
Abstract
Background. Spinal cord injury (SCI) patients have respiratory complications because of abdominal muscle weakness and paralysis, which impair the ability to cough. Objective. This study aims to enhance cough in high-level SCI subjects (n = 11, SCI at or above T6) using surface electrical stimulation of the abdominal muscles via 2 pairs of posterolaterally placed electrodes. Methods. From total lung capacity, subjects performed maximum expiratory pressure (MEP) efforts against a closed airway and voluntary cough efforts. Both efforts were performed with and without superimposed trains of electrical stimulation (50 Hz, 1 second) at a submaximal intensity set to evoke a gastric pressure (P ga) of 40 cm H2O at functional residual capacity. Results. In the MEP effort, stimulation increased the maximal P ga (from 21.4 ± 7.0 to 59.0 ± 5.7 cm H2O) and esophageal pressure (P es; 47.2 ± 11.7 to 65.6 ± 13.6 cm H2O). During the cough efforts, stimulation increased P ga (19.5 ± 6.0 to 57.9 ± 7.0 cm H2O) and P es (31.2 ± 8.7 to 56.6 ± 10.5 cm H2O). The increased expiratory pressures during cough efforts with stimulation increased peak expiratory flow (PEF, by 36% ± 5%), mean expiratory flow (by 80% ± 8%), and expired lung volume (by 41% ± 16%). In every subject, superimposed electrical stimulation improved peak expiratory flow during cough efforts (by 0.99 ± 0.12 L/s; range, 0.41-1.80 L/s). Wearing an abdominal binder did not improve stimulated cough flows or pressures. Conclusions. The increases in P ga and PEF with electrical stimulation using the novel posterolateral electrode placement are 2 to 3 times greater than improvements reported in other studies. This suggests that posterolateral electrical stimulation of abdominal muscles is a simple noninvasive way to enhance cough in individuals with SCI.
Introduction
The abdominal muscles are the major expiratory muscles required to cough. The reduced ability to cough after high-level spinal cord injury (SCI) is critical because of the paralysis of abdominal muscles and the reduced ability to cough increase the risk of developing atelectasis and pneumonia. 1,2 Consequently, respiratory complications are the major cause of death in acute SCI.
The current treatments for impaired cough in SCI patients are often expensive, bulky, and do not allow for independent and portable operation. Manual assisted cough is the main treatment used to clear secretions and is normally performed by trained personnel as it is difficult to perform adequately. 3 Mechanical insufflation–exsufflation is another noninvasive method used to clear secretions in patients with respiratory muscle weakness. 4,5 In some cases, it can be operated by the patient but it can also be combined with abdominal compression to enhance expiratory air flow. Electrical stimulation of the abdominal muscles is another potentially useful method to enhance cough in SCI patients. This has been established by comparison of manual assisted coughs and electrically stimulated coughs in SCI patients. 6-8
An effective cough depends on strong contraction of the expiratory muscles, which develop high pleural pressures to produce dynamic compression of the intrathoracic airways, that results in turbulent expiratory airflow. The critical measurements for the purpose of assessing cough are thus gastric pressure and esophageal pressure. However, peak expiratory flow is also relevant, particularly when flow limitation is not yet reached due to low levels of expiratory muscle activation.
There have been several studies of surface electrical stimulation over the anterior abdominal wall near the midline to generate expiratory flow or pressure. 7-14 However, most of these studies have had limited success in producing high enough expiratory pressures for effective cough in SCI subjects. Other studies have used magnetic stimulation over the T10 spinous process to activate the nerve roots (T8-T12) that supply abdominal muscles. 15-21 Despite the success of magnetic stimulation in activating a larger portion of abdominal muscles in able-bodied subjects, the improvement in expiratory flow during coughs in SCI individuals has been only modest, ~10%. 19 Surgically implanted epidural electrodes to stimulate the T9-L1 spinal cord can improve cough markedly after SCI 22,23 ; however, this is likely to be applied in only a limited number of patients.
In a recent study in able-bodied subjects, we have shown that a single surface electrical stimulus to the abdominal muscles from electrodes placed posterolaterally on the torso was 2 to 3 times more effective at producing an abdominal muscle contraction than stimulation over the anterior abdominal wall and was equally good as magnetic stimulation over the T10 spinous process. 24 Therefore, in the current study, we aimed to determine whether stimulation at this new location evoked similar twitch pressures in healthy SCI subjects. We then hypothesized that tetanic stimulation could be used to enhance their voluntary cough. Some of these data have appeared in abstract form. 25,26
Materials and Methods
Studies were performed on 11 healthy subjects with SCI (Table 1). All subjects had weak coughs due to SCI. Selection of subjects was based on a clinical assessment of the neurological impairment level (above the level of T6 according to the American Spinal Injury Association [ASIA] international standards for classification [ASIA impairment scale, or AIS27]; mean ± standard error of the mean [mean ± SEM] time since injury, 9.2 ± 4.1 years; range, 0.3-43.4 years). Subjects gave informed written consent to the procedures as approved by the University of New South Wales Human Research Ethics Committee and conformed to the Declaration of Helsinki. All procedures were well tolerated and no subject developed any spasms.
