
Abstract
Academic medical centers comprise a diverse group of students, researchers, and health care professionals. There are also 3 unique environments: education, health care, and research. Differences in biosafety practices and procedures exist between these environments, but the common goal is to produce well-trained and successful health care and research professionals. An important part of the educational experience should include biosafety training. Having a strong foundation on biosafety principles will increase safety compliance in both the clinical and research workforces. Both students and employees should be knowledgeable and aware of biosafety. A biosafety survey was developed to measure the knowledge of students on biosafety principles at an academic medical center. This survey was validated by field professionals, including physicians, nurses, laboratory technologists, and researchers, who were surrogates for a multidisciplinary student population. The goal of the validation was to determine if the biosafety survey included appropriate questions and responses to adequately assess biosafety knowledge among students at an academic medical center. This step was very important because there are differences in the practices and guidelines for health care and research arenas. The validation results indicated that there are differences in the understanding of biosafety principles among different disciplines. There are also major differences in interpretations of biosafety principles between clinicians and researchers.
Introduction
Our institution is an approximately 697-bed facility with more than 10 000 employees. 1 Approximately 2385 students are enrolled in 28 degree programs offered through 6 schools: schools of dentistry, graduate studies in the health sciences, health-related professions, medicine, nursing, and pharmacy. Additionally, 626 medical residents and fellows receive graduate medical training. 2 Biosafety should be a top priority in an academic medical center that encompasses such a broad spectrum of students and employees. Both groups are important populations in terms of safety and compliance. A large portion of the employees are researchers, laboratory technicians, and other health care professionals. These groups make up various education levels and job descriptions. Indeed, students attending academic medical centers eventually may become employees, including faculty who will be responsible for training future students, many of whom will become physicians, nurses, researchers, laboratory workers, and other health care professionals. To ensure that health care and laboratory workers are adequately trained about biological risk (eg, hospital-acquired infections and accidental biological exposures) they are likely to face, it is essential to include and stress biosafety training as part of the educational curriculum. To decrease hospital-acquired infections and accidental biological exposures, educational institutions must promote and continually improve biosafety training. Biosafety must be stressed in all educational sectors, including undergraduate, graduate, and professional schools, which produce future health care and laboratory workers. Further, effective training must also address practices and procedures to prevent biological material exposure in all institutional settings to accommodate non–science personnel (custodial and nonmedical staff members). Thus, an institutional training program at an academic medical center must satisfy a number of regulatory standards, from the National Institutes of Health (NIH), the Centers for Diseases Control (CDC), the College of American Pathologists (CAP), and the Joint Commission (JC).
The importance of biosafety when handling microorganisms and other infectious materials must be recognized by both employees and students. There are different challenges faced by different groups in an academic medical center. Researchers and their students in a research lab may be exposed to a single or very limited number of infectious agents, but the quantities of the organism may be quite large (ie, a 1 L culture of Bacillus anthracis). Clinical personnel, including physicians, nurses, and laboratorians, may be exposed to a large variety of biological organisms of low to moderate infectivity that may or may not be recognized on initial contact. The application of safety guidelines and preventive measures in various settings is an important part of student and employee training. The key to a safe workplace is a workforce that is knowledgeable of the routes of transmission of infectious agents and applies safety principles and work practices to reduce the risk. 3 Factors such as proper use of personal protective equipment (PPE) as well as hand hygiene can mitigate risk of exposure to biological materials.
The risk to laboratory workers for exposure to common hospital-acquired infections such as Methicillin-resistant Staphylococcus aureus (MRSA) or ventilator-associated pneumonia (VAP) is much lower than to the patients. The laboratory worker may be more important as a potential source of contamination rather than as a potential infected patient given that laboratory workers share common spaces such as the cafeteria with patients and visitors. There is growing evidence that contaminated fomites or surfaces play a key role in the spread of viral infections. 4 Items such as doorknobs, countertops, elevators, and telephones often become contaminated and are capable of transmitting pathogens. Laboratory workers in research settings usually handle and manipulate organisms of known identity, whereas health care workers, including clinical laboratory personnel, are exposed to agents whose identity is initially unknown. In both cases, accidental transmission/infection and exposure to biological agents can be prevented through adequate biosafety training and precaution procedures.
