
Abstract
Background. In spinal cord injury, there are multiple databases containing information on functional recovery, but data cannot be pooled or compared due to differences in how function is measured. A crosswalk is needed to link or convert scores between instruments. Objectives. To create a crosswalk between the voluntary musculoskeletal movement items in the Functional Independence Measure (FIM®) and the Spinal Cord Independence Measure III (SCIM III) for spinal cord injury. Methods. Retrospective datasets with FIM® and SCIM III on the same people were used to develop (Swiss dataset, n = 662) and validate (US, n = 119, and Canadian datasets, n = 133) the crosswalks. Three different crosswalk methods (expert panel, equipercentile, and Rasch analysis) were employed. We used the correlation between observed scores on FIM® and SCIM III to crosswalked scores as the primary criterion to assess the strength of the crosswalk. Secondary criteria such as score distributions, Cohen’s effect size, point differences, and subgroup invariance were also evaluated. Results. All three methods resulted in strong correlation coefficients, exceeding the primary criterion value of r = .866 (.897–.972). Assessment of secondary criteria suggests the equipercentile and Rasch methods produced the strongest crosswalks. Conclusions. The Rasch FIM®/SCIM III crosswalk is recommended because it is based on co-calibration of linearized measures, allowing for more sophisticated parametric analyses. The crosswalk will allow comparisons of voluntary musculoskeletal functional recovery across international databases using different functional measures, as well as different systems of care and rehabilitation approaches.
Keywords
Introduction
Clinical outcome measures are essential to assessing functionally relevant improvements following central nervous system disease or insult. In the field of spinal cord injury (SCI), the two most common functional outcome measures for activities of daily living are the Functional Independence Measure (FIM®) and the Spinal Cord Independence Measure III (SCIM III).1,2
The FIM® is a generic rehabilitation outcome measure developed in 1984 to assess burden of care, document disability, and measure functional status in a consistent manner following rehabilitation. 3 Until recently, FIM® was required for inpatient rehabilitation units in North America and has been used in many other countries, for nearly 35 years. The SCIM was developed in 1997, to assess the ability of individuals with SCI to perform activities of daily living, 4 with SCIM III developed in 2007. 5 SCIM III is commonly used in Europe, due to its specificity and sensitivity to change in the SCI population.2,5-7
The two largest SCI databases, the US-based Spinal Cord Injury Model Systems and the European Multicenter Study about Spinal Cord Injury databases, use the FIM® and SCIM III, respectively; thus, data cannot be pooled or compared. A crosswalk, where scores from one measure are converted to scores on another measure, would facilitate our understanding of cross-national SCI functional recovery data.
The purpose of this research was to develop and validate crosswalks between FIM® and SCIM III for items reflecting voluntary musculoskeletal movement.
Methods
Research Design and Datasets
This study was exempt from IRB review as determined by the Colorado Multiple Institutional Review Board.
We conducted secondary data analysis using three retrospective datasets containing FIM® and SCIM III data from the same participant with SCI. For all datasets, we excluded missing or out of range values (values outside the scoring range for a given FIM or SCIM III item), including data for which it was not possible to calculate the time frame between FIM® and SCIM III or the time between the different assessments was more than 7 days (to minimize the possibility of changes in function between exams), data for which there was no FIM® locomotion modifier, or where SCIM III data were collected by questionnaire. Where repeated measures were available, data were randomized to a single time point. The crosswalks were created using data from the development dataset. Crosswalk assessment criteria were then applied in both the development and validation datasets.
The development dataset was collected from four SCI centers in Switzerland (Swiss) participating in a research study to compare FIM® and SCIM III. Cross-sectional data were collected approximately every 6–7 weeks during inpatient rehabilitation (within the calendar week). After applying the exclusions and randomization noted above, data from 662 subjects with both FIM® and SCIM III data were selected to develop the crosswalk. No demographic data were available.
Two datasets were used for validation. The first was the US-based SCIM III reliability study 7 and the second was from the Rick Hansen SCI Registry based in Canada. After applying exclusions noted above, 119 pairs of FIM®/SCIM III data pairs from the US dataset and 133 from the Canadian dataset were used for validation.
Standard FIM® training occurred for all datasets, either as part of routine training (United States and Canada) or for a specific study (Swiss). The developers of SCIM III suggest that no specific training is required; thus, none was provided for the US and Swiss datasets. 7 The Canadian dataset provides a SCIM III guidance manual.
Functional Assessments
Summary of FIM® and SCIM III Voluntary Musculoskeletal Movement Items.
