
Abstract
Introduction
Induction chemotherapy (IC) represents a standard treatment approach for locally advanced nasopharyngeal carcinoma (LA-NPC), yet marked interpatient heterogeneity in treatment response persists. This study sought to develop and evaluate a temporal Transformer–based fusion model integrating baseline pretreatment and early intratreatment MRI to facilitate early risk stratification and inform individualized therapeutic management.
Materials and Methods
In this retrospective multicenter study, 488 patients with pathologically confirmed LA-NPC were enrolled from two institutions. All patients underwent induction chemotherapy and received contrast-enhanced T1-weighted imaging (CE-T1WI) before treatment initiation (Pre-IC) and at an early post-treatment time point (Post-IC). A dual-branch independent network architecture with Twins-SVT as the backbone was implemented to separately extract deep learning features from Pre-IC and Post-IC CE-T1WI images. Subsequently, an attention-based temporal Transformer fusion module was designed to model nonlinear longitudinal interactions and dynamic evolutionary patterns between pre- and post-treatment tumor representations, yielding a longitudinal temporal fusion predictive model. Gradient-weighted class activation mapping (Grad-CAM) was applied to enhance interpretability through visualization of salient imaging regions.
Results
The deep learning model based on Pre-IC imaging yielded an AUC of 0.844 (95% CI: 0.767–0.922) in the internal validation cohort and 0.819 (95% CI: 0.725–0.913) in the external validation cohort. The Post-IC–based model demonstrated AUCs of 0.863 (95% CI: 0.790–0.936) and 0.838 (95% CI: 0.753–0.923) in the internal and external validation cohorts, respectively. The longitudinal temporal Transformer fusion model achieved higher predictive performance, with AUCs increasing to 0.889 (95% CI: 0.824–0.955) in the internal validation cohort and 0.865 (95% CI: 0.791–0.939) in the external validation cohort.
Conclusion
Compared with single–time point models, a longitudinal contrast-enhanced MRI–based temporal Transformer fusion model enabled more accurate early individualized prediction of induction chemotherapy response in patients with locally advanced nasopharyngeal carcinoma.
Keywords
Introduction
Nasopharyngeal carcinoma (NPC) is a malignant epithelial tumor arising from the nasopharyngeal mucosa, with approximately 70% of patients presenting with locally advanced disease (LA-NPC) at diagnosis. 1 According to National Comprehensive Cancer Network guidelines, induction chemotherapy (IC) followed by concurrent chemoradiotherapy represents the current standard treatment strategy and has been associated with improved progression-free survival and overall survival.2,3 Despite these therapeutic advances, substantial intratumoral heterogeneity in LA-NPC contributes to marked variability in treatment response, with approximately 20%–30% of patients demonstrating suboptimal response to IC. Overtreatment in potential nonresponders may increase treatment-related toxicity and compromise the timing of subsequent definitive therapy.4,5 Therefore, early identification of patients unlikely to benefit from IC during the treatment course remains critical for individualized management and risk-adapted therapeutic stratification.
Current treatment response assessment primarily relies on the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 and plasma Epstein–Barr virus (EBV) DNA levels. However, morphology-based RECIST evaluation at early treatment stages may not fully capture intratumoral biologic alterations, as subtle mucosal thickening or enhancement changes are often difficult to quantify reliably. In addition, the complex anatomy of the nasopharynx limits the accuracy of two-dimensional measurements. 6 Although plasma EBV-DNA serves as a useful systemic biomarker, it does not comprehensively reflect the spatial heterogeneity of local tumor burden. Furthermore, reliance on single–time point imaging before treatment initiation may be insufficient to characterize dynamic biologic alterations occurring during chemotherapy exposure.7,8 Recent advances in magnetic resonance imaging (MRI)–based radiomics have demonstrated potential for response prediction in NPC by extracting high-throughput quantitative imaging features.9,10 Nevertheless, most studies11,12 have focused predominantly on baseline imaging, thereby overlooking phenotypic alterations occurring during therapy that may encode early treatment-response signals. Delta-radiomics approaches incorporating temporal changes have been proposed13,14; however, these methods typically rely on handcrafted linear feature subtraction (post-treatment minus pre-treatment), which may not adequately model complex nonlinear longitudinal tumor evolution.
Deep learning enables end-to-end representation learning directly from imaging data, reducing dependence on handcrafted feature engineering inherent to conventional radiomics approaches. Transformer architectures incorporating self-attention mechanisms further allow modeling of long-range dependencies and global contextual information.15,16 For longitudinal imaging analysis, dual-branch network architectures enable parallel extraction of temporal features from different treatment phases while temporal attention–based fusion modules facilitate modeling of dynamic tumor microenvironmental evolution during therapy.17,18 Importantly, such capabilities may provide clinically relevant insights into treatment-induced changes and support earlier prediction of therapeutic response.
