
Abstract
This study aimed to evaluate both the short- and long-term efficacies of chemoradiotherapy in relation to the treatment of esophageal cancer . This was achieved through the use of dynamic contrast-enhanced magnetic resonance imaging–derived volume transfer constant and diffusion weighted imaging–derived apparent diffusion coefficient . Patients with esophageal cancer were assigned into the sensitive and resistant groups based on respective efficacies in chemoradiotherapy. Dynamic contrast-enhanced magnetic resonance imaging and diffusion weighted imaging were used to measure volume transfer constant and apparent diffusion coefficient, while computed tomography was used to calculate tumor size reduction rate. Pearson correlation analyses were conducted to analyze correlation between volume transfer constant, apparent diffusion coefficient, and the tumor size reduction rate. Receiver operating characteristic curve was constructed to analyze the short-term efficacy of volume transfer constant and apparent diffusion coefficient, while Kaplan-Meier curve was employed for survival rate analysis. Cox proportional hazard model was used for the risk factors for prognosis of patients with esophageal cancer. Our results indicated reduced levels of volume transfer constant, while increased levels were observed in ADCmin, ADCmean, and ADCmax following chemoradiotherapy. A negative correlation was determined between ADCmin, ADCmean, and ADCmax, as well as in the tumor size reduction rate prior to chemoradiotherapy, whereas a positive correlation was uncovered postchemoradiotherapy. Volume transfer constant was positively correlated with tumor size reduction rate both before and after chemoradiotherapy. The 5-year survival rate of patients with esophageal cancer having high ADCmin, ADCmean, and ADCmax and volume transfer constant before chemoradiotherapy was greater than those with respectively lower values. According to the Cox proportional hazard model, ADCmean, clinical stage, degree of differentiation, and tumor stage were all confirmed as being independent risk factors in regard to the prognosis of patients with EC. The findings of this study provide evidence suggesting that volume transfer constant and apparent diffusion coefficient as being tools allowing for the evaluation of both the short- and long-term efficacies of chemoradiotherapy esophageal cancer treatment.
Keywords
Introduction
Esophageal cancer (EC) represents a serious malignancy largely due to its poor prognosis and survival rate. Esophageal cancer can be subdivided into 2 main types: squamous cell carcinoma and adenocarcinoma. Esophageal cancer currently remains one of the deadliest cancers worldwide, ranking as the sixth among all cancers in terms of mortality rates, as well as ranking as the eighth most commonly occurring cancer on a global scale. 1 The occurrence of EC continues to grow at a progressive rate worldwide with approximately 460 000 patients diagnosed with the disease, resulting in 380 000 deaths. 2 The EC 5-year survival rate remains just around 15%∼25%. 3 In accordance with retrospective studies, greater EC risks have been predominantly associated with smoking, red meat consumption, poor oral health, hot tea intake, low intake of fruit, and vegetables, as well as low socioeconomic status. 1 Patients often present with the primary clinical symptoms of dysphagia and weight loss. Additionally, other clinical symptoms often observed include odynophagia, upper gastrointestinal bleeding, hoarseness, and respiratory abnormalities. 4 Patients with early-stage EC generally require endoscopic treatment including endoscopy resection or esophagectomy with lymphadenectomy. 3 Owing to the fact that patients having EC can only be diagnosed upon presenting with complaints of dysphagia, odynophagia, anemia, or weight loss, it has resulted in the wide use of chemoradiotherapy combined with surgical resection in cases of resectable EC. 2,5 Furthermore, previous studies have provided strong evidence highlighting the survival benefit of chemotherapy, neoadjuvant chemoradiotherapy in lieu of a solely surgical approach in patients with esophageal carcinoma. 6 –8 Thus, it has been deemed necessary to conduct a close assessment of the efficacy of chemoradiotherapy. Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI), an advanced MRI technique, is a universally used oncology tool that measures the properties of tumor microvascular structure and permeability, as a noninvasive means of acquiring functional tissue information. 