
Abstract
Keywords
Introduction
Tongue squamous cell carcinoma (TSCC) is one of the most common oral malignant tumors, accounting for 1/3 to 1/2 of cases. Due to factors such as unclean diet, food/environmental pollution, etc., China has over 300 000 new cases of TSCC each year. Tongue squamous cell carcinoma often greatly affects patients’ chewing, swallowing, language, breathing, and even threatens their lives due to the tongue's unique physiological and anatomical structure. Tongue squamous cell carcinoma has strong invasiveness, poor wound healing, and other clinical characteristics, making postoperative management and psychological counseling difficult and resulting in a high mortality rate.1–3 Although the treatment plan for TSCC is constantly updated and survival rates have improved in recent years, TSCC has a high degree of malignancy and is prone to recurrence and metastasis, and the 5-year survival rate is still relatively low, at only about 40% in China. Therefore, finding sensitive prognostic indicators and intervening early is of great clinical significance for improving TSCC survival rates. In China, TSCC usually occurs in people over 50 years old. Due to a lack of relevant medical knowledge or insufficient interpretation of TSCC popular science guidelines, many patients and even doctors mistakenly believe that TSCC has a good prognosis after radical resection surgery, similar to thyroid cancer. As a result, they do not restrict their diet or undergo regular follow-up examinations, making it difficult to comprehensively monitor and follow up TSCC in clinical practice. Therefore, selecting the target population for TSCC postoperative screening is extremely important for further treatment and management of TSCC.4–6 Neutrophil/lymphocyte ratio (NLR) and platelet/lymphocyte ratio (PLR) have been reported as classic indicators for evaluating the body's inflammatory and tumor immune responses. They are independent risk factors for the prognosis of salivary gland cancer, gastric cancer, and other cancers, and we found that they also affect TSCC prognosis.7,8 MRI has high tissue resolution and multi-plane imaging functions, making it an ideal method for monitoring TSCC. diffusion weighted imaging (DWI) imaging can distinguish the benign and malignant nature and differentiation degree of tumors, and enhanced MRI can show the degree of blood perfusion of tumor tissue capillaries, which is of great value for understanding the biological behavior and prognosis of tumors. Therefore, the MRI-Radscore extracted based on LASSO has important clinical value in this study.9–11 In addition, we found that new factors such as unclean oral sex, drug use, spicy hot pot, and consumption of pickled foods have important value in this study. We reviewed literature on TSCC published in the past 30 years on PubMed and found that existing research usually focuses on TSCC surgical methods and molecular pathological basis, with little discussion on clinical–MRI combined models for predicting TSCC prognosis (Figure 1).12,13 Therefore, by integrating MR radiomics features and clinical data, we established a combined model that achieved good predictive benefits, providing some new clues for predicting TSCC prognosis.