Accordingly, this study aimed to develop a longitudinal contrast-enhanced MRI (CE-MRI)–based temporal Transformer fusion model for early prediction of induction chemotherapy response in locally advanced nasopharyngeal carcinoma. A dual-branch architecture incorporating Twins-Spatially Separable Vision Transformer (Twins-SVT) as the backbone network was implemented to independently extract tumor-specific deep representations from Pre-IC and Post-IC imaging. These representations were subsequently integrated using an attention-based temporal fusion module to model nonlinear dynamic patterns associated with tumor regression. From a clinical perspective, this approach may assist in early identification of patients unlikely to benefit from induction chemotherapy and support more individualized treatment strategies.
Materials and Methods
Patients
This retrospective study included patients with pathologically confirmed LA-NPC who underwent nasopharyngeal MRI at two medical centers (n = 488) (Figure 1). Specifically, patients from Center 1 (n = 363) were randomly divided into a training cohort (n = 254) and an internal test cohort (n = 109) at a ratio of 7:3. Patients from Center 2 (n = 125) were used as an independent external test cohort. Inclusion criteria were as follows: (1) histopathologically confirmed nasopharyngeal carcinoma with clinical stage III–IVa disease according to the eighth edition of the American Joint Committee on Cancer (AJCC) staging system; (2) completion of three cycles of standard platinum-based induction chemotherapy (IC); (3) baseline MRI acquired before IC and follow-up MRI performed within 1 week after completion of the first IC cycle; (4) complete clinicopathologic and follow-up data. Exclusion criteria were as follows: (1) receipt of any antitumor therapy before IC (radiotherapy or immunotherapy); (2) distant metastasis at diagnosis or concomitant malignancy; (3) missing or poor-quality CE-T1WI; (4) interruption of IC or failure to complete the planned cycles due to severe adverse events. This study was performed in line with the principles of the Declaration of Helsinki (as revised in 2024) and was approved by the Ethics Committee our The Huai’an Second People’s Hospital (Approval No. HEYLL20230053) and the Ethics Committee of The Affiliated Huaian No.1 People’s Hospital of Nanjing Medical University (Approval No. KY-2022-045-01). The requirement for written informed consent was waived because of the retrospective design of the study. This study was conducted and reported in accordance with the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD) guidelines.
19
Flow chart of the patients’ recruitment pathway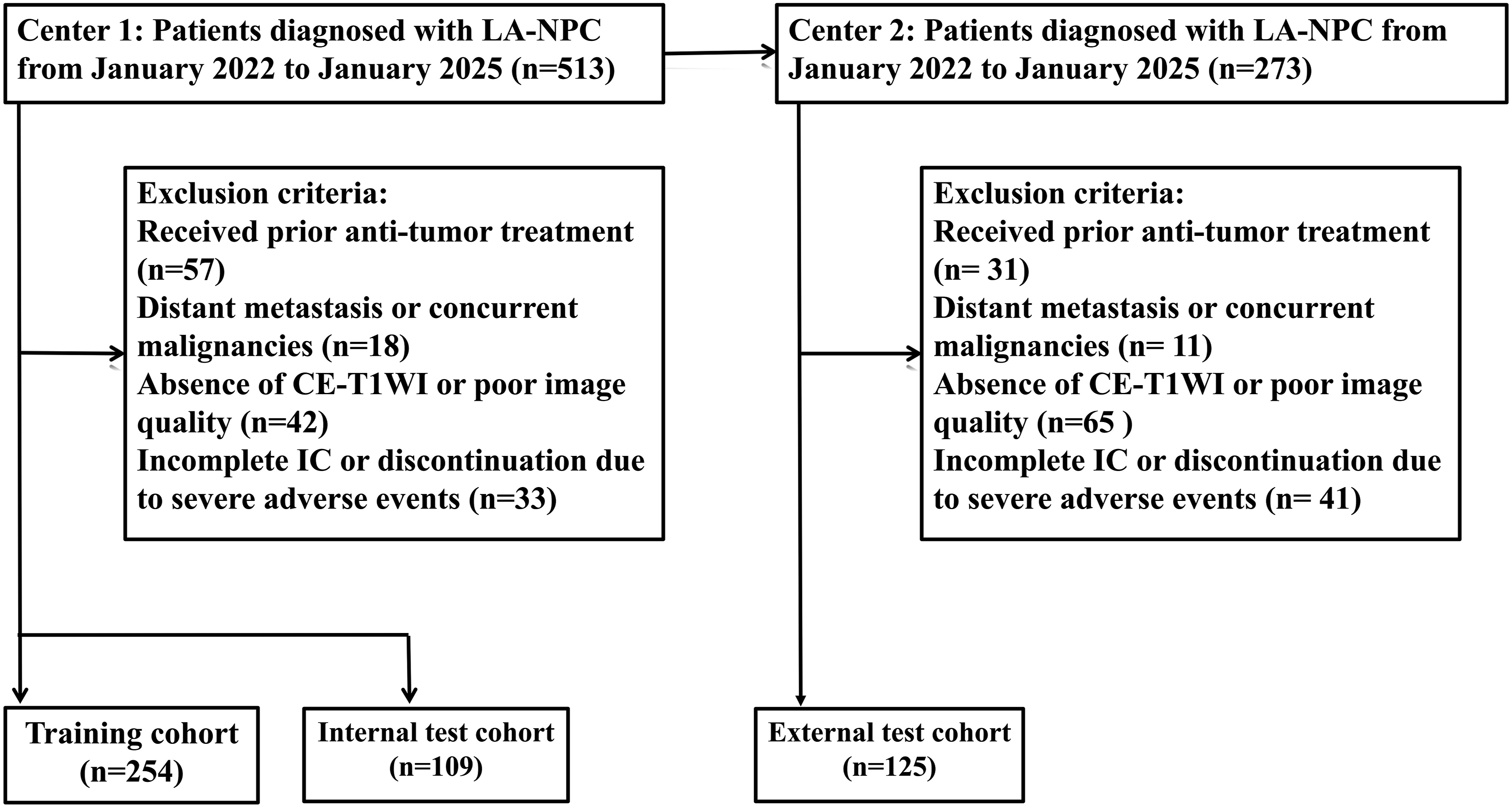
Evaluation of Induction Chemotherapy Efficacy
Treatment response was assessed according to the RECIST, version 1.1. 20 The percentage change in the sum of the longest diameters of target lesions was calculated by comparing CE-T1WI obtained before IC and after completion of IC. Treatment response was categorized as follows: (1) complete response (CR), defined as disappearance of all target lesions and reduction of all pathological lymph nodes to a short-axis diameter < 10 mm; (2) partial response (PR), defined as a ≥30% decrease in the sum of the longest diameters of target lesions compared with baseline; (3) progressive disease (PD), defined as a ≥20% increase in the sum of the longest diameters of target lesions compared with baseline or the appearance of new lesions; and (4) stable disease (SD), defined as neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD. Based on these criteria, patients were further grouped into responders (CR and PR) and nonresponders (SD and PD). All imaging assessments were independently performed on a dedicated imaging workstation by two head and neck radiologists who were blinded to clinical outcome data. In cases of discrepancy, a third senior radiologist adjudicated the findings, and a consensus was reached.
