
Abstract
Objective:
To investigate the application value of apparent diffusion coefficient value in the pathological type, histologic grade, and presence of lymph node metastases of esophageal carcinoma.
Materials and Methods:
Eighty-six patients with pathologically confirmed esophageal carcinoma were divided into different groups according to pathological type, histological grade, and lymph node status. All patients underwent conventional magnetic resonance imaging and diffusion-weighted imaging scan, and apparent diffusion coefficient values of tumors were measured. Independent sample t test and 1-way variance were used to compare the difference of apparent diffusion coefficient value in different pathological types, histologic grades, and lymph node status. Correlation between the apparent diffusion coefficient value and the histologic grade was evaluated using Spearman rank correlation test. Receiver operating characteristic curve of apparent diffusion coefficient value was generated to evaluate the differential diagnostic efficiency of poorly and well/moderately differentiated esophageal carcinoma.
Results:
No significant difference was observed in apparent diffusion coefficient value between esophageal squamous cell carcinoma and adenocarcinoma and in patients between those with and without lymph node metastases (P > .05). The differences of apparent diffusion coefficient value were statistically significant between different histologic grades of esophageal carcinoma (P < .05). The apparent diffusion coefficient value was positively correlated with histologic grade (rs = 0.802). The apparent diffusion coefficient value ≤1.25 × 10−3 mm2/s as the cutoff value for diagnosis of poorly differentiated esophageal carcinoma with the sensitivity of 84.3%, and the specificity was 94.3%.
Conclusions:
The performance of apparent diffusion coefficient value was contributing to predict the histologic grade of esophageal carcinoma, which might increase lesions characterization before choosing the best therapeutic alternative. However, they do not correlate with pathological type and the presence of lymph node metastases of esophageal carcinoma.
Keywords
Introduction
Esophageal carcinoma is one of the most common digestive carcinomas with a steadily increasing incidence and morbidity in the world. 1 Esophageal cancer mainly includes esophageal squamous cell carcinoma and esophageal adenocarcinoma in accordance with the histopathological appearance of tumor tissues, and esophageal squamous cell carcinoma represents the majority of cases. The overall survival of patients with esophageal carcinoma remains poor, with the 5-year survival ranging from 15% to 20%. 2 The histological tumor grade of esophageal carcinoma is segregated into grade 1 (well differentiated), grade 2 (moderately differentiated), and grade 3 (poorly differentiated) according into the World Health Organization classification. 3 Patients with esophageal carcinoma with poor differentiation have a poorer prognosis compared to those with high and moderate differentiation. Pathological type, histologic grade, and lymph node status of esophageal carcinoma may play a dominant role in the selection of clinical treatment and prediction of the prognosis. However, conventional imaging examination methods were hard to determine the accurate preoperative grading of esophageal carcinoma. 4,5 Endoscopy biopsy of esophagus can be used to diagnosis esophageal cancer and its differentiated grade, although it is an invasive examination and cannot represent the whole grade of the tumor. 6 However, diffusion-weighted magnetic resonance imaging (DW-MRI) is a noninvasive examination that is based on the microscopic Brownian motion of water molecules, and the diffusion of water molecules can be quantitatively expressed by the value of apparent diffusion coefficient (ADC). Diffusion-weighted imaging may reflect the pathological changes of tumor at molecular level, and the ADC values are related to histopathology features. 7 Some studies have found that the ADC value can be used to reflect the pathological type and histologic degree of tumor to a certain extent. 8 -10 Besides, ADC value can also be used to evaluate the early response to neoadjuvant chemotherapy of the tumor. 11 Recently, majority of studies have suggested that DWI may be used for predicting histologic differentiation of tumor by measuring the mean ADC values. 12 -19 However, fewer reports indicate that the ADC value can be served as the objective indicator to estimate the tumor grade and malignant degree of esophageal carcinoma. To our knowledge, the possible correlation between ADC value and the presence of lymph node metastases has not been evaluated in esophageal carcinoma to date. Hence, the purpose of this study is to compare the ADC values of 86 cases of esophageal carcinoma in predicting the pathological type, histologic grade, and presence of lymph node metastases.
