
Abstract
This study was conducted to assess the knowledge and practices of laboratory standard precautions (LSP) among laboratory staff working in Yemen clinical laboratories. A cross-sectional study was conducted among all laboratory staff in main public and private laboratories between September and October 2015. Data were collected using a self-reported questionnaire. A total of 362 participants had filled the study questionnaire with a response rate of 94%. Of the private and public laboratory staff, 67% and 32% had received training on biosafety (P < .001), respectively. Only 18% of respondents had received the biosafety manual (49% in private laboratories and 11% in public laboratories, P < .001). Overall, only 38% of respondents had good knowledge of LSP, 49% had fair knowledge, and 13% had poor knowledge. Only 32% of respondents had good practice of LSP, 59% had fair practice level, and 9% had poor practice. In conclusion, this study showed fair to poor biosafety knowledge and practices among laboratory staff as well as weak commitment to biosafety policies as reflected by low percentage of laboratory staff who received a biosafety manual and training. This finding underlines the need to strengthen the biosafety program and policies in laboratories in Yemen.
Keywords
Introduction
Biosafety is an important concern in laboratories worldwide, especially in developing countries where standard operating procedures (SOPs) are lacking. There are different sources and actions in laboratories that can lead to biological and chemical hazards, including exposure to aerosols, spills and splashes, accidental needle stick injuries, cuts from sharp objects and broken glass, oral pipetting, and centrifuge accidents. 1 Exposure to bloodborne viruses and exposure to aerosols are the most critical biohazards facing laboratory staff. 2 The World Health Organization (WHO) reported that about 3 million health care workers (HCW) all over the world experience percutaneous exposure to bloodborne viruses; 2.5% of HIV cases and 40% of Hepatitis B and C cases among health workers occur as the result of these exposures worldwide. 3
Biosafety during work and handling laboratory materials is important for prevention of laboratory-acquired infections and exposures among laboratory staff, particularly among those who are working in microbiological laboratories. 4 Without laboratory standard precautions (LSP) and proper training of laboratory staff, the laboratory environment can become very hazardous.5,6
Although awareness among health workers in developed countries is increasing, the situation is quite different in developing countries. The lack of knowledge of biosafety issues leads to improper handling and practice during sample collection, processing, and discarding, potentially exposing laboratory staff to pathogens. 6 Furthermore, such practices reduce the quality of laboratory services. Previous reports in developing countries showed poor awareness and practice of biosafety.7 –9 One study in Pakistan revealed that 32% of the laboratory staff did not use any kind of personal protective equipment, and 85% of technicians had no training on biosafety issues. 10
There is scarcity of data in Yemen about the level of awareness and compliance to standard biosafety precautions among laboratory staff. One study among health care workers in Sana’a health care centers reported a low awareness of infection control. 9 Understanding current knowledge and practice is important to design any future interventions to improve biosafety at the laboratories level. Therefore, this study was conducted to assess the knowledge and practices of LSP among laboratory staff working in the main public and private clinical laboratories in Yemen.
Methods
Study Design and Study Population
A descriptive cross-sectional study was conducted among all laboratory staff who were involved in processing laboratory samples in the main public and private clinical laboratories in Yemen. The study included those who were working in the National Center of Public Health Laboratories (NCPHL) as well as 3 main public (Al-Thawra, Al-Jomhory, and Al-Kuwait) and 3 main private (Saudi Germany, University of Science & Technology [USTH], and Azal) laboratories in Yemen. Staff who were not involved in processing laboratory samples, such as administrative staff, were excluded.
Data Collection and the Study Questionnaire
Data were collected between September 1 and October 31, 2015, using a self-administered semi-structured questionnaire. The quality control officers (QCOs) at each laboratory were trained to distribute the questionnaires to the participants, collect the necessary data, and review the completed questionnaires on the spot to assess for any missing data or misinterpretation. Ethical approval was obtained from the National Committee for Medical and Health Research at the Ministry of Public Health and Population. Informed consent was obtained from all participants.