Subjects were seated in their wheelchairs and breathed through a mouthpiece. Air flow was measured by a pneumotachometer and integrated to give volume. We made measures of lung function including, inspiratory capacity (IC), slow vital capacity (VC), forced vital capacity (FVC), and forced expiratory volume in 1 second (FEV1, Table 1). A gastroesophageal catheter was inserted via the nose with one pressure transducer in the stomach to measure abdominal or gastric pressure (P ga) and the other transducer 20 cm rostrally to measure thoracic or esophageal pressure (P es; CTG-2, Gaeltec Ltd, Dunvegan, UK). All signals were digitized (1401 Plus, CED Limited, Cambridge, UK) and stored on a computer.
Subject Data and Lung Function
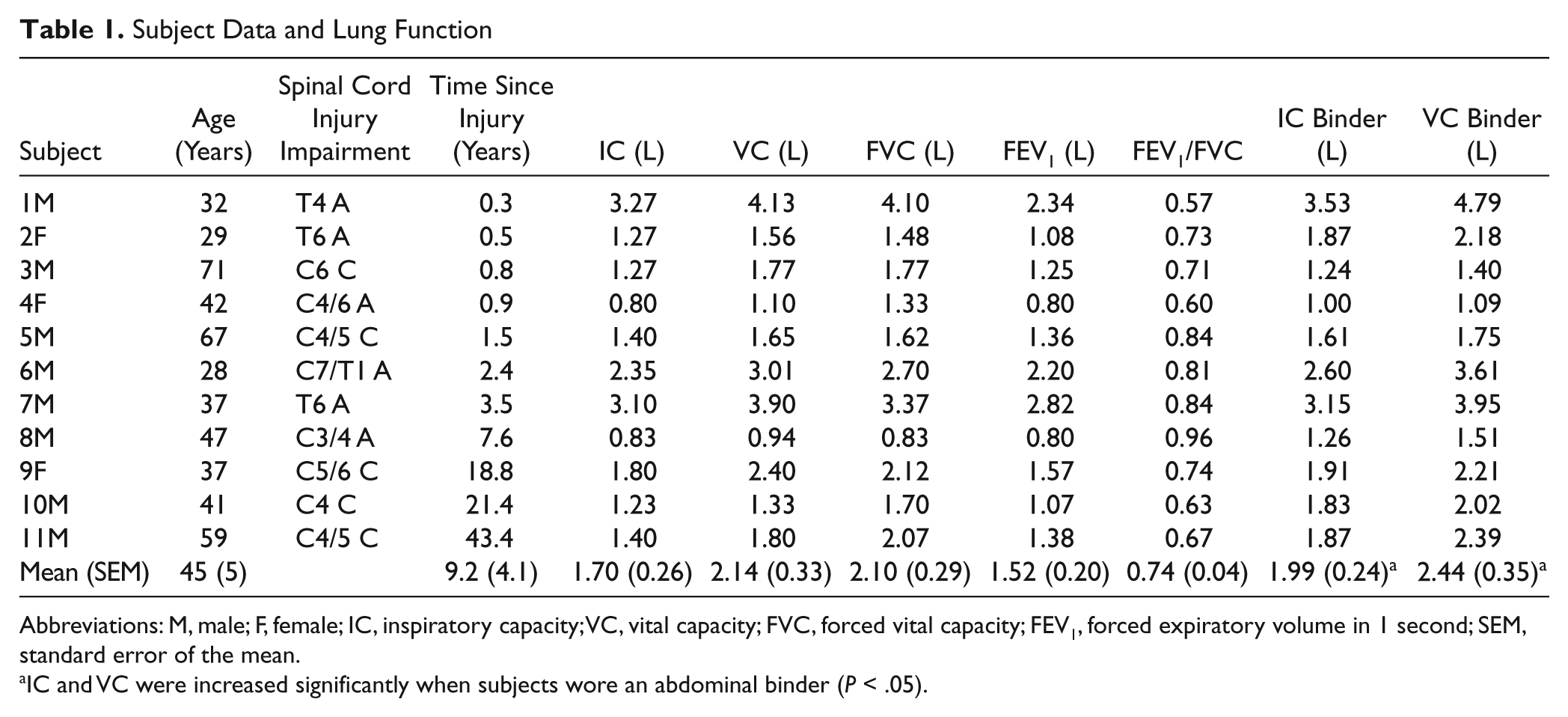
Abbreviations: M, male; F, female; IC, inspiratory capacity; VC, vital capacity; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; SEM, standard error of the mean.