Material and Methods
Study Population
As a retrospective study, the requirement for informed consent was waived. Eighty-six patients with histologically confirmed esophageal carcinoma (age range from 50 to 85; 56 males, 30 females) were recruited between June 2015 and December 2018. Of these, pathological type: 73 cases of esophageal squamous cell carcinoma and 13 cases of esophageal adenocarcinoma; lesion location: 25 cases of the upper thoracic part, 32 cases of the middle thoracic part, and 29 cases of the lower thoracic part; pathological grading: 35 cases of poor differentiation, 27 cases of moderate differentiation, and 24 cases of high differentiation; lymph node status: 51 cases with lymph node metastases and 35 cases without lymph node metastases. All the patients received the MRI and DWI examinations, and the pathological results were obtained by surgery at 1 week after examinations. Besides, patients who underwent radiotherapy or chemoradiotherapy were excluded in our study.
Magnetic Resonance Imaging Protocol
Magnetic resonance imaging examinations were performed with a 1.5-T MR scanner (Magnetom Avanto; Siemens Medical Systems, Erlangen, Germany) with a 16-channel phase array body coils for anatomic coverage of the chest and upper abdomen. The conventional esophagus MRI protocol included (1) T1-weighted imaging (T1WI) axial scan (time to repeat [TR]: 140 milliseconds; echo time [TE]: 2.5 milliseconds; matrix, 256 × 256; field of view [FOV], 36 cm × 36 cm; layer thickness, 6.0 mm; and interlayer interval, 20%); (2) T2WI axial scan (TR: 1580 milliseconds; TE: 72 milliseconds; matrix, 384 × 276; FOV, 35 cm × 35 cm; layer thickness, 6.0 mm; and interlayer interval, 20%); and (3) DWI axial scan (TR: 6800 milliseconds; TE: 70 milliseconds; matrix, 128 × 128; FOV, 40 cm × 40 cm; layer thickness, 4.0 mm; and interlayer interval, 0%) using the single-shot spin-echo-echo-planar imaging (SE-EPI) sequence. Two different diffusion-sensitive factors were simultaneously collected during the scans: b = 0 and 700 s/mm2.
Imaging Analysis
All images were anonymized and reviewed on a workstation (Siemens Sygno) by 2 senior radiologists with 20 years of experience in esophageal MRI. The reviewers were blinded to the pathologic types and histologic grades of esophageal carcinoma. The region of interest (ROI) was placed to include the target lesion on the ADC map and exclude the necrotic or hemorrhagic areas in the tumor according to T1WI and T2WI. Area of ROI was no less than 50 mm2. The ADC value of each ROI was recorded in every level of the tumor and calculated the mean ADC value of all the levels. If the size of the lesion was less than 3 levels, 3 different parts were taken for measurement and calculate the mean value.
Statistical Analysis
The data were analyzed using SPSS version 19.0 and the mean quantitative data were expressed as mean ± standard deviation. A modified Kolmogorov-Smirnov test evaluated the data distribution normality. Independent sample t test was used to compare the ADC values between the 2 pathological type groups (esophageal squamous carcinoma vs esophageal adenocarcinoma) and the 2 lymph node groups (with lymph node metastases and without lymph node metastases). One-way analysis of variance with least square difference post hoc test was used to compare the ADC value between the different histologic grade groups (poor differentiation vs moderate differentiation vs high differentiation). Spearman rank correlation test was used to compare the correlation between the ADC value and the histologic grade of esophageal cancer. Receiver operator characteristic (ROC) curves were performed for assessing the efficacy of ADC value in the identification of poorly differentiated and moderately to highly differentiated esophageal cancer. The ADC value that corresponded to Youden Index (Youden Index = sensitivity + specificity − 1) was chosen as optimal ADC threshold value. Interobserver agreement in measuring the ADC value was assessed by calculating an intraclass correlation coefficient (ICC). A level of P < .05 was considered statistically significant.
