
Abstract
Introduction:
This study was conducted to assess the biosafety knowledge among laboratory staff working in Morocco.
Methods:
A cross-sectional study was conducted among all laboratory staff in public and private clinical diagnostic and research laboratories between December 5, 2018, and January 5, 2018. Data were collected using a self-administered questionnaire distributed via Google Form.
Results:
A total of 235 participants completed the study questionnaire with an estimated response rate of 19%. Overall, 79% of respondents had a high or intermediate level of knowledge. Only 17.4% had participated in prior formal biosafety training courses. The level of knowledge did not differ significantly with gender or activity sector, but it increased with work experience. Knowledge was generally intermediate for signage and principles of biosafety levels (42.1%), low for distinction between technical operations that could pose a risk by generating aerosols (30.2%), and high for wearing personal protective equipment and its components (92.8%). There was a very high level of knowledge on proper waste sorting (100%).
Conclusion:
These findings underline the need for establishing a biosafety policy and strengthening biosafety training programs in laboratories in Morocco.
Biosafety is a discipline that focuses on the safe handling and containment of infectious microorganisms and hazardous biological materials. 1 It is an important issue in laboratory settings worldwide and can be especially challenging for developing countries. 2 In recent years, research on infectious pathogens has been on the rise due to the emergence and reemergence of new and previously identified infectious agents and diseases. 3 Since the emergence of avian influenza and Middle East respiratory syndrome (MERS) coronavirus, Morocco has made a significant effort in the implementation of biosafety procedures and equipment in health care facilities, as well as training programs among health workers for individual and collective protection rules. 4
Despite these efforts, we have observed in the public Laboratoire de Recherche et de Biosécurité–P3 (Biosafety Level 3) in Morocco that there is a discrepancy between experienced workers and recent graduates of educational institutions. Since laboratory workers often do not receive formal biosafety training courses throughout their academic career, recent graduates appear to have little knowledge or perception of the risk of infection, and most do not conform to the basic principles of universal precautions. Biosafety training is provided in the Laboratoire de Rcherche et de Biosécurité–P3 in Morocco, and it has been observed that over time, the new graduates adapt and begin to follow some of the practices of the more experienced workers who have obtained biosafety training.
According to the Moroccan government and the Moroccan Union of Biological Pharmacists, there are 425 research, private, and public medical diagnostic laboratories in Morocco (2017), and we estimate that 5100 people are employed in these facilities.5,6 These workers can be medical or scientific biologists, researchers, laboratory technicians, or surface technicians. Both groups are important populations in terms of safety and compliance.
If adequate preventive protective measures are not taken, laboratory workers can be exposed to a large pool of specimens from patients with infections such as human immunodeficiency virus (HIV), hepatitis B virus, and other blood-borne pathogens.7,8 Universal precautions should be observed by these workers since blood and some body fluids of all patients are considered potentially infectious. 9 These workers may handle pathogenic microorganisms categorized in risk groups that require level 3 facilities, and therefore they need to follow precautions commensurate with the hazards.
It has been demonstrated that a thorough knowledge of the risks involved in handling microorganisms and the adoption of measures to minimize risks leads to an improvement in the prevention of occupational risks of pathogen transmission. 10
There is a scarcity of data in Morocco about the level of knowledge of, awareness of, and compliance to standard biosafety precautions among laboratory staff. The purpose of this study was therefore to assess the level of knowledge about biosafety precautions among laboratory workers in private and public medical and research laboratories in Morocco.
Materials and Methods
Study Setting and Design
A cross-sectional study 11 was conducted online by using Google forms 12 to solicit responses from public- and private-sector laboratories in the kingdom of Morocco. The sample size formula (n = Z2 p (1 – p) / d2) for field studies according to Thrusfield 13 was used to obtain the target sample size. This gave a minimum sample size of 96 respondents.
To increase engagement, we asked for collaboration from 2 biologists’ associations and 1 biosafety association in Morocco, and we advocated the snowball sampling method. 14 This is a chain referral process in which respondents were asked to recommend other biologists until the desired sample size was reached or exceeded. The snowball sampling method is used for obtaining responses when it may be hard to locate enough subjects to perform the study. The disadvantage to this method is that there may be selection bias, since respondents may refer individuals who are in the same institution or follow the same practices. However, in view of the limited responses, this method was deemed as appropriate.
Questionnaire Design and Implementation
A structured, anonymized self-administered questionnaire was sent to the directors of medical diagnostic laboratories through the Moroccan Association of Medical Biology (http://www.ambmmaroc.net), the Moroccan Society of Medical Microbiology (http://smamm.ma/), and Moroccan Association of Biosafety (http://www.ambs-maroc.com/). The letter stated that only confirmed laboratory workers directly involved in medical diagnostics or microbiology research could participate in the study. Data collection lasted 1 month, from December 5, 2017, to January 5, 2018.