9 Reports have indicated that MRI utilization provides excellent diagnostic accuracy for assessing EC. 10,11 Likewise, DCE-MRI also provides quantitative information illustrated by a few parameters in its tumor evaluation. The volume transfer constant (Ktrans) acts as a functional parameter in connection with an appropriate pharmacokinetic model and possesses the ability to highlight the transport rate of the contrast agent from blood plasma to the extravascular–extracellular space, which can be used when evaluating tumor treatment response. 9 Furthermore, DCE-MRI has shown great potential in regard to the treatment response assessment and prediction of patients with EC undergoing chemoradiotherapy. 12,13 Diffusion-weighted imaging (DWI)-MRI is an advancing imaging technology that exerts greatly positive effects on the management of patients with EC. 14,15 The value of the apparent diffusion coefficient (ADC) is calculated for each pixel in an image, exhibited by a parametric map. The ADC of various tissues can be derived through regions of interests (ROI). 16 Apparent diffusion coefficient as a reliable and reproducible value tool serves as a promising noninvasive indicator that assesses tumor aggressiveness as well as patient tumor responses to chemoradiotherapy. 17,18 The potential of the ADC value as a useful marker has been well-documented in various studies, which have highlighted its ability in predicting response to treatment and the survival chances of patients with esophageal squamous cell carcinoma (ESCC). 19 Recent improvements in DWI-MRI have resulted in better imaging quality and further improvements in radiation treatment planning together with the assessment of treatment response. 14 Furthermore, another study suggested that the variable tumor ADC of DWI-MRI may provide accurate early prediction of histopathologic response during the 2 to 3 weeks of neoadjuvant chemoradiotherapy for EC. 20 Hence, the central objective of our study was to evaluate both the short- and long-term efficacy of chemoradiotherapy in the treatment of EC using Ktrans and ADC.
Materials and Methods
Ethics Statement
This study was conducted with the approval of the Ethical Committee of our hospital. All patients and their families were provided with and subsequently signed informed consent documentation.
Study Participants
Between January 2009 and January 2011, a total of 237 patients who had been previously diagnosed with EC at our hospital were recruited for the purposes of the study. All patients at the time of recruitment had been diagnosed with either early stage or advanced stage EC and were yet to undergo any form of surgical therapy. The participants consisted of 134 males and 103 females with a mean age of 56.99 ± 9.23 years (ranging between 24 and 89 years), of which 19 cases were older than 70 years of age, while 218 were younger than 70 years of age. Esophageal cancer was diagnosed either by pathologic or cytological confirmation. The pathological types were as follows: adenocarcinoma (n = 119), squamous carcinoma (n = 87), and others (n = 31). Lesion sites were cervical segment and upper chest (n = 105), middle and lower chest (n = 132). The Karnofsky performance score (KPS) was adopted, 21 and the length of lesion (cm) was subsequently recorded. Tumor (T) stage: T1/2 (n = 68), T3 (n = 93), and T4 (n = 76). Tumor node metastasis (TNM) stage 22 : II (n = 95), III (n = 142). Degree of differentiation: well differentiation (n = 86), middle differentiation (n = 60), and poor and no differentiation (n = 91). The inclusion criteria were as follows: (1) patients who were diagnosed as definitely having EC with the initial treatment confirmed by pathology and imaging means; (2) patients without distant metastasis; (3) patients with normal blood cells count, liver, and kidney function as well as electrocardiogram; (4) patients without any serious medical diseases; (5) patients without any known history of chest chemoradiotherapy or surgical treatment; (6) KPS ≥ 70; and (7) patients without any contraindications for chemoradiotherapy. The exclusion criteria were as follows: (1) patients were unable to adhere to a semi-liquid diet or normal diet; (2) patients with any signs of esophageal perforation, for example, niche, penetrating ulcer, tortuosity, and angulation; and (3) patients with any known history of systemic heart, liver, and kidney diseases.