As noted previously, training in biological safety is required by several regulatory agencies before laboratory personnel handle the hazardous materials. Most educational institutions require all laboratory personnel to complete safety training prior to the commencement of laboratory activities. Typically, all health care workers, plus nonmedical employees and staff, are also trained on blood borne pathogens (BBP) standards and precautions. Furthermore, each institution’s safety team usually develops specific training to meet the processes and regulations of the institution, requirements of funding and/or accreditation agencies, and applicable state and federal laws. Even though training is provided, in our experience, there is a lapse in some areas, and laboratory and health care personnel do not completely understand the requirements for maintaining a safe working environment in laboratories or patient care areas.
Most students receive specific training through clinical rotation and hands-on learning, but the fundamentals of biosafety are not always delivered directly. Students spend different periods of time in various training areas, and they develop a variety of biosafety techniques. This training varies from very generalized orientation or lectures to specific training in clinical microbiological laboratories and courses in microbiology or epidemiology. This lack of standardized training could contribute to the lack of biosafety knowledge and awareness. Hence, it is important to promote biosafety education from the beginning of any health science program. Emphasis should be placed on reduction of occupational exposure and application of standard precautions. Measures such as hand washing and appropriate use of PPE must be adopted by our future health care professionals. Knowledge concerning biosafety is essential so they can develop the necessary preventive measures in their respective fields. To determine the knowledge of biosafety practices among students at an academic medical center, a survey based on biosafety guidelines from several regulatory agencies was created. The survey was validated by a group of stakeholders: researchers, clinicians, and health care workers at an academic medical center. A study validated for appropriateness of content will identify gaps in student knowledge, practice, and perception that can be addressed by revisions to biosafety training.
Methods
Subjects
This project describes the validation of a biosafety training instrument and was conducted at a large academic medical center. The participants were health care professionals and faculty members representing basic science researchers/teachers, medical practitioners (physicians and nurses), and laboratory workers (both clinical and research settings) involved in training students and employees.
Instrumentation
The purpose of this project was 2-fold: the development of a survey instrument to assess the level of biosafety knowledge and the validation of this instrument. Before distribution to the validation participants, the survey was critiqued by the authors, who have expertise in biosafety as members of the Institutional Biohazards Committee. The participants in the project were then asked to provide validation of the questions for clarity and applicability.