The questionnaire was pilot tested on 10 respondents who were not included in the study, and necessary changes were made. The questionnaire was developed based on the available standard guidelines and practices and based on the reviewed literature9 –14 with feedback from some local experts in the field. The questionnaire was divided into 3 parts. Part 1 included information on sociodemographic characteristics of participants and information on the biosafety manual and training. Part 2 included 8 items to assess the level of knowledge of the biosafety among the laboratory staff. The questions were in multiple choice formats where only 1 answer was correct. The questions included information on the risks associated with work in the laboratory, the best concentration of alcohol to use for disinfection, the correct procedure to discard used syringes, clean-up of specimen spillage, and disinfection. Part 3 included 15 items on the practice of standard biosafety precaution with possible responses of always, sometime, and never. The items assessed storing laboratory clothing, wearing gloves and coat, procedures for handling infectious material, handwashing, and managing contaminated wastes.
Each question on knowledge of biosafety measures was scored as 1 point for the correct answer and 0 for the wrong answer or the “I don’t know” answer. Questions about positive practices of biosafety measures were scored 2, 1, and 0 for always, sometimes, and never, respectively. Questions about negative practices were scored 0, 1, and 2 for always, sometimes, and never, respectively. The total score on 0 to 100 scale was calculated for knowledge and practice domains and classified as good (score of 75-100), fair (score 50-74), and poor (score < 50).
Statistical Analysis
Data were analyzed using SPSS version 18 and described using frequencies and percentage. The differences between proportions according to studied characteristics were tested using chi-square test. A P value of less than .05 was considered statistically significant.
Result
Participants’ Characteristics
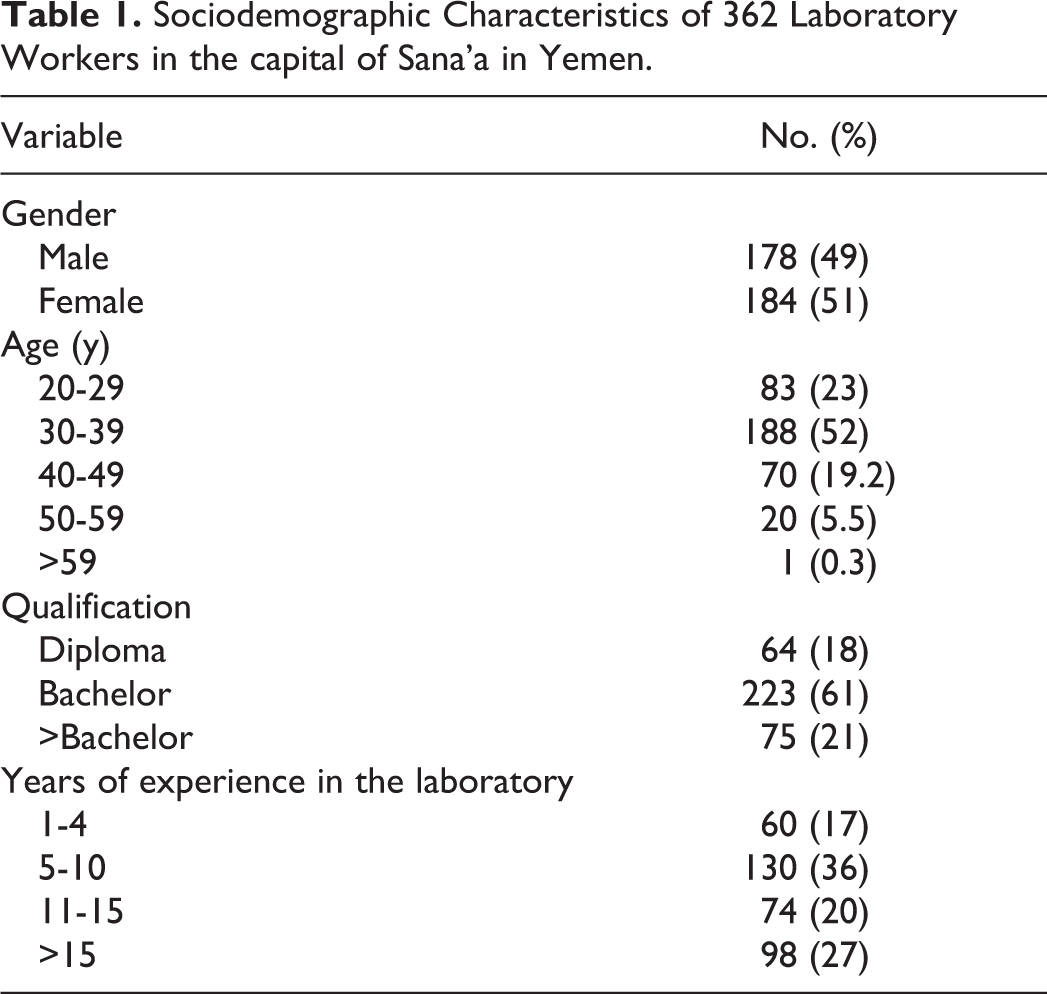
Of a total of 385 laboratory staff, 362 (292 from public laboratories and 70 from private laboratories) had completed the study questionnaire, with a response rate of 94%. Table 1 shows their sociodemographic characteristics. About half of the respondents were aged 30 to 39 years. Less than two-thirds (61%) were holding a bachelor’s degree, and 47% had >10 years of experience.