Magnetic Resonance Imaging
A total of 237 patients were instructed to fast and were water-deprived on the day of the concurrent chemoradiotherapy procedure. Patients were required to remove all metal objects. Before the examination, patients were provided with shallow and slow uniform breathing training, while breath-controlled free breathing was used to collect the required signals. A Discovery MR 750 3.0T magnetic resonance scanner (General Electric Company, Boston, USA) and an 8-channel phased-array coil were used. Diffusion-weighted imaging (DWI) and dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) were performed before and after chemoradiotherapy (29 ± 2.1 days after chemoradiotherapy), as well as in the event of the radiation dose reaching 20 Gy (15 ± 1.5 days after chemoradiotherapy). The sequence and parameters for the 3 individual scanning were all consistent. Diffusion-weighted imaging transverse axial scanning was performed using a single-shot, spin-echo and echo-planar imaging (SE-EPI) sequence. During the scanning process, pulse-gating and diaphragm navigation were used. The parameters were as follows: repetition time (TR): 2000 ms; echo time (TE): 73 ms; field of view (FOV): 380 mm × 285 mm; matrix: 128 × 128; number of excitations (NEX): 2; slice thickness: 5 mm; inter-slice spacing: 0 mm; and scanning time: 349 s. The 2 b-values at 0 and 800 s/mm2 were selected during the scanning process of DWI. Sagittal scanning was performed using the contrast agent omniscan (gadodiamide injection) at a dose of 0.5 mmol/kg. After 6 phases of plain scanning, a jet injection was performed using a retention catheter that was placed in the ulnar vein with a high-pressure injector at a speed of 3.0 mL/s. Next, the catheter was irrigated via an intravenous bolus injection with 25 mL of normal saline, followed by a continuous process of 54 phases with a duration of 4.29 seconds per phase. In total, 60 phases and 960 images were acquired (scanning 16 layers per phase and acquiring 1 image per layer). Dynamic enhancement was achieved by liver acquisition with a volume acceleration sequence. The parameters for DCE-MRI were as follows: TR: 4 ms; TE: 1.9 ms; slice thickness: 3.8 mm; interslice spacing: 1.8 mm; FOV: 34 × 34 cm; and matrix: 256 × 192.
Image and Data Processing
According to the images obtained from DWI, when the b value was 0 and 800 s/mm2, the corresponding ADC maps were obtained through DWI image fusion. Thus, lesion sites and the location of enlarged lymph nodes were determined, and the value of ADC was calculated using the following formula: (ADC = ln(SI1/SI2)/(b2-b1), SI1 and SI2 refers to 2 values of signal strength in the ROI at different b-values. 23 The largest and clearest regions on the lesion sites from the images of dynamic scanning were selected as the ROI. Each ROI was measured 3 times, and 3 ADC values were subsequently obtained, that is, the maximum one as ADCmax, the mean 1 as ADCmean, and the minimum 1 as ADCmin. The ROI of each ADC was intended to reside in the same vicinity. Ktrans was measured using the 2-compartment model CINETOOL version 2 software (General Electric Company), which was equal to the product of permeability and the surface area per unit of volume, of the capillary wall. The CINETOOL version 2 software, washin-Ax Vibrant + C (phase 12) was combined with washout-Ax Vibrant + C (phase 10). MODEL mode was selected as the arterial input function. The data were analyzed using CINE software, which facilitated the automatic procurement of Ktrans maps.
Treatment Regimens
The dynamic Collimation Radiotherapy (dCRT) protocol comprised of neoadjuvant and concurrent chemotherapy (each 2 cycles). Cisplatin (60 mg/m2) was administrated for 3 weeks, with a continuous infusion dosage of capecitabine at 625 mg/m2/d. In the cases of elderly patients, or with that of patients exhibiting poor performance, the protocol was adjusted accordingly. Radiotherapy was administrated at a dose of 40 Gy in 20 fractions over a period of 4 weeks, and neoadjuvant and concurrent chemotherapy were also prescribed (1 cycle each). Since 2007, during the neoadjuvant and concurrent phase of the protocol, 625 mg/m2 capecitabine was used in place of the regiment of fluorouracil twice a day. The neoadjuvant chemotherapy allowed for systemic treatment to begin earlier, thus allowing for a rapid improvement in patient’s dysphagia, while allowing an adequate amount of time for circumspect planning in relation to conformal radiotherapy. Regarding patients with adenocarcinoma, epirubicin was added to the neoadjuvant chemotherapy regimen; however, this was omitted during the radiotherapy process.