IC and VC were increased significantly when subjects wore an abdominal binder (P < .05).
Stimulation
Electrical stimuli were delivered bilaterally (200-µs pulse width; DS7, Digitimer Co, Hertfordshire, UK) via 2 pairs of high-conductivity gel-skin plate electrodes (4 × 18 cm, Split 1180, 3M HealthCare, St Paul, MN) placed in the posterolateral position on each subject 24 (Figure 1A).
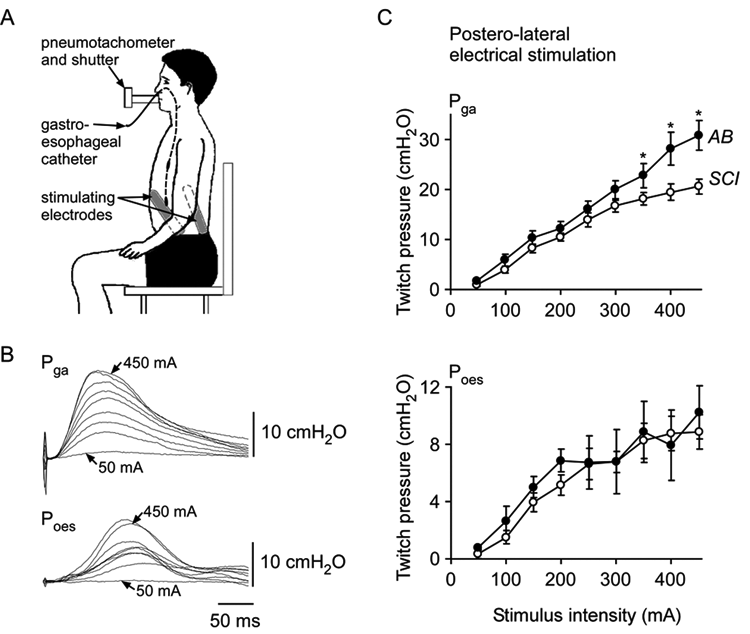
Experimental setup and recruitment of twitch pressure
The recruitment of the abdominal muscles was assessed initially with single stimuli delivered bilaterally at increasing intensities from 50 to 450 mA (50-mA increments) at functional residual capacity (FRC) with the muscles at rest. 24
Trains of 50-Hz stimuli were then applied for 1 second to create a fused contraction of the abdominal muscles. The trains were delivered to the relaxed muscles at FRC, with the aim to increase intensity until the P ga produced was ~40 cm H2O. This intensity was chosen as it was large enough to be effective and increase expiratory flow in the patients but was deliberately relatively low compared with that which produced a maximal pressure twitch. This level was then used as the level for abdominal muscle stimulation for the rest of the experiment. The mean ± SEM stimulus intensity used was 128 ± 15 mA, which produced a mean P ga of 38 ± 4 cm H2O at rest at FRC. This stimulus intensity caused no side effects such as skin redness or burns or signs of autonomic dysreflexia over the course of the study.
Experimental Protocol
First, voluntary maximal expiratory pressure (MEP) efforts (~4-seconds long) against a closed shutter at total lung capacity (TLC) were performed without and then with the train of stimuli (1-second long) superimposed during the voluntary effort. The train (1 second) also was delivered with the subject relaxed at TLC with no voluntary effort (repeated 3 times each).
Second, maximal voluntary coughs were performed on the mouthpiece from TLC without and then with the train of stimuli (1-second long) superimposed on top of the voluntary cough effort (repeated 3 times each). This time the stimuli were delivered at TLC while the glottis was still closed to build up intra-abdominal pressure over 0.2 to 0.3 seconds before the subject voluntarily opened their glottis with the cough expiratory effort. 2 This strategy produced the most effective cough. Subjects were instructed to breathe in to TLC and wait for the stimulus train. As soon as the subjects felt the pressure build up as a result of the stimuli (while their glottis was closed), they were told to cough. For 6 subjects, the trains of stimuli were applied by an experimenter via a computer-controlled stimulator. For 5 subjects (chosen randomly), the stimuli were self-triggered by a switch that the subjects easily learned to operate to time the delivery of the electrical stimuli with their voluntary cough effort. The cough efforts, in which the timing of the stimulation was not optimal (5% to 10% of efforts), were excluded from the analysis and these efforts were then repeated.