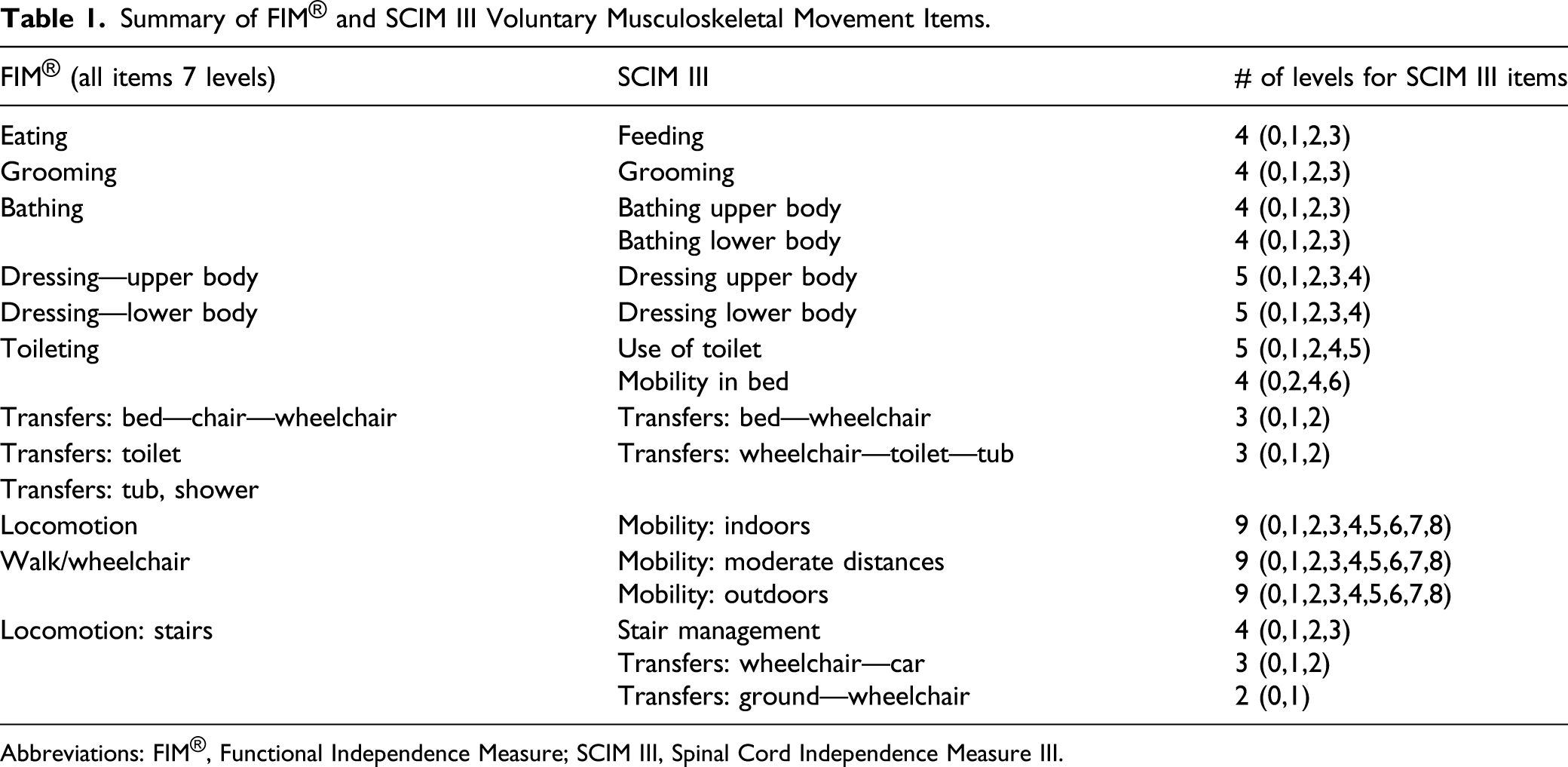
Abbreviations: FIM®, Functional Independence Measure; SCIM III, Spinal Cord Independence Measure III.
Dimensionality Evaluation
As a prerequisite to crosswalk development, it is essential to determine the extent to which the instruments to be crosswalked assess a single underlying construct.12,13 If measures assess multiple constructs, crosswalks for each construct would need to be created separately. FIM® and SCIM III both assess activities of daily living, and only items reflecting voluntary musculoskeletal movement were used for crosswalk development. We used exploratory factor analysis (SPSS version 24) to assess factor structure where the “factors” represent dimensions. For a single factor structure, the primary criterion was a ratio > 4 between the first and second factors, indicating that the first factor explains 4 times the variance of the second factor.13,14
Crosswalk Methods
We used three methods to generate crosswalks, the details of which are described below:
Method 1—expert panel: Three experts (two coauthors and an experienced SCI researcher) created algorithms for recoding both FIM® and SCIM III items and scores into a new common measure—the expert panel FIM®/SCIM. The expert panel recoding algorithms were then reviewed and modified where needed, based on input by six physical and occupational therapists from three different rehabilitation facilities who routinely use both FIM® and SCIM III in clinical practice.
Method 2—equipercentile: We aligned total scores on each instrument by percentile rank of the score distributions. 15 For example, total observed scores at the 25th percentile for FIM® were lined up with the SCIM III observed scores at the 25th percentile and so on. Due to differences in rounding and the total range of scores between instruments, two crosswalk tables (observed FIM® to equipercentile SCIM III and observed SCIM III to equipercentile FIM®) were created.
Method 3—Rasch analysis: Classical test theory focuses on the test score, while Rasch analysis, a modern statistical approach, focuses on test items. With this approach, the difficulty of individual test items can be determined by considering item difficult relative to person ability, by placing them on a common (log transformed) linear scale. This is not possible with classical approaches which only use total scores. A comprehensive description of the applications of Rasch analysis in rehabilitation is outside the scope of this manuscript but can be found in Velozo, Kielhofner, and Lai. 16
To develop the Rasch crosswalk, we co-calibrated 11 FIM® and 16 SCIM III items on a common Rasch linear scale (Winsteps version 4.5.1) using the method described by Velozo et al. 17 A Rasch group rating scale model was used where items with the same scoring options are grouped. Crosswalked scores were derived by matching the closest logits for FIM® and SCIM III total scores. Winsteps steps and coding can be found in Supplemental Appendix 1.
Crosswalk Assessment
Observed FIM® and SCIM III scores were first re-coded to crosswalk scores for each method (see SPSS coding in Supplemental Appendix 1). For Method 1, comparisons were between the crosswalked expert panel FIM® scores and expert panel SCIM III scores. For Methods 2 and 3, comparisons were between observed and crosswalked scores (e.g., observed FIM® and equipercentile FIM®, observed FIM® and Rasch FIM®, etc.).
The primary crosswalk assessment criterion was a correlation coefficient between observed and crosswalked scores greater than .866, as established by Dorans,
18
which reduces crosswalk uncertainty by 50% in predicting a person’s score. Correlations were assessed using the Pearson correlation coefficient, in order to enable comparisons with existing literature. Secondary criteria were applied to all crosswalks that met the primary criteria, to further assess and differentiate the crosswalks and determine if they could be used at the individual or group level. Secondary criteria included the following: Similar subpopulation invariance between actual and crosswalked scores across gender (male and female), age-groups (0–30, 31–60, and 61–100 years), level of injury (paraplegia and tetraplegia), and severity of injury (motor complete and motor incomplete), as defined by standard mean differences (SMD = mean score of group 1 minus mean score of group 2, divided by total group standard deviation) Similar score distributions between actual and crosswalked scores as defined by no statistically significant differences in means, means within one standard deviation of one another, standard deviations within one unit of each other, and overlap of confidence intervals for skewness and kurtosis.20,21 Similar distribution of differences between actual and crosswalked scores as assessed by Bland–Altman plots.