The information sought included sociodemographic characteristics such as age, sex, participant’s occupation, length of work experience, and issues related to their knowledge about biohazards and biosafety concepts. The questions tested knowledge of (a) pathogen risk groups and biosafety levels (5 questions), (b) equipment and personal protective equipment (PPE; 5 questions), (c) risky behaviors (2 questions), (d) the use of disinfectant and antiseptic solutions (2 questions), (e) waste transport and disposal (2 questions), and (f) the safe transport of biohazardous materials with infectious potential (1 question). The questionnaire was developed on the basis of available standard texts about biosafety facilities and universal precautions from third edition of the Laboratory Biosafety Manual by the World Health Organization (WHO) 15 and the fifth edition of the Biosafety in Microbiological and Biomedical Laboratories by the Centers for Disease Control and Prevention (CDC). 1 Ranking of priority pathogens according to risk group and select agent status was performed according to the ABSA International website. 16
The questionnaire was approved by 3 biosafety officials working in 3 different laboratories and pretested on 5 researchers in the laboratory of research and biosafety of Rabat.
Data Management and Statistical Analysis
All returned questionnaires were analyzed with a computer using SPSS version 17.0 software (SPSS, Inc, an IBM Company, Chicago, Illinois). Both descriptive and inferential statistics were computed. The level of significance was set at P < .05.
A numeric scoring system was developed to assess general biosafety knowledge. Since most of the questions were multiple choice and checkbox type, the workers’ responses had to be transformed into “correct = 1” or “incorrect = 0.” For others, the answer was scored as “high = 2,” “intermediate = 1,” or “low = 0.” For example, the answer to the question regarding which biosafety containment level to adopt for the handling of multidrug-resistant strains of Mycobacterium tuberculosis would be “1” if the worker responded “BSL-3” and “0” if he or she responded by another level or if he or she checked the box “I do not know.” To the question, “Which of the following manipulations are aerosol generating?” the proposed answers were “homogenization,” “lyophilization,” “incineration,” “centrifugation,” and “sedimentation.” Each correct checkbox was scored “1” and each incorrect checkbox was scored “–1.” The score of the question was the sum of the scores, and 3 levels were defined: “–3 to –1” for “low,” 0 to 1 for “intermediate,” and 2 to 3 for “high,” respectively.
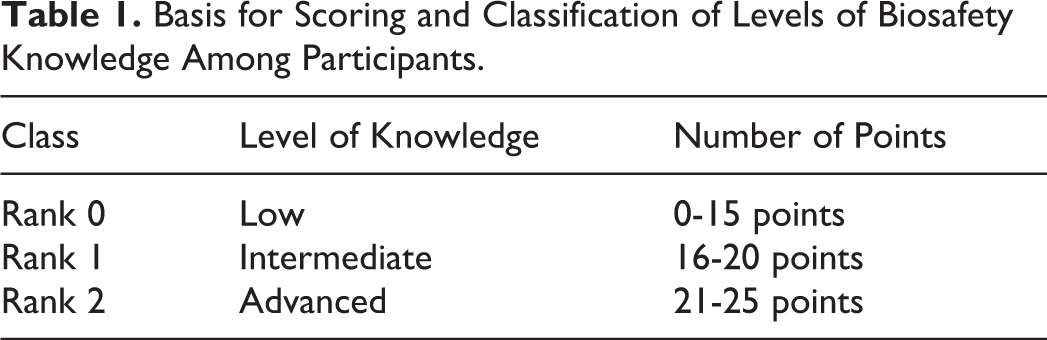
Each of the 18 questions was scored from 0 to 3 according to its importance. The participants received an overall score ranging from 0 to 25 points. The highest score was given to the participants who accumulated the most correct answers. After discussion with biosafety officials and the overall statistical analysis of the distribution of scores, a system was defined for scoring and classifying biosafety knowledge levels among participants according to Table 1.
Basis for Scoring and Classification of Levels of Biosafety Knowledge Among Participants.
Results
Response Rate
This study was conducted in clinical microbiology and research laboratories throughout the kingdom of Morocco. In total, 139 private laboratories and 65 public laboratories were contacted, with an approximate total of 1220 workers involved. A total of 235 workers returned the questionnaire, giving a response rate of 19%.
Sociodemographic Characteristics of the Participants
The demographic information for the respondents is presented in Table 2. The respondents were mostly from the public sector 73% (n = 171), with 27% (n = 64) of workers in private laboratories. The mean value for work experience was 17.2 ± 3.3 years, and 45.1% (n = 106) of the participants had worked less than 5 years. They were predominantly females (58%, n = 137) with a ratio of males to females of 0.75. The mean age was 37.6 ± 7.5 years, and 60% (n = 141) were older than 36 years.
Demographic Distribution and Characteristics of Biologists, Researchers, and Technicians Participating in the Survey (N = 235).
