
Abstract
High frequency oscillations (HFOs) are being incorporated into the presurgical evaluation of patients with epilepsy and also represent a rapidly evolving field in basic epilepsy research. Animal models have been pivotal in uncovering the mechanisms underlying HFOs and their role in epilepsy. In this review, we provide an overview of HFOs recorded in animal models, highlighting their relevance not only to epilepsy but also to neuropsychiatric and Alzheimer's diseases, suggesting a broader role in brain disorders. Then we explore recent advances, including innovative computational methods for the automated detection and analysis of HFOs. Building on this analysis, we propose guidelines for HFO identification and reporting with translational potential from animal models to humans. Finally, we discuss existing knowledge gaps and outline future directions for research in this rapidly evolving field.
Introduction
High frequency brain oscillations (HFOs), typically faster than 80 Hz, have attracted the interest of neurophysiologists for decades, due to their association with local circuit function. 1 These functions include both normal brain processes such as memory but also pathological ones such as the emergence of seizures. 2 Perhaps one of the first reports of HFOs in humans dates back to 1950 when Lion et al developed and tested a special amplifier to record electroencephalographic (EEG) signals exceeding 200 Hz. 3 They recorded more than 40 apparently normal subjects using scalp EEG electrodes placed over the temporal and occipital regions and showed that ∼200 Hz oscillations up to 70 μV could be recorded.
The link between HFOs and epilepsy was not described until 1999 when Bragin et al recorded fast oscillations intracranially in individuals with epilepsy. 4 They found that electrodes within the epileptogenic region showed striking predominance of pathological HFOs in the 250 to 500 Hz frequency range, the so-called fast ripples. The name was adopted in animal models of temporal lobe epilepsy (TLE), where these fast oscillations resembled physiological ripples (80-250 Hz)—typical characteristics of hippocampal activity during immobility periods and slow-wave sleep. 2 Bragin et al also recorded fast oscillations in lower frequencies such as those within the 80 to 250 Hz range in both epileptogenic and presumably normal regions. 4 Since then, the term “fast ripple” evolved into “HFOs” to integrate observations beyond hippocampal territories. Here we use the term “HFOs” to refer to oscillations below 250 Hz and the term “pathological HFOs” to refer to oscillations greater than 250 Hz, which typically do not occur in the normal hippocampus.2,5 When we refer to both HFOs and pathological ones the term “pathological” appears in parentheses.
The strong link between pathological HFOs and areas that generate seizures gave rise to several studies investigating their role as a promising epilepsy biomarker. 6 Despite seminal inroads into the role of pathological HFOs in epilepsy, key challenges remain. Detecting (pathological) HFOs is not straightforward, especially in light of the lack of formal definition and agreed criteria for their detection. This review provides new vistas on the emerging roles of (pathological) HFOs in brain disease followed by advancements in ways to analyze them. We conclude by proposing guidelines for recording, defining, detecting, and reporting (pathological) HFOs with the goal to further advance their translational potential and reproducibility of findings.