22
Small amount of difference between distributions as assessed by Cohen’s effect size using the criteria of .8 = large, .5 = medium, and .2 =small.
23
Small point differences between actual and crosswalked scores as defined by at least 75% of score differences less than ½ standard deviation apart.
19
Results
Demographic, injury characteristics, and data characteristic data are in Supplemental Appendix 2. In addition to no demographic and injury characteristics being available for the Swiss sample, there were considerable missing data for level and severity of injury, particularly for the US sample (51% for level and 41% for severity of injury). The Canadian sample had a higher percentage of individuals with cervical injury relative to the US sample (66% vs 47%) and a longer length of stay (139 ± 76 vs 69 ± 50), but there were no other significant differences among the samples.
Exploratory factor analysis FIM®/SCIM III data supported a single underlying construct. The first factor explained 60% of the total variance, while the second factor explained 11%, a ratio of 5.5. Thus, we proceeded with the assumption of unidimensionality of voluntary musculoskeletal function and created a single crosswalk using each method.
Method 1—Expert Panel
Due to FIM® scoring consistently ranges from 1–7, and SCIM III scoring ranges varying between items, this method produced reduced score ranges for all expert panel FIM®/SCIM III items. An example of score reduction is illustrated in Supplemental Appendix 2, for the FIM®/SCIM III grooming item where SCIM III scoring ranges from 0–3 and FIM® scoring ranges from 1–7. The expert panel FIM®/SCIM III grooming item therefore has three possible scores from 0–3.