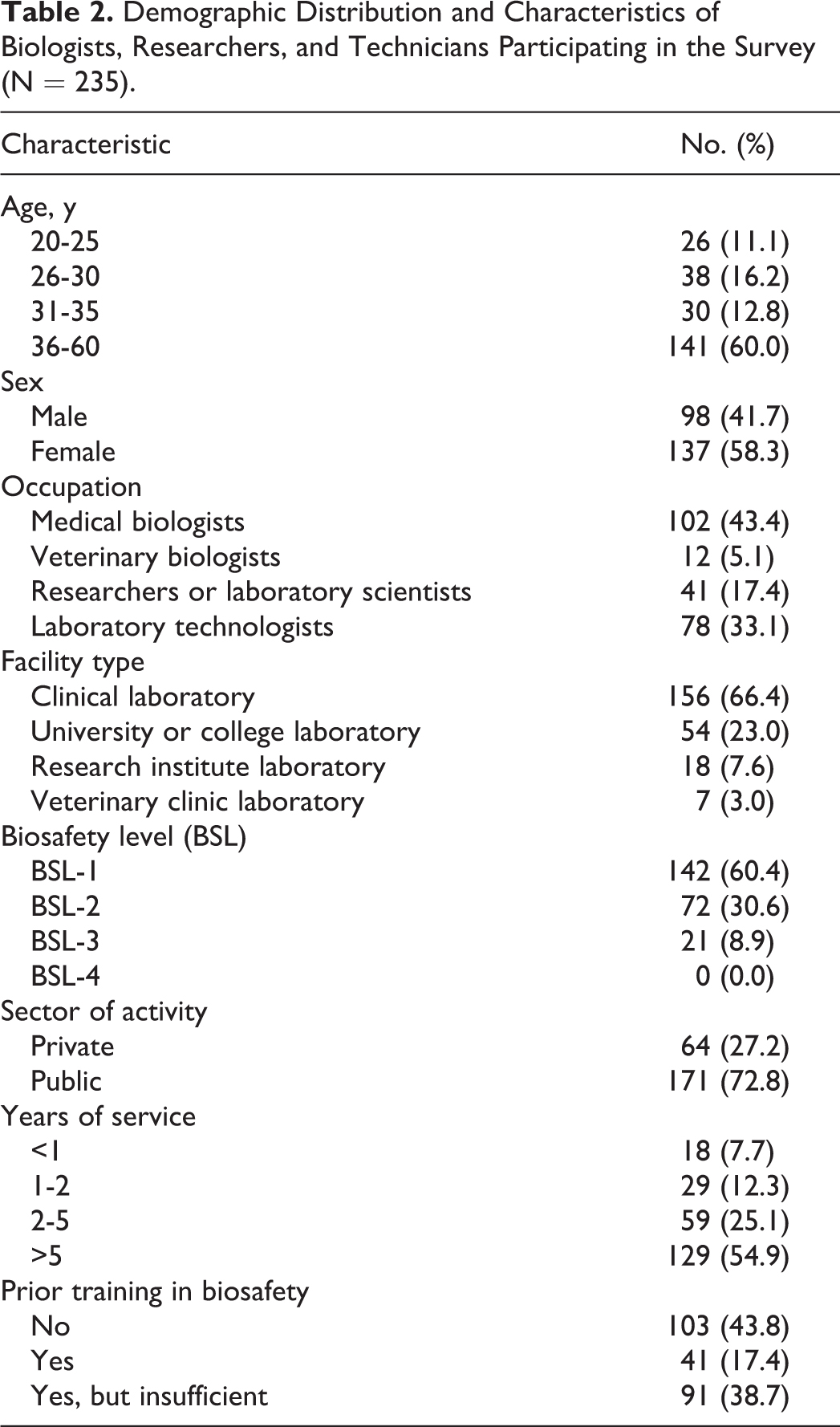
Most respondents were medical biologists (43.4%, n = 102), followed by medical laboratory technicians (33.1%, n = 78) (Table 2). Respondents’ facilities were represented in all categories, although those working in clinical laboratories composed the greatest proportion (66.4%, n = 156).
Global Knowledge of Biosafety with Regard to Participants
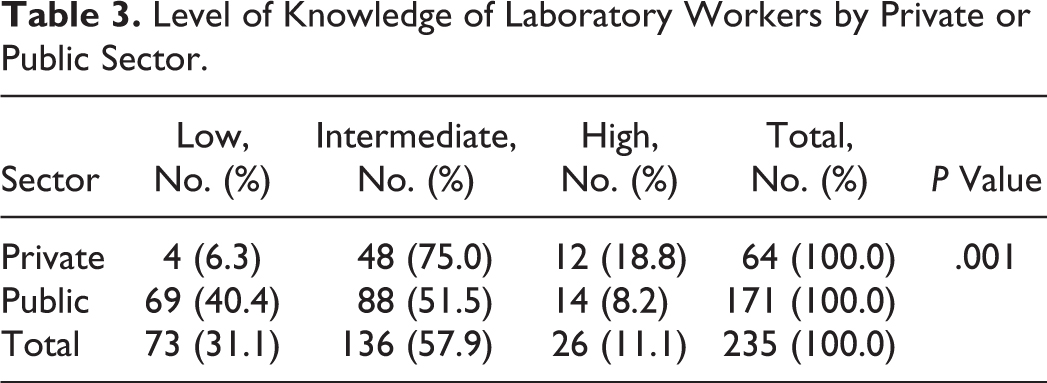
General knowledge scores (average of private- and public-sector labs) ranged from 7 to 24 points. These scores were normally distributed with a mean of 18.7 ± 2.9. Overall, a majority (57.9%, n = 136) of the respondents had intermediate knowledge scores, but those with higher knowledge levels were predominantly in the private sector (18.8%) compared to respondents in the public sector (8.2%) (Table 3).
