
Abstract
The extent to which breast cancer impacts well-being depends on the patient’s psychosocial resources for coping with the stressors the illness entails. Recent research has shown that character strengths, such as hope and zest, play a role in the life satisfaction of breast cancer patients, although the underlying mechanisms are yet to be explored. This study, involving 173 Spanish women with breast cancer, analyses the mediating role of hope and zest in the association between illness-specific stressors and 2 indicators of well-being, namely life satisfaction and flourishing. Both hope and zest were positively correlated with life satisfaction and flourishing, and negatively with stressors. Mediation analysis revealed that the relationship between stressors and the 2 indicators of well-being is mediated by both these character strengths. These results suggest that a lack of hope and zest is one mechanism through which stress may diminish well-being, whereas high levels of these character strengths may buffer the impact of stressors and improve well-being in breast cancer patients. Psycho-oncologists are encouraged to develop effective psychological interventions to promote these strengths in women with breast cancer.
Introduction
Psychological research in the field of breast cancer has focused on both the psychological maladjustment associated with the disease1 -4 and the psychosocial resources that improve coping and promote well-being. 5 Subjective well-being (SWB) has been widely used as a health outcome. The study of this construct within positive psychology has focused on 2 approaches6,7: hedonic and eudemonic. The former considers that SWB encompasses both a cognitive and an emotional component. 8 The cognitive component refers to life satisfaction (LS), which represents an evaluation of life as a whole. The emotional component relates to positive and negative affect, representing how a person reacts emotionally to life events (ie, whether these generate feelings of pleasure or displeasure). The eudemonic view of SWB is related to flourishing, which refers to “the experience of life going well” and the combined sense of “feeling good and functioning effectively.” 6 More specifically, flourishing refers to a sense of psychosocial prosperity and well-being, as well as to perceived success in terms of positive relationships, purpose in life, engagement, competence, self-esteem, optimism and contribution to the well-being of others. 9
Recent research suggests that women with breast cancer have a distinct profile in terms of their assessment of LS, 10 with lower scores compared to both other oncology patients 11 and the general population. 12 Importantly, patients with low LS scores have been reported to show lower levels of resilience, self-esteem, emotional intelligence and optimism and higher levels of anxiety and depression.10,13 In this population, and as expected, LS is also strongly related to flourishing, insofar as people with low LS scores tend to show lower levels of psychosocial prosperity.10,14 The 2 constructs are also associated with the level of stress, such that patients with lower levels of SWB exhibit higher levels of stress.10,14
High levels of stress are common among breast cancer patients.15,16 However, the reaction to stress and how it impacts mental health differs from 1 individual to another. Pearlin and Bierman 17 proposed the stress process model to explain individual differences in how sources of stress are faced on a behavioural and cognitive level. This model considers several factors that can interact and determine how a person reacts to a stressful situation: (1) contextual variables; (2) stressors or sources of stress that are directly related to the demands of the situation and that are derived from the stressful situation but not related to it; (3) mediating or moderating variables, in the form of psychosocial resources that determine how the person responds to stress; and (4) health outcomes or the consequences of the whole process related to physical and mental health. Mediating/moderating variables may provide an explanation for the way in which particular individuals cope with a situation. From this perspective, health outcomes will be determined by contextual factors, stressors and mediating/moderating variables (Figure 1). The stress process model has been used to explain stress in caregivers of people with specific needs,18 -20 as well as among individuals with chronic disease, including adults with HIV, 21 cancer in general 22 and women with breast cancer. 23

The stress process.
In the case of breast cancer patients, contextual variables include sociodemographic characteristics (eg, age, educational level, marital status, etc.), as well as illness-specific factors (eg, cancer stage, time since diagnosis, etc.). Research has shown that breast cancer patients with a partner have a higher level of LS,11,24 although this association has not been observed in all studies. 25 There is also empirical evidence for the impact of age and level of education on SWB, with younger age25,26 and higher education 27 being associated with enhanced psychological functioning. Advanced cancer stage has also been linked to poorer quality of life. 2
In the breast cancer literature, disease-related variables are defined as stressors because they imply chronic strain. 28 Variables of this kind include body image dissatisfaction, 23 fatigue or pain, 2 negative social interactions, 29 inadequate access to healthcare services 30 and maladaptive health-related worry. 31 Drawing on this work, Cerezo et al 32 recently developed the Stressors in Breast Cancer Scale (SBCS) to assess stress as stimulus. The SBCS yields a total stressors score and scores on 5 factors: physical appearance and sex strains, health and daily difficulties, interpersonal relationship strains, healthcare strains and worries and concerns about the future. Total and subscale scores on the SBCS were found to correlate positively with depression, anxiety, stress as response, perceived health and quality of life, indicating that the stressors it measures can significantly impact the mental health of women with breast cancer.
