see Results section). Cronbach α was used to assess internal consistency. A moderately high α (ie, .95 > α > .7) was desired because this indicates good internal consistency without much redundancy. 22 SCI-FAP scores used from the UA participants were those measured by the lead rater at session 1.
Interrater reliability
SCI-FAP scores from the 3 original raters at session 1 were used to assess interrater reliability (ie, data from UA only). A 2-way random effects intraclass correlation coefficient (ICC) for absolute agreement was used. 22,23 ICC values were calculated for the total SCI-FAP score as well as individual task scores to determine if all tasks had similar reliability. For the 5 participants whose SCI-FAP performance was assessed by 5 raters, interrater reliability was also calculated using the total scores of the lead rater and the 2 additional raters.
Test-retest reliability
SCI-FAP scores assigned by the lead rater at sessions 1 and 2 were used to assess test-retest reliability (ie, data from UA only). Two participants did not return for session 2, so a total of 22 participants were included in this analysis. A 1-way random effects ICC for absolute agreement was used. 22,23 ICCs were calculated for the total SCI-FAP score and each task score.
Discriminative validity
Each participant with ISCI was age matched (±5 years) and gender matched to an able-bodied subject. Total SCI-FAP scores, as well as scores on each task, were compared between the 2 groups using a 1-tailed, independent t test. For participants with ISCI tested at UA, SCI-FAP scores measured by the lead rater at session 1 were used.
Convergent validity
Performance on the SCI-FAP (ie, total score) was correlated with performance on the 10MW and 6MW using Pearson correlation coefficient (r) for all participants with ISCI. SCI-FAP scores were correlated with self-selected and maximal WISCI II scores using Jaspen coefficient of multiserial correlation (M), which is appropriate when correlating ordinal and interval scales. 24 For UA participants, SCI-FAP scores measured by the lead rater at session 1 were used.
Results
Participants