Results
Patient Background and MRI Features
Patients had a mean age of 68.4 ± 8.2 years (range: 50-85 years), and 56 (65%) of them were male. Pathologic tumor type consisted of either squamous cell carcinoma (n = 73, 85%) or adenocarcinoma (n = 13, 15%). Twenty-five lesions were located in the upper thoracic part, 32 were located in the middle thoracic part, and 29 were located in the lower thoracic part. In addition, there were 35 lesions confirmed to poor differentiation, 27 lesions of moderate differentiation, and 24 lesion of high differentiation. Patient- and tumor-related characteristics were summarized in Table 1. Characteristic MRI features of esophageal cancer were esophageal wall thicken asymmetrically and its lumen narrowed irregularly on T1WI. The high signal annular mucosa was disrupted on T2WI and presented with obviously inhomogeneous high signal on DWI. While on the ADC map, the lesion showed with low signal (Figures 1 and 2).
Patient and Tumor-Related Characteristics.a

a Data are the mean ± standard deviation.

A 68-year-old man with upper poorly differentiated esophageal squamous carcinomas. A, On T1WI, upper esophageal wall thicken asymmetrically with iso-intensity and its lumen arrowed irregularly. B, On T2WI, the lesion was shown with slightly high signal and the high signal mucosa was interrupted. C, On DWI, the lesion was shown with obviously heterogeneous high signal. D, On ADC map, the lesion was shown with low signal. ADC indicates apparent diffusion coefficient; DWI, diffusion-weighted imaging; T1WI, T1-weighted imaging; T2WI, T2-weighted imaging.

A 57-year-old man with lower segment of moderately differentiated esophageal adenocarcinoma. A, On T1WI, lower segment of esophageal wall thicken asymmetrically and established soft-tissue mass with iso-intensity. B, On T2WI, the lesion was shown with slightly high signal and the high signal mucosa was interrupted. C, On DWI, the lesion was shown with obviously high signal. D, On ADC map, the lesion was shown with low signal. ADC indicates apparent diffusion coefficient; DWI, diffusion-weighted imaging; T1WI, T1-weighted imaging; T2WI, T2-weighted imaging.
Comparison of ADC Values of Esophageal Carcinoma Between Different Pathologic Types, Histologic Grades, and the Presence of Lymph Node Metastases
The ADC value was (1.51 ± 0.28) × 10−3 and (1.38 ± 0.25) × 10−3 mm2/s for esophageal squamous carcinoma and esophageal adenocarcinoma, respectively. The ADC value of the group with lymph node metastases was (1.55 ± 0.20) × 10−3 and for the group without lymph node metastases was (1.63 ± 0.10) × 10−3 mm2/s. No significant differences were found between these 2 groups (P < .05). All samples were divided into poor differentiation group (35 cases), moderate differentiation group (27 cases), and high differentiation group (24 cases). The ADC values of the 3 groups were (1.28 ± 0.14) × 10−3, (1.49 ± 0.17) × 10−3, and (1.82 ± 0.23) × 10−3 mm2/s, respectively. Significant differences of ADC values were found between the intragroups (Table 2). A box plot comparing the ADC values of the 3 different differentiation groups is shown in Figure 3.
Comparison of ADC Values Among Different Pathological Grades of Esophageal Carcinoma.a

Abbreviations: ADC, apparent diffusion coefficient; EAC, esophageal adenocarcinoma; ESC, esophageal squamous carcinoma; high, high differentiation; moderate, moderate differentiation; poor, poor differentiation.
a Data are the mean ± standard deviation; P < .05 is considered statistically significant.

Box plot comparison of the apparent diffusion coefficient (ADC) values among different histologic grades. Mean ADC values were statistically different between G1 (high differentiation group) and G2 (moderate differentiation group), G1 and G3 (poor differentiation group), and G2 and G3 of esophageal carcinoma.
Correlation Between ADC Values of Esophageal Carcinoma and the Histologic Grade
Positive correlation between ADC value of esophageal carcinoma and the histologic grade was found in our study (rs = 0.802). Namely, as the degree of tumor differentiation decreased, the value of ADC will decrease similarly.
