
Abstract
Keywords
Introduction
In recent years, with the rapid growth of China's industrial economy, issues like environmental pollution, stress, and eating disorder are getting more and more serious, and the incidence of pancreatic tumors is surging in China, reaching a number of 5.1/100 000. At the same time, pancreatic cancer is challenging to treat and has a poor prognosis with a median survival of 6 months reported by nature journal.1–4 Pancreatic body tail cancer (PBTC) accounted for 20% of pancreatic cancers. Because of its occult location as well as the lack of specific clinical presentations and tumor markers in the early stage, 70% of the PBTC patients were in the middle and late stages when diagnosed. In addition, the complete surgical resection rate was less than 40% due to commonly coeliac trunk and superior mesenteric artery involvement or liver-intestinal metastasis.5–7 Although a small portion of PBTC patients gained the opportunity of surgical resection, they often suffered from uncontrollable recurrence and death because of the high vascular and nerve invasion, lymph node metastasis characteristics, and poor sensitivity to current chemoradiotherapy and immunotherapy. The 5-year overall survival was less than 10%. Therefore, early preoperative diagnosis and outcome prediction of PBTC are crucial to adjust the treatment plan to prolong the survival period as much as possible.8,9 More specifically, outcome prediction of PBTC may effect its treatment, The results of this study indicate that for older PBTC patients with diabetes and peripancreatic lymph node swelling, intensive care management, dietary treatment or insulin therapy for blood glucose control, and minimally invasive clearance or proton heavy ion therapy of peripheral lymph nodes can effectively reduce the incidence of postoperative complications; PBTC with carcinoembryonic antigen (CEA) increased cases should be vigilant in getting a short-term ultrasound or MR rechecks to detect surrounding tissue or liver metastasis early and undergo the targeted treatment; for PBTC cases with more peripancreatic fluid, dilation of the pancreatic ducts and bile ducts, we recommend that patients undergo 1 to 3 days abdominal external drainage, percutaneous transhepatic cholangial drainage, and anti-inflammatory treatment before operation. In addition, for PBTC with poor prognosis prediction, longer regular targeted chemotherapy, molecular targeted drugs (erlotinib, everolimus, or sunitinib), and regular imaging rechecks should be conducted to maximize the life expectancy of patients after surgery. The development of radiomics technology, which started in 2012, has greatly promoted the evolution of imaging diagnosis. Now it has been widely used in the artificial intelligence recognition of liver cancer, kidney cancer, and lung nodules, and has achieved better clinical benefits. In the same way, our team applied computed tomography (CT) radiomics technology to the diagnosis and treatment evaluation of PBTC and obtained good benefits. The results confirmed that the radiomics score (Radscore), surgery in the specialized medical center of pancreatic disease, nerve invasion, etc, were independent factors affecting the prognosis of PBTC; the comprehensive radiomics score obtained by CT image segmentation of pancreatic mass may represent the basic texture information of the mass image and reflects its essential characteristics (including mass heterogeneity, possible fat or cancerous soft tissue replacement, dynamic enhancement mode, tissue necrosis, tissue ischemia, enhancement mode of PTBC dense tissue, local tissue sclerosis of pancreas, etc). There are few reports on clinical data combined with radiomics to predict the prognosis of PBTC after consulting the references in PUBMED, Therefore, this study has some novelty that may be helpful to the prognosis management of PTBC. This study aimed to establish a model to predict the prognosis of PBTC based on clinicopathological-CT imaging features, and achieved good results, providing a reference for patients’ prognosis prediction and targeted treatment.
Materials and Methods
The clinical and imaging data of 203 patients who underwent surgical resection or endoscopic ultrasound biopsy and were pathologically diagnosed with PBTC between December 2012 and December 2022 in the Pancreatic Surgery Department of Xiangyang NO.1 People's Hospital were retrospectively collected. All PBTC patients had complete preoperational abdominal enhancement and chest CT examinations. The data included age, gender, diabetes condition, hypertension condition, CEA, carbohydrate antigen 19-9 (CA19-9), tumor location, tumor size, tumor, node, and metastasis (TNM) stage, CT enhancement mode, and CT texture parameters. Inclusion criteria: patients accepted surgical treatment with complete clinicopathological, imaging, and follow-up data. Exclusion criteria: patients accepted conservative treatment, or with pancreatic metastases from other primary malignancies; combined with other tumors; and combined with multiorgan dysfunction syndrome (Figure 1).4,9 Finally, a total of 143 PBTC patients were included, and they all signed the informed consent. And then PBTC was divided into a good prognosis group (survival time ≥ 6 months) and a poor prognosis group (survival time < 6 months) according to a median survival of 6 months reported by nature journal. 4

The simplified inclusion and exclusion criteria for patient enrollment in the present study.