A total of 32 individuals with ISCI participated (24 males; age = 47.6 ± 14.2 years; age range = 20-81 years); 8 were tested at UBC. All participants were community dwelling but varied greatly with respect to injury and walking ability (Table 1 25 ); 60 able-bodied adults participated (34 males; age = 42.9 ± 16.0 years; age range = 23-88 years). The age categories and number of participants (in brackets) were as follows: 20 to 29 years (16), 30 to 39 years (13), 40 to 49 years (9), 50 to 59 years (12), 60 to 69 years (6), 70 to 79 years (3), and 80 to 89 years (1).
Characteristics of Participants With ISCI
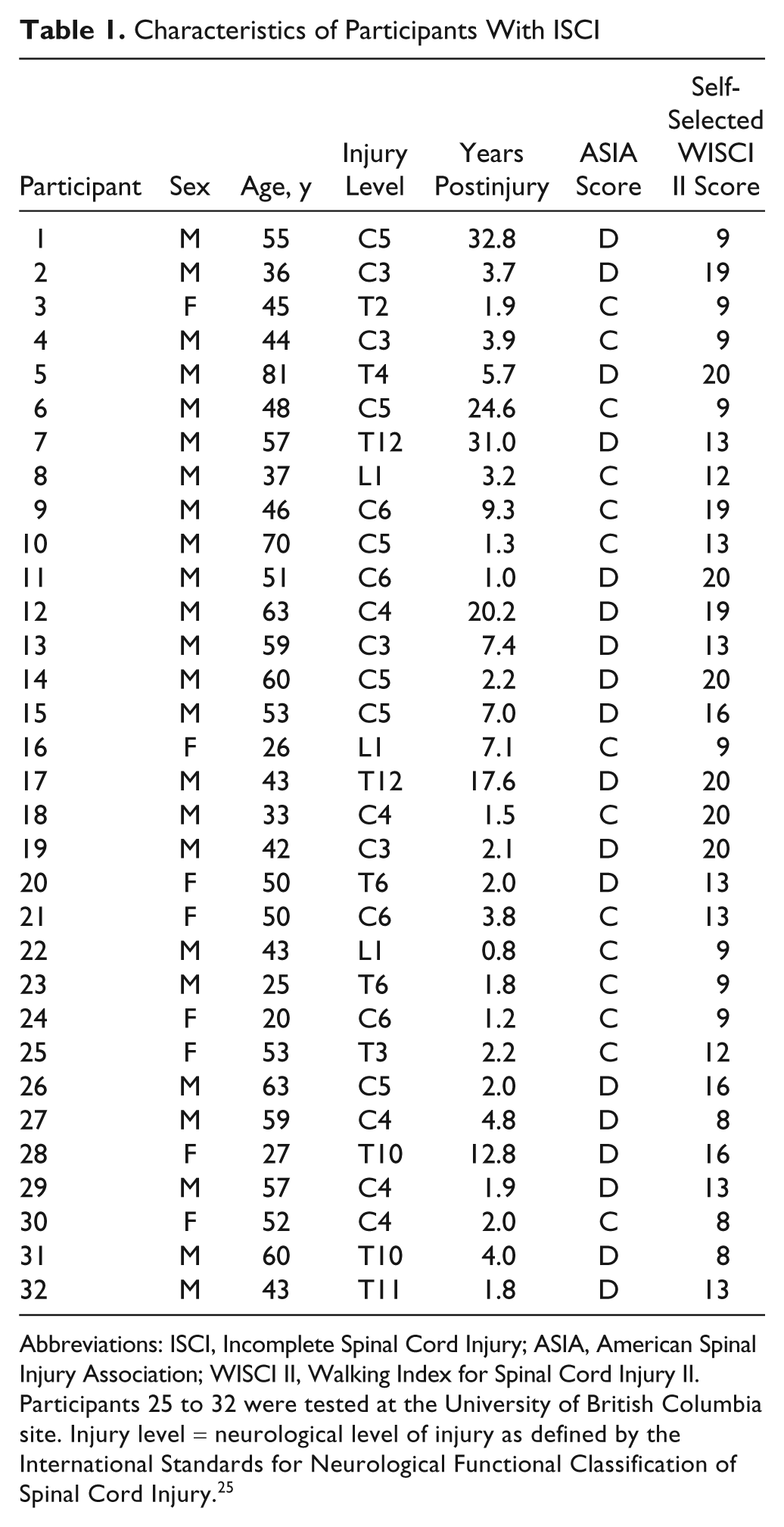
Abbreviations: ISCI, Incomplete Spinal Cord Injury; ASIA, American Spinal Injury Association; WISCI II, Walking Index for Spinal Cord Injury II.
Participants 25 to 32 were tested at the University of British Columbia site. Injury level = neurological level of injury as defined by the International Standards for Neurological Functional Classification of Spinal Cord Injury. 25
SCI-FAP Performance by Able-Bodied Participants
All able-bodied participants completed the SCI-FAP without assistance. SCI-FAP tasks (mean time) were as follows: floor (4.4 + 0.6 s); carpet (4.4 + 0.6 s); up & go (9.1 + 1.2 s); obstacles (11.4 + 1.3 s); stairs (6.2 + 0.8 s); carry (4.4 + 0.5 s); step (3.7 + 0.5 s); ramp (6.2 + 1.0 s); door (5.0 + 0.7 s). These mean times are used to normalize the task scores (see Equation 1). There was no difference in the total SCI-FAP score or task scores across ages (ie, 20-69 years), with the exception of the up & go task (P = .031). For this task, participants in their 20s scored significantly lower (ie, performed the task faster) than participants in their 50s.
SCI-FAP Performance by Participants With ISCI
A total of 29 of the 32 participants with ISCI were able to complete all SCI-FAP tasks. Participants 27, 30, and 31 did not complete all tasks—see Table 1. The tasks (number of participants that did not complete in parentheses) were as follows: obstacles (2), stairs (3), carry (1), step (3), ramp (3), and door (3). In all, 15 participants hit ≥1 obstacle at either the first or second session, resulting in a penalty of 1 factor (see “obstacles” in the appendix). Two participants (6 and 30) exceeded the maximum time on some tasks (including step, carpet, up & go). The SCI-FAP took 15 to 45 minutes to complete.