Efficacy Evaluation
Six weeks after chemoradiotherapy, patients with EC underwent an esophageal barium meal diagnostic examination, gastroscopy, and an enhanced chest computed tomography (CT). The response of tumors to chemoradiotherapy was evaluated on the basis of the results from the aforementioned diagnostic tests and in accordance with the efficacy evaluation standards of response in connection with the Evaluation Criteria of Solid Tumors 1.1 24 : complete response (CR) referred to a scenario in which all lesions had disappeared; partial response (PR) referred to a decrease in the sum of the maximum diameter of the primary lesion and a decrease in lymph-node metastasis ≥30%; stable disease (SD) referred to the length of the primary lesion, while the lymph-node metastasis was between PR and PD; and progressive disease (PD) which referred to an increase in the sum of the maximum diameter of the primary lesion as well as an increase in lymph-node metastasis ≥20%, in addition to the appearance of a new lesion was considered as PD. Patients with CR and PR were assigned to the sensitive group, while those with SD and PD were placed into the resistant group. Calculation of the tumor size reduction rate was as follows: magnetic resonance imaging and CT were performed on all patients 6 months after chemoradiotherapy. The tumor size reduction rate was calculated in combination with the diameter of the tumor using CT before chemoradiotherapy. Calculation formula: tumor size reduction rate = (diameter of the tumor before chemoradiotherapy − diameter of the tumor 6 weeks after chemoradiotherapy) / diameter of the tumor before chemoradiotherapy ×100%.
Follow-Up Process
All patients with EC were subject to a follow-up process. The process started on the first day of treatment until the death of the patient, the final follow-up, or in a scenario where a patient was lost to the follow-up. The last follow-up was conducted in June 2016. The follow-up process was conducted either by means of telephone or via outpatient. The survival time was calculated on a monthly basis. A 5-year total survival time and rate were then calculated accordingly, of which, 106 cases were confirmed to have died and 19 cases were lost to follow-up.
Statistical Analysis
SPSS 22.0 (IBM-SPSS Inc, Chicago, Illinois) was used to statically analyze all data collected. Measurement data were presented as mean (standard deviation [SD]). The collected data from the study were subject to normal distribution and nonnormal distribution, which were subsequently analyzed by a t test and by a Kruskal-Wallis H test. Enumeration data were presented as percentage or ratio, and tested by χ2. Correlation analysis was evaluated using a Pearson correlation analysis. The diagnostic value regarding the sensitivity of chemoradiotherapy was analyzed in concert with the receiver operating characteristic (ROC) curve. A Kaplan-Meier curve was constructed to analyze the survival of all patients with EC and tested using log-rank. The risk factors in relation to the prognoses of the patients with EC were evaluated using the Cox proportional hazard model. P < .05 was considered to be statistically significant.
Results
The Baseline Characteristics of Patients With EC Between the Sensitive and Resistant Groups
Among the 237 patients with EC in this study, there were 137 cases in the sensitive group (37 cases with CR + 95 cases with PR), while 105 cases in the resistant group (76 cases with SD + 29 cases with PD). No apparent statistical differences were detected between the sensitive and resistant groups in relation to the factors of age, gender, KPS, lesion site, length of lesion, pathological type, T stage, clinical stage, and degree of differentiation (all P > .05; Supplemental Table 1). Comparisons of Ktrans and ADC between the sensitive and resistant groups before and after chemoradiotherapy. The ADC and Ktrans representative maps from both the sensitive and resistant groups are illustrated in Figure 1. The statistical analyses results are depicted in Table 1. The Ktrans of both groups displayed notably decreased levels following chemoradiotherapy (both P < .05). The Ktrans of the sensitive group was considerably higher than that of the resistant group both before and after chemoradiotherapy (both P < .05). The ADCmin, ADCmean, and ADCmax of both groups exhibited distinct increases postchemoradiotherapy (all P < .05). The ADCmin, ADCmean, and ADCmax of the sensitive group were lower than those of the resistant group before chemoradiotherapy, but higher than those of the resistant group after chemoradiotherapy (all P < .05).