This is an exploratory, single-center, and retrospective study. This study was approved by the local Institutional Review Board (Ethics number: No. 1126 [2020]), and conducted in accordance with the Declaration of Helsinki. This study obtained informed consent from participants. The reporting of this study conforms to STROBE guidelines. 10 We have de-identified patient details such that the identity of any person may not be ascertained in any way. This study has followed relevant Equator guidelines 11 and started in March 2021 and ended in December 2022.
CT Scanning
① The 64-slice CT scanner (Definition AS, Siemens Healthineers, Germany) and the 320-slice CT scanner (Aquilion ONE, Toshiba Medical Systems Corporation, Japan) were used. CT scanning parameters were set as tube voltage 120 kV, tube current 150 mAs, collimator width 160 mm × 0.5 mm, and matrix size 350 × 350. Enhanced scanning was performed while injecting 90 to 95 mL contrast agent iopromide (335 mgI/mL) using a high-pressure syringe, at a flow rate of 5.5 mL/s. Scans were conducted 20 to 30, 60 to 80, and 100 to 130 s after the injection to obtain the arterial phase, portal venous phase, and delayed phase images, respectively. The slice thickness and interval of the scanned and reconstructed images were 0.8/1.0 and 1.0/1.0 mm, respectively. ② Scan extended from the diaphragm to the lower border of the kidney, and the images were independently reviewed by 2 to 3 senior specialists who had over 15 years of experience in pancreas-related disease diagnosis. The indicators included lesion location, size, and CT enhancement mode, dilation of the main pancreatic duct (upstream main pancreatic duct diameter > 5 mm), acute obstructive pancreatitis, vascular invasion, nerve invasion, etc. ③ CT enhancement mode is mainly divided into homogeneous enhancement and slight fast enhancement. The former may represent poor blood supply and slow growth of the tumor, while the latter may represent that the tumor has a branch blood supply (partially confirmed by CTA), grows faster, and infiltrates more of the surrounding tissues. ④ Diagnostic criteria for extrapancreatic nerve plexus invasion of pancreatic cancer: the peripancreatic fat space narrows or the peripancreatic vascular space disappears (including the superior mesenteric artery, superior mesenteric vein, celiac artery trunk, and splenic vein), with banded and reticular soft tissue density shadows in it; Peripancreatic fat space disappeared, and irregular soft tissue mass was seen in the area of the extrapancreatic nerve. ⑤ Diagnostic criteria for peripancreatic vascular invasion: the normal fat space between the tumor and the blood vessel disappears, and there is a pressure mark on the blood vessel; Vascular flattening or slight irregular change on one side of the vessel; the blood vessel is totally embedded in the tumor, or the tumor surrounds the blood vessel at least 2/3 of the circumference. The vascular lumen is central or eccentric stenosis.
CT Image Segmentation, Texture Feature Extraction, and Selection
All CT data were imported into a 3D slicer software (version 5.2.2, https://download.slicer.org/) and read under abdominal window (width 400/40 HU) settings. The whole PBTC lesion was selected for carcinoma volume segmentation after data acquisition. A radiographer and radiologist without knowledge of the pathology results manually delineated the volumes of interest (VOI) layer by layer, respectively. The PBTC’s VOI must enclose the entire mass as much as possible, including the fat, cyst, vasculum, necrosis, etc within the mass, and exclude the normal pancreatic tissue. Inter- and intraclass correlation coefficients (ICCs) were used to calculate the inter- and intraobserver reproducibility, and reliability of texture feature extraction. In this study, ICC is required to be greater than 0.7.