With respect to factors that may mediate/moderate stress, Pearlin and Bierman 17 propose 4 psychosocial resources: social support, coping strategies, mastery or locus of control and belief systems, meaning and values. Most research has focused on the first 3 of these,33 -35 whereas the latter has received limited attention. It has been suggested that the impact of a stressor may vary in terms of its relevance to a person’s values. 18 Values can be explored using the Values in Action (VIA) classification, a tool developed within the field of positive psychology that lists 24 character strengths according to the values they represent.36,37 These values, which according to Peterson and Seligman 37 have proven to be universal (across religions, cultures, philosophical theories and history) are humanity, justice, courage, wisdom and knowledge, temperance and transcendence. The 24 strengths that reflect these values are: Hope, humour, creativity, bravery, zest, perseverance, self-regulation, humility, love of learning, curiosity, spirituality, appreciation of beauty and excellence, perspective, prudence, fairness, gratitude, forgiveness, honesty, kindness, love, judgment, social intelligence, leadership and teamwork.
Research has shown that certain character strengths are associated with SWB in the general population,36,38,39 as well as in clinical settings.18,40,41 Recently, hope, zest, self-regulation and gratitude have been identified as the most significant strengths associated with positive health-related quality of life in a large sample of adults from 159 countries. 42 Regarding the relationship with LS, hope, zest, gratitude, curiosity and love are considered key strengths.36,39 Of these, Soria-Reyes et al 27 found that hope and zest were the strengths most closely associated with LS in breast cancer patients. In the same population, Givi et al 43 found that pain in these patients could be buffered through zest, among other factors. Hope and zest have also been reported to be strongly correlated with flourishing in the general population. 44 Hope is defined as an optimistic perception of the future that orientates behaviour towards attaining goals, while zest is described as a tendency to engage in life with energy and enthusiasm. 36 Importantly, research indicates that character strengths may buffer the perception of stress, thereby acting as a protective factor and promoting psychological adjustment to stress.18,45,46
Park et al 36 argue that although character strengths remain broadly stable over the course of a lifetime, they can be targeted with psychosocial interventions. A better understanding of the mechanisms through which character strengths may buffer the impact of illness-induced stress could therefore help to develop more efficient and precise treatment programmes that enhance psychological adjustment to cancer. Character strengths have scarcely been studied, however, in the context of breast cancer, and to our knowledge, no studies to date have explored their capacity to mediate the relationship between stressors and SWB.
The aim of this study was therefore to analyse the mediating role of character strengths in the relationship between stressors and SWB (considered in terms of LS and flourishing) in a sample of women with breast cancer. We test a mediation model consistent with the stress process model, controlling for relevant contextual variables. Based on the empirical evidence, we expected to find significant mediation by character strengths, specifically hope and zest, in the relationship between stressors and the 2 indicators of SWB. The hypothesis of this study is therefore that lower levels of hope and zest are pathways through which stressors may cause a decrease in LS and flourishing.