The survey contained 4 demographic questions and 8 knowledge questions, as shown in Table 1. The questions were based on biosafety guidelines, predominantly the Biosafety in Microbiological and Medical Laboratories (BMBL). 5 The Clinical Laboratory Improvement Amendment (CLIA) 6 , College of American Pathologists (CAP) 7 , Joint Commission (JC) 8 , and NIH guidelines 9 were used by the author to develop the specific questions employed in the survey itself. Note that CLIA, CAP, and JC adopt the Occupational Safety and Health Administration’s (OSHA) regulations, specifically OSHA’s Bloodborne Pathogens Standard. 10
Responses to Knowledge Questions by Question Type.
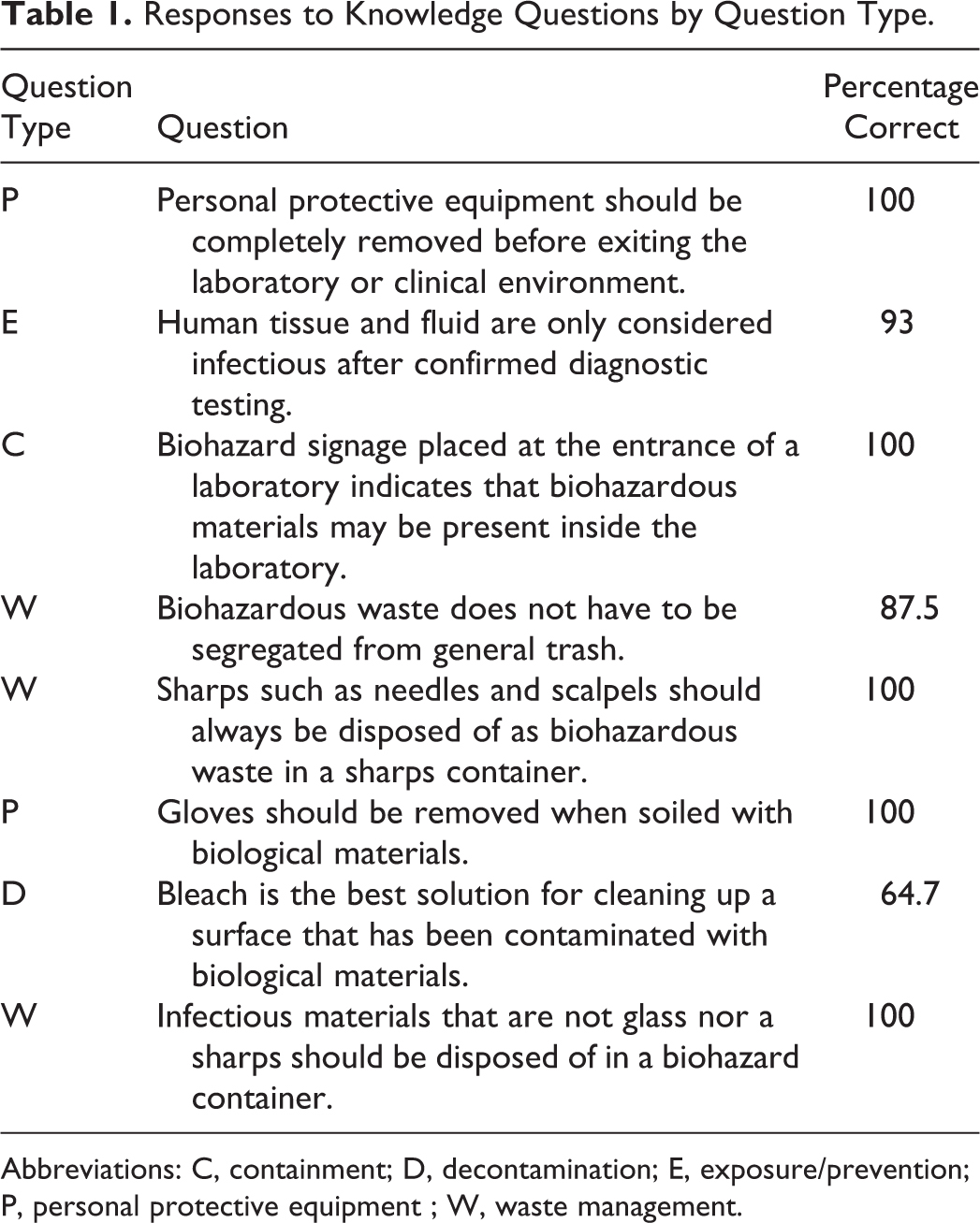
Abbreviations: C, containment; D, decontamination; E, exposure/prevention; P, personal protective equipment ; W, waste management.
All of the questions in the knowledge section were assigned a category based on the content of the question. There were 5 categories: PPE (P), exposure/prevention (E), containment (C), waste management (W), and decontamination (D). This section contained 8 questions for which true or false options were given as response choices. The goal of the questions in the knowledge section is to address the following: “How knowledgeable are students regarding biosafety principles?”
Validation
The purpose of validation is to ensure that an instrument actually measures what it is designed to measure. There are 4 methods of survey validation: face, content, criterion, and construct. Face and content validation include a panel of experts who judge the survey’s appearance, relevance, and representativeness of its elements. 11 The purpose of face validation is to ensure the instrument’s ease of use, clarity, and readability, whereas the purpose of content validation is to establish the instrument’s credibility, accuracy, relevance, and breadth of knowledge regarding the domain. 11
Both face and content validation were used to evaluate the survey instrument. A group of experts specialized in the field of biosafety and academic medicine were selected to evaluate the survey instrument. The experts evaluated the instrument’s appearance (face validation) and the instrument’s representativeness of the topic to be studied (content validation). 11 The main goal of the validation was to ensure that the instrument actually measures the intended domain, knowledge of biosafety.
For the validation of the survey, participants critiqued each survey question. For each question on the survey instrument, 5 critique questions were asked to help validate each question. These questions were: (1) Are the questions clear? (2) Are the questions appropriate? (3) Are the questions relevant? (4) Do the questions adequately measure the intended research question? (5) Are the response options appropriate? For each of these questions, 2 response options were given, yes or no. The participants were also asked to indicate if modification was required. The response options were major, minor, or none to allow participants to suggest a range of corrective actions from punctuation to deletion to an alternative descriptive. A text box was also provided for the participant to provide any additional comments regarding each question.