Third, an adjustable elastic abdominal binder was fastened firmly around the abdomen (below the rib cage) by Velcro straps. Then, the voluntary cough protocol without and with stimulation was repeated. We also measured the effects of the abdominal binder on IC and slow VC.
Measurements
We measured the peak increase in P ga and P es pressure produced during each of the MEP and cough efforts and the peak expiratory flow, the mean expiratory flow (=volume in liters/duration of cough in seconds), and the total expired volume during the cough and the expired volume in 1 second (FEV1) during the cough. All data are presented as absolute values. However, as there was a large degree of variability between subjects in the baseline measures during voluntary MEP and cough efforts, data are also expressed as relative changes from the baseline (unstimulated) condition in the text.
All statistical comparisons were made on the raw data. A 1-way repeated measures analysis of variance (ANOVA) was used to compare the maximal pressures (P ga and P es) produced during MEP efforts. Paired t tests were used to compare each respiratory variable during the cough efforts and the effect of the abdominal binder. The recruitment of abdominal muscles by single stimuli (50-450 mA) was compared with data from able-bodied control subjects from a previous study 24 using a 2-way ANOVA with Tukey post hoc pairwise comparisons. Data are expressed throughout as mean ± SEM. A P value <.05 was taken to indicate statistical significance.
Results
Resting Twitch Pressures at FRC
As stimulus intensity increased, the twitch pressures (P ga and P es) increased. Figure 1C illustrates the mean (±SEM) increase in gastric and esophageal pressures with the increase in stimulus intensity for the SCI group plotted on the same graph as data from able-bodied subjects from a previous study, which used identical techniques. 24 P ga twitch pressures for the SCI subjects were similar to able-bodied subjects for intensities up to 350 mA but then became smaller for the SCI subjects between 350 and 450 mA (67% of control twitch size at 450 mA). P es twitch pressures were similar across all intensities. Typical P ga and P es twitches across all intensities are shown in Figure 1B. A maximal P ga twitch force was reached in only 5 of the 11 SCI subjects, as judged by a plateau in the relationship between stimulus intensity and the evoked P ga twitch amplitude.
The P es/P ga ratio was similar for SCI subjects and able-bodied subjects (on average 0.43 ± 0.02 and 0.41 ± 0.03 for SCI and control subjects, respectively; nonsignificant). However, at the higher intensities ≥350 mA, the ratio was higher for SCI subjects (0.44 ± 0.01 vs 0.33 ± 0.03, P < .05), suggesting greater transfer of the P ga twitch pressures to the thorax for the SCI subjects at the higher stimulus intensities.
Maximum Expiratory Pressure and Cough Efforts
Trains of electrical stimulation of abdominal muscles superimposed during voluntary MEP efforts improved P ga and P es, and when delivered during voluntary coughs trains increased P ga, P es, peak and mean expiratory flow, and expired lung volume. Figure 2 shows the data for a single SCI subject (subject 5 in Table 1) during MEP and cough efforts with and without electrical stimulation of the abdominal muscles. The increases in all measures as a result of the stimulation are clear. A representative flow–volume loop for another single SCI subject (Figure 3, subject 10 in Table 1) highlights the increase in expiratory flow maintained during the cough and the increased expired volume in the cough when electrical stimulation was applied. Qualitatively, the sound of the stimulated cough was also improved (see the sound file in the supplementary material available online at nnr.sagepub.com/supplemental). Flow–volume loops showed greater expiratory flow at all lung volumes with stimulation in all but one subject (subject 6 in Table 1).