HFOs in Epilepsy
HFOs comprise a wide frequency range that includes frequencies critical to normal brain function such as those within the ripple band (typically from 80 to 250 Hz). 7 However, oscillations faster than normal ripples (e.g., pathological HFOs) are not typically found in normal human and rodent2,5 brain networks and thus their emergence has historically been linked to epilepsy. Soon after the initial reports of pathological HFOs in patients and chronic models of TLE, the formation of pathologically interconnected neuron clusters was proposed as a mechanism of epileptogenesis, 8 with HFOs emerging as a consequence of their hyperexcitable interactions. 9 One of the leading hypothesis regarding the mechanisms underlying pathological HFOs suggests that they reflect the asynchronous or out-of-phase firing of bursting cells giving rise to an event as fast as a pathological HFO.9,10 It is unlikely that a single neuron can give rise to a population event as rapid as a pathological HFO as single neurons do not fire at such high frequencies. TLE animal models like kainic acid- or pilocarpine-induced status epilepticus, with relatively brief “silent” periods and reasonable percentages (25-50%) of animals developing spontaneous seizures, are commonly used to study the development of epilepsy. In these models, pathological HFOs can be detected at sites adjacent to hippocampal injury and/or near to the seizure onset zone in the temporal lobe (Figure 1A 11 ), supporting their pathological nature. In most cases, pathological HFOs occur immediately after the precipitating event and are stable up to the appearance of spontaneous seizures, 12 indicating they could be a biomarker of epileptogenesis, though not temporally specific. Strikingly, co-occurring (pathological) HFOs with different types of EEG spikes progressively increase up to the first occurrence of seizures, 13 suggesting that (pathological) HFOs with EEG spikes are distinct entities from isolated (pathological) HFOs or EEG spikes alone.14,15
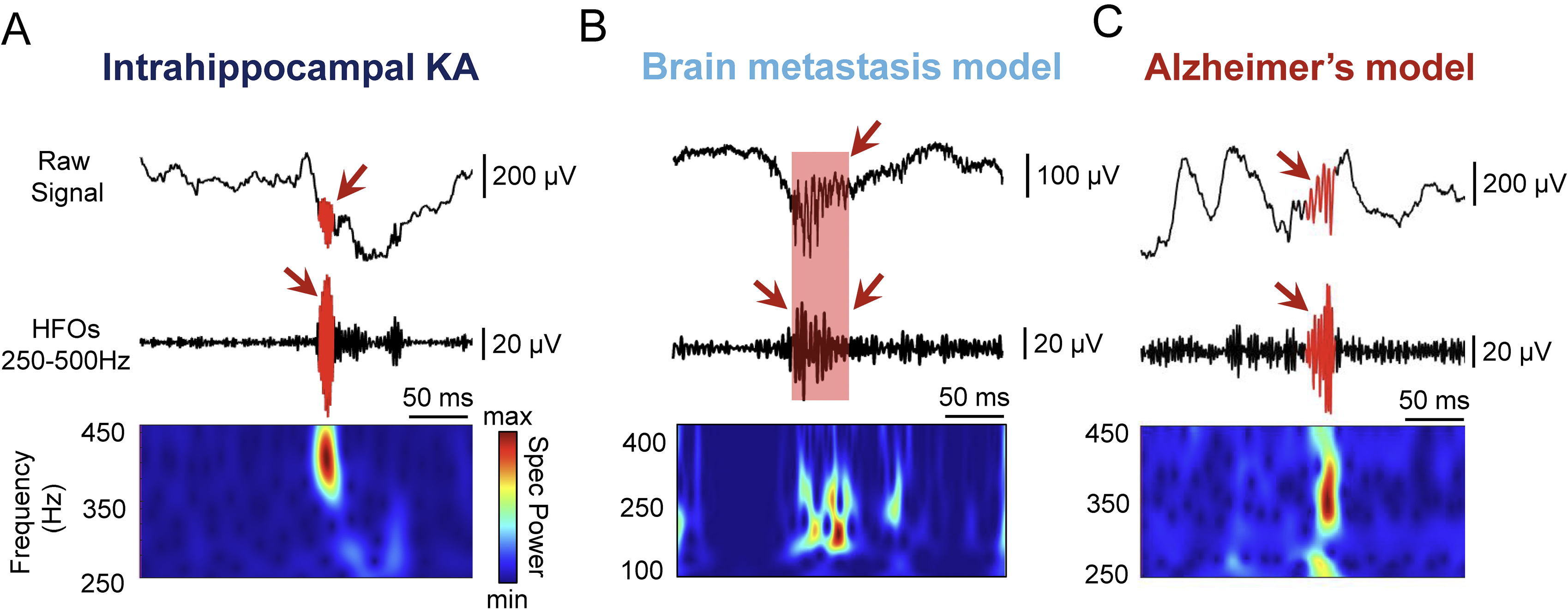
Examples of pathological high frequency oscillations (HFOs) recorded from the hippocampus in different animal models. (A). Pathological HFOs recorded in the intrahippocampal kainic acid (KA) mouse model. 11 The top trace is the raw (unfiltered) local field potential (LFP), the middle trace is the filtered LFP in the 250 to 500 Hz frequency range and the bottom panel shows a spectrogram of the filtered LFP. Warm colors denote increased power for a certain frequency. (B). Pathological HFOs recorded from the CA1 region of the hippocampus in an animal model of brain metastasis from melanoma cancer cells (B16/F10-BrM). 18 Data recorded by A. Sanchez-Aguilera. The top trace is the unfiltered LFP, the middle trace is the filtered LFP in the 100 to 400 Hz frequency range and the respective spectrogram is shown at the bottom. (C). Pathological HFOs recorded from the dentate gyrus of the Tg2576 mouse model of cerebral amyloid overexpression simulating Alzheimer's disease. 24 The top and middle traces as well as filter settings are the same as in Panel A.