Informatics-radiomics module in 3D slicer was used to extract a total of 897 × 3 radiomics features, including histogram, gray level co-occurrence matrix (GLCM), gray level run length matrix (GLRLM), gray level size zone matrix (GLSZM), neighboring gray-tone difference matrix (NGTDM), gray level dependence matrix (GLDM), etc. Lasso regression with 10-fold cross-validation was performed to extract effective texture data, and then a radiomics label was constructed, and the radiomics score (Radscore) of each CT enhanced phase was calculated accordingly after feature screening. Radscore1 was for arterial phase, Radscore2 was for venous phase, and Radscore3 was for delayed phase (Figure 2).12–14
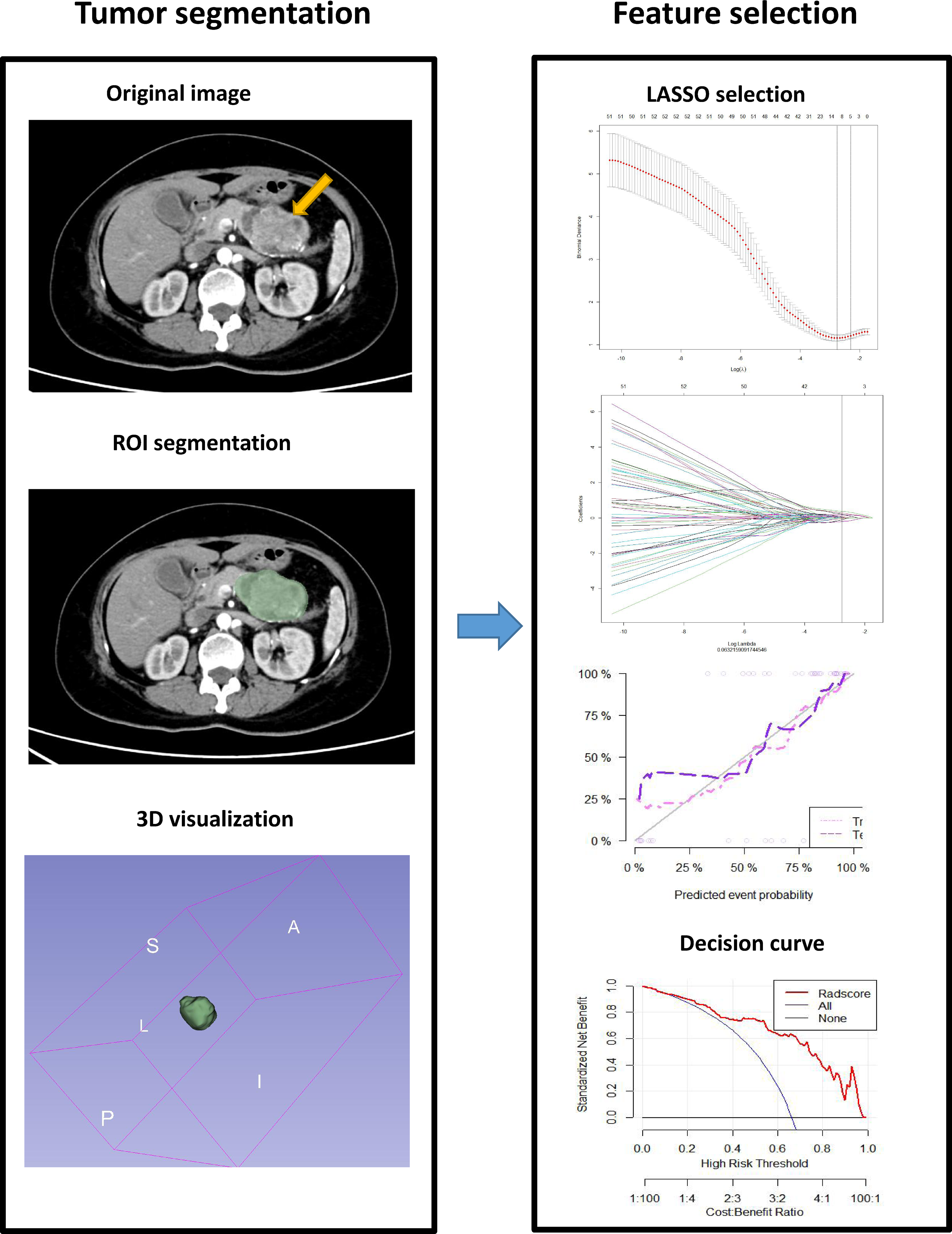
Sketch map of texture parameter extraction of pancreatic tumor CT image using 3D slicer.
