
Abstract
While both the biological safety and infection prevention professions exist to help individuals avoid contracting disease, there are distinct differences between the vocations. Biosafety professionals traditionally focus on the protection of laboratory workers from exposure to infectious biological agents by promoting safe microbiological practices and procedures and the proper use of containment equipment and facilities. Infection preventionists primarily focus on patient safety using epidemiology and the clinical applications of microbiology to prevent the spread of disease in the health care setting. Despite these differences, practitioners in both professions must possess a basic understanding of infectious diseases to perform their jobs effectively. For example, the principles of disease transmission and prevention, risk assessment, and sterilization are a few key concepts common between the professions. The recent outbreak of Ebola virus disease in West Africa and the subsequent lessons learned from patient care efforts abroad and in the United States revealed gaps highlighting the need for the sharing of skill sets between biosafety and infection prevention to work in concert to prevent occupational infections, especially during outbreaks of diseases of public health significance. Since such global infectious disease threats will inevitability occur into the future, now is the time to gain a better understanding of how these professions can work together, by identifying common competencies and highlighting differences. The codification of these similarities and differences can provide a roadmap to new professional development training initiatives for the enhancement of the biosafety profession.
While both the biological safety and infection prevention professions exist to help individuals avoid contracting disease, there are distinct differences between the vocations. Biosafety professionals traditionally focus on the protection of laboratory workers from exposure to infectious biological agents by promoting safe microbiological practices and procedures and the proper use of containment equipment and facilities. Infection preventionists primarily focus on patient safety using epidemiology and the clinical applications of microbiology to prevent the spread of disease in the health care setting. Despite these differences, practitioners in both professions must possess a basic understanding of infectious diseases to perform their jobs effectively. For example, the principles of disease transmission, disease prevention, risk assessment, risk management, disinfection, and sterilization are a few of the key concepts common between the 2 professions. The recent outbreak of Ebola virus disease (EVD) in West Africa and the subsequent lessons learned from EVD patient care efforts abroad and in the United States revealed gaps that highlighted the need for the sharing of skill sets between biosafety and infection prevention to work in concert to prevent occupational infections, especially during outbreaks of diseases of public health significance. 1 Since such global infectious disease threats will inevitability occur into the future, now is the time to gain a better understanding of how these professions can work together, by identifying common competencies and highlighting differences. The codification of these similarities and differences can provide a roadmap to new professional development training initiatives for the enhancement of the biosafety profession in this new era.
Professional Competencies
To ensure a high quality of professionalism, 2 professional disciplines establish standards for the knowledge, skills, and abilities of a competent practitioner. Competence can be defined “as the ability to do something well, or to do a job properly.” 3 “Competencies” are a set of defined knowledge and behaviors that provide a structured guide for enabling of the identification, evaluation, and development of a competent individual, and “core competencies” are capabilities and/or technical expertise that is unique to a particular organization or profession. 3 Similar to other professional organizations, the biosafety and infection prevention disciplines have utilized the collective wisdom of their organizations’ practitioners to develop and establish the competencies, experience, and educational attainment levels necessary to be credentialed in the field. Credentialing within a professional organization is often considered a tangible demonstration of the highest level of competency within one’s field.
Biological Safety
Professional competencies have been established for the biosafety profession by ABSA International and are embodied in the credentialing examination administered by the National Registry of Certified Microbiologists. Applicants who meet the education and experience criteria set forth by ABSA International and the National Registry of Certified Microbiologists and who are successful in demonstrating competency by passing the examination are afforded 2 certifications simultaneously—the certified biological safety professional and the specialist microbiologist in biological safety microbiology. There are 65 stated competencies that practitioners must master, which fall into 7 categories: (1) disinfection, decontamination, and sterilization; (2) safe work practices and procedures; (3) risk assessment and hazard identification, including infectious agents and recombinant or synthetic nucleic acid molecules; (4) regulatory aspects, standards, and guidelines; (5) program management and development; (6) equipment operation and certification; and (7) facility design.4,i
Infection Prevention
The Certification Board of Infection Control and Epidemiology 5 established 48 professional competencies for infection preventionists, which fall within 8 categories: (1) identification of infectious disease processes; (2) surveillance and epidemiologic investigations; (3) preventing/controlling the transmission of infectious agents; (4) employee/occupational health; (5) management and communication, including leadership; (6) education and research; (7) the environment of care; and (8) cleaning, sterilization, disinfection, and asepsis. Those who meet the education and experience requirements set forth by the Association for Professionals in Infection Control and Epidemiology (APIC) and pass the associated examination are afforded the credential called “certified in infection prevention and control.”