HFOs in Other Neurological Conditions
Apart from TLE, changes in (pathological) HFOs have been described in other conditions typically associated with epileptogenesis, such as in experimental models of developmental cortical malformations,16,17 traumatic brain injury, 12 and in models of brain metastasis 18 (Figure 1B). In these models, changes are not unique to the high-frequency band but they also affect slow oscillations, such as delta oscillations (1-4 Hz) or those below 1 Hz. It has been proposed that coupling between the amplitude of fast oscillations and the phase of the slow waves can help distinguish physiologic and pathologic HFOs. 19 Moreover, the repeated occurrence of sleep slow waves coupled with pathological HFOs could fortify the formation of remote pathological circuits,20,21 as could the repeated bombardment of (pathological) HFOs during subsequent seizures. 22 Feature analysis of multidimensional interactions between frequency bands may help predict progression of these diseases, as recently suggested. 18
HFOs in Alzheimer's Disease
Ripples are critical to memory formation, and their selective disruption has been linked to memory deficits. 2 In this context, fewer ripples and reduced gamma oscillations have been correlated with memory performance in mouse models simulating Alzheimer's disease (AD). 23 Strikingly, hippocampal and cortical fast ripples were found to occur in three mouse lines with AD features 24 (Figure 1C). Notably, they occurred primarily during slow wave sleep similar to pathological HFOs occurring in epilepsy. 25 They emerged well before overt AD-related neuropathology developed (ie, amyloid-β plaques) and at an age when mice did not show impaired memory, 24 supporting the idea that HFOs emerge early during the AD continuum and could be used as biomarker. The presence of pathological HFOs in the hippocampus of both AD and epilepsy models suggests shared microcircuit alterations. 26
HFOs in Schizophrenia
Oscillatory disturbances have also been identified in the context of schizophrenia. For example, reductions in frontal cortex beta (12-30 Hz) and gamma (30-80 Hz) oscillations were found in responses to auditory stimuli in a mouse model. 27 Another study identified spontaneous HFOs in the frequency range of 130 to 180 Hz in nucleus accumbens of a neurodevelopmental rat model of schizophrenia. 28 In these models altered oscillations in the gamma and fast ripple bands were mostly associated with N-methyl-D-aspartate receptor hypofunction. 29
Advancements in Detection and Analyses of HFOs
As (pathological) HFOs consolidate as a biomarker in different preclinical models of neurological conditions, new methods are required for their detection and analysis. Given the burden and difficulties of manual detection, automatic methods have emerged as a prominent research area. Typically, raw data undergoes preprocessing and transformation using various techniques, such as bandpass filtering, root-mean-square (RMS) analysis, Fourier transforms, or wavelet transforms. Candidate events are then identified by applying amplitude thresholds to the transformed signal (Table 1, thresholding approaches). However, such thresholding approaches are prone to artifact contamination and exhibit poor reproducibility largely because a unified threshold is challenging to determine or extrapolate across different studies.
Automatic detection and analysis of HFOs.