Comparisons of Ktrans and ADC Between the Sensitive and Resistant Groups Before and After Chemoradiotherapy.

Abbreviations: ADC, apparent diffusion coefficient; Ktrans, volume transfer constant; pre-, before chemoradiotherapy; post-, after chemoradiotherapy.
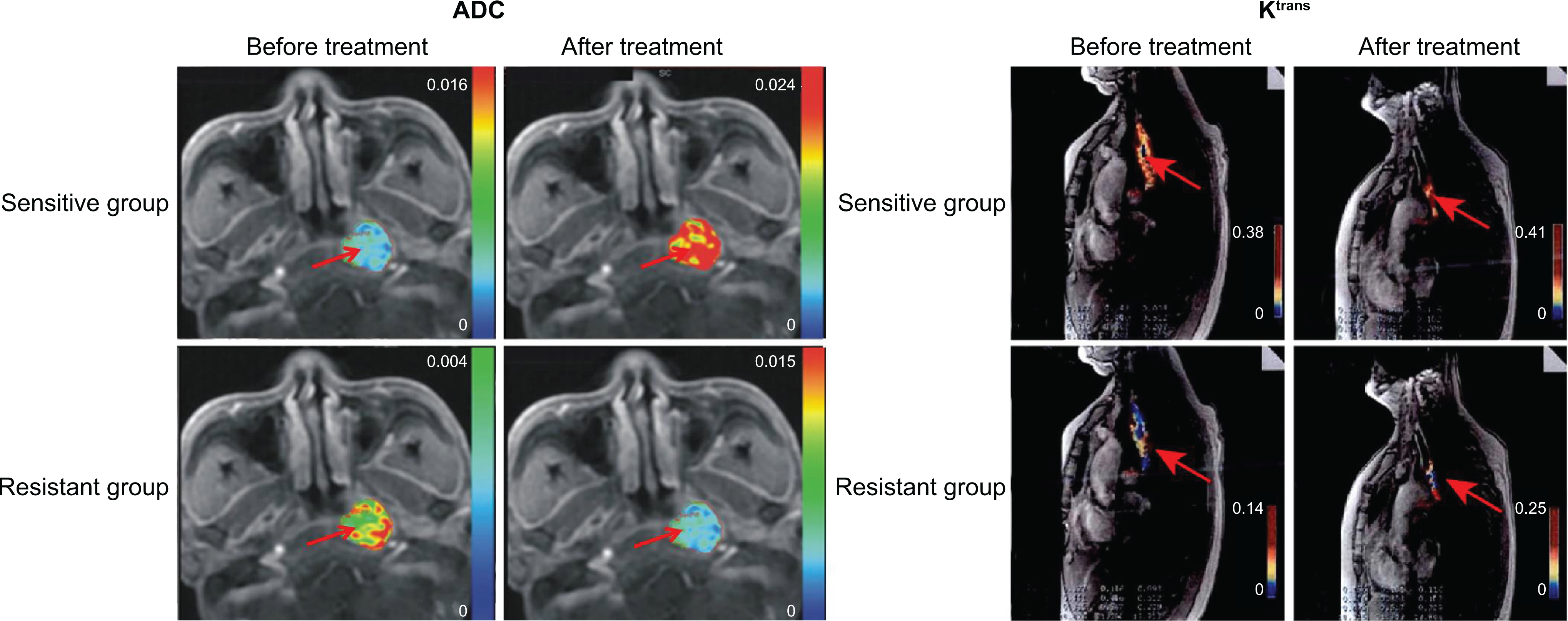
The ADC and Ktrans representative maps in the sensitive and resistant groups. The Ktrans range is 0.000 to 1.000; the arm colors correspond to the higher the values. The arrow marked tumor region. ADC indicates apparent diffusion coefficient; Ktrans, volume transfer constant.