Data Collection
Participants were recruited during departmental meetings. The study was introduced by explaining the purpose and goal of the study. Participants were asked to participate, and those who agreed received a copy of the survey. The survey was administered on paper. This was more time-consuming than electronic surveys, but this method was chosen to increase response rates. Participants were asked to return the survey within 2 weeks. Twenty-three participants completed the survey.
Data Analysis
Responses were entered manually into Microsoft Access (Microsoft Inc, Redmond, WA) as they appeared on the survey. Blank responses were entered as “no response.” For the validation portion of the survey, some responses were paraphrased to fit into the test fields. Once all the data were entered into an Access form, an Access table was automatically generated to include all the survey data. The Access table was exported into a Microsoft Excel (Microsoft Inc) file, and Excel statistical functions were used to analyze the data. Frequencies and percentages were calculated to summarize the information from the survey. Charts and other graphics were made to reflect the summaries.
Results
Twenty-three participants completed the validation. The validation requested demographics and completion of the knowledge section of the survey. As described in the methods section, all questions were assigned a category based on the content of the question. The results from the survey validation are described in the following.
Demographics
Field professionals at an academic medical center were randomly selected and asked to participate in the validation study. Figure 1 displays the participants by job titles. Researchers (36%) and clinical laboratory technologist (36%) were the largest groups represented in the survey population. Twenty three percent of the participants were physicians, and 5% of the participants were nurses. The participants were from various departments. The “microbiology department” category included both researchers in the microbiology and immunology department and clinical laboratory technologists of clinical laboratory services in the pathology department. These 2 groups were combined due to misidentification by respondents. This category was the largest group (58%) represented in the survey population. Of the remaining participants, 37% were from various sections in clinical laboratory services, and 5% were from the pharmacology research department.
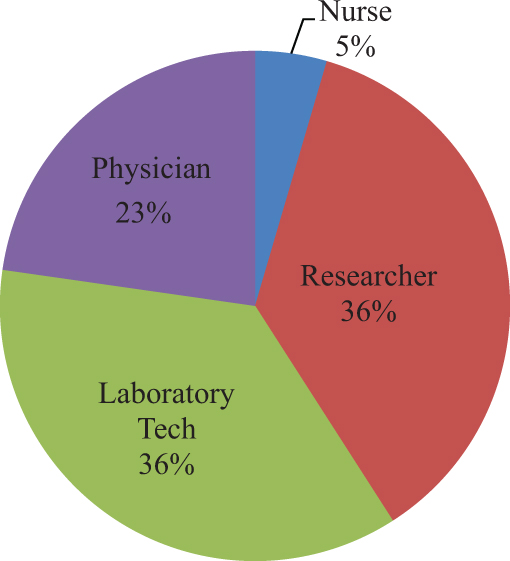
Participants by job title. Individuals participating in the validation of the survey instrument were asked to provide their job titles.
Figure 2 describes the highest education level of the participants. A majority of participants either had a PhD degree (41%, including a MD/PhD) or a bachelor’s degree (36%). Nine percent (9%) of the participants had a master’s degree, 9% had a MD degree, and 5% had a nursing degree. The participants also indicated when they were first introduced to the concept of biosafety. Most participants were introduced to biosafety either in high school (38%) or undergraduate school (38%). For the remaining participants, 14% were introduced to biosafety in graduate school, and 10% were introduced to biosafety in professional school.
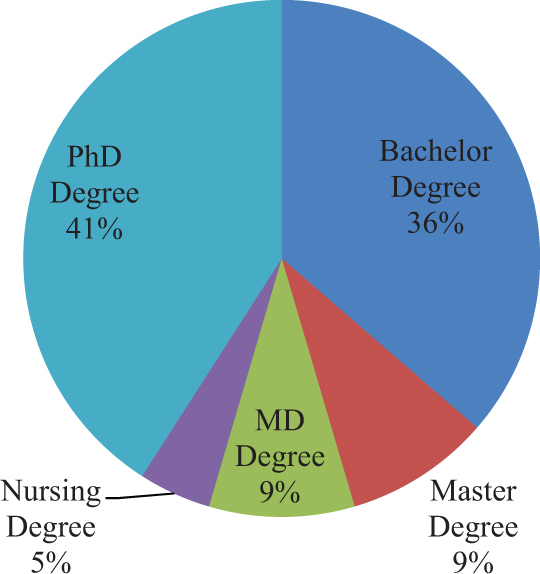
Highest level of education. Individuals participating in the validation of the survey instrument were asked to provide their educational degrees.