Where needed, individual items were combined to form the expert panel FIM®/SCIM, such as with bathing where FIM® has one item and SCIM III separates bathing into upper and lower extremity. Not all SCIM III items were used as they do not have an equivalent FIM® item such as mobility in bed and action to prevent bed sores, wheelchair to car, and ground to wheelchair transfers. For SCIM III mobility items, only the moderate distance category was utilized as it most closely aligned with FIM® mobility. In total, 11 of 16 SCIM III mobility items and all 11 FIM® voluntary musculoskeletal motor items were used.
Method 2—Equipercentile
Figure 1 provides a graphical example of the crosswalked scores using Method 2. In our sample, the percentile ranks were well distributed (indicating that a single value on one scale generally corresponds to a single value on the second scale); thus, no statistical smoothing of score distributions to approximate population scoring was required. Equipercentile linking observed SCIM III to converted FIM® by percentile rank in the development (Swiss) dataset. Total score percentile ranks are matched for both outcome measures, from which the crosswalk score is derived. For example, a raw SCIM III score of 30 is equivalent to a raw FIM score of 50, based on a percentile rank of approximately 60%. FIM®, Functional Independence Measure; SCIM III, Spinal Cord Independence Measure III.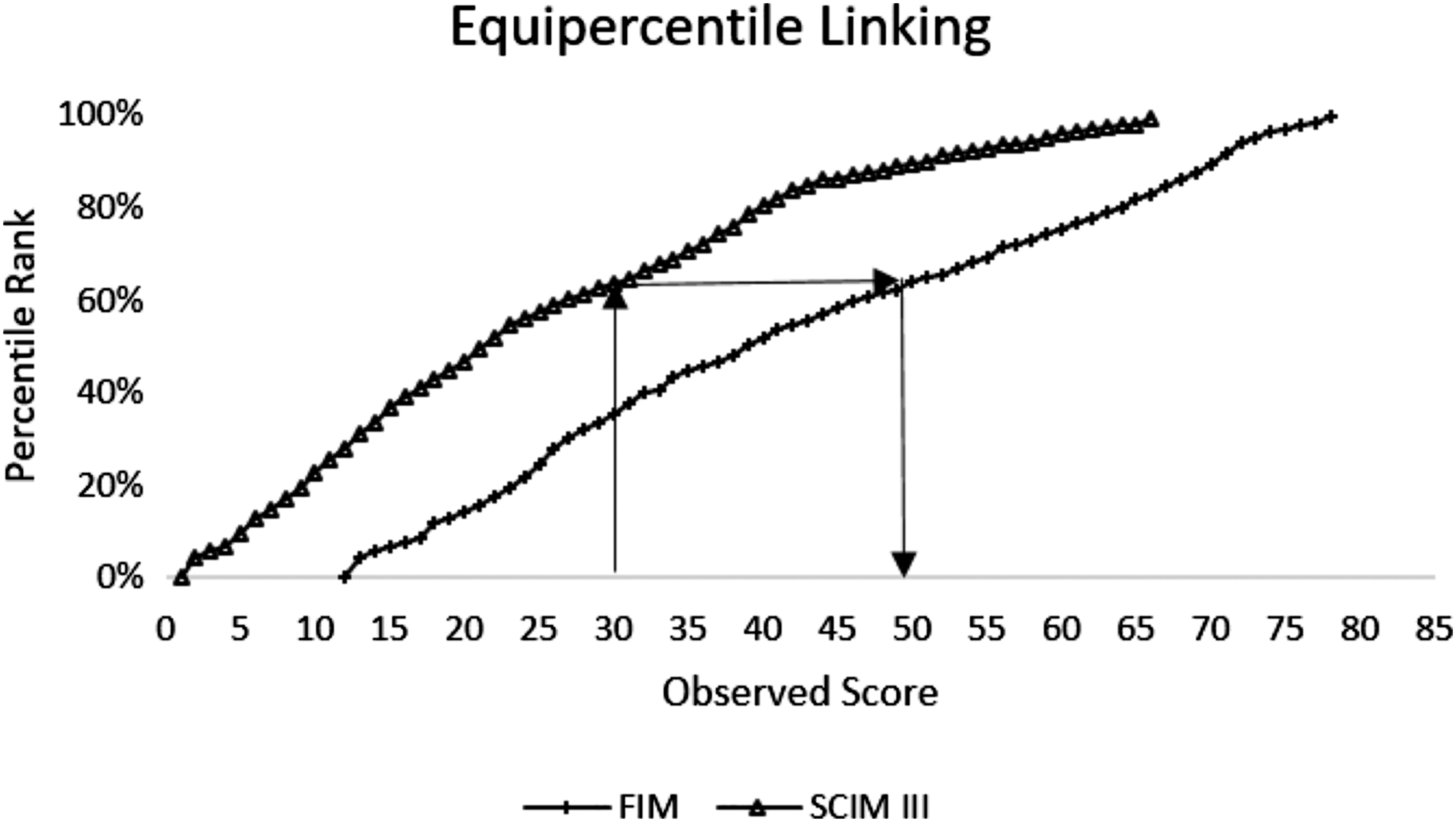
Method 3—Rasch Analysis
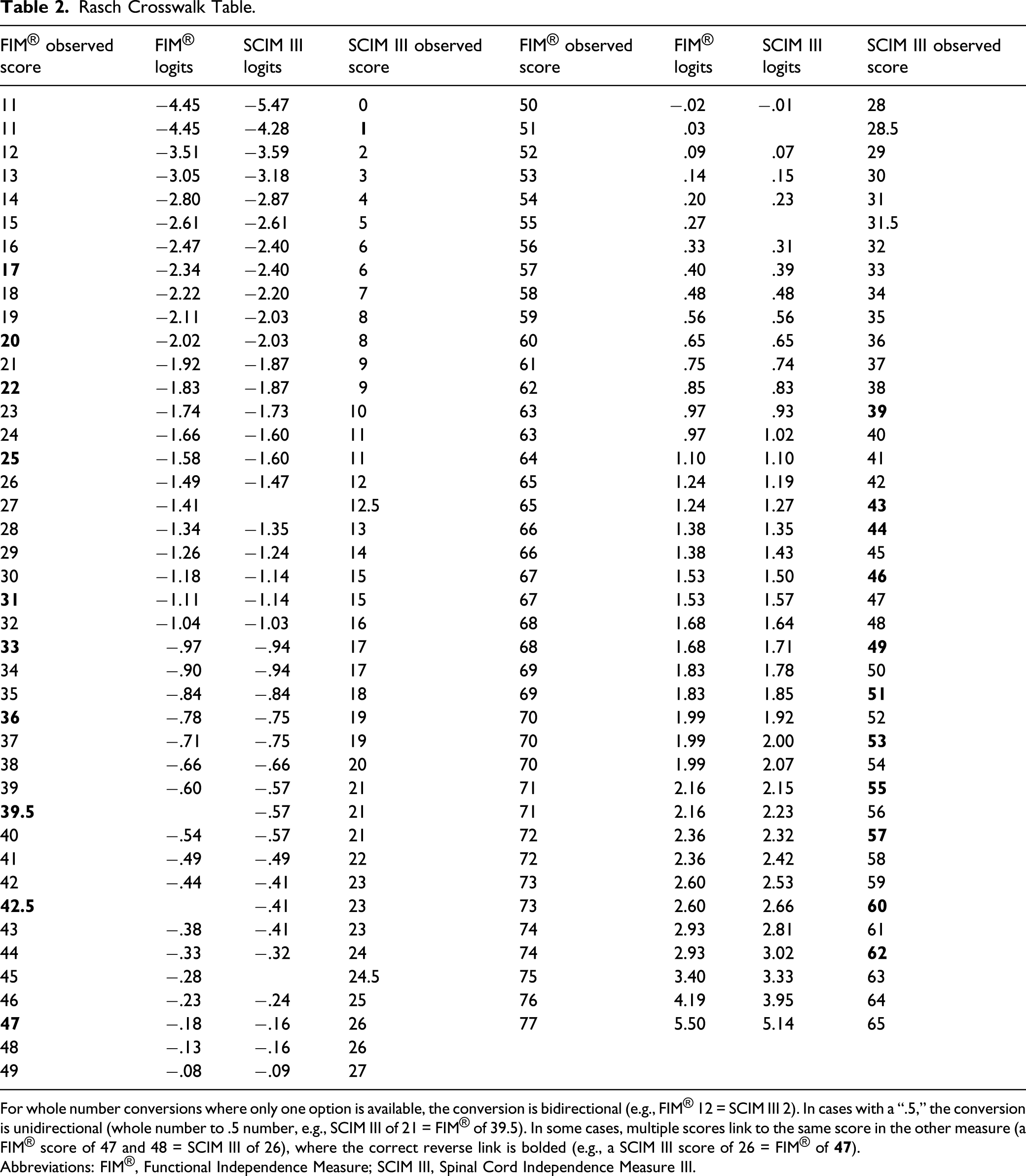
The Rasch person item map (Figure 2) shows person ability relative to item difficulty, on the same linear (logit) scale. For example, FIM® eating and SCIM III feeding are both on the lower end of the scale, meaning these two items demonstrate similar item difficulty and are relatively easy items to perform. Conversely, FIM® and SCIM III stairs and SCIM III ground