Treatment Method
According to the patient's preferences, medical insurance, economic conditions and tolerance, Da Vinci surgical robot surgical treatment, laparoscopic surgery, and conservative symptomatic treatment, chemotherapy combined with immunotherapy, surgery treatment in a general tertiary hospital or treatment in a top tertiary hospital in big cities such as Beijing and Shanghai were provided. Chemotherapy may choose gemcitabine (day 1 & 7, 1000 mg/m2) combined with Tegafur (day 1-20, 40-60 mg/time, 2 times/day), gemcitabine alone for 3 weeks (day 1, 7, and 14, 1000 mg/m2), or nab-paclitaxel for 3 weeks (day 1 & 7, 100-125 mg/m2). Subcutaneous injection of thymosin (1.6-2.0 mg/time, 2 times/week) was administered during chemotherapy to boost the patient's immune function and reduce chemotherapy adverse effects. A total of 6 to 8 courses of treatment were performed, and the treatment was terminated if PBTC patients cannot tolerate chemo, or the disease progressed rapidly. Surgery may be open radical anterograde modular pancreatosplenectomy or extended radical resection of pancreatic tail cancer. The modes were conventional laparotomy, laparoscopy, or Da Vinci surgical system, and intensive care in the intensive care unit (ICU) was provided after surgery. Radiofrequency ablation usually combines chemotherapy or immunotherapy in intolerant radical surgery cases, or radiofrequency ablation combines minimally invasive surgery; these cases were all classified as conservative treatment and were excluded in this study.13,15
Follow-up
Symptomatic supportive care or palliative hospice care was provided to some end-stage PBTC patients after surgery, and the date of death was recorded. For the other patients with PBTC, telephone or outpatient follow-up was conducted till December 2022. Starting point of the survival term was the day of surgery and the ending point was the date of death or the end of follow-up in the surgery group. 14
Statistical Processing
Data analysis was performed using R (version 4.3) and Jamovi (version 2.23). The Kolmogorov-Smirnov test was used to test whether the measurement data conformed to the normal distribution. If the data conformed to the normal distribution, it was expressed as X ± S, and the independent samples t-test was used. Otherwise, it was expressed as M (range), and the Mann-Whitney U-test was used. Enumeration data were expressed in the form of frequency, and the X2 test or Fisher's exact test was adopted. Moreover, the least absolute shrinkage and selection operator (Lasso) was used to select the optimal texture features with 10-fold cross-validation to adjust the elastic network parameters to select the best combination of feature parameters (Radscore) to avoid overfitting according to many previous studies. Survival curves were generated by the Kaplan-Meier method, and the survival rates were compared with the log-rank test. According to the median survival of 6 months, the PBTC patients were divided into 2 groups, the group with good prognosis (survival time ≥ 6 months) and the group with poor prognosis (survival time < 6 months). Then a training set and a test set were established at a 7/3 ratio, and statistically significant variables were included in multivariate logistic regression analysis for modeling and validation. Decision curve analysis (DCA) was conducted to evaluate the clinical application value of the model. P < .05 was considered statistically significant.12,16,17
Result
Patients’ General Condition and Treatment
45 cases underwent conservative treatment were excluded from this study: 19 cases underwent radiofrequency ablation with chemotherapy, 7 cases underwent High-intensity Focused Ultrasound (HIFU) combined with chemotherapy/immunotherapy, 11 cases underwent 125I radioactive particle minimally invasive interventional surgery, 8 cases only underwent chemotherapy/immunotherapy. A total of 143 cases that underwent surgical treatment were included in this study: 79 were males and 64 were females; the age ranged from 28 to 83 years, with a median age of 62.62, and 83 patients had diabetes. The overall average survival was 7.4 months in this study. Among the 143 surgery patients, 121 cases underwent radical resection, and 22 cases (12 cases of stage III and 10 cases of stage IV) underwent extended radical resection. There were 16 cases combined with resection and reconstruction of the colonic splenic flexure, left adrenal gland, and celiac trunk, as well as resection of liver metastases, 8 cases with resection of the stomach, left kidney, and adrenal gland, and 5 cases combined with partial resection of horizontal duodenum and/or transverse colon. Pancreatic leakage occurred in 24 cases, and no other serious complications occurred postoperationally.
Kaplan-Meier Analysis of Factors Affecting PBTC Recurrence
The univariate analysis demonstrated that Age, diabetes, TNM stage, CT enhancement mode, nerve invasion, peripancreatic lymph node swelling, advanced hospital surgery, tumor size, CA19-9, CEA, Radscore1/2/3 were the influencing factors of PBTC recurrence (P < .05), while gender, lesion morphology, dilatation of main pancreatic duct, acute obstructive pancreatitis, pancreatic atrophy, vascular invasion, BMI were not significantly correlated with the recurrence of PBTC (Table 1 and Figure 3).