The participants also had various methods of biosafety training. Most participants received on-the-job training (45%) as the means of prior biosafety training. Thirty percent of the participants received school/employer orientation, 20% of participants had a lecture associated with a course, and 5% of the population had both on-the-job training and school/employer orientation. The participants gained prior biosafety experience in different roles throughout their career. Most participants had prior biosafety experience either in a research laboratory (5) or clinical laboratory (5). Three had been students, and 2 had been health care workers. The remaining participants had a combination of research laboratory, clinical laboratory, student, and/or health care worker as prior biosafety experience.
Survey Instrument
Participants responded by selecting yes or no to a series of knowledge questions related to biosafety. Figure 3 shows the percentages of the correct responses for the questions listed in the knowledge section of the survey. Table 1 also list the questions along with the category of the question and the percentages of correct responses.
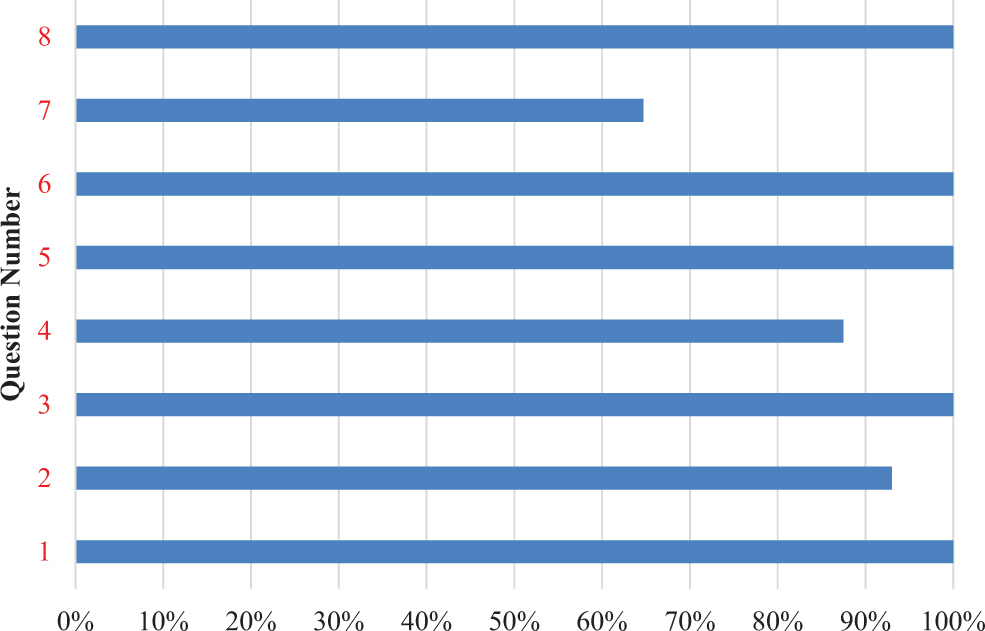
Responses to knowledge questions. Percentage of expected correct responses to knowledge questions are shown.
As displayed in Figure 3, the participants scored 100% on 5 of 8 of the questions regarding biosafety knowledge. The 2 questions for which the participants scored less than 100% were related to biohazard exposure/prevention, biohazardous waste segregation, and decontamination.
Validation
Table 2 provides a summary of the responses from participants for the validation portion of the survey on the knowledge questions. One hundred percent of participants thought that all the questions in the knowledge section were appropriate and relevant. There were mixed responses for the other questions: clarity, measures knowledge effectively, appropriate responses, and suggested modifications. These will be discussed individually in the following sections.