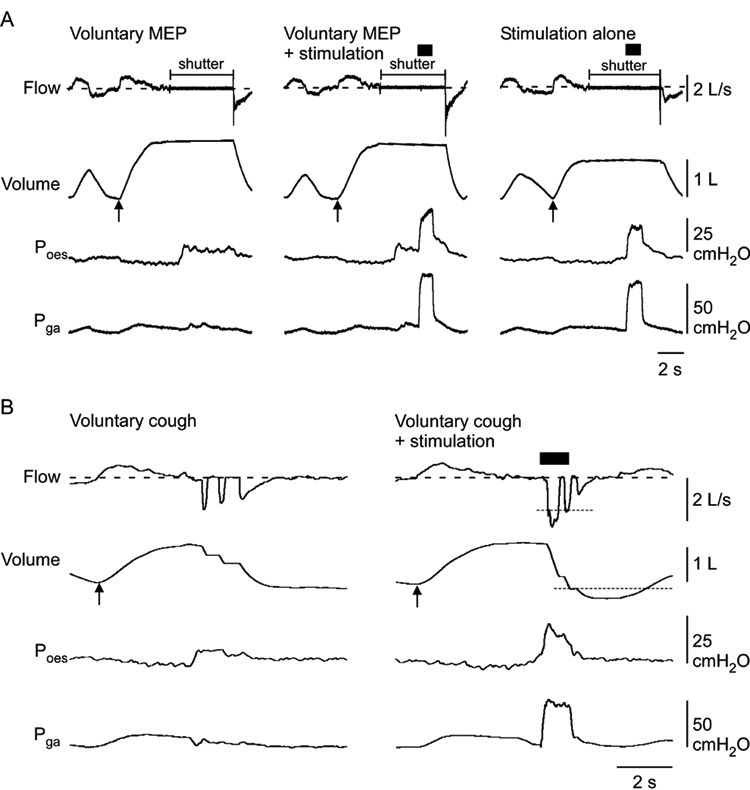
Data from a single SCI subject during MEP and cough efforts
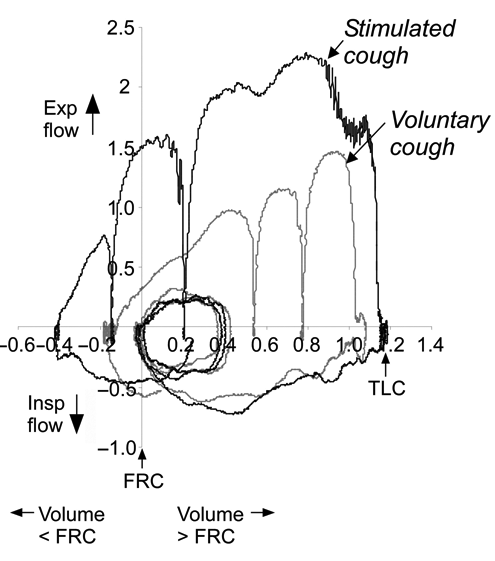
Flow–volume curves for voluntary and stimulated coughs from a single SCI subject
Figure 4 shows the pooled data for the group and the data from each SCI subject during MEP and cough efforts. For MEP efforts, P ga and P es were larger when the abdominal muscles were stimulated. The P ga generated voluntarily was 21.4 ± 7.0 cm H2O, and the P ga produced during voluntary efforts combined with stimulation was 59.0 ± 5.7 cm H2O. The peak P es generated voluntarily was larger than P ga (47.2 ± 11.7 cm H2O). It also increased when voluntary effort was combined with electrical stimulation of the abdominal muscles (65.6 ± 13.6 cm H2O). Across individuals, this represented a 5.6-fold increase in P ga and a 1.6-fold increase in P es (P < .05, see Figure 5A).
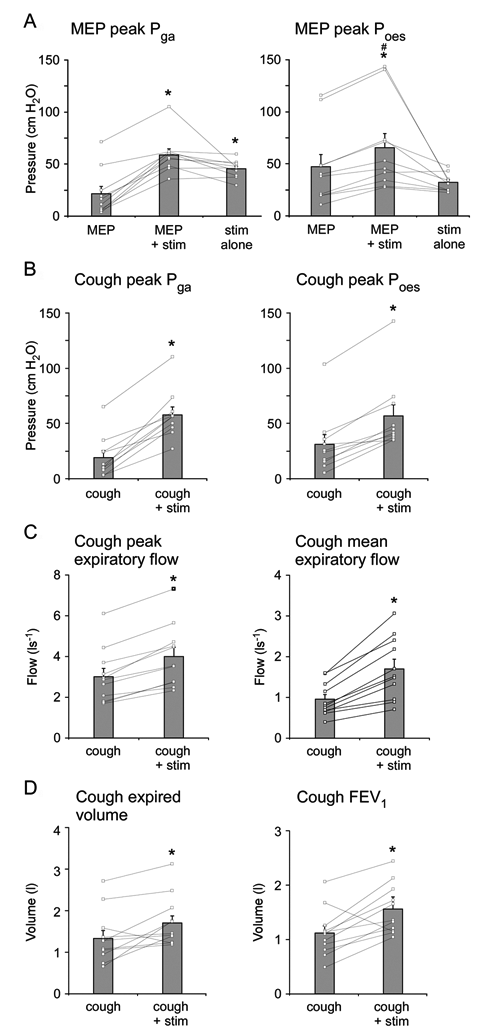
Effects of stimulation on maximum expiratory pressure (MEP) and cough efforts
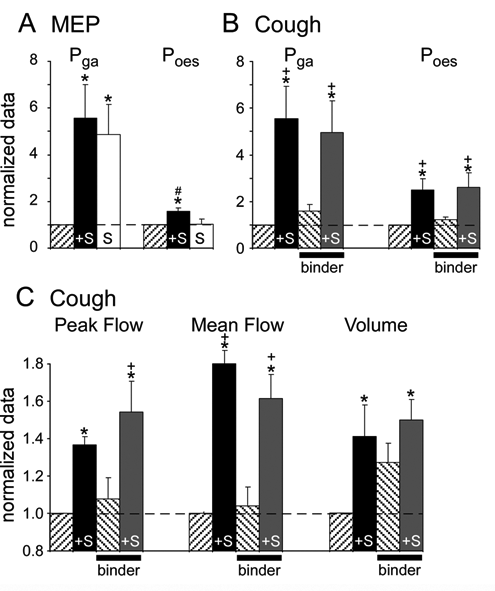
Relative increases in respiratory measures during maximum expiratory pressure (MEP) and cough efforts with application of electrical stimulation and abdominal binder
During the coughs, the stimulation also significantly increased abdominal and thoracic pressures. The P ga generated voluntarily in a cough was 19.5 ± 6.0 cm H2O, and the P ga produced during voluntary coughs combined with stimulation was 57.9 ± 7.0 cm H2O. Stimulation increased P es from 31.2 ± 8.7 to 56.6 ± 10.5 cm H2O. Across individuals, this represented similarly a 5.5-fold increase in P ga and a 2.5-fold increase in P es (P < .05, Figure 5B). The increase in expiratory pressure resulted in increased peak expiratory flow (by 36% ± 5% to 4.00 ± 0.46 L/s), mean expiratory flow (by 80% ± 8% to 1.72 ± 0.23 L/s), expired lung volume (by 41% ± 16% to 1.72 ± 0.18 L), and FEV1 (by 39% ± 12% to 1.58 ± 0.14 L). The relative increases in the expiratory flow and expired volume during cough efforts are shown in Figure 5C.