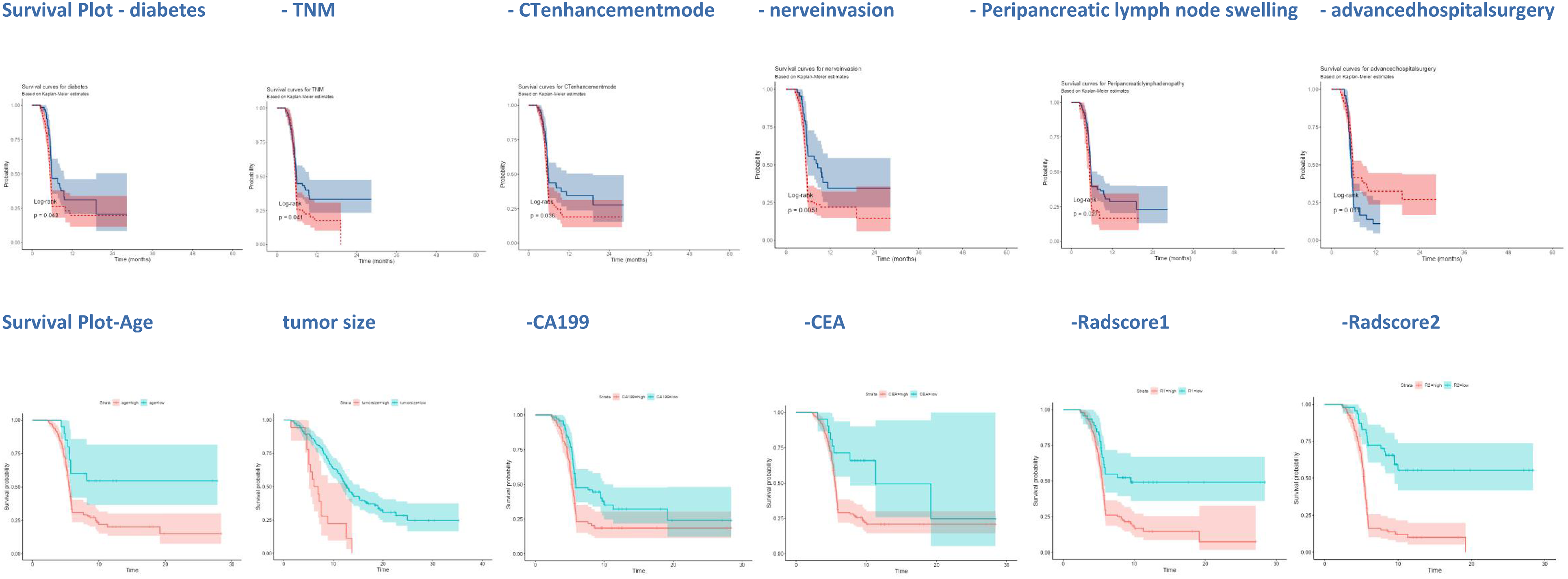
Kaplan-Meier analysis diagram (Log-rank method) of pancreatic body tail cancer (PBTC) recurrence based on the above risk factors.
Kaplan-Meier Analysis of Factors Affecting PBTC Recurrence.

Abbreviations: PBTC, pancreatic body tail cancer; TNM, tumor, node, and metastasis; CA19-9, carbohydrate antigen 19-9; CEA, carcinoembryonic antigen; CT, computed tomography; BMI, body mass index.
Establishment of 3 Predictive Models by Logistic Regression and Model Validation
According to the median survival of 6 months, the PBTC patients were divided into 2 groups, a group of good prognoses and a group of poor prognoses, followed by the establishment of a training set and a test set at a ratio of 7/3. Multivariate logistic analysis confirmed that nerve invasion, advanced hospital surgery, dilation of the main pancreatic duct, Radscore2 were independent factors affecting the death/survivals of PBTC patients (P < .05). In the training set, the combined model achieved the best predictive performance [AUC 0.976, 95% CI (0.924-0.996)], significantly higher than that of the clinicopathological model [AUC 0.821, 95% CI (0.732-0.890), P = .0001] and that of the CT radiomics model [AUC 0.943, 95% CI (0.879-0.980), P = .0623]. Also, in the test set, the combined model achieved the best predictive performance [AUC 0.944, 95% CI (0.826-0.991)], significantly superior to the clinicopathological model [AUC 0.770, 95% CI (0.615-0.886), P = .0145], and the CT radiomics model [AUC 0.883, 95% CI (0.746-0.961), P = .1311]. DCA confirmed that the clinical net benefits of the combined model were better. The nomogram simplified the process of predicting the prognosis of PBTC in clinical practice (Tables 2 to 4 and Figures 4 to 6).

DeLong nonparametric method was used to estimate the area under the curve of ROC between different prediction models of the training set (a) and test set (b) and compare its effectiveness in predicting the PBTC prognoses. The area under the curve of the combined model was the largest.