Level of Knowledge of Laboratory Workers by Private or Public Sector.
Most of the participants recognized that the relationship between science and safety is very strong (76.2%, n = 179) despite the fact that only 15.7% (n = 37) of respondents felt that they have an advanced level of knowledge in biosafety when they self-assessed their knowledge (Table 4), and only 17.4% (n = 41) had benefited from prior training courses or seminars specifically oriented to biosafety (Table 2).
Self-Assessment of Biosafety Knowledge According to Respondents.
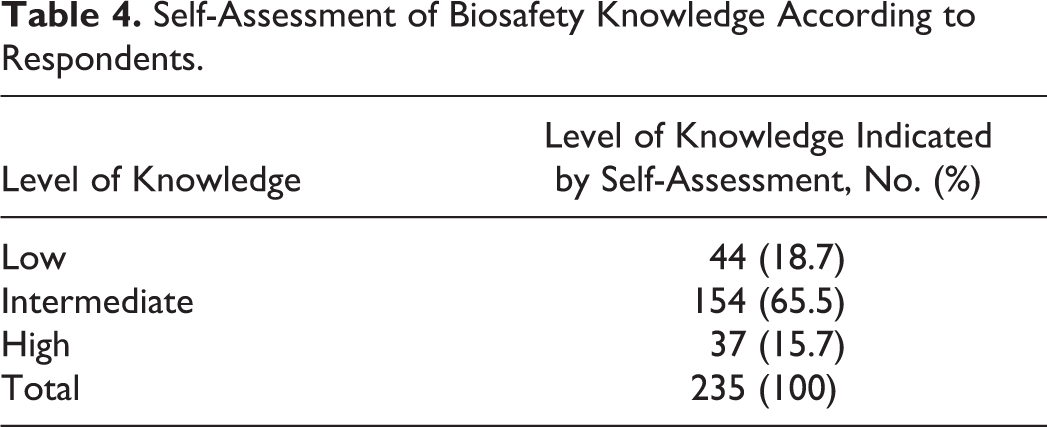
The overall analysis of our resulting data showed that only 11.1% (n = 26) of respondents had a high level of knowledge in biosafety while 57.9% (n = 136) showed an intermediate level (Table 3). This same analysis showed a statistically significant difference between the low and the intermediate self-estimated levels and the level determined by the analysis (P < .005). But among individuals who indicated that they have a high level of knowledge, only 37.8% were correct in this assessment when their responses were evaluated (Table 4).
Table 5 shows the levels of knowledge according to other characteristics of the participants. Knowledge levels did not differ significantly with gender or the activity sector, but they increased with work experience. Biologists, researchers, and technicians had a predominantly intermediate level while there was a slight predominance of a high level of knowledge among medical biologists (17.2%). Regardless of whether or not the respondents had received prior biosafety training, their prevailing knowledge level was mostly intermediate, while a small percentage of respondents with prior biosafety training showed a high level of knowledge (24.4%).
Actual Level of Knowledge as Measured by Respondent Answers to the Questionnaire and Significant Differences of Knowledge Among Categories of Participants.