Homogeneity and Redundancy of the SCI-FAP Tasks
The factor analysis revealed all 9 tasks loaded strongly onto a single factor (right column Table 2; accounted for 86.4% of the variance). Intertask correlations ranged from 0.63 to 0.99 (P < .001; Table 2). Very high intertask correlations (ie, r = 0.99) were found for 3 groups of tasks: (1) the floor, carpet, and carry; (2) the up & go and obstacles; and (3) the stairs, ramp, and door (Table 2, asterisks). The task-total correlations ranged from 0.82 to 0.95 (P < .001; Table 2). Two tasks with very high correlations were removed. First, the floor task in the first grouping was removed because walking on a smooth surface is a component of other SCI-FAP tasks. Because the task-total correlations for carpet and carry tasks were <0.90, these tasks were retained. Second, in the third grouping of stairs, ramp, and door tasks, we chose to remove the ramp task because it may be difficult to reproduce exactly in a clinical setting (as identified by one of our experts). It was surprising that the stairs and door tasks were correlated so highly. Both require use of the upper extremities, but otherwise, they appear to be very different in nature, and so were retained. No changes were made to the second grouping because the up & go and obstacles tasks are very different. The revised SCI-FAP, comprising 7 tasks (appendix), has high internal consistency (Cronbach α = .95).
Intertask and Task-Total Correlations of the SCI-FAP Tasks a
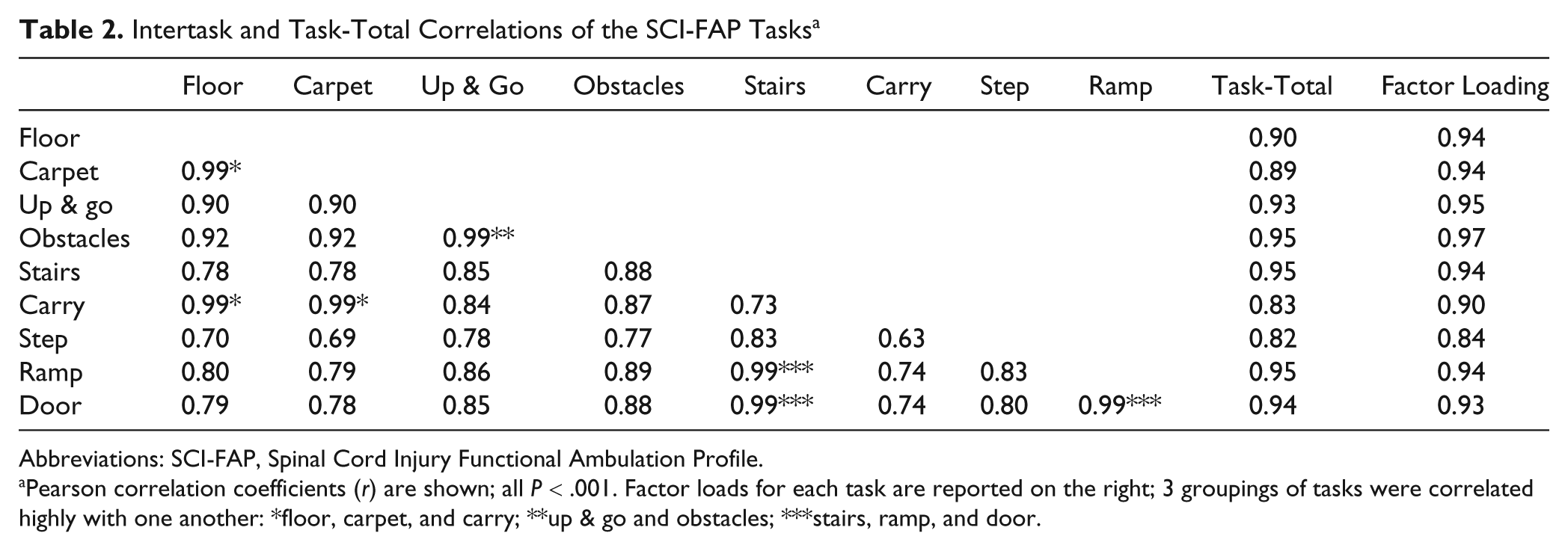
Abbreviations: SCI-FAP, Spinal Cord Injury Functional Ambulation Profile.