Sociodemographic Characteristics of 362 Laboratory Workers in the capital of Sana’a in Yemen.
Biosafety Manual and Training
Only 18% of respondents had received the biosafety manual (49% in private laboratories and 11% in public laboratories, P < .001). Of the private and public laboratory staff, 67% and 32% had received training on biosafety (P < .001), respectively. About 16% (39% in private and 6% in public laboratories, P < .001) had received training on how to deal with fire in the laboratory.
Knowledge Level of Laboratory Standard Precautions
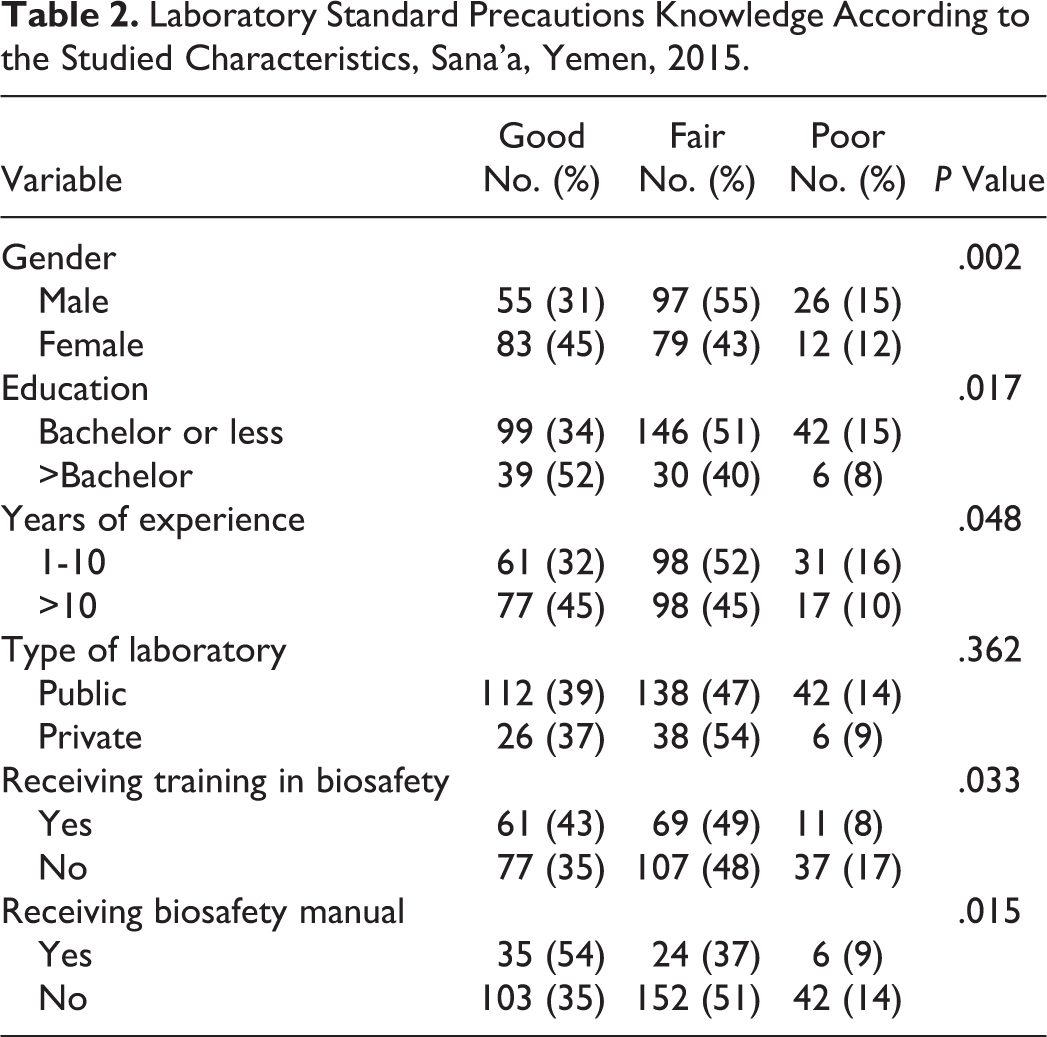
Only 38% of respondents had good knowledge of LSP, 49% had fair knowledge, and 13% had poor knowledge. Table 2 shows the level of knowledge according to the studied variables. Females, those with higher level of education, and >10 years of experience had better knowledge of LSP. The level of knowledge did not differ significantly according to the type of laboratory. Receiving biosafety manual and biosafety training were significantly associated with better knowledge.