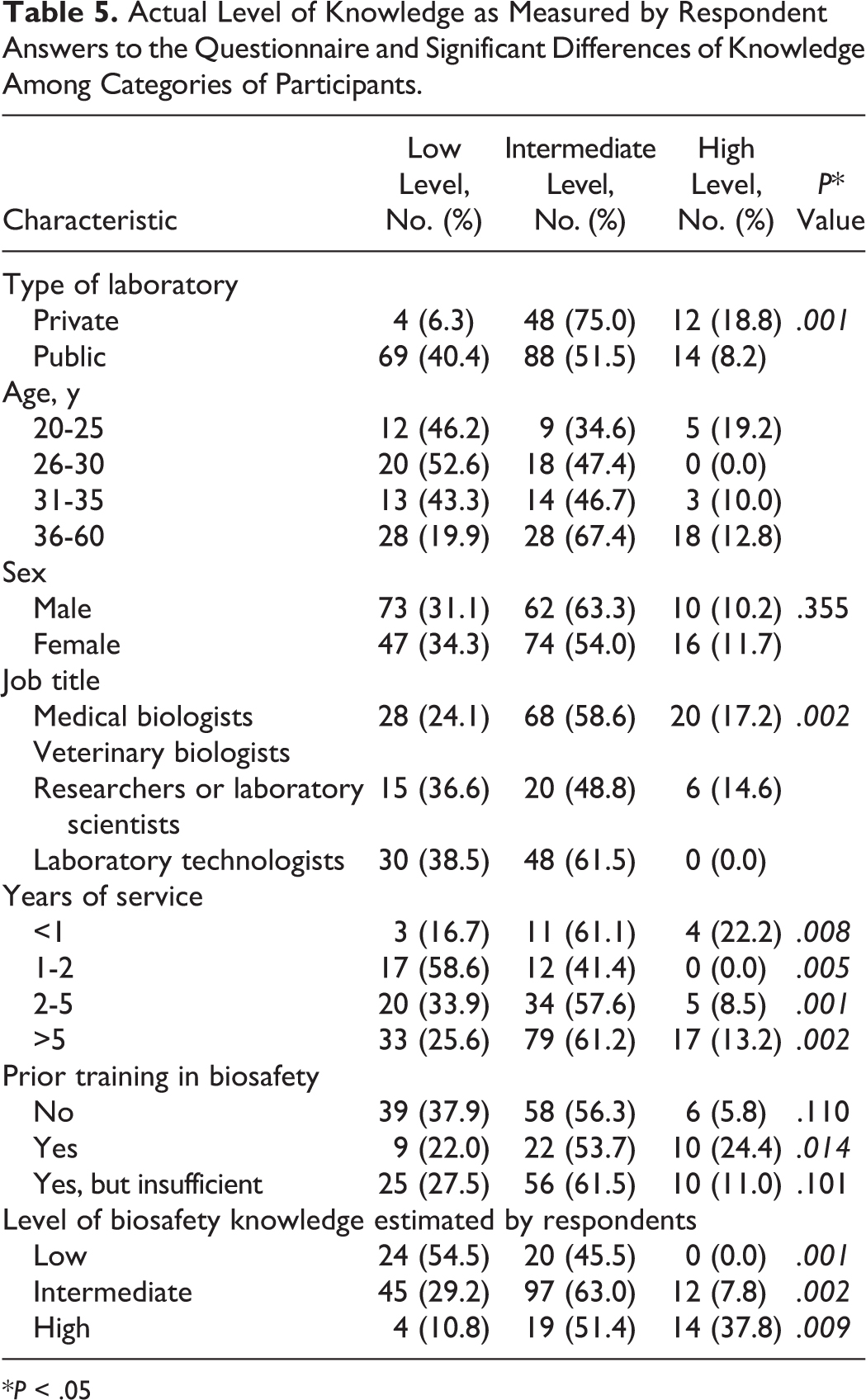
*P < .05
Knowledge of Pathogen Risk Group and Principle of Biosafety Levels
Most respondents (60.4%) reported working in a biosafety level 1 (BSL-1) laboratory (Table 2). Less than one-tenth (8.9%) reported working in biosafety level 3 (BSL-3) laboratories. Knowledge of signage and principles of biosafety levels was generally intermediate among both private and public laboratory staff without a significant distinction between these groups. However, workers in the private sector seem to be better acquainted with the objectives of containment (Table 6, section 1).
Specific Knowledge of Biological Hazards and Risks, Biosafety Concepts, and Practices Among Participants.
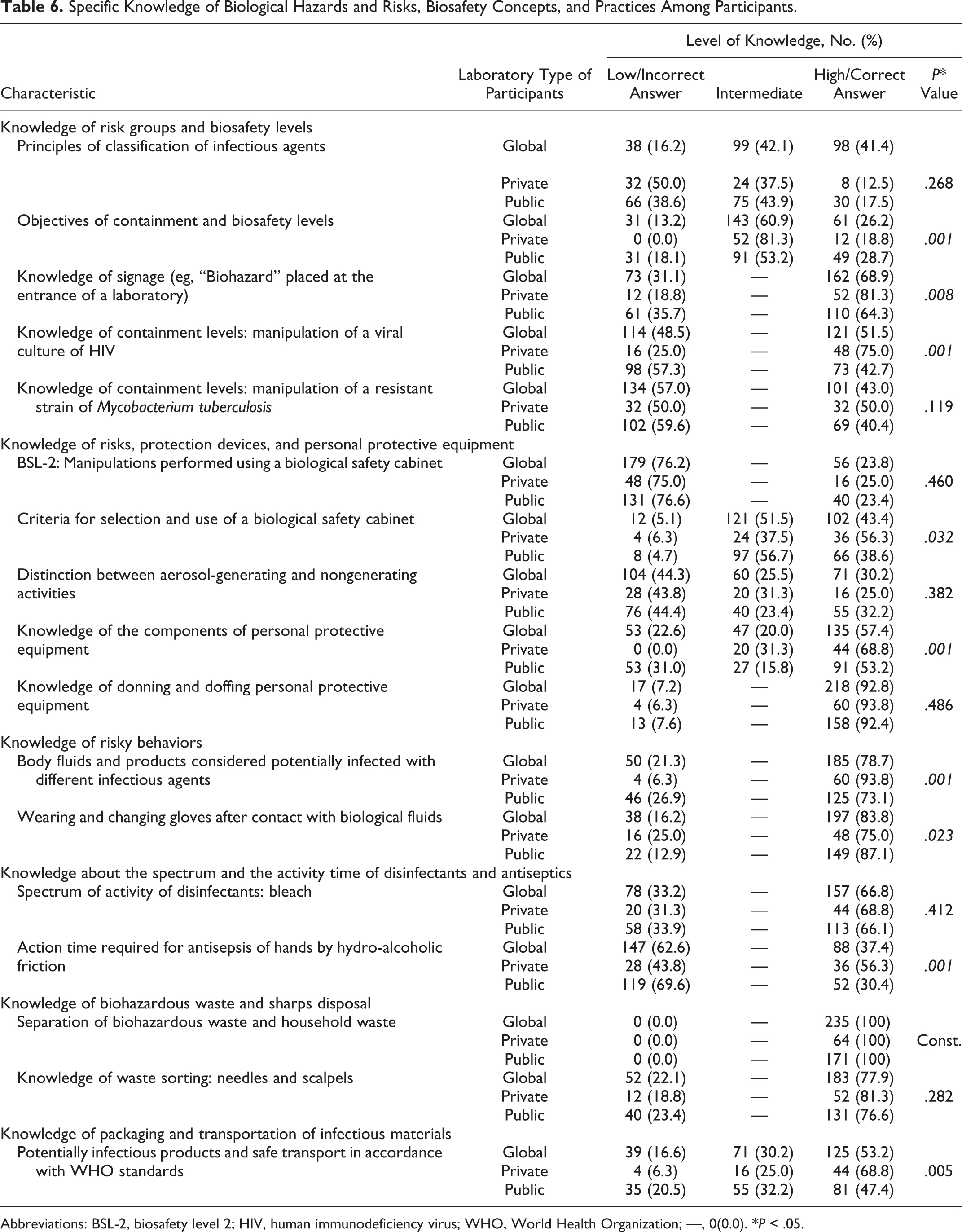
Abbreviations: BSL-2, biosafety level 2; HIV, human immunodeficiency virus; WHO, World Health Organization; —, 0(0.0). *P < .05.
Determining the required biosafety level and mitigation of hazards for handling pathogenic microorganisms is a crucial point in the prevention of accidental transmission of pathogens. Most of the respondents in the private sector (75.0%) gave a correct answer concerning the biosafety level (BSL) required for the manipulation of a viral culture of HIV, but 50.0% gave an incorrect answer concerning the BSL for the handling of a resistant strain of M tuberculosis (Table 6, section 1). Respondents were scored as correct if they chose biosafety level 2 (BSL-2) or BSL-3 as the correct response for handling HIV cultures since there is variation in procedures at different facilities, with some requiring BSL-3 containment and others requiring BSL-2 containment with BSL-3 practices. The same rationale was used for scoring responses concerning M tuberculosis handling. In Morocco, many operations in diagnostic laboratories are performed with M tuberculosis using BSL-2 containment. However, when manipulating antibiotic-resistant strains, using cultures with high titers, or performing manipulations that generate aerosols/droplets, BSL-3 containment is used as advised by the WHO guidelines. 