Image Acquisition and Region of Interest Segmentation
MRI data were acquired from two medical centers using protocols that included CE-T1WI (detailed scanner parameters are provided in Supplementary Material 1). All images underwent intensity normalization and resampling to an isotropic voxel size of 1 × 1 × 1 mm3. N4 bias field correction was subsequently applied to reduce intensity inhomogeneity. For each patient, Post-IC images were rigidly registered to the corresponding Pre-IC image space to ensure anatomical alignment, with manual adjustments performed when necessary. Regions of interest (ROIs) were manually delineated using ITK-SNAP (version 3.8.0; https://www.itksnap.org) by two experienced head and neck radiologists who were blinded to treatment response and clinical information. On Pre-IC images, the primary tumor was contoured slice by slice along its margins. On Post-IC images, residual tumor was delineated with reference to the Pre-IC tumor extent; if complete tumor regression was observed, the original tumor bed was contoured. In cases of disagreement, a third senior radiologist reviewed the segmentation to reach consensus. Interobserver segmentation consistency was evaluated using the Dice similarity coefficient (DSC), and cases with DSC > 0.85 were considered to demonstrate high agreement and were included in subsequent analyses.
Deep Learning Model Construction and Feature Fusion
A deep learning framework based on a dual-branch independent architecture was developed, with Twins-SVT serving as the backbone network to extract tumor-specific representations from Pre-IC and Post-IC imaging, respectively. Using the delineated three-dimensional segmentation masks, ROIs were cropped to include the largest tumor slice and its adjacent superior and inferior slices, thereby constructing multi-channel 2.5D input data. This strategy preserved essential spatial contextual information while reducing computational complexity. All ROI images were resized to 224 × 224 pixels and normalized using Z-score standardization before model input to ensure distributional consistency. The preprocessed Pre-IC and Post-IC images were then fed into two parallel branches of the network. Each branch employed Twins-SVT, a hierarchical vision Transformer architecture that integrates locally grouped self-attention (LSA) and globally sub-sampled attention (GSA) mechanisms. The LSA module operates within non-overlapping local windows to capture fine-grained regional texture patterns, enabling efficient modeling of intratumoral heterogeneity. In contrast, the GSA module performs attention on spatially downsampled feature maps, allowing the model to capture long-range dependencies and global contextual information. Leveraging the spatially separable self-attention mechanism of Twins-SVT, hierarchical feature representations were independently extracted through alternating locally grouped self-attention and global sub-sampled attention modules. High-dimensional feature vectors characterizing pre- and post-treatment tumor phenotypes were subsequently generated via branch-specific fully connected layers.