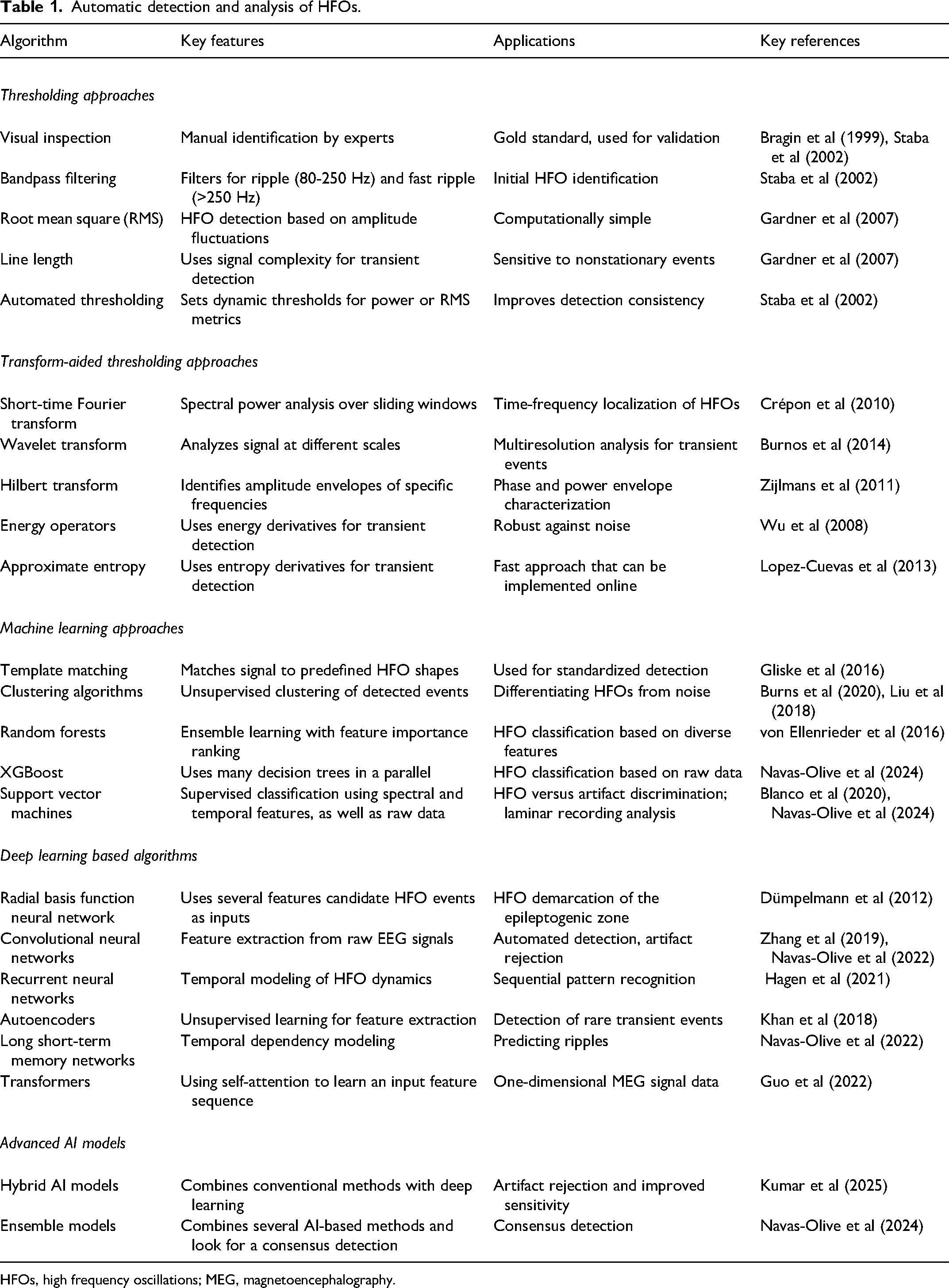
HFOs, high frequency oscillations; MEG, magnetoencephalography.
To address these limitations, researchers have developed enhanced signal processing techniques. For example, Zelmann et al 30 refined the RMS detector by deriving energy thresholds from baseline segments, while Ren et al 31 introduced the method of maximum distributed peak points to enhance baseline accuracy. Chaibi et al 32 further advanced detection by combining RMS analysis with empirical mode decomposition.