Abdominal muscle stimulation improved the expiratory pressures (P ga and P es) during the MEP and cough efforts in all 11 subjects (Figure 4). During voluntary coughs with superimposed electrical stimulation, all subjects improved both the peak and mean expiratory flow (by 0.99 ± 0.12 L/s and 0.77 ± 0.12 L/s, respectively), whereas 10 of the 11 subjects increased expired volume and FEV1 (by 0.37 ± 0.13 L and 0.44 ± 0.12 L, respectively) during a cough compared to the voluntary cough without stimulation. One subject decreased expired volumes despite higher expiratory flows because the duration of the cough with stimulation was reduced. There were no differences in any of the improvements in respiratory measures made during the stimulated cough between the 5 subjects who triggered the stimuli themselves and the group of subjects in whom stimuli were triggered by an experimenter.
Effect of Abdominal Binder
The effect of the abdominal binder worn during cough efforts on the expiratory pressures, peak and mean expiratory flow, and expired volume was minimal (Figures 5B and 5C). The aim of the binder was to increase IC and VC. Inspiratory capacity increased by 17% and VC by 14% (P < .05, Table 1), but this did not translate into significantly higher expiratory flows.
Wearing the binder during an unstimulated voluntary cough increased expired volume (by 22%, 1.7 ± 0.2 vs 1.4 ± 0.2 L, P < .05) and abdominal pressure (by 21%, 22.1 ± 5.6 vs 18.6 ± 5.6 cm H2O, P < .05) compared with the values during voluntary unstimulated coughs without the abdominal binder. Peak and mean expiratory flow and P es increased on average but not significantly or consistently. During stimulated coughs, the abdominal binder made no further improvements to any respiratory measures.
The combined effect of electrical stimulation and the abdominal binder on the cough was to increase the P ga and Pes (by 4.9 ± 1.3 times and 2.6 ± 0.6 times, respectively). The peak and mean expiratory flow were increased by 53% ± 16% and 61% ± 13%, respectively, and expired volume increased by 49% ± 11%.