17 Respondents in the public sector showed a low level of knowledge concerning the determination of the risk group and the level of containment for these 2 infectious agents (42.7% and 40.4%, respectively).
Knowledge of Risk, Protection Devices, and Personal Protective Equipment
When answering questions concerning the handling of infectious agents in a biological safety cabinet (BSC) in a BSL-2 lab and the distinction between technical operations that could pose a risk by generating aerosols, most participants gave incorrect answers (76.2%) or showed a low or intermediate level of knowledge (69.8%), respectively. On the other hand, with regard to the questions related to the criteria of selection and use of a BSC, 43.4% of their responses were correct. For questions on the components and use of PPE, as well as proper donning and doffing of PPE, 57.4% and 92.8% of respondents answered at a high level (Table 6, section 2).
Knowledge of Risky Behaviors
Respondents were rated as having a good level of knowledge about risky behaviors: 78.7% had correct knowledge in handling body fluids and products considered potentially infectious regardless of the sector where they work, and 83.8% answered questions correctly about wearing and changing gloves after contact with human body fluids (Table 6, section 3).
Knowledge About the Spectrum of Disinfectants and the Contact Time with Antiseptic Solutions
More than two-thirds of both private- and public-sector participants knew that bleach is an effective disinfectant and has a broad spectrum of activity (66.8%). However, an average of 62.6% of all workers (with 69.6% of the workers in public laboratories) misjudged the time required for antisepsis of hands by hydro-alcoholic friction (Table 6, section 4).