Pearson correlation coefficients (r) are shown; all P < .001. Factor loads for each task are reported on the right; 3 groupings of tasks were correlated highly with one another: *floor, carpet, and carry; **up & go and obstacles; ***stairs, ramp, and door.
Reliability of the SCI-FAP
Interrater and test-retest reliability were both high (Table 3). Interrater reliability for the total SCI-FAP, the normalized total time, and the total assistance scores were all 1.000. ICC values for the 7 tasks individually were all ≥0.975. The tasks with the lowest interrater reliability were the obstacles and stairs. This resulted from an occasional discrepancy in whether or not an obstacle was hit or in the number of rails used (stairs). The ICC values for interrater reliability were very similar for the original 3 raters (ICC = 1.000) and the lead rater with the 2 therapists unfamiliar with the SCI-FAP (ICC = 0.998). Test-retest reliability of the SCI-FAP was slightly lower than interrater reliability (ICC = 0.983; Table 3). ICC values for the tasks range from 0.959 to 0.992.
Interrater and Test-Retest Reliability a
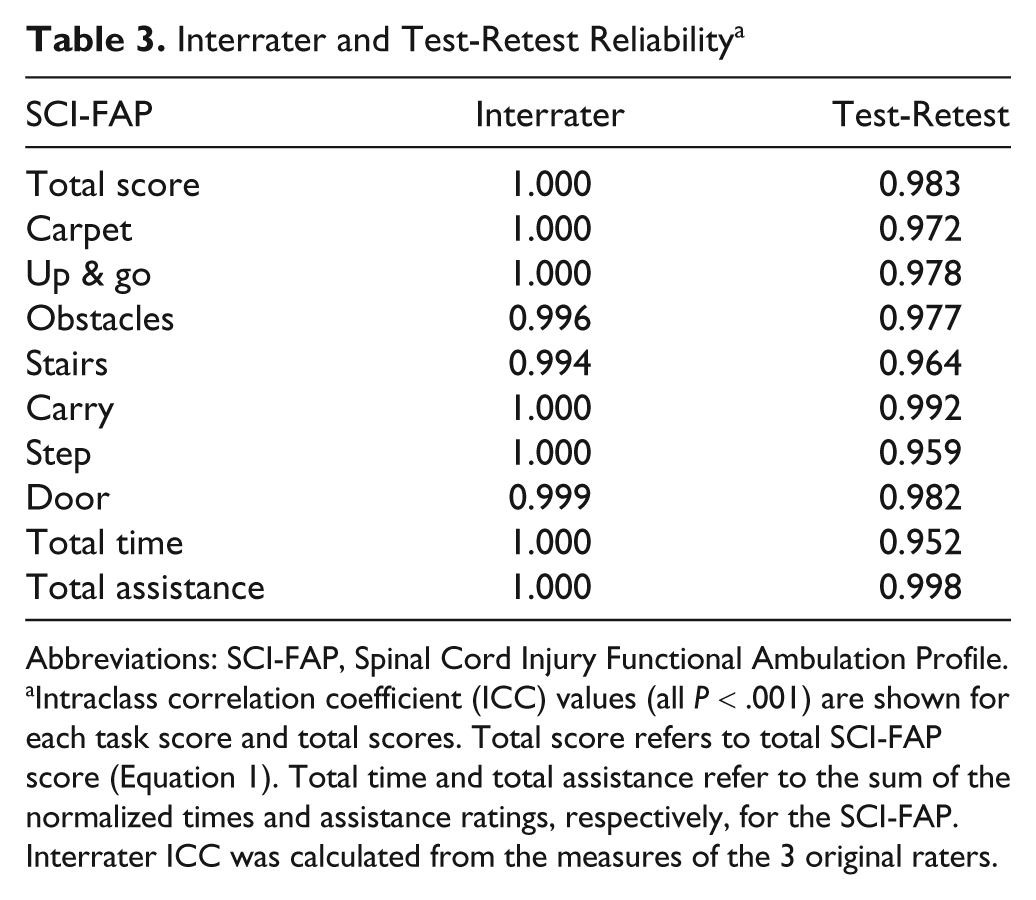
Abbreviations: SCI-FAP, Spinal Cord Injury Functional Ambulation Profile.