To model longitudinal interactions between treatment phases, a Transformer encoder–based temporal fusion module was constructed. Independent feature vectors from the dual branches were first projected into a shared latent feature space through linear transformation, followed by incorporation of sinusoidal positional encoding to preserve temporal order information. The fusion module comprised six stacked encoder layers, each integrating multi-head self-attention (eight heads) and a position-wise feed-forward network, with residual connections and layer normalization applied to facilitate stable optimization and capture long-range contextual dependencies. Through the self-attention mechanism, the model learns nonlinear cross-temporal dependencies between Pre-IC and Post-IC features, enabling effective integration of temporal evolution patterns beyond simple feature subtraction. A dedicated aggregation token was used to summarize global spatiotemporal representations, and its output embedding was passed through a fully connected layer with a sigmoid activation function to generate the final binary prediction of treatment response (Figure 2). To enhance transparency and reproducibility, the implementation details, including network architecture configuration, training strategy, and hyperparameters, have been made publicly available at our GitHub repository (URL: https://github.com/gf19921111/Longitudinal-MRI-Temporal-Transformer-Fusion-Model). Workflow of the proposed Dual-Branch Temporal Transformer Model. The framework consists of three stages: (Left) Data collection and preprocessing of longitudinal MRI scans from a cohort of 488 patients; (Middle) The deep learning architecture, which utilizes a dual-branch TwinsSVT backbone for feature extraction and a Temporal Transformer Fusion Module with self-attention to capture temporal dynamics for treatment response prediction (Responder vs. Non-Responder); (Right) Comprehensive model evaluation using quantitative performance metrics and Grad-CAM interpretability visualization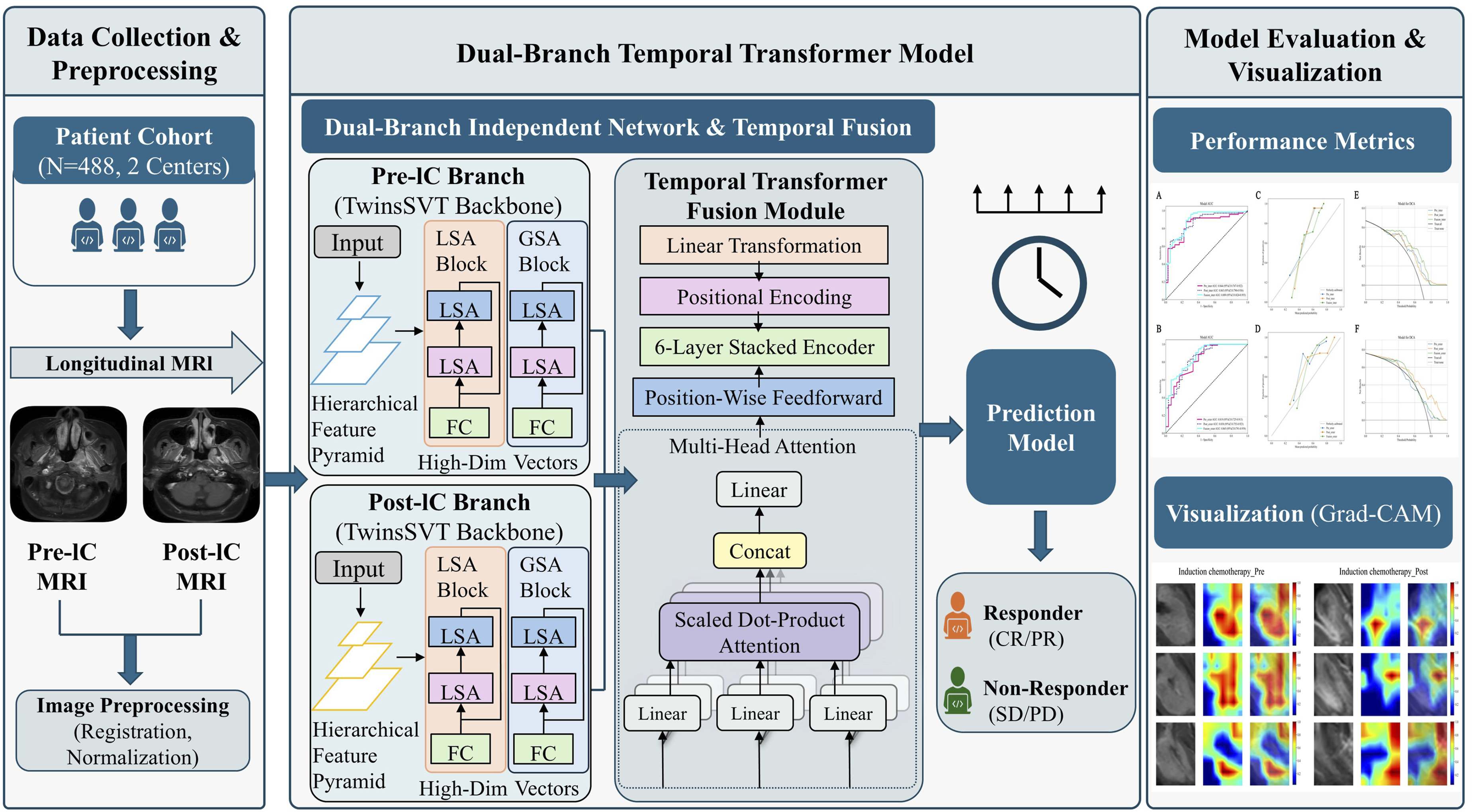
Statistical Analysis
Statistical Analysis Statistical analyses were performed using SPSS (version 25.0), R (version 4.1.2), and Python (version 3.8.5). Continuous variables were analyzed using the Mann-Whitney U test, while categorical variables were evaluated using the Chi-square test or Fisher’s exact test, as appropriate. Model performance was assessed by calculating the Area Under the Curve (AUC) and F1-score. Additionally, sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were measured. The DeLong test was employed to compare the AUCs across different models. Calibration curves were used to assess the accuracy of probability predictions.