Another strategy was leveraging transformations that enhance the localization and analysis of transient events (Table 1, transform-aided thresholding approaches). For example, the Short-Time Fourier Transform applies spectral power analysis over sliding windows, providing time-frequency localization of (pathological) HFOs, as demonstrated by Crépon et al. 33 Similarly, wavelet transforms offer multiresolution analysis by analyzing signals across different scales, making them particularly effective for transient event detection. 34 Other methods emphasize amplitude and phase characterization, like the Hilbert Transform for identifying amplitude envelopes and phases, 35 or entropy-based approaches for detecting transient irregularities. 36
An important development was the use of expert-annotated datasets to establish consensus criteria for differentiating HFOs from other oscillations. 2 This permitted the implementation of template matching and clustering strategies based on the features of bona fide HFO events. 2 For example, Jrad et al 37 constructed a relevant feature vector based on energy ratios (calculated using Wavelet Transform in predefined frequency bands) to train a multiclass linear discriminant analysis. This marked a shift toward machine learning approaches (Table 1, machine learning approaches), which refers to relatively simple algorithms such as Random Forest, XGBoost or multiple decision trees.19,38 Support vector machines have also been used for supervised classification, aiding in HFO versus artifact discrimination and laminar recording analysis.38,39
Recently, deep learning was introduced to the detection of (pathological) HFOs (Table 1, deep learning based algorithms). A notable advantage of these methods is their capacity to identify abstracted features, facilitating generalization beyond human-defined parameters. One of the earlier attempts was by Dümpelmann et al, 40 who used power, line-length, and the instantaneous frequency as input features for a radial basis function neural network. Recent studies have applied advanced architectures such as convolutional neural networks, which enable feature extraction from raw EEG to improve sensitivity and specificity for detecting ripples and fast ripples.41,42 Recurrent neural networks model temporal dynamics, enhancing pattern recognition in HFOs, 43 while Autoencoders allow identifying rare HFO events. 44 Finally, transformers have been successful in analyzing magnetoencephalography signals, 45 offering significant improvements in detection accuracy.
Finally, hybrid and ensemble AI models have been applied to enhance HFO detection (Table 1, advanced AI models). Hybrid models integrate conventional methods with deep learning techniques, improving artifact rejection and sensitivity. For instance, Kumar et al 46 developed a hybrid model that combined traditional signal processing with deep learning algorithms. Navas-Olive et al 38 demonstrated that ensemble approaches, by aggregating the strengths of various models, can enhance detection accuracy and robustness. These innovative AI strategies have significantly advanced the field, offering more accurate and efficient methods for (pathological) HFO detection and analysis.
Guidelines to Identify and Report HFOs
Identifying HFOs (Record, Define, Report)
One of the main starting points when studying (pathological) HFOs is the careful consideration of signal acquisition parameters. Therefore, any proper recording of HFOs should take into account several key aspects, which we discuss below. First, it is important to ensure that the sampling rate of the amplifier is set high enough to be able to record fast events (Figure 2, Reporting). Specifically, recording of ripples (80-250 Hz) would require a sampling rate of at least 1000 Hz, while fast ripples (250-500 Hz) would benefit from sampling of at least 2000 Hz. 47 Very fast HFOs, such as those exceeding 1000 Hz, would require sampling above 5000 Hz. 47 Moreover, hardware or software filters used during acquisition are critical as they can screen out (pathological) HFOs. 48 As an example, recording of fast ripples would benefit from using a low pass of 500 Hz and a high pass of 0.5 to 1 Hz, although the latter is less critical. Reporting additional information (Figure 2, Bonus) such as electrode type, impedance and reference montage details will help ensure reproducibility across studies.