Discussion
The electrical stimulation of abdominal muscles via surface electrodes placed over the torso in the posterolateral position enhances cough in individuals with high-level SCI. Expiratory pressures increased in all subjects on average in the abdomen from ~20 to ~60 cm H2O and 2.5 times in the thorax from ~40 to ~60 cm H2O, resulting in ~1 L/s or 35% increase in peak expiratory flow and an 80% increase in mean expiratory flow. These improvements in the cough are 2 to 3 times greater than other published studies using noninvasive stimulation (see below). The timing of the stimuli to begin after the subject had breathed in to TLC, prior to the voluntary initiation of the cough, optimized the expiratory flows. Subjects were easily able to coordinate the self-triggering of the stimuli and their cough effort.
The recruitment of abdominal muscle force in the SCI subjects, assessed by twitch force, was similar to able-bodied control subjects at all but the highest intensities of stimulation. This suggests similar thresholds for activation of the intercostal nerve fibers despite chronic paralysis in most cases, despite a recent report of reduced axonal excitability post-paralysis for limb nerves. 28 The peak twitch force for abdominal pressure in SCI subjects was only two thirds the size of the peak twitch force in able-bodied control subjects. Although there may be some muscle weakness, 15 the peak twitch force in the current study was not necessarily maximal as we did not stimulate at intensities >450 mA. 24 Alternatively, the reduced twitch pressures at high intensities may reflect reduced stiffness of the abdominal wall because of the absence of any activity in the paralyzed muscles. 29
The transfer of expiratory pressure from the abdomen to the thorax resulted in similar thoracic twitch pressures in SCI and able-bodied control subjects. The P es/P ga ratio was similar across all stimulus intensities. At higher stimulus intensities, however, the ratio was higher for SCI subjects, suggesting that the transfer of pressure from the abdomen to the thorax was more efficient in the SCI subjects. This may reflect altered “passive” properties of the chest wall after SCI such as a decrease in rib cage compliance, 30-32 or alternatively, an increase in diaphragm compliance.
The frequency of stimulation used in this study (50 Hz) was chosen as there is close to full fusion of muscle force in many human skeletal muscles at this frequency, including chronically paralyzed muscles and has been shown to be optimal for abdominal muscles. 23 As judged by the pressure responses, contractions were well fused in this study. The intensity of stimuli used for the tetani was chosen to produce an abdominal pressure of ~40 cm H2O at rest at FRC. This level required a much lower current (128 mA) than the maximal intensity used to produce twitch responses (450 mA), yet it produced a significant increase in abdominal pressure. There is clearly the potential to increase the abdominal pressure produced by surface electrical stimulation to a greater extent than tested here. We predict that this would further improve expiratory flow during a cough. Preliminary observations suggest that flow limitation was not yet reached with the stimulus intensities used here (unpublished observations).
The expiratory pressures produced during maximal expiratory efforts were increased significantly by the addition of the tetanic stimulation of the abdominal muscles. We were unable to measure pressure reliability at the mouth for 2 reasons. First, because of the very weak expiratory pressures developed voluntarily by the SCI subjects, extra pressures developed by cheek muscle contraction (despite measures taken to avoid this) had large effects on the maximal pressures achieved voluntarily. Second, during stimulated contractions, at TLC, the glottis often closed inadvertently 23 in the MEP protocol despite instruction to try to keep the airway open. Inadvertent closure of the glottis did not prevent the initiation of a voluntary cough. Measurement of gastric and esophageal pressures avoids these artifacts.
During cough efforts, expiratory pressures were also significantly increased with superimposed electrical stimulation. This resulted in increased peak expiratory flow and a large improvement in mean expiratory flow for the duration of the cough. The flow–volume loop in Figure 3 shows these improvements in flow as well as in expired volume during the stimulated cough. In addition, another indication of the efficacy of the stimulated cough was its sound: this was markedly improved in all subjects by superimposition of electrical stimulation. Glottic control was never a problem during stimulated coughs and was coordinated easily with the stimulation. The peak expiratory flows during the stimulated coughs improved in all subjects to an average level close to that considered sufficient in otherwise healthy people with neuromuscular disorders, 4.5 L/s. 5 Some subjects in this study reached flows comparable with those in coughs of able-bodied people (>6 L/s). 2 The expiratory flows in the current study could be further enhanced by the application of higher intensity tetanic stimulation. In our laboratory, using the same experimental setup, able-bodied control subjects reached a peak expiratory flow of ~5 L/s with a P ga of ~180 cm H2O and P es of 140 cm H2O during a cough from TLC (unpublished observations).
Here, we show that this posterolateral electrode placement 24 can enhance cough in SCI subjects when 50-Hz trains of stimuli were delivered for 1 second. As mentioned above, we limited our study to stimulus intensities that produced a P ga of only ~40 cm H2O at FRC. Even at this submaximal intensity, which produced <50% maximal twitch pressure, our results compare well with previous studies using both electrical and magnetic stimulation.