Result
Clinical Data
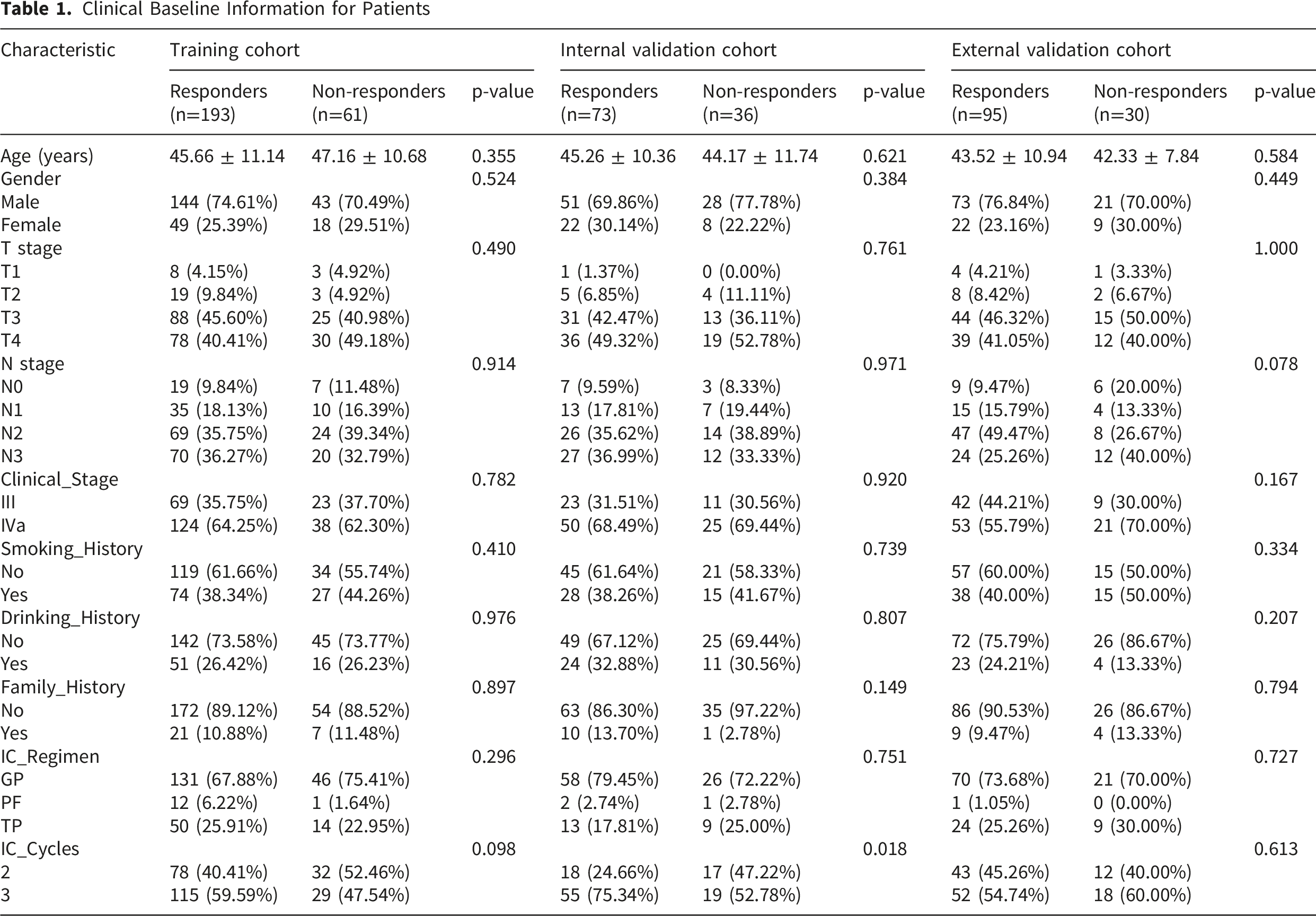
Clinical Baseline Information for Patients
Construction of Single-Timepoint Deep Learning Models
Based on the Twins-SVT backbone, separate single–time point deep learning models were constructed for Pre-IC and Post-IC imaging. The Pre-IC model achieved AUCs of 0.844 (95% CI: 0.767–0.922) and 0.819 (95% CI: 0.725–0.913) in the internal and external validation cohorts, respectively, with corresponding F1-scores of 0.877 (95% CI: 0.797-0.947) and 0.921 (95% CI: 0.879-0.957), the accuracy values were 0.835 (95% CI: 0.761-0.899) and 0.872 (95% CI: 0.808-0.928), the sensitivity values were 0.877 (95% CI: 0.794-0.947) and 0.979 (95% CI: 0.947-1.000), and the specificity values were 0.750 (95% CI: 0.600-0.886) and 0.533 (95% CI: 0.353-0.714). The Post-IC model yielded AUCs of 0.863 (95% CI: 0.790–0.936) and 0.838 (95% CI: 0.753–0.923) in the internal and external validation cohorts, respectively, with F1-scores of 0.780 (95% CI: 0.696-0.857) and 0.856 (95% CI: 0.798-0.907), the accuracy values were 0.752 (95% CI: 0.670-0.835) and 0.792 (95% CI: 0.720-0.864), the sensitivity values were 0.658 (95% CI: 0.554-0.766) and 0.811 (95% CI: 0.725-0.882), and the specificity values were 0.944 (95% CI: 0.857-1.000) and 0.733 (95% CI: 0.565-0.880). DeLong testing demonstrated no statistically significant differences in AUC between the two models in either the internal or external validation cohorts (all P > 0.05). Grad-CAM visualization showed that the Pre-IC model predominantly highlighted intratumoral heterogeneous regions, whereas the Post-IC model more frequently focused on residual enhancement areas and early structural alterations after treatment (Figure 3). Interpretability visualization of model decisions using Grad-CAM. Representative MRI images and their corresponding Grad-CAM heatmaps are displayed for the Pre-Induction Chemotherapy (Pre-IC, left) and Post-Induction Chemotherapy (Post-IC, right) phases
Establishment and Evaluation of the Longitudinal Temporal Fusion Model