Laboratory Standard Precautions Knowledge According to the Studied Characteristics, Sana’a, Yemen, 2015.
Laboratory Standard Precautions Practice
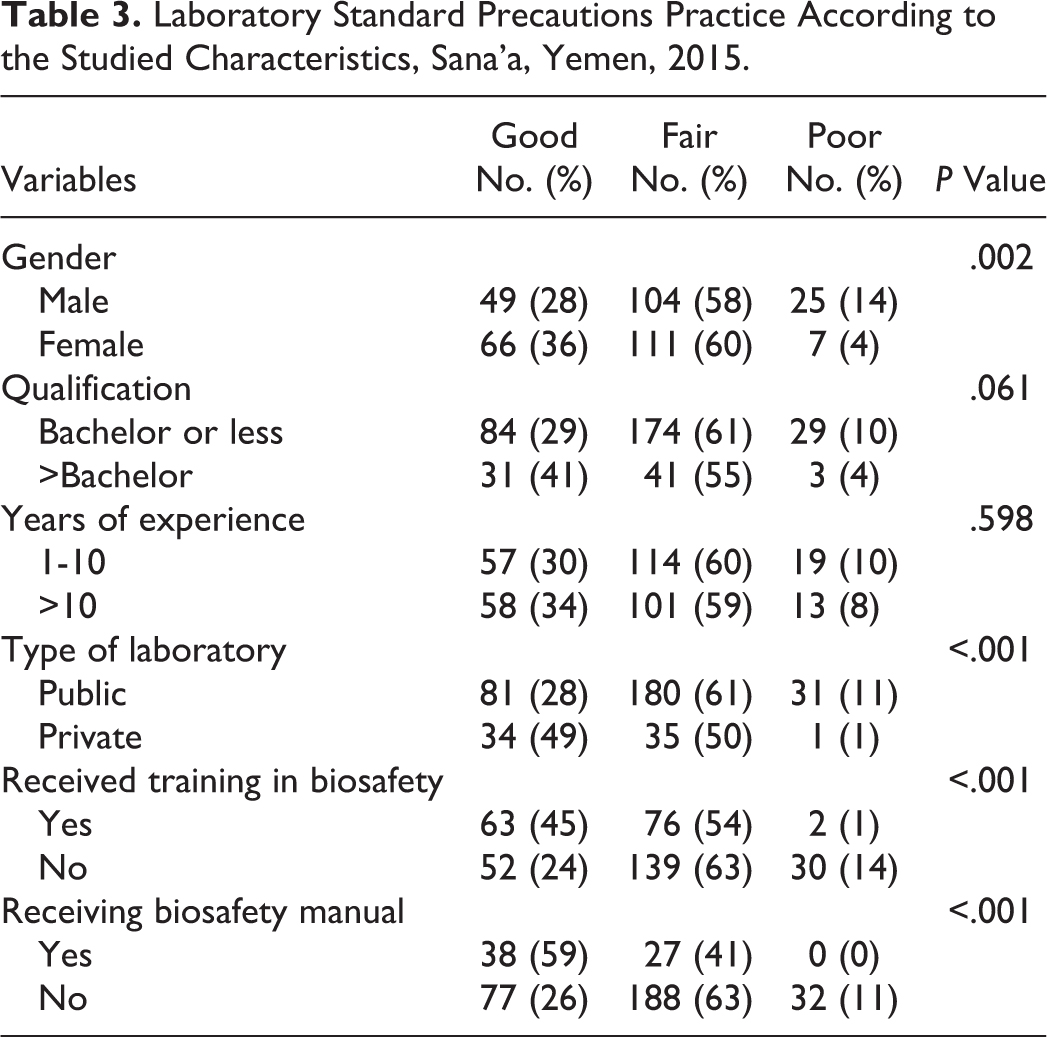
Respondents were rated as having a good practice level of LSP, 59% had a fair practice level, and 9% had poor practice. Table 3 shows the level of LSP practice according to the studied characteristics. Females and those in private laboratories had better practice. Receiving a biosafety manual and biosafety training were significantly associated with better level of LSP practice.