Pearson Correlation Analysis of Ktrans, ADC, and the Tumor Size Reduction Rate Before and After Chemoradiotherapy
The tumor size reduction rate of the sensitive group was observed to be much higher than that of the resistant group (63.53% ± 12.90% vs 16.35% ± 10.74%; t = 30.07, P < .05). Pearson correlation analysis of ADC, Ktrans, and the tumor size reduction rate before and after chemoradiotherapy demonstrated that ADCmin, ADCmean, and ADCmax of both groups as being negatively correlated with the tumor size reduction rate before chemoradiotherapy (all P < .05), while displaying a positive correlation with the rate of tumor regression following chemoradiotherapy (all P < .05). Both groups displayed a positive correlation between Ktrans and the tumor size reduction rate before and after chemoradiotherapy (all P < .05; Table 2).
Pearson Correlation Analysis of Ktrans and ADC and Tumor Regression Rate Before and After Chemoradiotherapy.

Abbreviations: ADC, apparent diffusion coefficient; Ktrans, volume transfer constant; pre-, before chemoradiotherapy; post-, after chemoradiotherapy.
ROC Analysis for the Diagnostic Value of Ktrans and ADC in Regard to the Short-Term Efficacy of Chemoradiotherapy in Patients With EC
According to the ROC analysis, the efficacy of chemoradiotherapy in regard to the treatment of EC was best evaluated at the point where ADCmin prior to chemoradiotherapy was at a threshold of 1.155 × 10−3 mm2/s; sensitivity was 75.2%, specificity was 87.9%, and the area under the ROC curve (AUC) was 0.885. The efficacy of chemoradiotherapy in the treatment of EC was best evaluated when the ADCmean before chemoradiotherapy at the point where 1.525×10-3 mm2/s was the threshold; sensitivity was 78.1%, specificity was 59.1%, and AUC was 0.738. The efficacy of chemoradiotherapy in treatment of EC was best evaluated when ADCmax before chemoradiotherapy was at a threshold of 1.565 × 10−3 mm2/s; sensitivity was 87.6%, specificity was 76.5%, and AUC was 0.873. The efficacy of chemoradiotherapy in the treatment of EC was best evaluated when Ktrans before chemoradiotherapy was at a threshold of 0.505 min−1; sensitivity was 89.4%, specificity was 57.1%, and AUC was 0.814 (Figure 2).

Receiver operating characteristic analysis in relation to the diagnostic value of Ktrans and ADC in short-term efficacy of chemoradiotherapy in patients with EC. A, ROC analysis in relation to the diagnostic value of ADCmin before chemoradiotherapy in the efficacy of chemoradiotherapy in patients with EC. B, ROC analysis in relation to the diagnostic value of ADCmean before chemoradiotherapy in the efficacy of chemoradiotherapy in patients with EC. C, ROC analysis in relation to the diagnostic value of ADCmax before chemoradiotherapy in the efficacy of chemoradiotherapy in patients with EC. D, ROC analysis in relation to the diagnostic value of Ktrans before chemoradiotherapy in the efficacy of chemoradiotherapy in patients with EC. ADC indicates apparent diffusion coefficient; EC, esophageal cancer; Ktrans, volume transfer constant; ROC, receiver operating characteristic curve.