Method
Participants
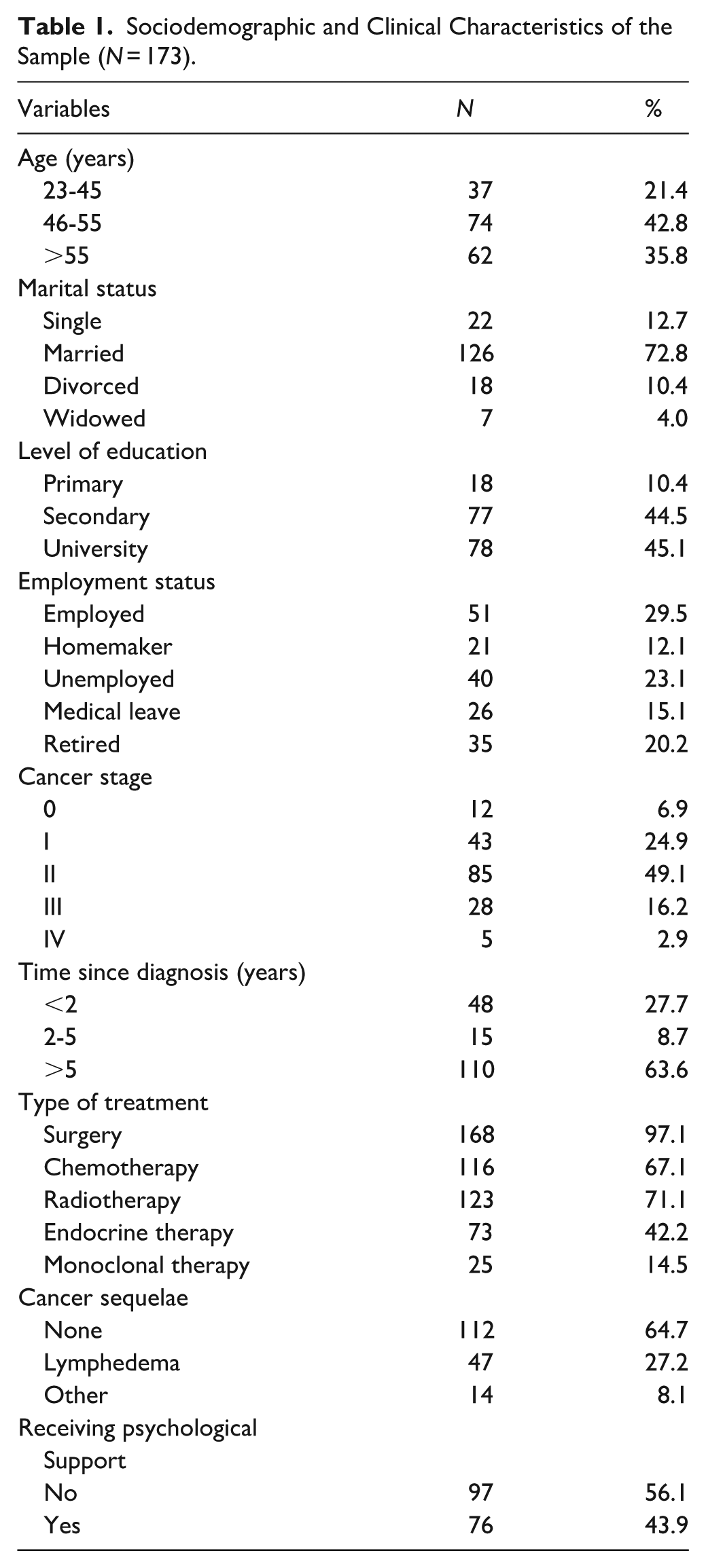
Participants were 173 Spanish women diagnosed with breast cancer and recruited through different health centres in Spain. They ranged in age from 23 to 76 years (M = 52.23, SD = 9.70) and the inclusion criteria were: (1) having a diagnosis of breast cancer, (2) having no diagnosis of any other type of cancer, and (3) signing of informed consent. The mean time since diagnosis was 5.95 years (SD = 6.79), and most participants had a stage II cancer or higher according to the TNM tumour classification system. Possible treatment combinations in this population vary and depend on factors such as the specific characteristics and stage of cancer, age and health status. In our sample the most frequent treatment was surgery (97.1% of women), with 14.5% of participants only receiving this treatment. Of the possible combinations, the most frequent (in combination with surgery) were chemotherapy, radiotherapy and endocrine therapy (23.1%), followed by chemotherapy and radiotherapy (19.1%). Sociodemographic and clinical characteristics of the sample are shown in Table 1.
Sociodemographic and Clinical Characteristics of the Sample (N = 173).
Instruments
Sociodemographic and disease-related data sheet. Participants were requested to report their age, marital status, level of education, employment status, cancer stage, time since diagnosis, type of treatment and presence of post-treatment sequelae.
Stressors
Sources of stress associated with the illness were assessed using the Spanish version of the Stressors in Breast Cancer Scale 32 (SBCS). The SBCS is a tool designed to measure the factors that generate stress in women diagnosed with this illness, independent of time since diagnosis. It has recently been translated into Chinese, showing adequate psychometric properties in a sample of women with breast cancer. 47 The SBCS comprises 24 items, each rated on a 5-point Likert-type scale from 1 (not at all stressful or is irrelevant to me) to 5 (very stressful). It provides a total score for stressors and scores on 5 factors: physical appearance and sex strains, health and daily difficulties, interpersonal relationship strains, healthcare strains, and worries and concerns about the future. The mean across the respective items provides the score for each factor, ranging from 1 to 5. The total score represents a global measure of stress and it was used in the present analysis. High scores on the SBCS indicate a higher level of stress. Cronbach’s alpha coefficient for total scores was .96 in the present sample.