Responses to Knowledge Questions: Validation.a
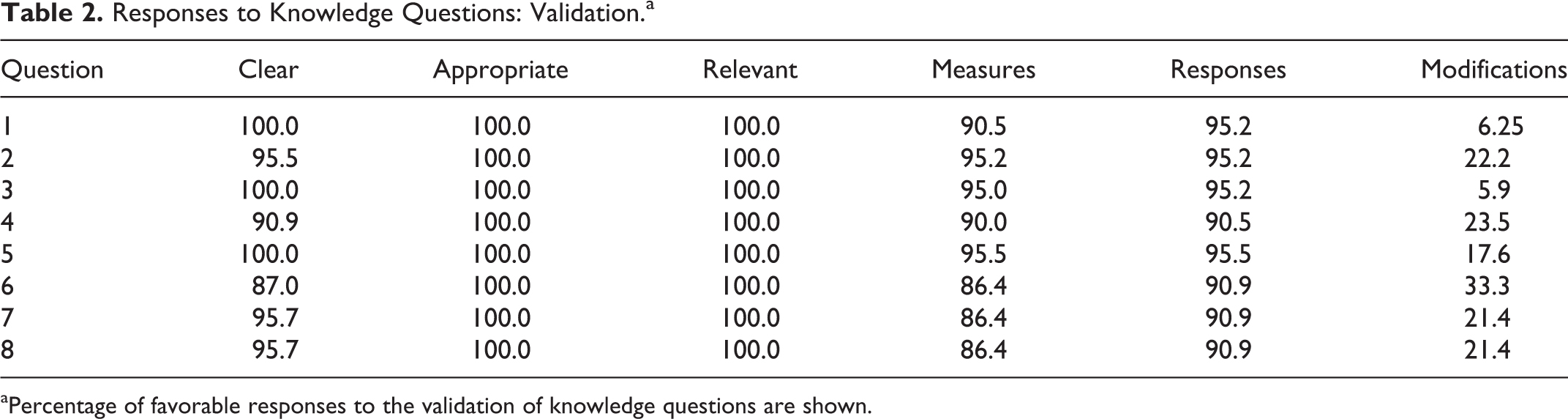
Percentage of favorable responses to the validation of knowledge questions are shown.
Clarity
A majority of the participants thought that the questions were clear. For each question, 87% to 100% of participants responded by selecting yes to indicate that the questions were clear. Questions for which participants did not all agree (100%) that the questions were clear included questions 2, 4, 6, 7, and 8. Question 6 appeared to be the most unclear to participants. Only 87% of participants thought this question was clear.
Measures
A majority of the participants thought that the questions adequately measure knowledge. For each question, 86.4% to 95.2% of participants responded by selecting yes to indicate that the questions measured knowledge. None of the questions received 100% agreement among the participants that these questions measured knowledge. Questions 6, 7, and 8 received the lowest score for knowledge. For these questions, 86.4% of participants responded that these questions adequately measure knowledge.
Responses
A majority of the participants thought that the survey instrument provided appropriate response options. For each question, 90.9% to 95.2% of participants responded by selecting yes to indicate that the questions provided appropriate response options. None of the questions received 100% agreement among the participants that the response options were appropriate. Questions 4, 6, 7, and 8 were questions whose responses were rated as not as appropriate as the others. For these questions, only 86.4% of participants responded that these questions provided appropriate response options.
Modifications
Participants indicated that all questions required modifications. For each question, 5.9% to 33.3% of participants responded by selecting either minor modification or major modification to indicate that the questions required changes. Question 6 has the greatest percentage of participants who thought modifications were required. For this questions, 33.3% of participants suggested modifications.
Discussion
The long-term goal of this project is to develop a training tool suitable for a large institution with a variety of activities involving biological hazards. At an academic medical center, this includes patient care activities, medical diagnostic laboratories, and specialized research laboratories that may have unique infectious agents. The personnel involved in such a complex ecosystem include everyone from high school graduates to PhDs. The risks encountered are as varied as soiled linens to large quantities of biosafety risk group 3 and risk group 4 organisms. Developing adequate training tools for online use requires a clear understanding of both the audience/group as well as expected risk encounters. This validation is a prerequisite for the deployment of an effective training tool.
Survey Instrument
There were 3 questions for which the participants did not score 100% on questions designed to test knowledge of biosafety. These questions were related to biohazard exposure/prevention (question 2), biohazardous waste segregation (question 4), and decontamination (question 7).