Cox Proportional Hazard Model as Risk Factors in the Prognosis of Patients With EC
Kaplan-Meier survival curves were graphed for all patients with EC. During the 5-year follow-up process, 106 cases were confirmed to have died, while 19 (8%) cases were lost to follow-up. The total survival rate was 46.84%, and the total survival time was 44.8 months. In the sensitive and resistant groups, patients with EC having high ADCmin (≥1.155 × 10−3 mm2/s), ADCmean (≥1.525 × 10−3 mm2/s), ADCmax (≥1.565 × 10−3 mm2/s), and Ktrans (≥0.505 min−1) had a greater 5-year survival rate than those with low ADCmin (<1.155 × 10−3 mm2/s), ADCmean (<1.525 × 10−3 mm2/s), ADCmax (<1.565 × 10−3 mm2/s), and Ktrans (<0.505 min−1; all P < .05; Figure 3). According to the COX proportional hazard model, the ADCmean, clinical stage, degree of differentiation, and T stage were all highlighted as being independent risk factors in the prognosis of patients with EC (all P < .05; Table 3).

Kaplan-Meier curves for survival analysis of patients with EC. A, Kaplan-Meier curve of ADCmin in the sensitive and resistant groups. B, Kaplan-Meier curve of ADCmean in the sensitive and resistant groups. C, Kaplan-Meier curve of ADCmax in the sensitive and resistant groups. D, Kaplan-Meier curve of Ktrans in the sensitive and resistant groups; ADC indicates apparent diffusion coefficient; EC, esophageal cancer; Ktrans, volume transfer constant.
Cox Proportional Hazard Model for Risk Factors for Prognosis of Patients With Esophageal Cancer.

Abbreviations: ADC, apparent diffusion coefficient; CI, confidence interval; Ktrans, volume transfer constant; KPS, Karnofsky performance score.
Discussion
Recent years have brought with them truly great advancements regarding screening and multimodality treatment processes for the treatment of EC. However, this being said, EC outcomes remain particularly poor. This highlights the imperative role and requirement of both early detection and prognostic markers in the treatment of EC. 25 During this study, we investigated the values of Ktrans and ADC in regard to the evaluation of chemoradiotherapy for patients with EC. The results of this study highlighted the strength possessed by both Ktrans and ADC, and their potential to be used as significant clinical tools in predicting the efficacy of chemoradiotherapy for patients with EC.
A particular key finding of our study was the detection of the negative relationship shared between Ktrans and the efficacy of chemoradiotherapy for patients with EC. Volume transfer constant is estimated by analyzing the temporarily obtained DCE-MRI data. This is largely an indirect measurement of the physiological parameters involved in the changes in the connection with vascular attenuation and angiogenic activity. 26 Volume transfer constant is a perfusion parameter embodying the vascular transfer coefficient and reflecting vascular permeability 27 . In certain tumors, Ktrans is regarded as comprising of a reflection of vascular permeability, which has demonstrated its potential ability as a tumor grading tool and capability in the determination of the progression of diseases and treatment response 28 . During our study, after chemoradiotherapy, the Ktrans values were observed to have decreased accordingly. Additionally, the Ktrans values were significantly higher in the sensitive group than that of the resistant group. These results were consistent with previously conducted studies, which highlighted that a decrease in Ktrans was in fact connected to a reduction in vascular permeability as well as tumor vascular density.