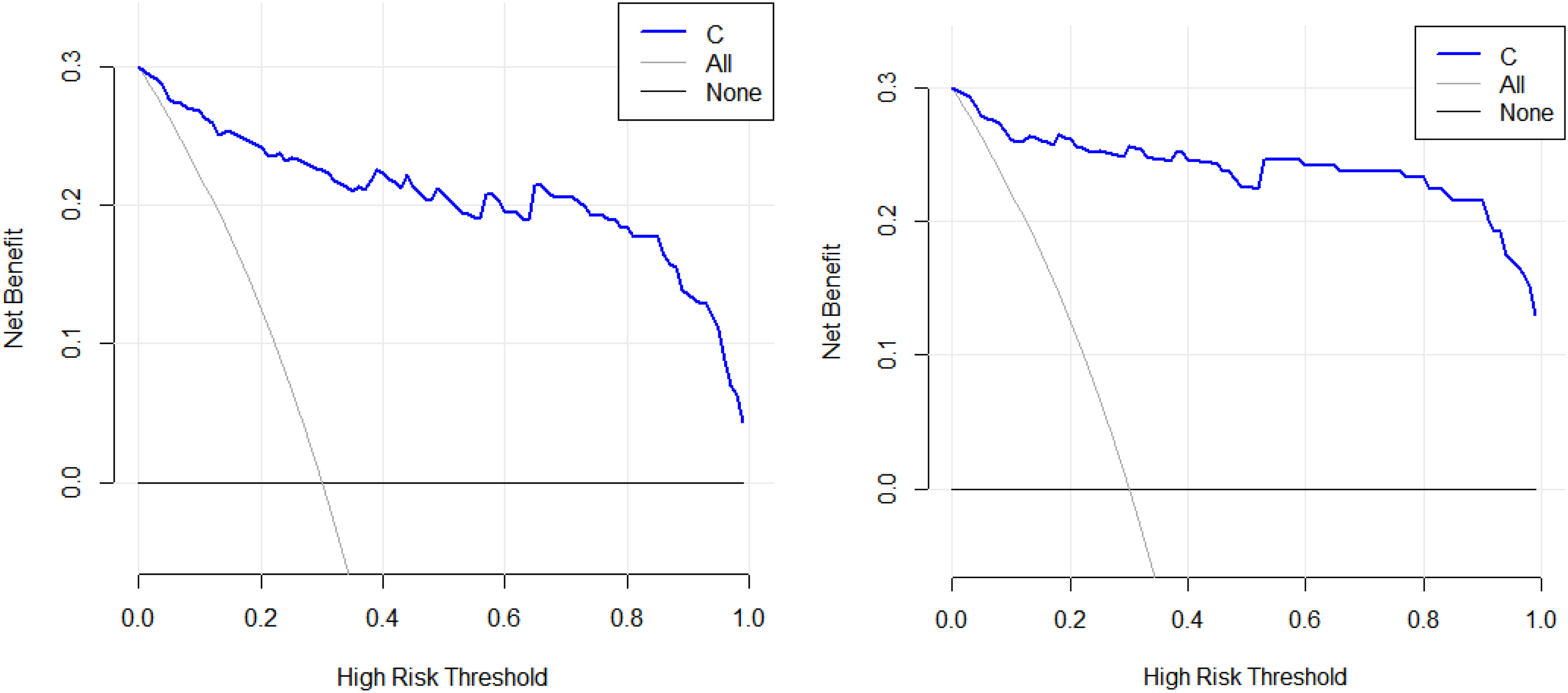
In the training set (a) and the test set (b), the better clinical net benefit of the combined model (C) was analyzed and confirmed using a decision curve.

Based on the combined model, we created a new nomogram (A) and calibration curve (B), which simplified the process of predicting the prognosis of pancreatic body tail cancer (PBTC) in clinical practice (R2: Radscore 2).
Logistic Regression Analysis Results of Clinicopathological Model Based on Clinical/Pathological Characteristics for Predicting PBTC Prognoses.

Abbreviations: PBTC, pancreatic body tail cancer; TNM, tumor, node, and metastasis; CA19-9, carbohydrate antigen 19-9; CEA, carcinoembryonic antigen; BMI, body mass index.
*P < .05.
Logistic Regression Analysis Results of CT Radiomics Model Based on CT Texture Analysis for Predicting PBTC Prognoses.

Abbreviations: PBTC, pancreatic body tail cancer; CT, computed tomography.
*P < .05.
Logistic Regression Analysis Results of Combined Model Based on Above Risk Factor for Predicting PBTC Prognoses.

Abbreviations: PBTC, pancreatic body tail cancer; CT, computed tomography; TNM, tumor, node, and metastasis; CA19-9, carbohydrate antigen 19-9; CEA, carcinoembryonic antigen.
*P < .05.