Building upon the Transformer-based feature fusion module, a longitudinal temporal fusion model was developed. The model achieved AUCs of 0.889 (95% CI: 0.824–0.955) and 0.865 (95% CI: 0.791–0.939) in the internal and external validation cohorts, respectively (Figure 4A, 4B), with corresponding F1-scores of 0.909 (95% CI: 0.868-0.947) and 0.914 (95% CI: 0.878-0.948), the accuracy values were 0.872 (95% CI: 0.807-0.927) and 0.864 (95% CI: 0.808-0.920), the sensitivity values were 0.959 (95% CI: 0.904-1.000) and 0.947 (95% CI: 0.895-0.989), and the specificity values were 0.694 (95% CI: 0.528-0.833) and 0.600 (95% CI: 0.433-0.767). Compared with the single–time point models, the fusion model demonstrated higher accuracy, sensitivity, and specificity (Table 2). However, DeLong testing indicated no statistically significant differences in AUC between the fusion and single–time point models in either the internal or external validation cohorts (all P > 0.05) (Supplementary Materials 2 and 3). Calibration performance assessed using the Hosmer–Lemeshow test showed good agreement between predicted and observed outcomes in both validation cohorts (P > 0.05), which was consistent with the calibration curves (Figure 4C, 4D). Decision curve analysis demonstrated that within a threshold probability range of 0.2–0.8, the longitudinal fusion model provided greater net clinical benefit than the single–time point models in both validation cohorts (Figure 4E, 4F). To enhance interpretability, SHapley Additive exPlanations (SHAP) analysis was performed for the longitudinal fusion model (Supplementary Material 4), demonstrating that model predictions were derived from integrated cross-temporal feature interactions rather than reliance on baseline features alone. Quantitative performance evaluation of the prediction models in internal and external validation cohorts. (A, B) Receiver Operating Characteristic (ROC) curves comparing the Pre-IC, Post-IC, and Fusion models. (C, D) Calibration curves assessing the agreement between predicted probabilities and observed outcomes. (E, F) Decision Curve Analysis (DCA) illustrating the net clinical benefit of the models across a range of threshold probabilities F1-Score, Sensitivity, Specificity, and AUC Values in the Three Models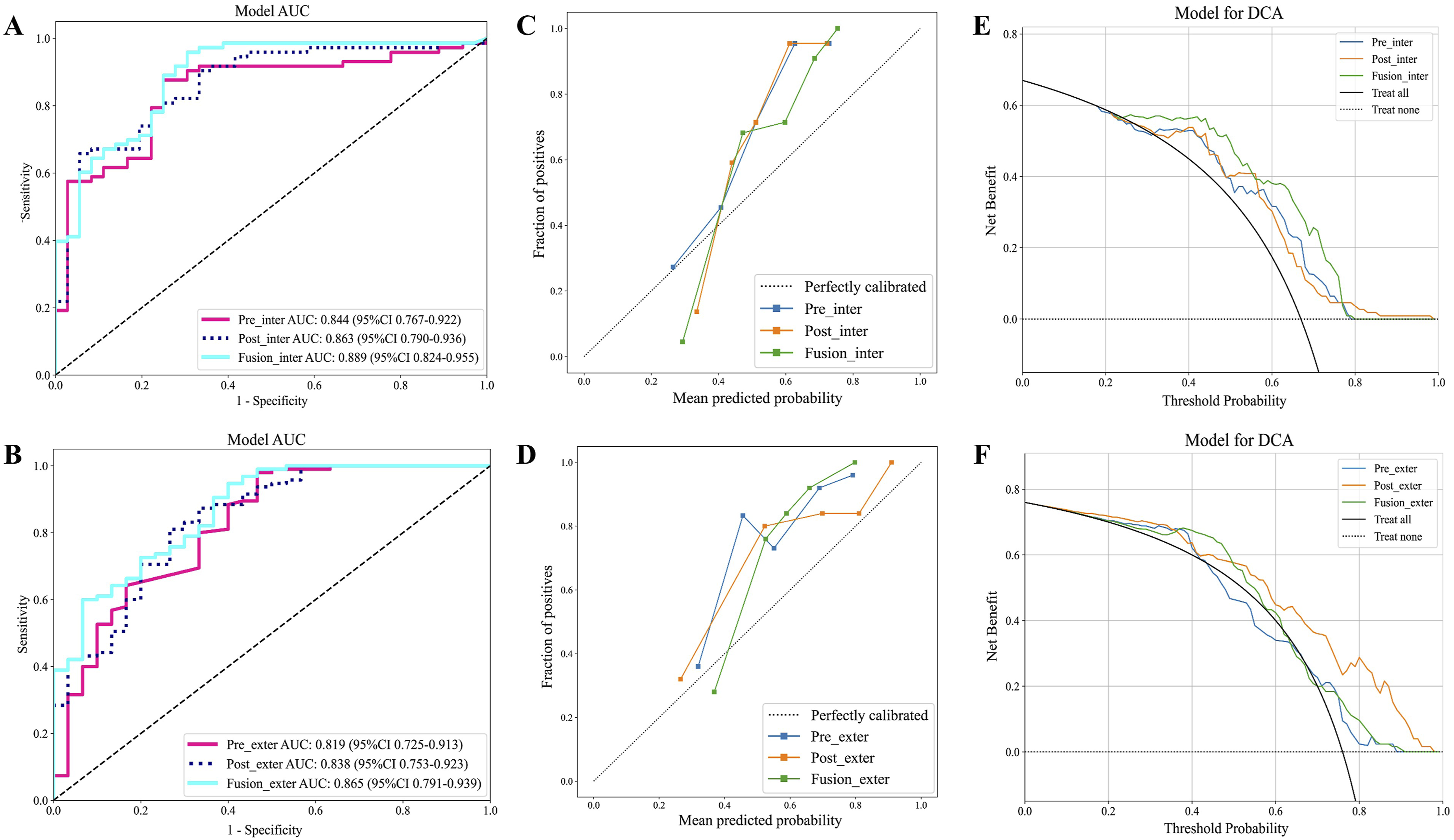

Discussion
This study developed a longitudinal contrast-enhanced MRI–based temporal fusion deep learning model to enable early prediction of induction chemotherapy response in patients with locally advanced nasopharyngeal carcinoma. By integrating deep spatiotemporal representations derived from Pre-IC and Post-IC imaging through a Transformer-based framework, the proposed model demonstrated consistent predictive performance across internal and external validation cohorts. These findings suggest that incorporation of longitudinal imaging information may provide complementary value beyond single–time point assessment in treatment response prediction.