Character Strengths
These were assessed using the Spanish version 48 of the Values in Action Inventory of Strengths 37 (VIA-IS). This instrument considers 24 character strengths, each of which is assessed by 3 items rated on a 5-point Likert-type scale, from 1 (very much unlike me) to 5 (very much like me). The mean across the 3 items provides the score for each strength, ranging from 1 to 5. Higher scores indicate stronger presence of a given character strength. For the present study, we only considered scores on hope and zest. In the present sample, Cronbach’s alpha coefficient was .74 for hope and .79 for zest.
Life Satisfaction
This was assessed with the Spanish version of the Satisfaction with Life Scale49,50 (SWLS), which has been validated in a sample of patients with breast cancer. 10 The SWLS measures satisfaction with life as a whole. It comprises 5 Likert-type items ranging from 1 (strongly disagree) to 7 (strongly agree), and thus the total score ranges between 5 and 35. The higher the score, the higher the level of life satisfaction. Cronbach’s alpha coefficient in the present sample was .87.
Flourishing
This was measured using the Spanish version of the Flourishing Scale9,51 (FS), which has been validated in a sample of patients with breast cancer. 14 The FS comprises 8 items that explore different aspects of human functioning, such as the perception of relationships, sense of purpose in life, personal competence, self-confidence, optimism, and so on. Each item is rated on a 7-point Likert-type scale from 1 (strongly disagree) to 7 (strongly agree), and thus the total score ranges from 8 to 56. Higher scores indicate a higher level of flourishing. Cronbach’s alpha coefficient in the present sample was .90.
Procedure
The study was approved by the Research Ethics Committee of the University of Malaga (Spain) and was conducted in accordance with the ethical standards of the Declaration of Helsinki. Participants were recruited by convenience sampling through various centres offering cancer care in Spain. The research team first contacted the managers of these centres to request their collaboration in recruiting participants, while also clarifying the purpose of the study. All centres consented, with the psychologist from each centre inviting women to take part. Women who accepted were sent an e-mail setting out the goals of the study and including a link to the questionnaires, which were hosted online. It was made clear to participants that this was a secure online survey and that all data collected would remain anonymous and confidential. Once participants had signed (electronically) the informed consent form on the first page of the survey, they could proceed to answer the questionnaires (sociodemographic and illness-related data sheet, SBCS, hope and zest subscales of the VIA-IS, SWLS and FS). The survey could not be submitted unless all questions had been answered, therefore avoiding missing data.
Data Analysis
As a preliminary analysis, we calculated Pearson correlation coefficients between the predictors, mediators and outcome variables considered in the study (Table 2). A coefficient of |.10| was interpreted as a small correlation, |.30| moderate and |.50| or above a strong correlation.
Correlation Coefficients Between Dependent Variables, Mediators and Predictors.

P ≤ .01. ***P ≤ .001.
We then tested a mediation model consistent with Pearlin’s stress process model. Mediation effects were determined using the procedure described by Hayes 52 and the PROCESS macro 4.2 for IBM SPSS Statistics (version 28), which consisted of performing 10 000 bootstrap iterations to generate 90% confidence intervals in order to test for the indirect effect. One-tailed tests were performed, given their suitability when directional effects are expected, 53 especially in mediation analysis. 54 An indirect effect was considered significant when the confidence interval did not include 0.
For the mediation analysis, contextual variables were introduced as control variables, stressors as predictors, zest and hope as mediators, and LS and flourishing as dependent variables. The contextual variables were: age, marital status (0 = single/divorced/widowed; 1 = married), primary education (0 = other; 1 = primary), secondary education (0 = other; 1 = secondary), employment status (0 = homemaker/unemployed/medical leave/retired; 1 = employed), time since diagnosis in years, and cancer stage. All analyses were conducted using IBM SPSS Statistics v.28.
Results
The results of the correlation analysis (Table 2) yielded small and moderate negative associations between stressors and hope, zest, LS and flourishing. In turn, hope and zest showed a strong positive correlation with LS and flourishing.
The mediation model tested to predict LS and flourishing included stressors as a predictor and hope and zest as mediators, controlling for the contextual variables listed above. Significant paths are represented in Figure 2. Regression equations are shown in Table 3. Residuals fulfilled the assumptions of linearity, normality and homogeneity.