Interobserver Agreement
Intraclass correlation coefficient for the measurement of ADC value between both readers was 0.89 (95% confidence interval, 0.80-0.92). The ICC value ranges from 0 to 1, and the level was defined as follows: ICC < 0.2, poor; ICC = 0.2 to 0.4, fair; ICC = 0.4 to 0.6, moderate; ICC = 0.6 to 0.8, good; and ICC = 0.8 to 1.0, excellent.
Receiver Operator Characteristic Curves of ADC Value of Esophageal Carcinoma in Differentiation of Histologic Grade
In the identification of poorly and well/moderately differentiated esophageal carcinoma, the area under the ROC curve (AUC) of ADC was 0.901. Therefore, ADC value has higher diagnosis efficacy in the identification of the degree of histologic grade of esophageal carcinoma. The ADC cutoff value was set at 1.25 × 10−3 mm2/s for the differentiation between poorly and well/moderately differentiated esophageal carcinoma, with the sensitivity and specificity of 84.3% and 94.3%, respectively (Figure 4).
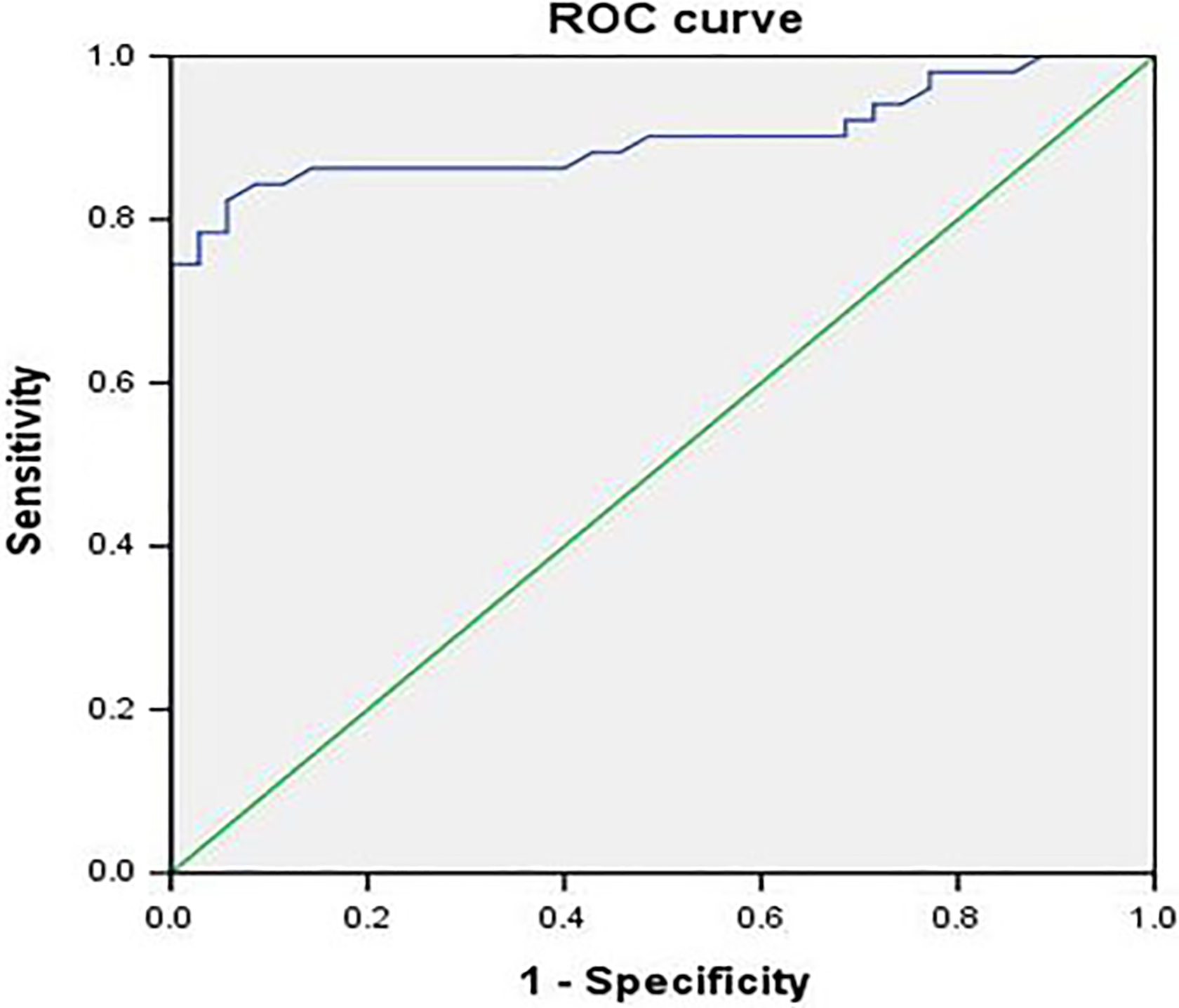
Receiver operating characteristic (ROC) curves of ADC values for differentiating between different histologic grades of esophageal carcinoma. The ROC curve showed that ADC value has higher diagnosis efficacy in the identification of the degree of histologic grade of esophageal carcinoma. The mean area under the ROC (AUC) was 0.901 with the cutoff value of 1.25 × 10−3 mm2/s for the differentiation between poorly and well/moderately differentiated esophageal carcinoma, and the sensitivity and specificity of 84.3% and 94.3%, respectively. ADC indicates apparent diffusion coefficient; AUC, areas under the ROC curves.
Discussion
Esophageal carcinoma ranks the eighth most common cancer in the world and the sixth most cause of death due to cancer. 20 Pathological characteristics are important prognostic factors in patients with esophageal cancer. Pathological type, histologic grade, and lymph node metastases status may determine the prognosis, the therapy, and patient survival. Precise prediction of pathological grade before operation is extremely important to determine the suitable clinical treatment and influence the prognosis. Diffusion-weighted imaging is a noninvasive imaging method, which can probe molecular diffusion of water on the microscopic scale and then reflect histopathological features of the tumors. The value of ADC could be used as objective and quantitative parameter for DWI. Esophageal squamous cell carcinomas represent the majority of esophageal carcinoma cases compared to adenocarcinomas. In this study, we want to know whether ADC value differs between squamous cell carcinomas and adenocarcinomas. Although results in our study demonstrate that there was no relationship between the ADC values of esophageal carcinoma with the histologic type.