transfers are the most difficult items. Rasch analysis of the combined FIM®/SCIM III item bank demonstrated good psychometric properties with person reliability of .94 and a wide range of item difficulty (−2.31 to 2.28 logits). Two misfitting items (items that may not fit the unidimensional construct) were identified but were retained in the model to facilitate ease of crosswalk use. The resulting crosswalk tables for converting FIM® scores to SCIM III scores and vice versa with associated logits are presented in Table 2 (instructions for use are in the footnote). Rasch person-item map. This figure illustrates person ability and item difficulty on the same linear scale. Person ability is on the left side of the figure, with item difficulty on the right, with higher ability/difficulty at the top, and lower ability/difficulty at the bottom, as measured by logits (on the left). Rasch Crosswalk Table. For whole number conversions where only one option is available, the conversion is bidirectional (e.g., FIM® 12 = SCIM III 2). In cases with a “.5,” the conversion is unidirectional (whole number to .5 number, e.g., SCIM III of 21 = FIM® of 39.5). In some cases, multiple scores link to the same score in the other measure (a FIM® score of 47 and 48 = SCIM III of 26), where the correct reverse link is bolded (e.g., a SCIM III score of 26 = FIM® of Abbreviations: FIM®, Functional Independence Measure; SCIM III, Spinal Cord Independence Measure III.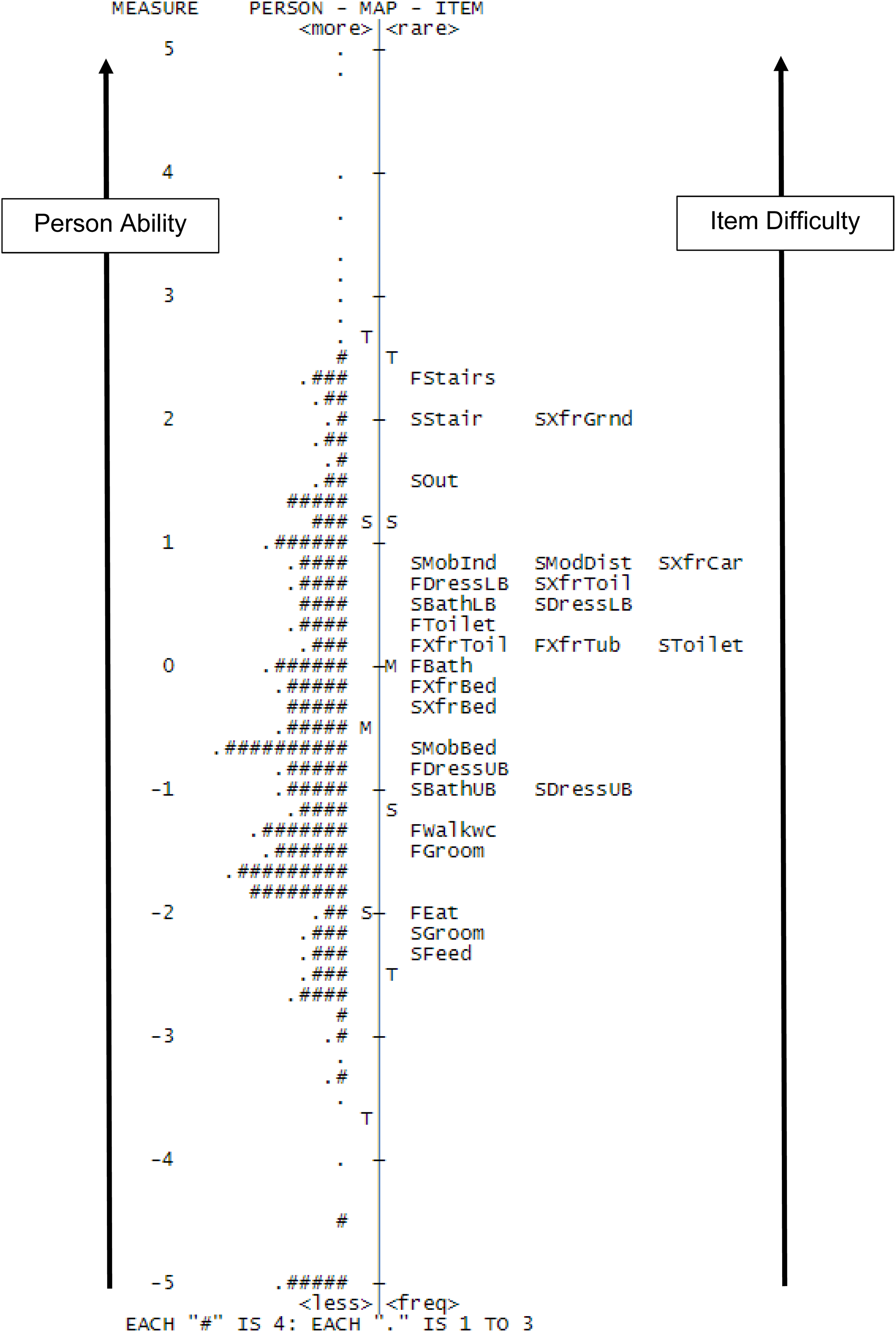
Primary Crosswalk Assessment
Summary of Primary and Secondary Crosswalk Assessment Criteria by Method and Dataset.
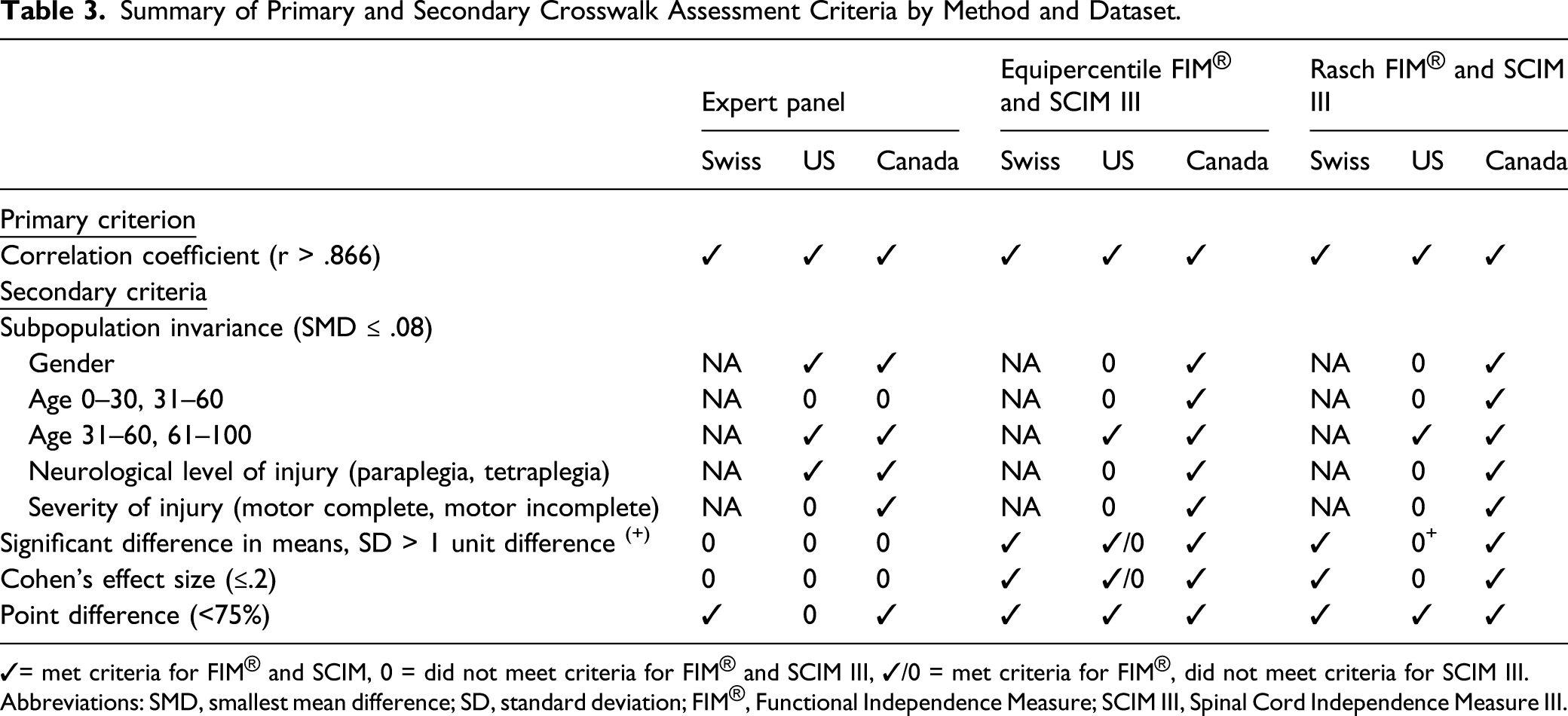
✓= met criteria for FIM® and SCIM, 0 = did not meet criteria for FIM® and SCIM III, ✓/0 = met criteria for FIM®, did not meet criteria for SCIM III.