In our study, the subjects achieved a 35% increase in peak expiratory flow, compared with a 13% to 18% increase reported in high-level SCI subjects using anterior placement of electrodes over the abdomen. 7,11,33 However, in a study of a single subject, peak expiratory flow increased by 45% with electrical stimulation over the anterior abdominal wall. 13 Other recent studies have combined anterior and lateral stimulating electrodes to enhance the expiratory flow in cough in a small group of patients with SCI by 31% to 54%. 9,10 However, the absolute increases in peak expiratory flows were relatively small (range of increase by 0.04-0.49 L/s), 10 compared with our study in which peak expiratory flow increased by 0.99 ± 0.12 L/s (range, 0.41-1.80 L/s).
Our subjects also showed a greater relative improvement in maximal abdominal pressures during coughs with superimposed electrical stimulation (increased from an average of 21 cm H2O to 60 cm H2O) than in a previous study that used stimulation over the anterior abdominal wall. 8 Here, the maximal expiratory pressure at the mouth increased from 27 to 60 cm H2O. Although the absolute peak pressure values are similar, our measurements of abdominal pressure are free of the artifact caused by pressures produced in the mouth by contraction of the cheeks. Such artifactual pressures do not contribute to expiratory flow in a cough. Abdominal pressures were not measured in any of the other studies using electrical stimulation, and expiratory flow was not measured in the study by Linder. 8
Magnetic pulses delivered over the T10 spinous process have also been used to improve coughs in SCI subjects and have shown increases in peak expiratory flow (by 10% to 5.3 L/s) and maximal expiratory pressure measured at the mouth (by 18% to 66 cm H2O). 19 Some of the studies using magnetic stimulation have also measured abdominal pressure. In SCI subjects, maximal abdominal pressures produced by pairs of magnetic stimuli are about half those produced in able-bodied control subjects (43 cm H2O vs 89 cm H2O, at TLC). 15 Other studies using pairs or trains of magnetic stimuli over T10 in able-bodied subjects have produced abdominal pressures closer to 100 cm H2O. 16,20 Lim et al, 24 showed that the posterolateral electrical stimulation evoked the same size maximal P ga twitches as magnetic stimulation over T10 in able-bodied subjects (both were 2-3 times better than anterior electrical stimulation). Surface electrical stimulation has cost and portability benefits over magnetic stimulation. However, currently most commercially available electrical stimulators have a maximal output of 100 to 130 mA, which may not be sufficient to produce an effective cough in all SCI individuals.
DiMarco et al 22,23 have shown that 50 Hz supramaximal stimulation at sites simultaneously via epidural electrodes over T9, T11, and L1 in SCI subjects can produce large cough expiratory pressures (124-150 cm H2O) and expiratory flows (7.8-8.8 L/s) and can be activated independently by the subject. The advantage of noninvasive surface electrical stimulation over implanted epidural electrodes is that no surgery is required. Surface stimulation might benefit SCI individuals who only occasionally require assistance with coughing. Nevertheless, the option for both effective implanted and surface electrical stimulation to enhance cough is a positive outcome, if the need for manually assisted cough can be reduced. For all forms of abdominal muscle stimulation, co-activation of the diaphragm or other inspiratory muscles either reflexly 34 or by stimulus spread will be counterproductive in enhancing expiratory airflow. 35
The application of an abdominal binder improved IC and VC similar to other studies, 11,36-38 but this did not consistently translate into improved expiratory flow, volume, or pressure during the stimulated coughs. However, it improved the expired volume and expiratory pressures generated during unstimulated voluntary coughs, and therefore may benefit some patients in whom electrical stimulation is contraindicated or who may not tolerate electrical stimulation.
Application of electrical stimulation using surface electrodes in the posterolateral position 24 has successfully enhanced cough in a group of high-level SCI subjects. All subjects in this study had reduced abdominal wall sensation and tolerated the stimulation well. Full abdominal sensation (or hyperesthesia) may limit the suitability of this technique for some subjects. Future studies will be needed to determine the optimal intensity of stimulation to evoke the best cough using this placement of stimulating electrodes. This will need to be tailored to individuals. The long-term aim of this work is to determine the parameters for a cost-effective and portable stimulator that can deliver the required stimulus currents for evoking a functional cough and easily interface with individualized triggering devices to promote functional independence.
Footnotes
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by the NSW Office of Science and Medical Research Spinal Cord Injury Grant Program and the National Health and Medical Research Council of Australia.