Analysis
To identify commonalties and differences between these 2 professional disciplines, we compared and contrasted the professional competency lists for each and then developed a summary comparison (Figure 1). The column on the left summarizes the competency categories that are primarily applicable or unique to the biosafety profession and would not typically be considered relevant to infection prevention practitioners. For example, working in the laboratory with recombinant or synthetic nucleic acid molecule technology or research animals is not typically relevant in the health care setting. The column on the far right summarizes infection prevention competency categories that are considered primarily applicable or unique to the infection prevention profession. For example, biosafety professionals are typically not concerned with environment-of-care issues related to patient care activities. Coalesced in the center column are competency categories where similarities exist between biosafety and infection prevention, in addition to often subtle and important differences. Improving the understanding of the different perspectives and approaches could serve as the basis for improved collaboration between the professions, as we believe there is sufficient to serve both professions in a practical and meaningful way.
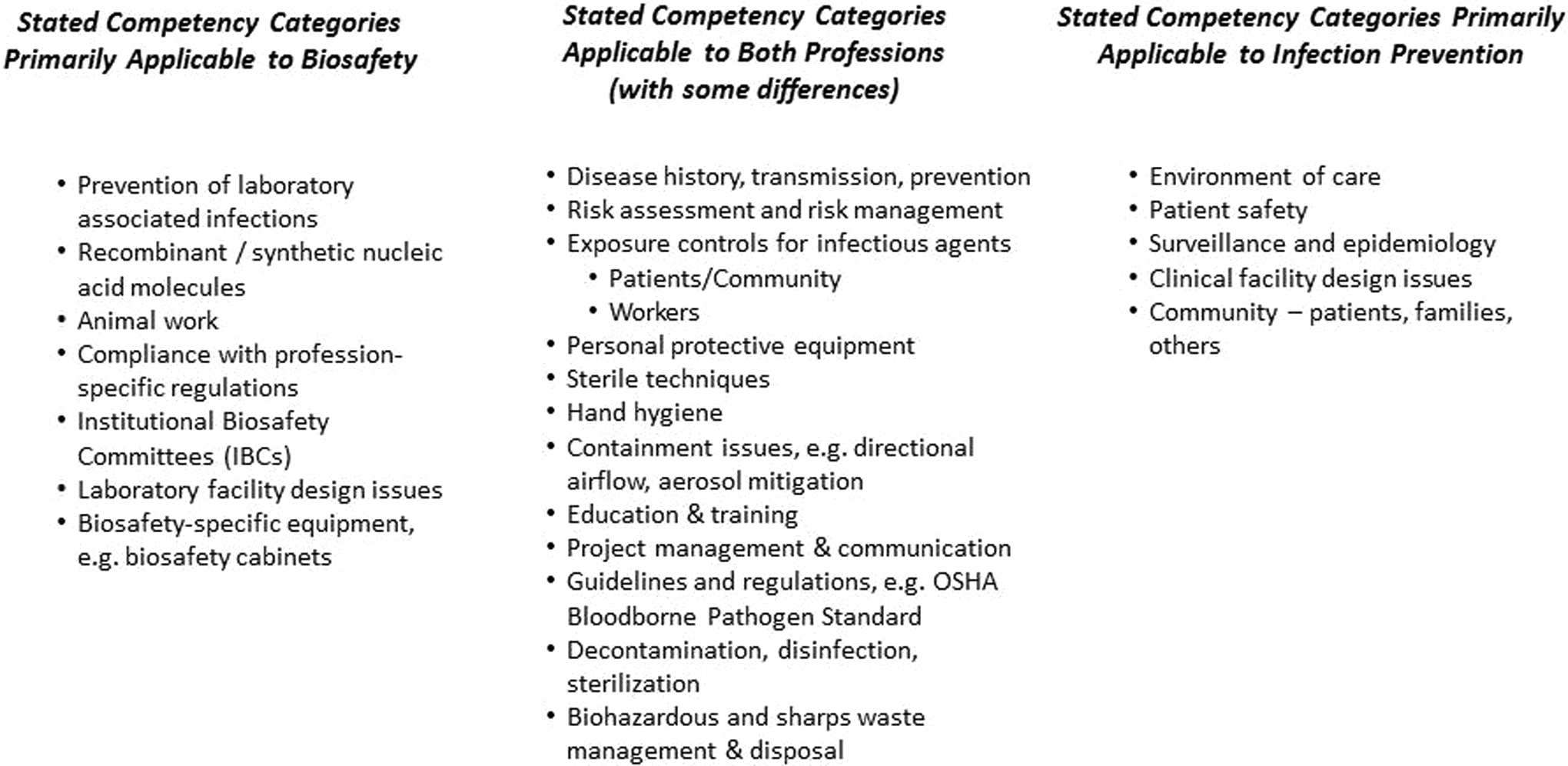
A comparison summary of stated competency categories for the biosafety and infection prevention professions.
As an example, consider “biohazardous and sharps waste management and disposal,” a common competency category that is listed at the bottom of the center column in Figure 1. Now consider Ebola virus medical waste regulations that require robust handling, packaging, and shipping procedures commonly implemented by biological safety professionals but now must be implemented in less controlled patient care environments and with the capacity to process significant quantities of waste. 6 Infection prevention does not specifically list biohazardous waste as a necessary competency, other than what can be inferred within the competency of safe injection practices. But, clearly, infection prevention professionals were required to consider these waste management issues during this time.
Another example is the selection and use of personal protective equipment. Infection preventionists are likely to be familiar with basic protective equipment, such as gloves, eye protection, gowns, laboratory coats, or isolation precaution ensembles routinely used in health care, but they may not be familiar with options for higher levels of protection, such as powered air-purifying respirators or ensembles that are commonly used in high-containment laboratories and can serve to protect health care workers in situations where patients may have a highly infectious disease.