Current clinical response assessment primarily relies on morphology-based RECIST criteria and plasma EBV-DNA levels, both of which have inherent limitations. RECIST depends on bidimensional diameter measurements, which are constrained by the complex anatomy of the nasopharynx and may not fully reflect early cytologic or microenvironmental alterations that precede macroscopic tumor shrinkage.21,22 Although EBV-DNA serves as an important prognostic biomarker, as a circulating indicator it does not capture the spatial heterogeneity of local tumor burden. 23 The present model extends beyond conventional assessment by enabling whole-tumor analysis and longitudinal monitoring. Through extraction of high-dimensional deep representations, the framework characterizes not only morphologic regression but also subtle imaging pattern alterations that may not be visually appreciable. Most prior deep learning studies for treatment response prediction in nasopharyngeal carcinoma have focused predominantly on baseline MRI, without incorporating dynamic changes occurring during therapy. Wang 24 reported that integration of MRI-based radiomics and deep learning features improved prediction of induction chemotherapy response, supporting the complementary value of multimodal features; however, the analysis was restricted to pretreatment imaging. Hu 25 developed an MRI-based deep learning model for stage II nasopharyngeal carcinoma to identify patients at high risk of distant metastasis who might benefit from chemotherapy, thereby informing treatment stratification in intermediate-stage disease. In another study, Wang 26 combined functional MRI–derived tumor perfusion parameters with deep learning radiomic features to construct a high-performing stacked model for radiotherapy response prediction; nevertheless, reliance on arterial spin labeling and other nonroutine imaging sequences may limit broader clinical applicability. In contrast, the present study leverages routinely acquired contrast-enhanced MRI and longitudinal modeling to capture treatment-induced temporal evolution.