Abbreviations: SMD, smallest mean difference; SD, standard deviation; FIM®, Functional Independence Measure; SCIM III, Spinal Cord Independence Measure III.
Secondary Crosswalk Assessment
Subpopulation invariance was assessed from available data in the US and Canadian datasets (as no demographic data were available in the Swiss dataset). The expert panel method met criteria for all comparisons in all datasets, except for differences between ages 0–30 and 31–60 (SMD = .09), which was not met in either dataset. Criteria for all equipercentile and Rasch comparisons were met in the Canadian dataset, and in the US dataset for age 31–60 and 61–100, but no other criteria were achieved in the US dataset (SMD = .09–.23).
Means were all within one standard deviation of each other, and all confidence intervals for skewness or kurtosis demonstrated overlap across all comparisons and datasets. Means were significantly different across expert panel comparisons in all datasets. Equipercentile and Rasch analysis met criteria for all comparisons in the Canadian dataset, and for observed FIM® to equipercentile SCIM III comparisons in the US dataset, but did meet criteria for other comparisons.
Distribution of score differences as assessed by Bland–Altman plots did not show any differences among methods or datasets. Cohen’s effect size exceeded .20 and ranged from medium to large effect sizes for the expert panel method for all comparisons (.38–.65). For the equipercentile and Rasch methods, effect sizes met criteria for all comparisons in the Canadian dataset, and for observed FIM® to equipercentile SCIM III in the US dataset, but slightly exceeded criteria in the US dataset for all other comparisons (.21–.28).
Point differences were within .5 standard deviations 75% of the time for all comparisons (range 77.7%–91.7%), except expert panel in the US dataset (74%).
In summary, primary criterion was achieved for all methods and datasets. Secondary criteria were more frequently met for the equipercentile and Rasch methods relative to the expert panel method and in the Swiss and Canadian datasets relative to the US.
Discussion
We have demonstrated three effective methods for creating a FIM® and SCIM III crosswalk for items reflecting voluntary musculoskeletal movement. This work is strengthened by the use of three different datasets created for different purposes (two research studies and a registry), which increases generalizability of the study findings. All methods met pre-established primary criterion. However, secondary analyses revealed that the equipercentile and Rasch crosswalks met more criteria than the expert panel crosswalk. This study found the equipercentile and Rasch crosswalks are nearly identical, as illustrated in Figure 3. However, we recommend use of the Rasch crosswalks (Table 2) as this method uses all items and scores and places both instruments on a common and linear scale prior to create the crosswalk. Linearized data allow for the use of parametric statistics (used for interval or ratio data that are normally distributed) which are considered to have higher statistical power than non-parametric statistics (used for ordinal or skewed data) and allow for comparisons to other linear measures. Graphical display of differences between equipercentile FIM® and Rasch FIM® crosswalk. Plot of scores for equipercentile FIM® (EQ FIM) and Rasch FIM® (R FIM). FIM®, Functional Independence Measure.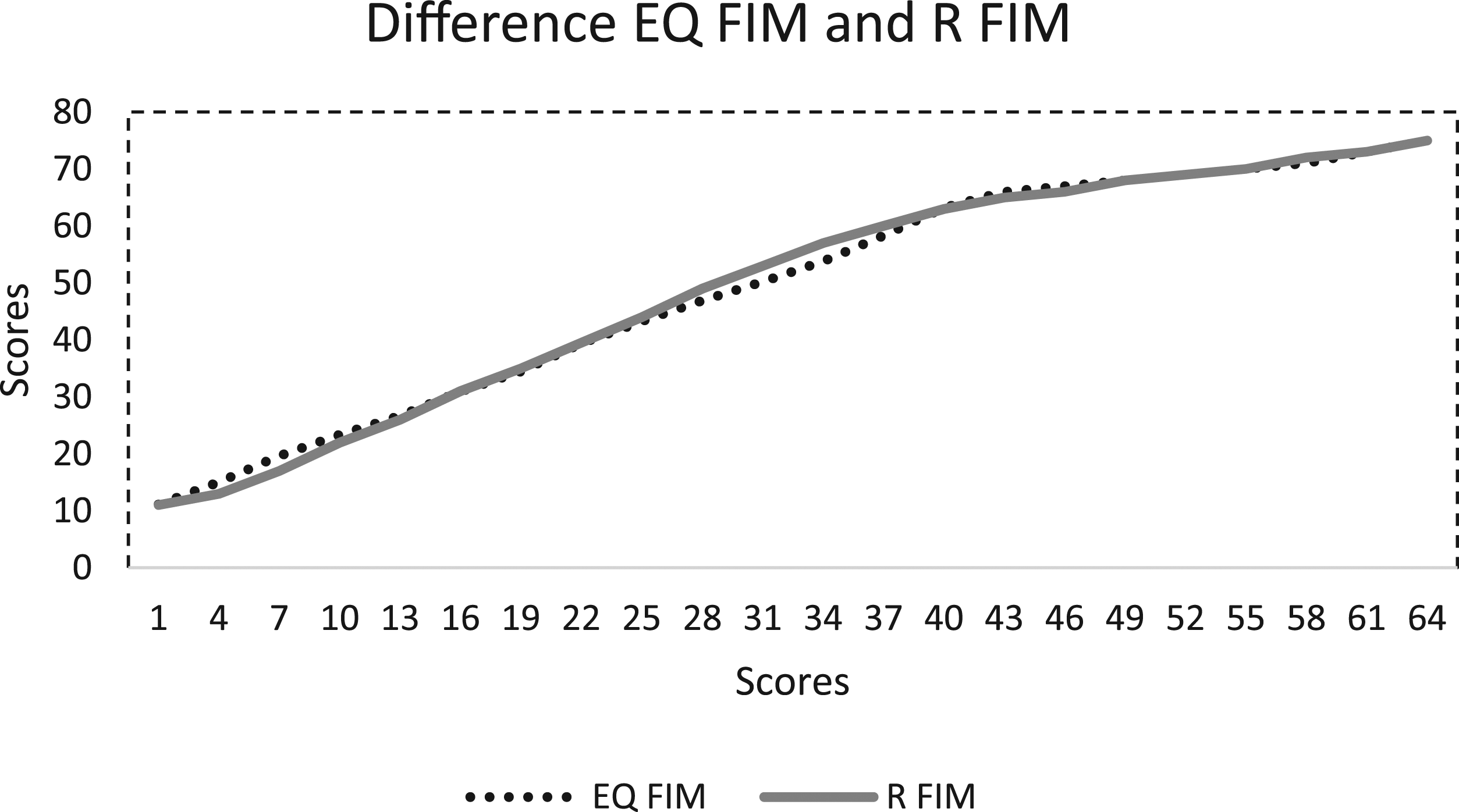
Given that all methods achieved the primary criterion, but differences were noted when assessing secondary criteria, our study suggests it is essential to apply secondary criteria when assessing crosswalk strength if correlation coefficients are within the acceptable range. Additionally, secondary assessments provide information about the use of a crosswalk at the group or individual level, the latter of which requires a stronger crosswalk. In particular, the percentage of point differences less than a .5 standard deviation from the mean exceeded 75% (except expert panel in the US dataset—74%) in all analyses and exceeded 80% (range 82.2–93.2%) for the recommended Rasch crosswalk. The high percentage of scores within a half standard deviation combined with high correlations suggests the Rasch crosswalk may be used at both the group and individual levels.