Intraclass correlation coefficient (ICC) values (all P < .001) are shown for each task score and total scores. Total score refers to total SCI-FAP score (Equation 1). Total time and total assistance refer to the sum of the normalized times and assistance ratings, respectively, for the SCI-FAP. Interrater ICC was calculated from the measures of the 3 original raters.
Discriminative Validity of the SCI-FAP
Participants with ISCI scored significantly higher on the SCI-FAP (total score P = .002; and task scores, .001 < P < .01) compared with their able-bodied counterparts. The mean total score of the SCI-FAP was 7.2 ± 0.8 (range, 5.8-9.6) for able-bodied participants and 271.3 ± 451.0 (range, 8.5-1900.0) for the ISCI group. Figure 1A shows the mean scores for each task for the ISCI group. There is a lot of variability among the participants with ISCI. In all, 5 participants achieved total scores on the SCI-FAP similar to those of able-bodied individuals, whereas the 3 participants who could not complete all SCI-FAP tasks scored >1000.
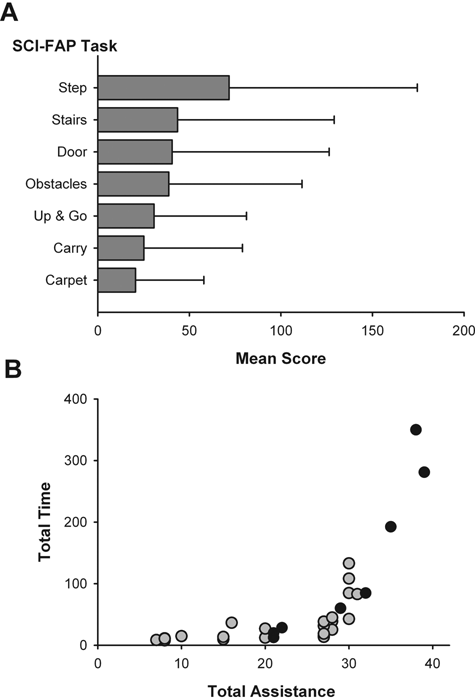
A. Mean score (+1 standard deviation) on SCI-FAP tasks for all 32 participants with ISCI. Scoring is shown in Equation 1. Mean scores for able-bodied participants (not shown here) were 1.0 for each task. B. Total normalized time versus total assistance score for each participant with ISCI. Total refers to the sum of the normalized times or assistance ratings for the 7 SCI-FAP tasks. Each dot represents a participant with ISCI. Gray and black dots represent participants tested at the University of Alberta and the University of British Columbia, respectively
Relationship Between Time and Assistance Scores
The assistance score helped reduce the ceiling effect of the time score. Figure 1B shows that many higher functioning participants with similar time scores had varying assistance scores, indicating that the assistance score made an important contribution to differentiating walking ability among the higher functioning individuals.
Convergent Validity of the SCI-FAP
Total scores on the SCI-FAP (Figure 2) were moderately correlated with the results from the 10MW (r = −0.59; P = .001), the 6MW (r = −0.59; P = .001), the self-selected WISCI II (M = −0.68; P = .001), and the maximal WISCI II (M = −0.70; P = .001). The individual SCI-FAP tasks also showed moderately strong correlations with the other 4 walking measures (Table 4).