Discussion
The incidence rate of pancreatic cancer in China is as high as 5.1/100 000 due to the acceleration of China's industrialization process, food pollution, high living pressure, and other factors, but the median survival period is only 4 to 6 months. With the development and wide application of imaging technology, the detection rate of pancreatic tumors keeps rising, about 5% to 10% of patients with jaundice and emaciation were finally confirmed pancreatic cancer. PBTC is a common type of pancreatic tumor with variable nature, insidious onset, and prone to be missed diagnosed or misdiagnosed.18,19 The early diagnosis of PBTC is very challenging, and the mortality rate keeps high, which is related to its unrepresentative imaging features, rapid progression, and high metastasis rate. Also, in the clinical diagnosis and treatment practice, most PBTC patients are diagnosed in the middle or late stages; Usually, the tumors may have already infiltrated the surrounding organs, blood vessels, nerve plexus, and peripancreatic adipose tissue. Currently, surgical resection and chemotherapy combined with immunotherapy remains the only means of curing PBTC or improving survival. Although it improves the quality/rate of life of patients to a certain extent, ultimately peripheral recurrence and metastasis are common. Therefore, the prognosis prediction of PBTC is extremely important for its postoperative treatment management. It is reported that accurate pancreatic tumor information (size, location, surrounding tissue invasion, lymph node metastasis, etc) and pathological staging play a decisive role in the postoperative survival time of PBTC patients. Moreover, the new emerging radiomics technology has a good predictive effect on the prognosis of many other tumors, which is also applicable to the PBTC. Therefore, accurate preoperative CT/MR imaging details, diagnosis, and texture parameters are of great value for the prognosis of PBTC. This important information can promote the change of clinical decision-making of PBTC patients, determine the operation mode, radiotherapy and chemotherapy options, and even timely transfer to the clinical palliative care wards, which is extremely important for the high-quality late survival of patients.20,21
Generally, the prognosis of PBTC also depends on the biological properties of the tumor itself. It has been reported that the prognosis of PBTC was related to TNM stage, degree of differentiation, histological type, surgical method, number of regional lymph node dissections, and radiotherapy and chemotherapy.7,22,23 To reduce bias, the PBTC cases included in this study were all ductal adenocarcinomas. In addition to the above-influencing factors, we also revealed that age, diabetes, CT enhancement mode, nerve invasion, advanced hospital surgery, tumor size, CEA, CA199, dilation of the main pancreatic duct, peripancreatic fluid, radscore1/2/3 were important factors affecting the fast progression-free survival rate of PBTC. It is well known that the immunity and physical function of elderly patients are significantly lower than those of young adults, so postoperative recovery is poor with many complications; In this study, the survival time of the younger patients was significantly higher than that of the older patients, which also confirmed this view. The high blood glucose concentration and poor immune function in patients with diabetes may be related to the recurrence of PBTC, whose wound healing is slow, and complications are even more, which worsens survival. The rapid enhancement of the tumor may be related to its multibranch blood supply and microvascular invasion, which may lead to recurrence and death. In this study, 69.93% of PBTC was accompanied by peripheral nerve invasion. To delay the recurrence, general radiotherapy and chemotherapy were required after the operation, which would further damage the body function and cause obvious pain/hematochezia in patients, resulting in a poor prognosis. Surgery in top hospitals was newly discovered recurrence and poor prognosis-related factors in this study. We found that the mortality risk of da Vinci surgical robot/advanced hospital surgery combined with chemotherapy and immunotherapy for PBTC was 0.45 times that of classical surgery and symptomatic treatment and 0.22 times that of interventional therapy with chemotherapy. Of course, surgery is still the first-line treatment for a good prognosis of PBTC in this study. Besides, 67.83% of PBTC patients with good economic conditions went to the top hospitals in big cities like Beijing and Shanghai and received the da Vinci operation, heavy-ion cancer therapy, and specialized/customized ICU care and achieved significantly improved survival rate. Although the unequal treatment caused by patients’ selection bias leads to a longer survival time, which will have a certain bias on the study, this factor will not cause a large bias on the study results, because its independent AUC is only 0.601. The size of the lesion determined the difficulty of the operation and varies the possibility of unavoidable pancreatic leakage, postoperative hemorrhage, and retroperitoneal infection, while the recurrence of PBTC in patients with larger tumors is still concerning. There 16.78% of PBTC patients with significantly elevated CEA levels had liver and intestines metastases, therefore, the recurrence and death rates were high after surgical resection. The degree of expansion of the main pancreatic duct reflects the tumor's space-occupying effect or invasion and compression of the pancreatic duct and surrounding tissues of the pancreas. Peripancreatic effusion reflects the degree of tumor necrosis and degeneration or peripheral carcinomatous lymphangitis to a certain extent, thus increasing the difficulty of surgery, leading to adverse events such as pancreatic leakage and continuous bleeding, It may be doomed to a bad prognosis. In this study, Radscore demonstrated excellent predictive performance, which may be related to the underlying imaging texture parameters of the masses it extracted. In previous studies, Radiomic features (such as intensity, shape, texture, or wavelet) were speculated may provide reliable data support and be correlated with global sensitivity, heterogenicity, possible fat or carcinoma soft tissue replacement of typical imaging features to some extent in the future. More importantly, Radscore may refine and classify the overall density, signal of the tumor based on some special algorithms, which may be similar to the distribution of CT value, and is helpful to distinguish the nature of the lesion, such as the percentage of fat, fiber, calcification, blood vessel, etc17,24,25; which has currently been applied in domestic pulmonary nodule AI recognition software and has received good clinical evaluation.25,26Our team found that Radscore 1 may represent the enhancement mode of PTBC dense tissue, similar to the local tissue hardening and enhancement of pancreas after detailed analysis of texture parameters, while it also highlights the possibility of local tissue necrosis and fluid exudation, which is difficult to identify by naked eye; However, Radscore 2 seems to represent the possibility of microvascular thrombosis in the mass and indicate the degree of enhancement in the venous phase, which is different from normal pancreas or inflammatory lesions. Radscore1/2/3 represented the preoperative CT image texture parameters, which can tell the nature of the tumor, and thus is valuable for recurrence prediction.17,23,27 And based on the combined model, a new nomogram was created. We also found that when R2 (radscore2) ≥ 6, the tumor's boundaries become blurred, the enhancement pattern changes, tissue density increases, ischemic necrosis increases, and so on. Moreover, as the R2 value increases and approaches 10, the possibility of low differentiation increases and the prognosis deteriorates.28–30 As a universal marker of gastrointestinal tumors, CA19-9 is higher sensitive. Although it is a bad prognostic factor in this study, its AUC (0.610) and specificity (0.141) are not strong, so it has little clinical significance.