Question 2: Human tissue and fluid are only considered infectious after confirmed diagnostic testing
For this question, 93% of participants responded with the expected correct response. The demographic information that corresponds to the participant who answered this question incorrectly reveals that this participant works in a clinical laboratory. This suggests that the response may be associated with different practices in the clinical laboratory environment. Clinical laboratory technologists often handle a large spectrum of clinical samples on the open bench using standardized procedures to minimize the potential for droplet exposures. The practice of working on the bench is acceptable under CLIA and CAP guidelines (governing clinical diagnostic laboratories). When physicians suspect that clinical samples may contain pathogens spread by aerosol, they are required to warn clinical laboratory technicians so that the procedures are conducted in the biosafety cabinet. When researchers conduct procedures involving the manipulation of infectious materials that may generate an aerosol, the BMBL requires use of a biosafety cabinet or other containment device.
Question 4: Biohazardous waste does not have to be segregated from general trash
For this question, 87.5% of participants responded correctly. The demographic information that corresponds to the participants who answered this question incorrectly indicates the participants are health care workers. Health care workers have a different view on the definition of biohazardous waste primarily because of OSHA regulations. OSHA’s Bloodborne Pathogens Standard, 29 CFR 1910.1030, 10 defines regulated waste as liquid or semi-liquid blood or other potentially infectious material (OPIM), contaminated items that would release blood or OPIM in a liquid or semi-liquid state if compressed, items that are caked with dried blood or OPIM and are capable of releasing these materials during handling, contaminated sharps, and pathological and microbiological wastes containing blood or OPIM.
Health care workers have a less stringent perspective on what is classified as biohazardous waste. In health care, the idea of “release blood or OPIM when compressed” is quite different than perceived in the research setting. Whereas a health care worker will dispose a cotton ball containing blood in the regular trashcan, a researcher would place the same item in a container for biohazardous waste disposal.
From a biosafety perspective, biohazardous waste is defined as any laboratory waste generated from human or animal specimens, cultures, and stocks of infectious agents. Individual states and jurisdictions may differ on how waste is regulated. In research laboratories, biohazardous materials are defined as materials of biological origin that have the ability to produce hazardous effects on humans or animals. This may include recombinant DNA molecules, microorganisms, human blood and tissues, and any waste that is generated from these activities. Hence, researchers have more stringent perspective on the definition of biohazardous materials.
Question 7: Bleach is the best solution for cleaning up a surface that has been contaminated with biological materials
For this question, 64.7% of the participants answered this question correctly. A majority of the participants who answered incorrectly were researchers in the microbiology department. These responses were surprising. However, in some cases, bleach is not always the best decontamination method. Respondents often use expensive equipment for which the use of bleach would be very harsh for the equipment and even harsh for some surfaces in laboratories.
Validation
From the validation results, questions 2, 4, 6, 7, and 8 were not completely clear to all the participants. Question 6 concerning the removal of gloves appeared to be the most unclear to participants. Participants rated questions 6, 7, and 8 as questions that least measure knowledge. Questions 4, 6, 7, and 8 were questions in which the responses were not as appropriate as the others. Question 6 had the greatest percentage of participants who thought modifications were required.