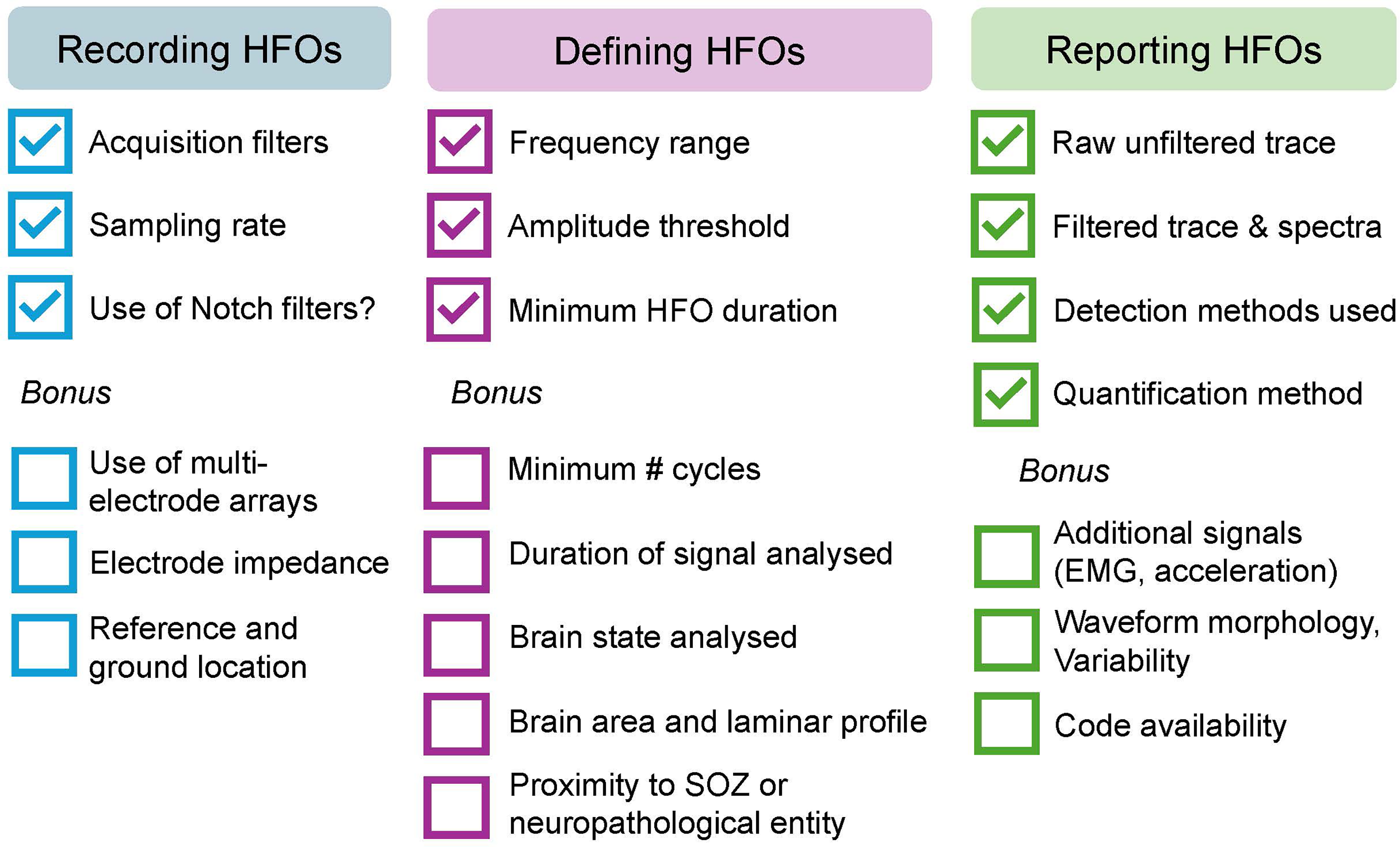
Proposed guidelines for recording, defining and reporting (pathological) high frequency oscillations (HFOs). Recording of (pathological) HFOs could include information about acquisition filters, sampling rate and whether a Notch filter was used during recording. Additional factors that would benefit (pathological) HFO recording are the use of multielectrode arrays of high impedance values and appropiate reference and ground montage. Defining (pathological) HFOs requires using the appropriate frequency range, amplitude threshold and minimum event duration for their detection. It would also be beneficial to report the minimum number of cycles, duration of signal analyzed, brain state and area, as well as proximity to seizure onset zone (SOZ) or known neuropathology. Reporting of (pathological) HFOs could include a representative example of unfiltered and filtered traces, spectrograms and detection methods used. The inclusion of additional signals such as EMG and acceleration is a bonus. Moreover, HFO waveform morphology and variability would be beneficial for inferring mechanistic information. Lastly, the code used for detection and analyses of (pathological) HFOs could be shared along with executable notebooks to promote reproducibility.