Furthermore, reports have revealed Ktrans as being a pharmacodynamics indicator of anti-angiogenesis therapy 29 . The higher value indicated an improved delivery of tumor 30 , which provided further support for our results obtained, in addition to the negative association that we observed between the Ktrans value and the tumor size reduction rate. Furthermore, our results were suggestive of a positive relationship shared between ADC and the efficacy of chemoradiotherapy in patients having EC. The ADC value, obtained from DWI, is a physiological parameter that is calculated on the basis of the features of water diffusion in the tissue of the ROI. 31 Apparent diffusion coefficient measurement plays an important part in the detection and determination of malignancy, the assessment of treatment response, and the features of lesions. 32 Generally speaking, high ADC values imply the corresponding tissue to be normal, with low cellularity and good tissue structure. On the contrary, low ADC values are reflective of malignancy in the corresponding tissue with high cellularity. 33 In tumors, a lower ADC value has been demonstrated to be linked with higher cell density, while higher ADC values have been widely observed in necrotic and edematous regions. 31 The major result of our study revealed that after chemoradiotherapy treatment, the ADC values in the sensitive and resistant groups have increased in addition to a positive correlation detected between the ADC values and the tumor size reduction rate. Thus, it highlights the potential of ADC in evaluating the clinical response to chemoradiotherapy for patients with EC in an effective manner. Diffusion-weighted imaging is able to differentiate between malignant and nonmalignant lesions, exhibiting a better performance for mass evaluation. 34 Furthermore, reports have indicated that ADC obtained from DWI is capable of acting as a biomarker in the evaluation of early responses to treatment in various forms of cancer. 35 Consistent with clinical literature, during our study, a significant change in tumor ADC values was observed following chemoradiotherapy treatment, which we considered as being positive response to therapy. 36 During this study, a relatively sharp difference in ADC values was observed before and after chemoradiotherapy treatment. Thus, it was subsequently deduced that ADC was of particularly high effectiveness in relation to the evaluation of clinical responses to chemoradiotherapy in patients with EC. Makino et al during their study demonstrated that ADC measurement to be effective in the early assessment of clinical responses to chemoradiotherapy in patients with cervical cancer. 33
In addition, it was revealed during this study that ADCmean, clinical stages, degree of differentiation, and T stages were all independent prognostic factors in relation to the overall survival of patients with EC. A previous study demonstrated that ADCmean could reflect the features of a tumor including tumor aggressiveness, which as a result could be regarded as a useful biomarker for patients with cervical cancer. 37 Our results revealed that the overall survival of patients with EC having higher ADCmean was higher than those with lower ADCmean. It was also revealed in our study that both Ktrans and ADC values displayed variations in patients at different clinical and T stages, as well as with different degrees of differentiation. This suggested that the clinical stages, degree of differentiation, and T stages all share a relationship with both Ktrans and ADC values, which were all confirmed as having a close correlation with the prognosis of patients with EC.
In summary, the results and observations of our study provided significant evidence suggesting that both Ktrans and ADC are effective predictor tools with regard to the efficacy of chemoradiotherapy for patients with EC. Our findings may pave the way for avenues yet to be explored with significant promise in order to enhance the clinical decision-making process. There were certain potential limitations of our study. Firstly, additional radiation exposure was somewhat inevitable. Secondly, the number of cases in our study was relatively small. In order to obtain more conclusive results and facilitate better evaluations, these 2 parameters should be addressed in the future. Additionally, because of the limited equipment conditions in our hospital, we were unable to select a clearer picture. Ultimately, further studies with larger sample size are required in order to further validate the findings of our study.
Supplemental Material
Supplemental Material, supplementary_table_1-TCRT-17-0031.R3 - DCE-MRI-Derived Volume Transfer Constant (Ktrans) and DWI Apparent Diffusion Coefficient as Predictive Markers of Short- and Long-Term Efficacy of Chemoradiotherapy in Patients With Esophageal Cancer
Supplemental Material, supplementary_table_1-TCRT-17-0031.R3 for DCE-MRI-Derived Volume Transfer Constant (Ktrans) and DWI Apparent Diffusion Coefficient as Predictive Markers of Short- and Long-Term Efficacy of Chemoradiotherapy in Patients With Esophageal Cancer by Zhi-Min Ye, Shu-Jun Dai, Feng-Qin Yan, Lei Wang, Jun Fang, Zhen-Fu Fu, and Yue-Zhen Wang in Technology in Cancer Research & Treatment
Footnotes
Acknowledgments
We are grateful for the contributions and useful suggestions of all reviewers on our article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Zhejiang Provincial Natural Science Foundation of China under Grant Nos. LQ15H160001, LY17H160039, LY18H160031, the General Project of Zhejiang Provincial Health Bureau (Grant Nos. 2015KYB063, 2015KYB048, 2016KYA051).
Supplemental Material
Supplementary material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.