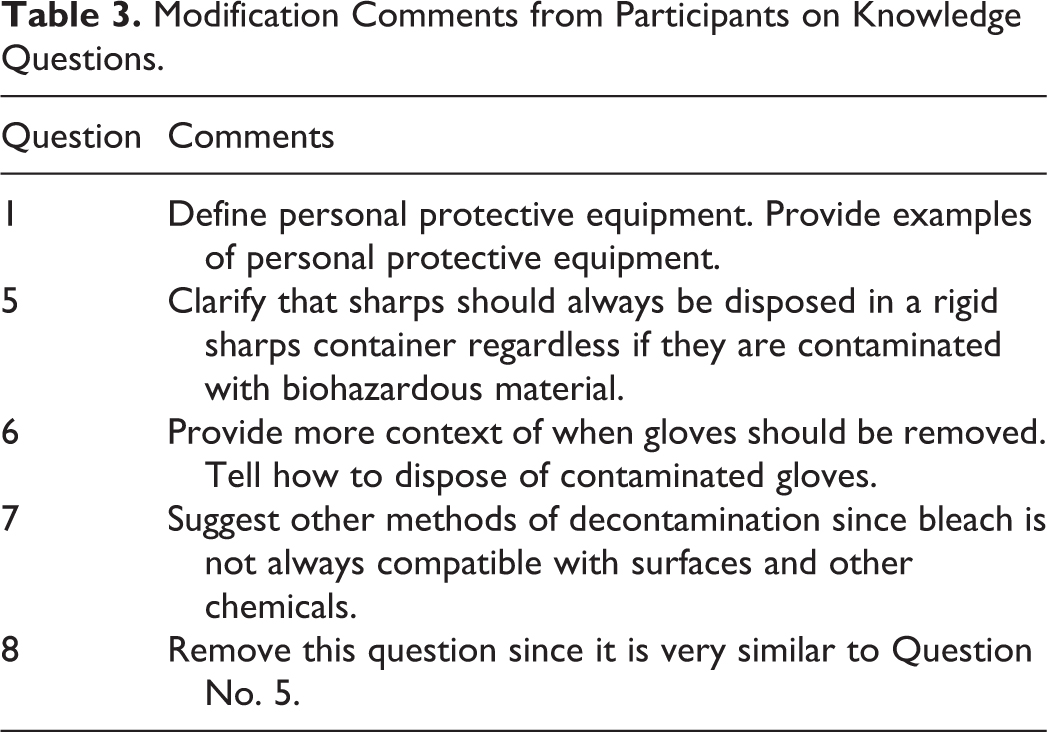
Of the questions, several received modification comments by participants. Table 3 shows some of the comments received by participants. The validation results help to explain why some participants responded incorrectly to questions 2, 4, and 7. Question 6 received the most criticism during validation by participants, but participants responded correctly. Only 64.7% of participants correctly answered question 7, use of bleach for decontamination. During the validation, participants made several comments to improve this question.
Modification Comments from Participants on Knowledge Questions.
Summary
The results reported here describe the construction and validation of a biosafety test designed for use in an academic medical center. This is a particularly challenging instrument to develop given the diversity of individuals who require biosafety training in such an environment. Participants that require safety training range from high school graduates to physicians and professors. Further, the types of laboratories and health care settings in an academic institution associated with a large number of schools are also varied. This includes students in allied health, nursing, dental, medical, and graduate school as well as employees in housekeeping, administration, maintenance, and other service areas who may be exposed to potentially hazardous biological materials. The validation of the survey instrument employed a number of health care professionals, including physicians, nurses, clinical laboratorians, researchers, and students.
The range of health care professionals who were sampled has provided some unique insights into the development of biosafety training tools. Ultimately, different backgrounds resulted in different understanding of questions. For example, while almost all researchers and laboratory personnel considered bleach the only appropriate method of disinfection, some respondents pointed out the corrosive effects this method has on certain types of materials used in non-laboratory settings. Care and use of personal protective equipment was also an area wherein discrepancies were identified. Some participants in the validation felt that lab coats should be completely removed when exiting the laboratory while others, primarily physicians, did not remove lab coats when exiting patient areas.
In conclusion, it is apparent that one size does not fit all when considering biosafety training at a multidisciplinary institution. Important differences exist between clinical and research domains in an academic medical center. Research laboratories may deal with very specific pathogens in high concentrations while clinical laboratories deal with a wide variety of organisms, both pathogenic and nonpathogenic. The employees range in education from high school graduates to advanced degree holders (physicians, nurses, dentists, and researchers). Training for all these diverse groups must encompass some common biosafety themes: personal protective equipment and decontamination/disposal of potentially infectious medical wastes. Therefore, a tailored approach to biosafety training is necessary.
Strengths
The professionals who completed the survey were all experienced field professionals. They directly handle biohazards or are involved in patient care activities.
Limitations
The sample size may not be a true representation of the larger population. Only representatives from 3 departments completed the survey. The responses may be biased due to the fact that these participants were interested in completing the survey, and they may be more knowledgeable of biosafety practices. Most participants had previous biosafety experience in their professional careers.
Future goals include the development of instruments to address perception of biological risks as well as the implementation of biosafety knowledge on practice of good biosafety protocols.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.