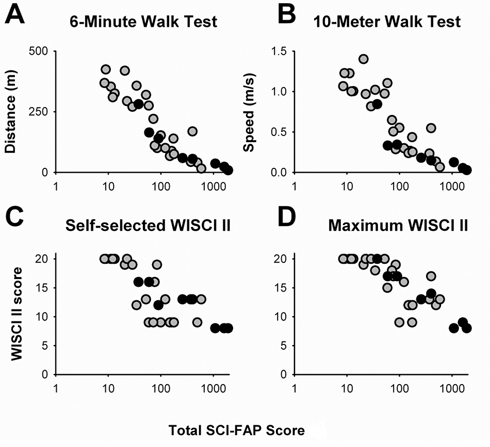
Total SCI-FAP score versus scores in the 6-minute walk test (A), 10-meter walk test (B), self-selected WISCI II (C), and maximal WISCI II (D): SCI-FAP scores for all 32 participants plotted on a logarithmic scale because of the large range of SCI-FAP scores seen in these individuals. Each dot represents a participant with ISCI. Gray and black dots represent participants tested at the University of Alberta and the University of British Columbia, respectively
Correlations Between SCI-FAP Scores and 4 Other Measures of Walking Function a
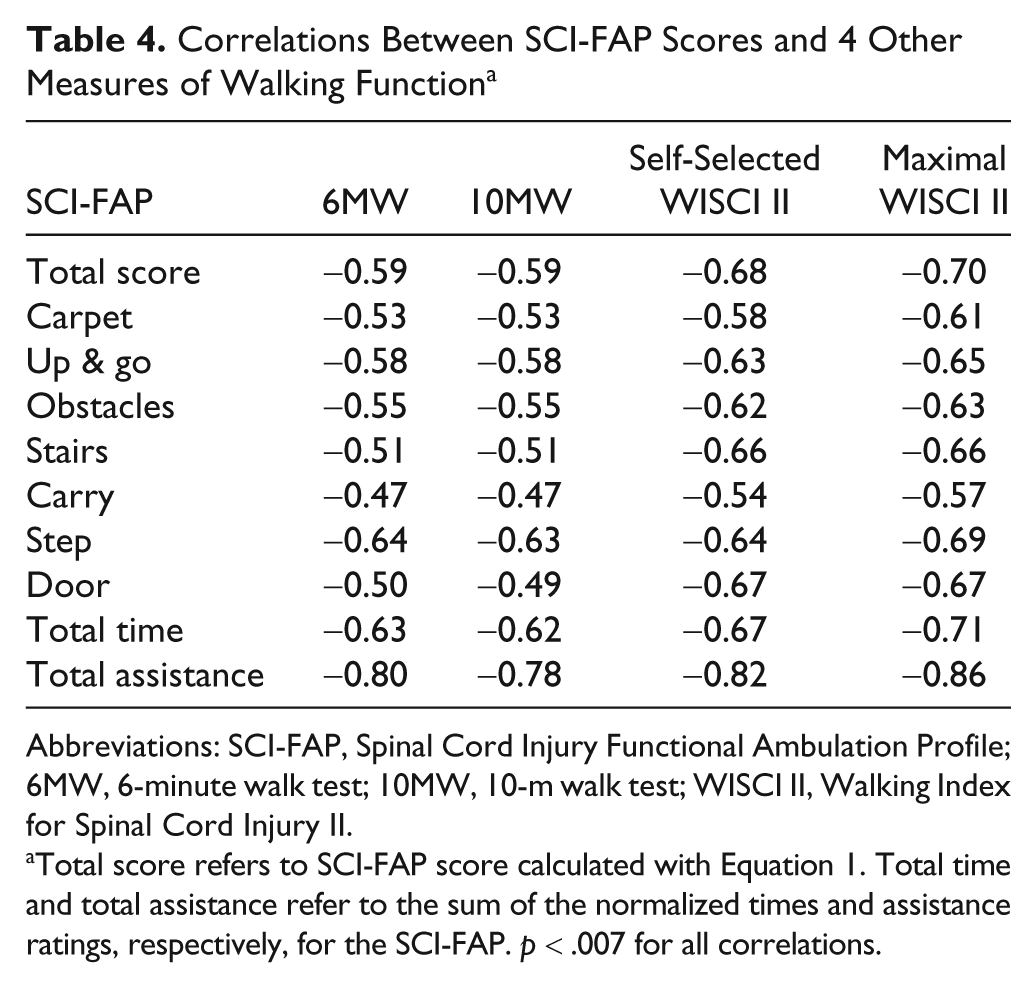
Abbreviations: SCI-FAP, Spinal Cord Injury Functional Ambulation Profile; 6MW, 6-minute walk test; 10MW, 10-m walk test; WISCI II, Walking Index for Spinal Cord Injury II.