Although several studies have attempted to incorporate delta-radiomics to explore longitudinal imaging features, most approaches rely on handcrafted feature subtraction between post-treatment and pretreatment scans, which may not adequately capture complex nonlinear temporal dependencies at the microstructural level. Huang 27 demonstrated that a delta-based model derived from longitudinal CT imaging achieved superior prognostic performance compared with single–time point analysis (C-index, 0.872); however, the relatively limited soft-tissue contrast of CT and the susceptibility of linear subtraction methods to imaging variability may constrain representation of subtle tumor alterations. Wang 28 constructed a delta-radiomics nomogram based on contrast-enhanced MRI that outperformed static models (AUC, 0.874), supporting the clinical value of dynamic monitoring, yet the framework remained dependent on handcrafted feature engineering and segmentation accuracy. Similarly, Pan 29 developed an MRI texture–based longitudinal nomogram for progression-free survival prediction (C-index, 0.820), further underscoring the potential of dynamic features, although conventional radiomic descriptors may be sensitive to segmentation variability and limited in capturing high-dimensional semantic representations. Kou 30 employed a graph convolutional network to integrate serial MRI features before and after induction chemotherapy to predict disease-free survival in locally advanced nasopharyngeal carcinoma (C-index, 0.79), identifying high-risk subgroups who might benefit from concurrent chemoradiotherapy. More recently, Liu 31 proposed a response-adapted individualized risk index model by jointly modeling longitudinal EBV-DNA levels and MRI-based morphologic regression, providing a framework for guiding adjuvant chemotherapy selection and reinforcing the clinical importance of dynamic assessment. Nevertheless, these approaches primarily rely on macroscopic volumetric changes or serum biomarkers, which may not fully reflect early microenvironmental remodeling occurring during treatment.
To better characterize the complex spatiotemporal evolution of locally advanced nasopharyngeal carcinoma during induction chemotherapy, Twins-SVT was adopted as the backbone network within a dual-branch independent architecture. The locally grouped self-attention module functions in a manner analogous to convolution by capturing fine-grained regional texture patterns, which may correspond to subtle intratumoral alterations such as early necrosis or cystic change following chemotherapy. 32 In parallel, the global sub-sampled attention mechanism facilitates modeling of long-range spatial dependencies across the entire field of view, enabling representation of tumor extent and its spatial relationship with adjacent critical structures. 33 The dual-branch independent design, consisting of two structurally identical yet parameter-independent pathways, allows separate modeling of Pre-IC and Post-IC imaging phenotypes. This strategy avoids enforced weight sharing and permits phase-specific feature representation, which may be particularly relevant given the biologic differences between untreated hypercellular tumor tissue and post-treatment residual lesions or fibrosis.34,35 Building upon these representations, the Transformer-based temporal fusion module was introduced to model cross-temporal interactions beyond linear feature subtraction. By learning nonlinear dependencies across treatment phases, the framework enables integration of multidimensional feature relationships rather than relying solely on predefined handcrafted differences. The incorporation of attention mechanisms and token-based aggregation further provides interpretable feature attribution, consistent with prior observations reported by Kim 36 and supports the feasibility of modeling longitudinal tumor evolution using attention-based architectures.
Several limitations should be acknowledged: (1) This was a retrospective study; although data from two centers were included with independent external validation, potential selection bias cannot be entirely excluded. Prospective, multicenter studies with larger sample sizes are warranted to further assess the generalizability of the proposed model. (2) Only contrast-enhanced T1-weighted imaging (CE-T1WI) was analyzed, and the proposed approach was not directly compared with a standalone clinical-variable model; integrating multiparametric MRI sequences and relevant clinical factors may further improve predictive performance. (3) Although the Transformer-based temporal fusion module demonstrated consistent performance, alternative longitudinal fusion strategies could be explored to optimize predictive accuracy.
Conclusion
In summary, this study developed a longitudinal contrast-enhanced MRI–based temporal Transformer fusion model that integrates deep features from baseline and early post-treatment imaging to predict induction chemotherapy response in patients with locally advanced nasopharyngeal carcinoma. Although no statistically significant differences in AUC were observed compared with single–time point models, the proposed model demonstrated favorable trends in predictive performance and showed potential clinical utility for early risk stratification and treatment response assessment. As a noninvasive and objective imaging tool, this approach may provide complementary information during the course of induction chemotherapy, while its clinical applicability warrants further validation in larger, multicenter prospective studies.
Supplemental Material
Supplemental Material - Longitudinal MRI Temporal Transformer Fusion Model for Predicting Induction Chemotherapy Efficacy in Locally Advanced Nasopharyngeal Carcinoma
Supplemental Material for Longitudinal MRI Temporal Transformer Fusion Model for Predicting Induction Chemotherapy Efficacy in Locally Advanced Nasopharyngeal Carcinoma by Lei Han, Xiaoyu Chen, Zhengyu Zhao, Yong Liu, Dongyang Yu, Hui Zhang, Fang Ge in Technology in Cancer Research & Treatment
Footnotes
Acknowledgments
Contributions: (I) Manuscript writing: All authors; (II) Final approval of manuscript: All authors.
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki (as revised in 2024) and was approved by the Ethics Committee of The Huai’an Second People’s Hospital (Approval No.HEYLL20230053) and the Ethics Committee of The Affiliated Huaian No.1 People’s Hospital of Nanjing Medical University (Approval No.KY-2022-045-01).
Consent to Participate
The requirement for written informed consent was waived because of the retrospective design of the study.
Author Contributions
HL and CXY contribute equally to this work. HL, CXY and GF contributed to the conception of the study. ZZY, HL and LY performed the data measurement. HL, CXY and YDY performed the model development. HL and CXY and ZH contributed significantly to analysis and manuscript preparation. HL and GF performed the data analysis and wrote the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.