Different histologic grades of esophageal carcinomas may have different ADC values theoretically. In malignant tumors, we discovered tissue invasion and cancer nets exhibiting increased cellularity and enlarged cells. The diffusion of water molecules in malignant tumors was limited by hypercellularity, enlarged nuclei, hyperchromatism, high nuclear to cytoplasmic ratio, and reduced extracellular space. 21 On pathology, the less differentiated grade of the tumor, the larger and dense the tumor cells will be, the more restricted the free diffusion of water molecules will be, and then lead to the lower ADC value finally. Hence, we want to know whether ADC value differs between different histologic grades of esophageal carcinomas. Our study showed that the differences of ADC values of esophageal carcinoma were statistically significant between different histologic grades. Previous researches have shown that the ADC values were associated with the tumor histologic grade. Tanaka et al 22 found that high-grade tumors had lower ADC values than low-grade tumors among 91 patients with endometrioid endometrial cancer. Ahmet et al 23 demonstrated that the size and Fuhrman grade of the clear cell renal cell carcinoma were inversely correlated with the ADC value. Yazdani et al 24 showed that significantly lower mean ADC values in high-grade compared to low-grade gliomas. Zhu et al 25 also reported that the ADC values of poorly differentiated esophageal carcinoma were lower than moderately differentiated and well-differentiated groups. The results in our study were consistent with these findings from previous studies in tumors of the whole body. Nasu et al 26 have found that the tumor pathological grade mainly depends on structural atypia and cellular atypia, while the tumor cellular atypia was mainly influenced by nuclear to cytoplasmic ratio. As the tumor histological grade increases, cellular atypia would increase, free diffusion of water molecules in the intracellular space would decrease and finally lead to a reduced ADC values. Recent researches have indicated that the mean ADC measurement can be used to predict the tumor pathological characteristics. Liu et al 27 found that the ADC value of the lesions decreased gradually from well- to poorly differentiated gastric adenocarcinoma. Li et al 28 demonstrated that the minimum and mean ADC values of hepatocellular carcinoma (HCC) are inversely correlated with tumor histopathological grade and there is no significant difference for their abilities in discrimination between poorly and nonpoorly differentiated HCCs. Watanabe et al 29 reported that ADCs of the meningiomas were inversely correlated with the histological grade and only the ADC value at b = 4000 was significantly correlated with the histological grade of meningiomas. On the basis of identifying the poorly differentiated and well/moderately differentiated esophageal carcinoma, the AUC of ADC was 0.901. Our study showed that the cutoff value of ADC for diagnosing poorly differentiated esophageal carcinoma was ≤1.25 × 10−3 mm2/s with the sensitivity of 84.3% and specificity of 94.3%. The results indicate that ADC value might better evaluate the tumor histologic grade and might increase lesions characterization before choosing the best therapeutic alternative.