Other competencies covered by biosafety, such as decontamination, sterilization and disinfection, biohazard exposures to workers, proper handling of biological material, exposure control procedures, emergency response, and biohazard waste management, can be the backbone for establishing processes for infection prevention. Biological safety professionals have extensive practice in proper sample handling techniques, shipping infectious samples, and handling personal protective equipment that may aid health care staff in an outbreak involving highly infectious but clinically rare diseases. A main focus of current biomedical research is to use biological materials as novel therapeutics options, such as gene, cell, and plasma therapies. As this work evolves, the biological safety profession will play a more significant role in the review and monitoring of associated clinical trials to (1) ensure worker safety, (2) protect patients from the specific risks associated with the therapy, and (3) explain the hazards and controls that need to facilitate the infection prevention procedures.
Recent Experiences Highlighting the Gaps
The value of an integrated approach to biosafety and infection prevention was exemplified in the experience of providing patient care for patients with EVD at the University of Nebraska Medical Center Biocontainment Unit and other high-level isolation patient care units in the United States. The experience at the biocontainment unit also highlights key areas that would benefit from cross-training the 2 disciplines. In the case of Ebola care in the United States, these 2 disciplines collaborated to enhance safety and reduce risk beyond what is provided by typical practices. 7 The introduction of a tier 1 select agent into clinical spaces presented unique challenges for utilization of complex medical devices, utilization and decontamination of clinical laboratory diagnostic devices, cleaning and disinfection of clinical spaces, and disposal of medical waste classified as category A infectious substance.7,8
Infection preventionists evaluated medical device integrity prior to use for EVD patient care. The infection prevention evaluation focused on the potential for contamination and the ability to withstand disinfection, whereas biological safety practitioners developed strategies for disinfection and decontamination of medical devices prior to reuse. Devices evaluated for infection control integrity and disinfection included portable x-ray, ultrasound, ventilator, and patient beds and mattresses.