Total score refers to SCI-FAP score calculated with Equation 1. Total time and total assistance refer to the sum of the normalized times and assistance ratings, respectively, for the SCI-FAP. p < .007 for all correlations.
Discussion
Our findings suggest that the SCI-FAP is a valid and reliable measure of functional walking for the ISCI population. It has high internal consistency, interrater reliability, and test-retest reliability. Experts in the ISCI rehabilitation field confirmed its content validity, and discriminative and convergent validity are demonstrated.
SCI-FAP as a Measure of Functional Walking Ability
Few SCI-specific measures of walking exist. 26,27 In addition to the WISCI II, there is the Spinal Cord Injury Functional Ambulation Inventory, which focuses on the quality of gait. 28 The Spinal Cord Independence Measure assesses indoor and outdoor mobility, 29 but because the tasks in this measure can be performed with a wheelchair, it is not strictly a measure of walking function.
The tasks included in the SCI-FAP were based on our knowledge of what constitutes functional walking. 2,12,16 All important tasks that can be reasonably assessed in a clinical setting were included. Moreover, many of the SCI-FAP tasks (obstacles, carry, door) are tasks that individuals with ISCI encounter at a significantly lower frequency than that of their able-bodied counterparts, 12 suggesting that they are a challenge for this population.
The SCI-FAP was intended to measure 1 construct only (ie, functional walking). The results from the factor analysis, assessment of internal consistency, and intertask correlations suggest that this is the case. 30 Redundancy was reduced by the removal of the floor and ramp tasks. Some other tasks may be improved in the future to further minimize redundancy. For example, the carry task did not challenge our participants, resulting in very similar results to the carpet task (Figure 1). A weighted bag held in the hand or on the forearm may be more challenging, as is done in the Community Balance and Mobility Scale. 31 The obstacles task was highly correlated with the up & go task. Removing the 180° turn (which is present in both tasks) from one of the tasks might help reduce the similarity in the future.
The step task showed the lowest correlations with the other tasks (Table 2). Moreover, it had the highest mean time (Figure 1), suggesting that it was the most challenging for individuals with ISCI. The step task likely requires greater limb strength and balance than the other tasks.
Scores on the SCI-FAP were moderately correlated with scores on the 6MW and 10MW, and WISCI II. Moderately strong correlations suggest that the SCI-FAP was measuring the same construct as the other tests but was also contributing new information. 22 Whereas all 3 tests are a function of overground walking speed, SCI-FAP adds the unique aspect of other daily walking tasks.
The SCI-FAP May Be Most Appropriate for Individuals With Moderate Walking Function
We have shown that the SCI-FAP is an appropriate measure for individuals with some walking function; however, even clients who cannot walk can be scored on the SCI-FAP. The SCI-FAP, however, has a ceiling effect. It will not discriminate between individuals who walk at normal speeds without devices or physical assistance. There is little difference in SCI-FAP scores for our highest-functioning participants. This is not surprising because the SCI-FAP is meant to reflect common walking tasks rather than challenge walking balance or skill beyond daily requirements. Measures like the 6MW, where individuals can walk at fast rather than comfortable speeds, may be more appropriate for tracking change over time in these very high-functioning individuals. The assistance ratings, however, reduce the ceiling effect. Without these ratings in the total SCI-FAP score, all participants who walked at normal walking speeds would experience a ceiling effect (Figure 1B).