Knowledge of Separation of Household and Medical Waste and Proper Sharps Disposal
Unanimously, all participants (100%) gave correct answers to the question related to the separation of potentially infectious waste from household waste, and this was independent of their sector of activity and their work experience or qualifications (Table 6, section 5). In addition, 77.9% of respondents gave correct answers regarding proper sharps disposal.
Knowledge of Packaging of Infectious Materials and Their Safe Transport
In total, 68.8% of private-sector staff and 47.4% of public-sector workers who participated in this survey correctly identified the importance of correctly transporting potentially infectious products and the need to do so in accordance with WHO standards (Table 6, section 6). Nevertheless, it was surprising that 6.3% of private-sector respondents had a low level of knowledge in this area.
Discussion
Recent events such as coronavirus in Saudi Arabia, 18 Zika virus in South America, 19 and Ebola virus outbreaks 20 in West Africa have called attention to the need for a biosafety culture in laboratories around the kingdom of Morocco. During these responses, significant gaps were identified in laboratory biosafety practices, specifically concerning the ability of some clinical laboratories to perform a risk assessment and select the equipment needed for the biosafety requirements related to the pathogen being handled and to safely and correctly package and ship specimens to other laboratories.
Strengthening biosafety and biosecurity is imperative to face the threats posed by emerging and reemerging infectious agents. Handling these microorganisms safely is a priority, but this cannot be done without the involvement of qualified, well-trained, and aware laboratory personnel. The qualification of the staff lies in their training and the maintenance of their knowledge at a significant level.21,22
To our knowledge, this questionnaire-based survey is the first to evaluate the knowledge of biosafety among Moroccan laboratory workers. In our study, the survey response rate of 19% was relatively reasonable. There was an 81% nonresponse rate, which could be interpreted as resulting in bias, assuming that results of nonrespondents would be different from those of the respondents. For cross-sectional studies identical to this one, some authors report high rates, as in the case of Zaveri and Karia 22 (77%) and Nabil Al-Abhar et al 23 (94%). Not having a higher response rate in the current study may be due to inadequate transmission of the questionnaire and to low motivation on the part of the respondents, which could infer that the attention attached to laboratory biosafety is low. Heckert et al 24 describe various aspects of constraints and challenges faced by low-resource countries, which severely inhibits building and maintaining biosafety programs.
Our respondents were asked about the perception of their level of knowledge in biosafety. The difference in level determined by the study between the groups seems to confirm and agree with their perception. For the authors, it was both encouraging and troubling that workers admit and recognize their low level of biosafety training.
The actual level of knowledge about biosafety among all (private and public) laboratory workers who responded to the questionnaire was rather satisfying because 69% of respondents had a high or intermediate level of knowledge as measured by their correct responses to the questions. In the study conducted in Yemen by Nabil Al-Abhar et al, 23 87% of participants had a high or intermediate level of knowledge in the Laboratory Precautions Standards. Efforts must therefore be made to reach a more acceptable level of knowledge in Morocco.
In our study, we noticed that the level of knowledge of workers was low among young people, while their knowledge improved with increased work experience. This situation, coupled with the fact that few have participated in biosafety training, suggests that the noticeable improvement was due to experience and not to training. This is supported by work by Miring’u et al, 25 who demonstrated by studying the evolution of knowledge among staff on the use of BSCs that participants who had fewer years of experience showed the greatest improvement. They indicated the need for proper training of laboratory workers early in their careers, coupled with close supervision, mentorship, and regular refresher training.
The difference between workers in the private and public sectors in their knowledge was significant, with a P value of .001. In both sectors, most respondents showed an intermediate level of knowledge, and the difference is due to the fact that in the public sector, those with a low level were more numerous: 40.4% vs only 6.3% in the private sector. Nabil Al-Abhar et al 23 found superimposable results in a similar study that collected data from 362 participants without a significant difference since in this study, 37% and 39% of workers, respectively, in the private and public sectors had a low level of knowledge, and about half of the participants had an intermediate level.