Laboratory Standard Precautions Practice According to the Studied Characteristics, Sana’a, Yemen, 2015.
Discussion
A limited number of studies had investigated the knowledge of and compliance of laboratory staff to standard biosafety precautions. Biosafety is compromised primarily in low-resource countries such as Yemen. This study revealed that biosafety in clinical laboratories in Yemen is neglected. Only 18% of the laboratory staff received a biosafety manual, a rate that is lower than that reported in Pakistan (20% and 24%).6,10 In addition, only 39% of laboratory staff received training on biosafety. A previous study in Yemen showed that 30% of laboratory staff had received laboratory biosafety training, 9 and another study in Pakistan reported that 15% of laboratory staff received a biosafety manual. 6 This finding highlights the need for laboratory biosafety training for all staff working with biological agents and materials in laboratories in Yemen.
This study showed that about one-third of laboratory staff in Yemen had good LSP knowledge and practice. This level of knowledge and practice was much better than the level that was reported in a previous study in Yemen. 9 However, laboratory staff in Yemen had poorer knowledge and practices compared to other developing countries such as Nigeria. 11 Poor knowledge and practice scores received by the laboratory staff indicate a big deficit in laboratory biosafety training and underdeveloped biosafety programs and policies in Yemen. Biosafety programs are needed now more than ever before because of the current crisis in Yemen, collapsed public health system, and the emergence of new serious epidemics.
In this study, females had a better knowledge and practice than males, a finding that is in agreement with the findings of a study in Iran 12 but in disagreement with the findings of a study in Ethiopia. 15 The observation that female staff demonstrated higher knowledge and practice scores than males is expected as more female respondents had received training on laboratory biosafety than females. It is also possible that females’ higher compliance may be associated with their tendency to practice socially acceptable behaviors. Moreover, the study showed that those with higher level of education had significantly better knowledge and practice. Although this finding is not consistent with the findings of 2 studies in Sana’a and Ethiopia,9,15 it is explained by the fact that those who had higher level of education had better opportunities to learn about the biosafety. Laboratory staff with >10 years of experience had better knowledge, a finding that agrees with the finding of a similar study in the United Arab Emirates 13 but disagrees with the findings from Sana’a study. 9 This finding is explained by the fact that the laboratory staff with higher experience have higher probability of receiving training, and they are more likely to realize the importance of and the need for biosafety practices.
Although there was no significant difference in the LSP knowledge between public and private laboratories, laboratory staff in the private sector had better LSP practice. Such difference in practice may be due to better LSP commitments among laboratory staff in private laboratories as part of biosafety policy enforcement through regular supervision. Consistent with a previous study, 14 our study showed significant positive impact for receiving a biosafety manual and training on LSP knowledge and practice. It is clear that receiving training in biosafety and receiving a biosafety manual are associated with better biosafety knowledge and practice. In the United States, significant gaps were shown to exist in US laboratory biosafety practices, specifically around the ability of some clinical laboratories to safely and correctly package and ship specimens to public health laboratories (PHLs) and the lack of biosafety programs in most clinical laboratories. 16
In conclusion, this study showed fair to poor biosafety knowledge and practices among laboratory staff as well as weak commitment to biosafety policies as reflected by the low percentage of laboratory staff who received a biosafety manual and training. This underlines the need to strengthen biosafety program and policies particularly in public laboratories. All laboratory staff in Yemen should be trained on biosafety, receive written biosafety procedures, and be monitored for their adherence with standardized laboratory safety practice. International procedures such as proper microbiological techniques, adequate facilities, protective barriers, and special training and education of laboratory workers should be applied. Moreover, proper design and construction of laboratory facilities must be followed.
Footnotes
Acknowledgments
Authors would like to acknowledge the Training Programs in Epidemiology & Public Health Interventions Network (TEPHINET) and Yemen Field Epidemiology Training Program for their technical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.