In prior studies, correlation coefficients between all 13 motor FIM® items and all 19 SCIM III items (inclusive of bowel, bladder, and respiratory [SCIM] items) ranged from .78–.80.5,7 In this study, where only items reflecting voluntary musculoskeletal movement were used, correlation coefficients were higher for observed FIM® and observed SCIM III scores (r = .898–.961) across all datasets compared to previous studies. This suggests that for items used in this study, the outcome measures assess a similar underlying construct, which was supported by exploratory factor analysis. Given the lower correlations when all motor FIM and SCIM III items are included, non-voluntary musculoskeletal movement items may represent a different construct (dimension) necessitating a separate crosswalk.
The primary purpose of this study was to create and validate a FIM®/SCIM III crosswalk. The recommended crosswalk may be used at the level of group or individual data. The rationale for crosswalk creation is to enable comparing, contrasting, and aggregating voluntary musculoskeletal movement data. This sub-set of items was chosen as it represents a common outcome/endpoint in SCI clinical trials. Charlifue et al. 24 discuss the advantages of harmonizing datasets in SCI to promote “new scientific discoveries and faster access to treatment interventions” and suggest that harmonization will enable meta-analysis, data pooling, and advanced statistical approaches. In clinical trials, harmonizing data will also allow for larger and more diverse international datasets from which to identify impactful outcomes that exceed natural recovery. Efforts are currently underway to compare neurological data from across Europe and North America; comparing functional outcomes is a natural next step. 25 A crosswalk provides a mechanism to compare data where different outcome measures are used prior to comparing or harmonizing datasets. A practical example of the utility of a FIM®/SCIM III crosswalk is when a research study has collected SCIM III data outside the United States and wishes to compare their findings to FIM® data collected in the United States.
Study Limitations
First, this study included a sample with considerable missing demographic data, which limited its analysis of subpopulation invariance. Second, FIM® and SCIM III scores collected within 7 days of one another were used to develop and validate the crosswalks as prior studies, 17 to minimize the potential for true change between time points. However, a closer time point may have resulted in even stronger crosswalks. As noted in the secondary crosswalk assessments, the US dataset met criteria less frequently than Swiss or Canadian datasets. This may have been due to the fact that the days between FIM® and SCIM III exams in the US dataset were significantly greater at discharge (averaging 1.90 days in the US dataset compared to .41 days in the Canadian dataset); thus, true change between FIM® and SCIM III may have occurred for these data points in the US dataset.
The crosswalk developed in this study only includes items reflecting voluntary musculoskeletal function and can only be applied to this dimension; thus, item level scores from FIM® and SCIM III are required to use the crosswalk. Additionally, these items may be considered a sub-set of items, which is a composite of items from different sub-scales, which have not been examined as such.
Future Directions
As noted, items used in this analysis represented a sub-set of FIM® and SCIM III items, from existing sub-scales within the measures. Further work to understand the strengths and limitations of this sub-scale is warranted.