Whether in the public or private sector, a participant’s knowledge of the principle of containment, biosafety levels and risk assessments, pathogens and their risk group classification, and working knowledge of containment equipment such as the BSC is low to medium. Determining the required biosafety practices involves a variety of factors, including an understanding of the risk group of a pathogen, recognizing the hazards involved with manipulating infectious agents, and knowledge of the biosafety facilities and how they work. 26
Although only general information on biosafety knowledge of facilities and equipment was collected in this study, it is clear that many, perhaps most, laboratories do not use adequate biosafety practices in BSL-2 containment. The lack of knowledge of biosafety concepts and the inadequacy of laboratories result from a lack of training on biosafety concepts, containment structures, and their objectives. Therefore, many workers, as shown in this study, do not know the facilities required to handle certain microorganisms, such as HIV and M tuberculosis. Improving the knowledge of laboratory biosafety in Morocco is fundamental to good, safe laboratory practices and worker health. In fact, the NSF International Standard and the American National Standard for Biosafety Cabinetry stated in its 2016 recommendation report that laboratory personnel should receive training in the handling of pathogens and potentially lethal agents in biosafety cabinets that must be supervised and controlled by scientists for the use of cabinets. 27
Wearing PPE was reported to be the most routinely used biosafety practice in a survey of research laboratories in various parts of the world. 28 Laboratory workers in our series, especially in the private sector, were knowledgeable with the use of PPE such as its components, proper donning and doffing of PPE, and the requirement of wearing and changing gloves after contact with biological fluids. The handling of viruses that have a pulmonary tropism is an exposure risk for the manipulator when not protected by a respirator and a suitable biosafety cabinet. 29 This risk is greatly increased by certain technical operations such as centrifugation and homogenization and by the manipulation of concentrated virus suspensions, as often occurs with viral cultures. 30
Since PPE is the immediate barrier between the microorganism and the manipulator, it is crucial that laboratorians understand the need for and practice of wearing PPE.
The respondents of our study were also familiar with products considered potentially infected with different infectious agents, like body fluids, and their safe transport in accordance with WHO standards. Any laboratory worker who handles blood or any biological sample may be at risk for accidental injury or exposure. Lack of awareness of biological hazards leads to improper handling and unsafe laboratory practices during sample collection, processing, and disposal. 31
Sharps constitute a special category of laboratory waste that can expose waste handlers to infection via puncture injuries during collection, transportation, and disposal. Most participants in this survey answered questions related to the separation of biological waste and household waste and disposal of sharps (needles and scalpels) correctly, and 77.9% to 100% of participants had very high scores on these questions. On the other hand, there were major gaps in the knowledge of public- or private-sector participants regarding the distinction between which manipulations generated aerosols and which did not.
To implement a laboratory biosafety program, it is important to understand the principles of decontamination, cleaning, sterilization, and disinfection. 32 Bleach solutions remain the disinfectant of choice in the laboratory of Morocco, and other antiseptic solutions and hydro-alcoholic gels, which are more expensive, do not have a wide use. Even though our participants correctly answered the question about the bleach solution and its effectiveness, which means that they are well informed about this solution (66.8%), only 37.4% are well informed about the time of action required for disinfection of hands by hydro-alcoholic friction.
Private-sector respondents demonstrated a good level of knowledge in the transportation of potentially infected substances. This is probably because these laboratories are more accustomed to sending specimens to other laboratories having more sophisticated equipment or as part of an interlaboratory collaboration or by outsourcing.
Conclusion
In Morocco, biosafety training in clinical and research laboratories is not neglected but needs to be improved. Although numerous laboratories have integrated biosafety into a quality approach and 2 biosafety associations provide training seminars and workshops, biosafety training is not legally required prior to the opening of public or private laboratories or when personnel handle biohazardous materials.
Most Moroccan educational institutions provide their graduates with some level of biosafety training, but it is sometimes incomplete or focuses only on certain subjects such as blood-borne pathogen standards and precautions. For this reason, generally, each laboratory management system develops its training program to meet the needs of its activities.
It is evident that difficult financial situations, resulting in lack of equipment and/or PPE, can increase the risk of infections, but this deficit can be counteracted by the development of practical biosafety training. 33 If the definition of biosafety refers to the application of knowledge, techniques, and equipment to prevent personal exposure to potentially infectious agents or biohazards, 15 then the objective of our study was precisely to measure this knowledge among workers in Morocco’s laboratories.
The knowledge on biosafety among clinical and research private and public laboratory workers in Morocco is moderate. Many gaps need to be addressed, such as lack of knowledge of biosafety levels required for different situations and understanding the characteristics and function of biosafety cabinets or antiseptic use. This underscores the need to strengthen training programs and biosafety policies so that the application of knowledge becomes not only a necessity but also a safety culture experienced daily by laboratory workers.
The ultimate responsibility for laboratory safety within an institution in Morocco lies with its chief executive officer, who, along with all associates, should have a commitment to the biosafety program. This commitment, as well as real support, should be obvious to all.26,34 Therefore, experts need to sensitize government officials to develop and implement biosafety committees and officials in health facilities and laboratories, as well as support university and institute directors in integrating biosafety learning into the basic training and continuing education curriculum. 35
Footnotes
Acknowledgments
We are sincerely grateful to all the participants both in public and private laboratories in Morocco for dedicating their time to fill out the questionnaires. We also thank the Moroccan Association of Medical Biology for their collaboration, the Moroccan Society of Medical Microbiology, and Moroccan Association of Biosafety for their collaboration.
Ethical Statement
This study was approved by the ethics committee of Research and Bioethics of the Military Teaching Hospital Mohammed V.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Human Rights
Not applicable.
Statements of Informed Consent
All participants gave their informed consent prior to their inclusion in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.