At last, we established a combined model, a clinicopathological model, and a CT radiomics model, and validated that the combined model provided the best predictive performance. Subsequently, similar results were obtained in the test set and DCA confirmed its superior clinical net benefit. The combined model has higher prediction efficiency than the previously reported nomogram clinical models (AUC: 0.976 vs 0.777). 27 This may be related to the combination of clinical, pathological, and CT imaging parameters and the acquisition of information about the nature of the tumor. The combined model is helpful for the treatment and management of PBTC and improves the life quality of patients, receiving clinical recognition.
Limitation
The LASSO regression is a powerful regularization technique, which has some limitations, such as sensitivity to outliers, which is particularly important given the small sample size of this study. Additionally, it has limited interpretability, making it difficult to understand which specific imaging features are more important. Moreover, the potential impact of patient selection may bias on the results, different patients may receive unequal treatment due to factors such as patient preferences, medical insurance, and treatment tolerance. Since this was a single-center study with a small sample size, we didn’t calculate sample size using random sampling, whole group sampling, or other statistical methods, it cannot present all population differences among PBTC patients. This study was based on the Kaplan-Meier method and logistic regression, and biased may present in data processing, and a high P < .05 requirement may cause missed potentially valuable data. In the future, multicenter big data research would be conducted, and deep learning and artificial intelligence methods may be used to improve the prediction performance of the model.31,32
Conclusions
In conclusion, the total survival period of PBTC patients is poor, and it is much challenging to improve this situation; The combined model has a high predictive efficiency for the prognosis of PBTC (AUC: 0.976), higher than previously reported clinical model (AUC: 0.777); because it is mainly generated based on clinical data and CT radiomics, it does not increase the medical cost and patient burden, and may produce more detailed clinical treatment and CT image fusion information, which may provide support for clinical decision-making and clinical management of PBTC, and help to prolong the survival time of PBTC as much as possible.
Footnotes
Acknowledgments
2021 Science and Technology Innovation Project of Xiangyang No.1 People's Hospital: Research on Risk Stratification Decision and Key Problems of Prostate Cancer Based on In-Depth Learning of MRI/Ultrasound Radiomics (XYY2021Q16, PENG AN); Graduate Education Research Project Fund of Hubei University of Medicine (YJ2022013) (YingJian Ye), Xiangyang Science and Technology Plan Key Project Fund (2022YL34A) (YingJian Ye).
Authors’ Contributions
Peng An, Yan Hu, and Xiumei Li conceived and drafted the manuscript. Peng An, Junyan Zhang, and Ping Qin contributed to the literature review, and Yingjian Ye and Guoyan Feng are responsible for the quality control of article statistics. Guoyan Feng, Yong Lin, and Jingsong Wang revised the manuscript critically for important intellectual content. Jingsong Wang and Guoyan Feng approved the final version to be published and agreed to act as guarantors of the work. Peng An, Yong Lin, and Junyan Zhang contributed equally to this work.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Consent for Publication
We all agree.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
The experimental protocol was established, according to the ethical guidelines of the Helsinki Declaration, and was approved by the Human Ethics Committee of Xiangyang NO.1 People's Hospital affiliated with Hubei University of Medicine (Issue No. 1126 [2020]). Written informed consent was obtained from individual or guardian participants.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 021 Science and Technology Innovation Project of Xiangyang No. 1 People’s Hospital: Research on Risk Stratification Decision and Key Problems of Prostate Cancer Based on In-Depth Learning of MRI/Ultrasound Radiomics, Graduate Education Research Project Fund of Hubei University of Medicine, Xiangyang Science and Technology Plan Key Project Fund (grant numbers XYY2021Q16, YJ2022013, and 2022YL34A).