As is known to all, lymph node metastases status remains an important prognostic factor and a critical determinant of the management of esophageal carcinoma. 30,31 The differentiation between benign and malignant lymph nodes is important for both staging and determining resectability in cases of esophageal carcinoma. Some studies have reported that DWI can be used to discriminate between metastatic nodes and benign lymph nodes with high degrees of accuracy. 32 -34 While some studies found that there were no differences in ADC value between normal and metastatic nodes. 35 -37 Our study also showed no significant difference in ADC value between patients with esophageal carcinoma with and without lymph node metastases. There are some explanations for those inconsistent results such as MRI parameters, magnetic field, location and area of ROI, sample size, and patient age.
There are some limitations in our study. First, it is prone to selection bias due to the small sample size and unevenly distributed cases of different pathological grades. Second, the ROIs were selected on several levels of the tumor instead of the whole part of the tumor, which may lead to measurement bias. The ADC histogram includes the whole tumor, which might be helpful to increase accuracy of tumor biological evaluation. 38 -41 Further studies using ADC histogram would be applied in my subsequent researches. As the esophagus located in the mediastinum and affected by heartbeat and respiratory movement, it is impossible to get accurate measurement of ADC value in the whole part of esophageal carcinoma. Resolve DWI is superior in this regard. Resolve DWI is less liable to susceptibility artifacts, T2* blurring, and motion-induced phase artifacts and provides higher resolution compared with standard single-shot SE-EPI sequences. 42,43 Third, DWI in our study was performed with 2 b values (0 and 700 s/mm2), while the measurement of ADC value was vulnerable to be affected by microcirculation perfusion. The values of ADC obtained from conventional monoexponential DWI could not accurately reflect the real diffusivity, as the low b values are more susceptible to capillary perfusion. 44 While biexponential DWI intravoxel incoherent motion (IVIM) might provide more accurate information about water diffusion, which contains true diffusivity (D), fraction of perfusion (f), and pseudodiffusion parameter (D*). 45 Further studies using multiple b values of IVIM are needed to explore the application of ADC value in pathological grading of esophageal carcinoma.
Conclusions
The ADC value of esophageal carcinoma was positively correlated with the histologic grade. Therefore, it is helpful to evaluate the histologic grade of esophageal carcinoma before operation by measuring the ADC value. Besides, it might help in stratifying patients and might increase lesions characterization before choosing the best therapeutic alternative.
Footnotes
Authors’ Note
As a retrospective study, the requirement for informed consent was waived.
Acknowledgments
First and foremost, I would appreciate the organization of the affiliated Huaian No. 1 People’s Hospital of Nanjing Medical University which gives me a comfortable learning atmosphere. Second, I would like to show my deepest gratitude to Dr Genji Bai, a respectable, responsible, and resourceful scholar, who has provided me with valuable guidance in every stage of the writing of this thesis. His keen and vigorous academic observation enlightens me not only in this thesis but also in my future study. Last but not least, I shall extend my thanks to all my teachers and colleagues who have helped me to develop the fundamental and essential academic competence.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.