As reflected in the professional competency analysis, it is common practice for infection preventionists to oversee biosafety with respect to clinical laboratories, which represents a clear linkage between the biological safety and infection control disciplines. 9 In support of EVD treatment in the Nebraska biocontainment unit, a joint effort was carried out by both biological safety and infection prevention professionals to conduct a focused risk assessment for every piece of diagnostic equipment in the clinical laboratory, as well as to identify potential strategies to optimize the use of biological safety cabinets, thus enhancing the environment of the clinical laboratory to safely arrive at a diagnosis.
Environmental cleaning within the Nebraska biocontainment unit also required a partnership of disciplines, demonstrating the value that each profession adds to ensuring greater safety. Environmental cleaning of patient care areas contaminated with Ebola virus involved robust protocols for manual disinfection, cleaning intervals, and quality assurance. Biosafety professionals developed comprehensive cleaning protocols for the clinical environment to inactivate Ebola virus, whereas infection prevention practitioners implemented those protocols into cleaning checklists for nurses and medical technicians that enabled systematic environmental cleaning at standard intervals that would not disrupt patient care. Similarly, terminal cleaning of the Nebraska biocontainment unit following conclusion of patient care was managed by biosafety professionals and evaluated for quality assurance by infection prevention.
Management protocols for medical waste generated from care for patients with Ebola virus were developed by drawing expertise from biological safety and infection control disciplines. Procedures for disposal of Ebola-contaminated medical waste requires packaging and shipping as category A infectious substances or onsite sterilization that is subsequently validated for adequate sterilization. Biological safety expertise was key to implementing necessary documentation and packaging protocols for large quantities of waste that met the category A infectious substance requirements, and infection prevention expertise was necessary to implement these strategies with health care workers in clinical spaces and in a manner that would enhance patient care.
While the Nebraska biocontainment unit experiences may represent extreme examples, they provide a tangible representation of the value in combining and cross-training 2 distinct but overlapping disciplines to enhance safety in a variety of environments where biological hazards exist.
Strategic Direction
These experiences suggest that new professional development training initiatives should be developed based on the comparison of competencies performed, as well as lessons learned from EVD patient care and associated activities. The most pragmatic way to reach biosafety and infection prevention professionals for cross-training is through their respective professional associations: ABSA International and APIC. Offering preconference course content on the basics of infection prevention as it relates to biosafety professionals at the annual ABSA International conference on biosafety is suggested, and this could be taught by practicing infection prevention professionals with an interest in this overlap. Vice versa, the biosafety basics for infection preventionists could be taught at the APIC conference by practicing biosafety professionals. Stand-alone courses or web-based learning offerings could also be effective for participants not able to attend annual conferences.
One group initiating efforts in this regard is the Biosafety and Infectious Disease Training Initiative (BIDTI), a multi-institutional collaboration funded in part by the National Institute of Environmental Health Sciences under award U45ES019360. The content being developed by this initiative represents a unique collaborative educational opportunity for both ABSA International and APIC. Although the BIDTI is in its early stages, its experts successfully developed, delivered, evaluated, and updated the daylong in-person course Fundamentals of Infectious Diseases of Public Health Significance. Moreover, the BIDTI has embarked on developing community-, awareness-, and operations-level training courses using various teaching modalities. 1 Content being developed through BIDTI could be delivered in person to both professions at the same time, providing the benefit of learning from the experiences of others in each profession.
Summary
Leveraging and sharing the collective skills of infection preventionists and biosafety professionals will enhance job performance and enable practitioners to respond to the next outbreak of infectious disease of public health significance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.