Although a single crosswalk for each method was supported by the dimensionality assessments, future studies could develop a separate crosswalk for self-care and mobility sub-scales and compare the accuracy between a single construct of voluntary musculoskeletal movement and separated construct crosswalks. Creating crosswalks for non-voluntary movement items could be explored to include these important domains. Additionally, although Rasch allows for item and score reduction to strengthen a measure, all items and scores were used to develop the crosswalk for ease of use. Future study could examine whether using item and score reduction techniques results in a stronger crosswalk.
SCIM III data used in this analysis were collected by observation. Further study to assess the validity of the crosswalk by FIM® and SCIM III interview is warranted as this data collection method is frequently used in research studies with long-term longitudinal (repeated measures) follow-up.
As of 2018, the United States migrated to using the Continuity Assessment Record and Assessment (CARE) tool (in lieu of FIM®). The current FIM®/SCIM III crosswalk is still highly relevant due to the vast amounts of historical data in the Model Systems database (1973-October 2018), and countries outside the United States continue to collect FIM®. However, in the future a SCIM/CARE tool crosswalk may be warranted.
Conclusion
We compared and validated three methods for crosswalk development using data from three datasets. We suggest SCI clinicians and researchers use the Rasch co-calibration crosswalk table to compare data reflecting voluntary musculoskeletal movement between FIM® and SCIM III. The crosswalk may also be used to assess functional recovery over time in different countries or systems of care, as well as enabling direct comparisons for the purposes of establishing appropriate outcomes in clinical trials.
Supplemental Materials
sj-docx-1-nnr-10.1177_15459683211033854 – Supplemental Material for Development and Validation of Crosswalks Between FIM® and SCIM III for Voluntary Musculoskeletal Movement Functions
Supplemental Material, sj-docx-1-nnr-10.1177_15459683211033854 for Development and Validation of Crosswalks Between FIM® and SCIM III for Voluntary Musculoskeletal Movement Functions by Linda A. T. Jones, Chih-Ying Li, David Weitzenkamp, John Steeves, Susie Charlifue and Gale Whiteneck in Neurorehabilitation and Neural Repair
Supplemental Materials
sj-docx-2-nnr-10.1177_15459683211033854 – Supplemental Material for Development and Validation of Crosswalks Between FIM® and SCIM III for Voluntary Musculoskeletal Movement Functions
Supplemental Material, sj-docx-2-nnr-10.1177_15459683211033854 for Development and Validation of Crosswalks Between FIM® and SCIM III for Voluntary Musculoskeletal Movement Functions by Linda A. T. Jones, Chih-Ying Li, David Weitzenkamp, John Steeves, Susie Charlifue and Gale Whiteneck in Neurorehabilitation and Neural Repair
Supplemental Materials
sj-docx-3-nnr-10.1177_15459683211033854 – Supplemental Material for Development and Validation of Crosswalks Between FIM® and SCIM III for Voluntary Musculoskeletal Movement Functions
Supplemental Material, sj-docx-3-nnr-10.1177_15459683211033854 for Development and Validation of Crosswalks Between FIM® and SCIM III for Voluntary Musculoskeletal Movement Functions by Linda A. T. Jones, Chih-Ying Li, David Weitzenkamp, John Steeves, Susie Charlifue and Gale Whiteneck in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgments
The authors would like to thank the RHSCIR network and all the participating local RHSCIR sites: Vancouver General Hospital, GF Strong Rehabilitation Centre, Foothills Hospital, Glenrose Rehabilitation Hospital, Royal Alexandra Hospital, University of Alberta Hospital, Royal University Hospital, Saskatoon City Hospital, Winnipeg Health Sciences Centre, Toronto Western Hospital, Toronto Rehabilitation Institute, St. Michael’s Hospital, Sunnybrook Health Sciences Centre, Hamilton General Hospital, Hamilton Health Sciences Regional Rehabilitation Centre, Victoria Hospital (London), University Hospital (London), Parkwood Hospital (London), The Ottawa Hospital Rehabilitation Centre, The Ottawa Hospital Civic Campus, Hôpital de l’Enfant Jésus, Institut de Réadaptation en Deficience Physique de Quebec, Centre de Réadaptation Lucie-Bruneau, Institut de Réadaptation Gingras-Lindsay-de-Montréal, Hôpital du Sacre Cœur de Montréal, Nova Scotia Rehabilitation Centre, QEII Health Sciences Centre, Saint John Regional Hospital, Stan Cassidy Centre for Rehabilitation, St. John’s Health Sciences Centre, and L.A. Miller Rehabilitation Centre. We also thank John (Kip) Kramer, who identified the need for a FIM®/SCIM III crosswalk, Vanessa Noonan who participated in the expert panel method, and physical and occupational therapists from Magee Rehab, Philadelphia, Pennsylvania, Praxis Spinal Cord Institute and GF Strong in Vancouver, British Columbia, and Shepherd Center in Atlanta, Georgia, who generously donated their time to review and comment on the expert panel crosswalk.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the University of Texas Medical Branch, Center for Large Data Research and Data Sharing in Rehabilitation (sub-award # 18-84411-9). This project is also supported in part by NIH/NCATS Colorado CTSA Grant Number UL1 TR002535. Dr. Li receives grant support from NIH, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and National Center for Medical Rehabilitation Research (K01HD101589) (PI: Li). Contents are the author’s sole responsibility and do not necessarily represent official NIH views. The Rick Hansen Spinal Cord Injury Registry and this work are supported by funding from the Praxis Spinal Cord Institute, Health Canada, Western Economic Diversification Canada, and the Governments of Alberta, British Columbia, Manitoba, and Ontario. For more information about RHSCIR, please visit www.praxisinstitute.org. Neurology data for this research/project were cleaned using the Praxis Spinal Cord Institute’s RHI ISNCSCI Algorithm ![]() . Additional data sources included data from the US-based SCIM III reliability study
7
and a Swiss study comparing FIM® and SCIM III in spinal cord injury, generously supplied by Kim Anderson and Armin Curt, respectively.
. Additional data sources included data from the US-based SCIM III reliability study
7
and a Swiss study comparing FIM® and SCIM III in spinal cord injury, generously supplied by Kim Anderson and Armin Curt, respectively.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.