Summary of significant pathways in the mediation analysis.
Results From Regression Equations in the Mediation Analysis.

P ≤ .05. **P ≤ .01. ***P ≤ .001.
Regarding the statistically significant effects of contextual variables on the dependent variables, age and marital status were significant in the prediction of zest, indicating that younger age and being married were associated with higher scores on zest. Marital status and educational level were significant in the prediction of LS, insofar as being married and having an educational level above primary were associated with higher levels of LS. The finding for educational level was also observed with respect to flourishing.
After controlling for contextual variables, the results yielded negative associations between stressors and hope, zest and LS. In addition, hope and zest were positively related to LS. The mediation analysis revealed a negative indirect effect of stressors on LS via hope and zest. The indirect effect via hope was −0.41, with a 90% bootstrapped confidence interval ranging from −0.82 to −0.10. The indirect effect via zest was −0.36, with a confidence interval ranging from −0.75 to −0.02.
The results also showed that hope and zest were positively correlated with flourishing. In terms of mediation, stressors had a negative indirect effect on flourishing via hope and zest. The indirect effect via hope was −0.78, with a 90% bootstrapped confidence interval ranging from −1.37 to −0.29. The indirect effect via zest was −0.86, with a confidence interval ranging from −1.40 to −0.37.
Discussion
The aim of this study was to analyse the mediating role of hope and zest in the relationship between stressors, LS and flourishing in a sample of women with breast cancer. We tested a mediation model consistent with the stress process model, and controlled for relevant contextual variables in the context of breast cancer.
The preliminary analysis using Pearson correlations yielded small and moderate negative associations between stressors and hope, zest, LS and flourishing. In turn, hope and zest showed a strong positive correlation with LS and flourishing. However, these patterns of correlations need to be interpreted more accurately through the mediation analysis in which contextual variables were introduced.
The mediation analysis identified 3 contextual variables as important: age, marital status and educational level. Regarding age, younger breast cancer patients tended to report higher levels of zest. Peterson and Seligman 37 pointed out that zest, at the somatic level, is linked to good physical health and bodily functioning. It is possible, therefore, that the negative association we observed between zest and age may be related to restrictions in physical activity that come with age. 55 The analysis also showed that women with a partner had higher levels of both zest and LS. The latter relationship (partner – LS) has been reported previously,11,24 although not all studies have found a significant correlation in this respect. 25 An explanation for these inconsistencies may be found in other studies showing the positive relationship between perceived social support from partners and better psychological adjustment to stress among women with breast cancer.2,35 That is to say, having a partner may not in itself be sufficient to enhance SWB if the interactions between the couple are not experienced as supportive. Finally, and in line with previous studies,26,27 we found that women with breast cancer who had only completed primary education scored lower on LS and flourishing. This may be explained by the association between a higher level of education and a healthier lifestyle, 56 as well as by the relationship between a lower level of education and both lower economic status and fewer psychosocial resources, which in turn are related to stress that negatively impacts physical and mental health.27,57 Other researchers have also found that a lower level of education resulted in late diagnosis of breast cancer and lower survival rate. 58
After controlling for contextual variables, breast cancer-specific stressors were found to be negatively correlated with both hope and zest. This is consistent with previous research in the general population showing that the presence of character strengths may act as a buffer against stress.45,46 Breast cancer-specific stressors were also negatively related to LS. This adds to existing evidence of the relationship between the 2 variables, reported using a different measure of stress in breast cancer patients. 10
Hope and zest, in turn, had positive direct effects on LS and flourishing, indicating that breast cancer patients with higher levels of hope and zest tend to evaluate their life as a whole as more positive, and also perceive themselves to be functioning more effectively. These results are in line with Soria-Reyes et al, 27 who found that both these strengths are related to LS, and they also extend knowledge regarding the association between these strengths and the eudemonic aspect of SWB.
In terms of indirect effects, the results revealed that hope and zest mediated the relationship between stressors and both indicators of SWB. This suggests that a lack of hope and zest is a mechanism through which stressors are associated with reduced levels of LS and flourishing. However, given that the direct effect of stressors on flourishing was not significant, stressors are only negatively related to this indicator of SWB when zest and hope (and specifically a lack of both) intervene. In other words, hope and zest may intervene as pathways buffering stress, while at the same time enhancing LS and flourishing. These findings underscore the significance of zest and hope as psychosocial resources that can mitigate stress and improve SWB in breast cancer patients. In terms of clinical implications, this suggests that psychological interventions targeting these strengths could boost SWB by fostering a proactive outlook on life, engagement and motivation.