Defining and detecting (pathological) HFOs have inherent challenges, as previously discussed. We propose that when (pathological) HFOs are defined, the minimum reporting should include the frequency range, amplitude threshold, and minimum duration used to differentiate them from background oscillatory activity (Figure 2, Defining). Additionally, the minimum number of cycles and the duration of signal analyzed should also be reported. In this context, analysis of prolonged duration signals is beneficial as event rates may vary in time and space. 49 Moreover, brain state is a major modulator of (pathological) HFOs, which are more robust during slow wave sleep. 25 It is also advisable to report the time before and after the last seizure, given their influence on (pathological) HFO rates.
Reporting HFOs
Recognizing (pathological) HFOs in electrographic signals can be challenging, as some may be invisible in raw data, requiring filtering to isolate frequencies of interest. For proper reporting (Figure 2, Reporting), we encourage investigators to show the raw (unfiltered) trace used for detection alongside filtered traces and spectrograms in the relevant frequency range, as shown in Figure 1. These practices are valuable for distinguishing (pathological) HFOs from artifactual events, as artifacts typically exhibit a candlelight-like appearance in the time-frequency domain, 50 while (pathological) HFOs show a more confined frequency pattern. Moreover, the quantification method used should also be reported (Figure 2). As an example, reporting on whether the rates of (pathological) HFOs were calculated per individual channel or all detected events in all available channels is important. Event rates within or outside an area of interest (e.g., epileptogenic lesion) can also be insightful and reporting is encouraged. Lastly, relationships between (pathological) HFOs and epileptiform events such as co-occurrence of (pathological) HFOs with interictal spikes11,13–15,24 are important to be reported as they may represent distinct pathophysiological entities.
Reporting the variability across candidate (pathological) HFO events may also help to separate them from interictal discharges, artifacts and noise. 51 Moreover, variations in the expression of spectral features are informative of the underlying mechanisms.52,53 For example, different correlations between the event entropy and a fast ripple index can help to disambiguate pathological HFOs that occur under different circumstances. Specifically, “pure” HFOs such as those occurring due to in-phase firing of synchronously bursting cells or “emergent” HFOs that occur as a result of out-of-phase firing of asynchronously bursting cells from interacting epileptogenic territories 9 could be separated, thereby disclosing different mechanistic insights. Variations in the HFO waveforms across a continuum can also be informative on the contribution of different input pathways, as recently shown for ripples. 53
We encourage detailed reporting of the detection methods used (Figure 2). Whenever possible, it is recommended to give access to codes and an executable notebook to run at least a subset of data to help the community test the different approaches and to compare results across labs. Finally, the use and analysis of additional signals that monitor movement would be beneficial in determining sources of noise such as electromyography artifacts caused by abrupt movements.
Conclusions and Future Directions
The role of (pathological) HFOs in various brain disorders may be wider than previously thought. More research is warranted to advance our understanding. The development of automated tools and machine learning algorithms represent important advances that significantly reduce the burden on manual review, which is time consuming and prone to errors. Thus, further development of automated tools is encouraged, especially when multidisciplinary teams are involved. Lastly, we propose that minimal reporting standards will greatly enhance the reproducibility of findings across laboratories and significantly enhance the translational value of (pathological) HFOs.
Footnotes
Acknowledgments
This article is an output of the Third International Workshop on High Frequency Oscillations in Epilepsy held in New York City in May 2024. The workshop was supported by a Research and Training Grant from the American Epilepsy Society, a CURE Epilepsy Workshop Grant, and funds from DIXI, AVrioMedTech, NYU FACES and NYU Comprehensive Epilepsy Center, NATUS, Ad-Tech, Brain Products and Brain Vision, Nihon Khoden, Neurosoft Bioelectronics, and RWD. The authors would like to thank the members of the organising committee of the Third International Workshop on High Frequency Oscillations in Epilepsy for their feedback on the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute of Neurological Disorders and Stroke, National Institute on Aging, Spanish Ministry of Science, Christina Louise George Trust (Grant Nos. 2RF1033310, R01NS106957, R01NS127524, R21AG086880, and PID2021-124829NB-I00).