We made an effort to minimize the floor effect of the SCI-FAP by setting high maximum times for the tasks. However, a participant who cannot walk at all would score the maximum score of 2100, as would a participant who could walk very short distances but never long enough to complete a task. Thus, the SCI-FAP may be most appropriate for clients with moderate walking function, that is, those who walk slower than their able-bodied counterparts or need walking aids to complete the tasks.
Considerations When Using the SCI-FAP
First, the SCI-FAP does not distinguish between different levels of manual assistance. This was done to remove subjectivity from the scoring of the SCI-FAP, a potential limitation that was identified by our experts. Furthermore, whether an individual requires supervision or moderate assistance to walk, he/she ultimately needs another person to complete the task. Therapists can make note of the amount of assistance provided in the “Comments” section (appendix).
Second, the SCI-FAP does not consider the use of braces, such as an ankle-foot orthosis. This differs from the WISCI II 18 and mEFAP. A rating for braces was removed from the SCI-FAP because none of our participants completed any tasks with braces only (ie, no other device or assistance). Likewise, a WISCI II rating of 18—“ambulates with no devices, with braces and no physical assistance”—is rarely encountered. 32 If someone completes a SCI-FAP task with braces only, he/she should be rated as independent.
Third, timing begins with participants in a stationary position, as opposed to already walking as is done for the 10MW. As a result, the recorded time includes acceleration effects. This better reflects functional walking, which consists of many starts and stops. Indeed, most SCI-FAP tasks involve periods of acceleration and deceleration throughout the task (eg, pause to lift a foot over the obstacle or open a door).
Fourth, the SCI-FAP score consists of 2 components: time and assistance rating. The sums of the normalized times and assistance ratings from each task can be reported separately to create a total score for both time and assistance. Both total time and assistance scores showed high interrater and test-retest reliability (Table 3) and moderately strong correlations with other measures of walking (Table 4).
Finally, although we choose equipment for the SCI-FAP that is generally available (eg, standard therapy stairs, a step height that approximates the standard curb height), it may still be difficult to reproduce in some centers. The SCI-FAP tasks, however, can be treated as independent tests. Each task has been shown to have acceptable interrater reliability, test-retest reliability, and discriminative and convergent validity. Clinicians and researchers can choose to include whichever tasks are feasible in their setting. In the appendix, we specify the dimensions of the equipment we used. These dimensions should be adhered to if one chooses to score the SCI-FAP as we have in the present study (appendix). The mean able-bodied times would have to be reevaluated if the dimensions of the equipment are different from those reported here.
Limitations
We tested the SCI-FAP on only a few individuals with very low walking function. We required our participants to be able to walk ≥5 m to ensure that all participants would likely be able to complete at least 1 SCI-FAP task (ie, carpet task) as well as attempt the WISCI II, 10MW, and 6MW. In the future, it would be beneficial to try the SCI-FAP in more individuals with very low walking ability.
Two procedural differences in the testing at the 2 sites may have influenced the results. The 6MW was performed on a 25-m walkway at UA and a circular loop at UBC. A loop is preferable for this test because it eliminates the need to make 180° turns, which can take a significant amount of time in lower-functioning individuals. Furthermore, the 6MW was performed first at UBC, whereas the SCI-FAP was performed first at UA. Both these differences could have biased the 6MW distance to be higher at UBC than at UA. Therefore, we matched the participants tested at the 2 sites according to their SCI-FAP scores (±10), and compared their 6MW distances. No differences were found (P = .685; n = 4).
Future Directions
The SCI-FAP may be a useful measure for the acute and subacute ISCI populations as well and should be tested in the future. Its sensitivity to change and the minimal clinically important difference will also need to be assessed.
Footnotes
Acknowledgements
We thank the participants, therapists, and therapy assistants (J. McPhail, K. Pope, B. Norton, G. Bostick, K. Pauhl, J. Loffree) and the MScPT students (Y. Hetze, J. Leathem, K. Nordquist, C. Nelson, H. Olsen).
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the Canadian Institutes of Health Research (JY). Scholarships from the Canadian Institutes of Health Research and the Alberta Heritage Foundation for Medical Research supported KM. TL was supported by a CIHR New Investigator Award.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.