Positive psychology interventions, aimed at fostering positive feelings, cognitions and behaviours, have been found to be effective in increasing quality of life, SWB, hope, benefit finding and optimism in breast cancer patients.59,60 Character strengths-based programmes have also been shown to increase SWB in patients with cancer. 61 Specific programmes targeting hope have likewise been developed for cancer patients. Examples include HOPE-IN 62 and AWAKE, 63 focusing on beliefs of self-efficacy in life and the pursuit of goals in young adults, respectively. Although hope-specific interventions may also impact zest, to our knowledge no protocols have been developed to specifically target zest in people diagnosed with cancer.
Hope and zest in breast cancer patients might also be promoted through other psychotherapeutic interventions, such as acceptance and commitment therapy (ACT), cognitive-behavioural therapy (CBT) and mindfulness-based cognitive therapy (MBCT). The aims of ACT are to make thinking more flexible, minimizing ruminative thoughts and seeking realistic goals that can favour the acceptance of adverse situations while reducing fatigue. 1 This approach might therefore promote hope by helping patients to set realistic goals, and zest through activities aimed at reducing fatigue, which could help them to experience life with more energy and activation. In a recent meta-analysis, Li et al 16 found that ACT has a beneficial effect on hope and other health indicators such as anxiety, depression and stress in breast cancer patients. Cognitive-behavioural therapy could also serve to promote hope, insofar as it focuses on cognitive restructuring and the setting of attainable and clear goals, which also involves seeking to replace negative thoughts towards the future with more adaptive and hopeful ones. This could also promote zest through the technique of behavioural activation (BA). Indeed, both ACT and BA emphasise values and engagement with aligned behaviours, which has been associated with an increase in vitality. 1 Finally, MBCT combines mindfulness-based stress reduction techniques with cognitive-behavioural techniques such as psychoeducation, cognitive restructuring and engagement in pleasant activities. 64 This approach could impact hope through cognitive restructuring and realistic goal planning, while patients’ zest might be increased by helping them to maintain energy and enthusiasm for the present by focusing on the here-and-now. Studies with breast cancer patients have found that MBCT significantly reduced anxiety, depression and fatigue, among other indicators.5,65 Overall, however, there is still limited research on the effectiveness of these interventions in the breast cancer context.
In light of the aforementioned research, it is worth noting that these interventions share several components that are crucial for enhancing SWB. Recent developments in therapy have shifted towards a process-based approach, moving away from different protocols for each diagnostic entity, and focusing instead on identifying key underlying processes common to various therapeutic strategies that mitigate dysfunctional mechanisms and enhance functional ones on a transdiagnostic level. 66 Consequently, exploring the shared components that are most relevant in targeting hope and zest is of considerable interest as a means of developing more effective and efficient interventions for promoting SWB among women with breast cancer. Mediation analysis could prove valuable in identifying these crucial processes.
This study has a number of limitations. First, the use of convenience sampling may limit the generalizability of results. Second, the online procedure through which data were collected could lead to both non-response bias and self-selection bias, which would threaten the external validity of the study. The use of self-report measures may likewise be a source of response bias. Finally, the cross-sectional design of the mediation model provides limited information about causal associations. Longitudinal studies could provide causal evidence to support the present findings.
In conclusion, this study provides evidence of the mediating effect of hope and zest among women with breast cancer, indicating that these 2 strengths buffer the impact of illness-specific stressors on LS and flourishing. In general, those women who experience life with greater enthusiasm and who maintain a positive outlook and commit to action to attain goals are less likely to perceive diminished SWB due to stress. These results suggest that interventions based on enhancing hope and zest may be useful in mitigating the impact of stressors on breast cancer patients. Future studies should aim to develop and test the efficacy and efficiency of treatment programmes that target these 2 character strengths so as to provide protection against stress and, at the same time, promote SWB in women with breast cancer.
Footnotes
Ethical Considerations
This study followed the ethical standards of the Declaration of Helsinki and was approved by the Experimentation Ethics Committee of the University of Malaga (55-2017 H).
Informed Consent
All participants signed informed consent to participate in the study.
Author Contributions
L.M.S-R. and M.V.C. were responsible for data collection. L.M.S-R. and A.T.P. wrote the first draft. M.J.B. led the research. All authors conducted data analysis and were involved in revising the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding from the Regional Government of Andalusia to Consolidated Research Group CTS110.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.