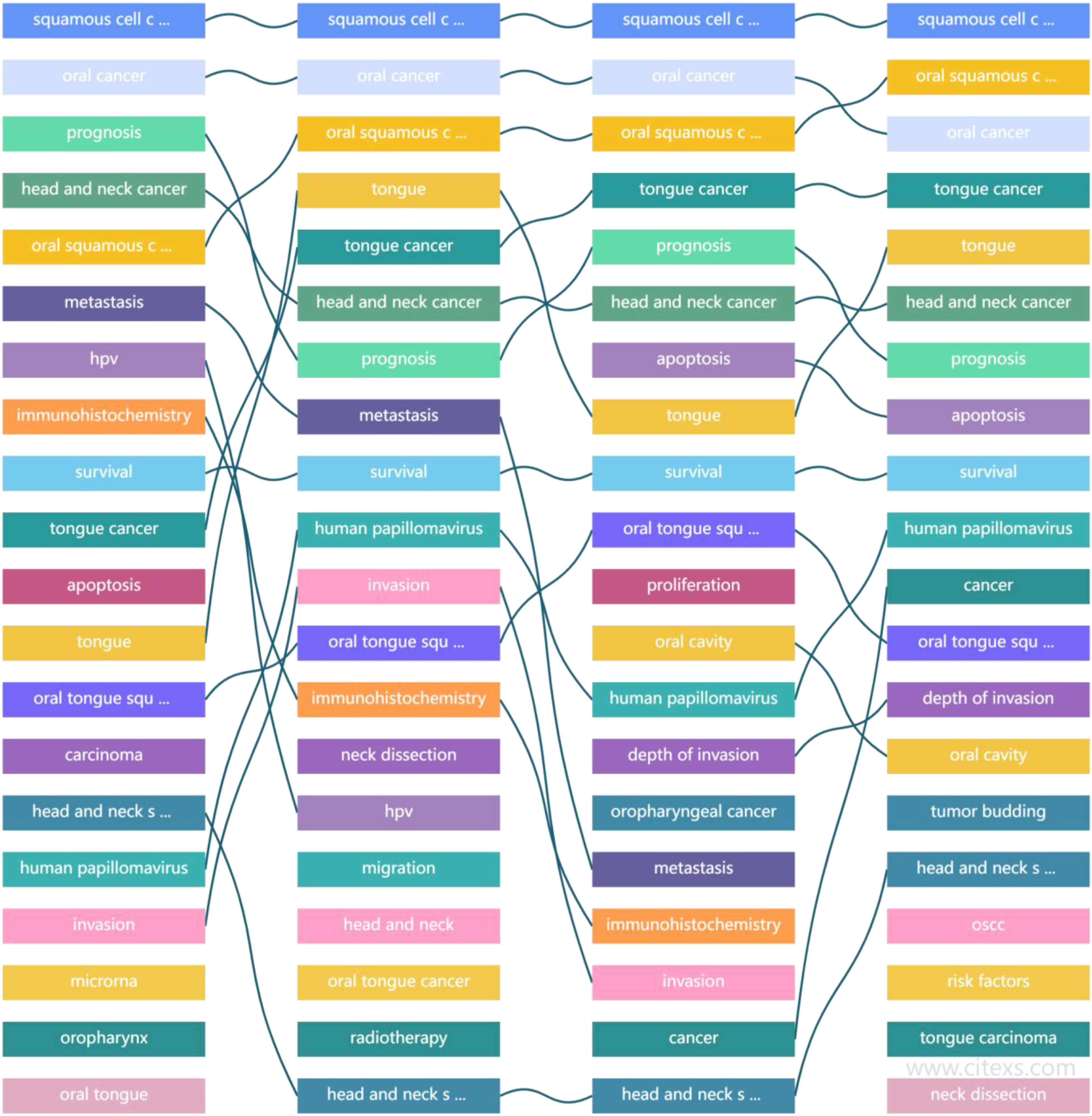
The results of quantitative literature analysis based on tongue squamous cell carcinoma (TSCC) search indicate that surgical treatment and molecular pathology has always been a hot topic in TSCC research, but clinical imaging radiomics prediction models have not been reported before.
Research Methods
Data Collection
We retrospectively analyzed the clinical and imaging data of 236 patients who underwent radical surgery and were pathologically diagnosed with TSCC from February 2011 to January 2020 at XX Hospital. There were 131 male cases and 105 female cases, with an age range of 41 to 70 years and a mean age of 56.31 ± 9.36 years and a median age of 53 years. Inclusion criteria: (1) all underwent radical surgical resection; (2) postoperative pathology was TSCC; (3) only single lesions visible on MRI and computed tomography (CT) without distant metastasis were studied to reduce bias; (4) primary TSCC without other tumor history; and (5) patients had complete clinical and radiological data, good compliance, and long-term follow-up. Exclusion criteria: (1) cases lost to follow-up or died from non-TSCC-related causes; (2) cases with severe complications during the perioperative period leading to death; (3) cases with other types of tumors; (4) patients with claustrophobia, contraindications for enhanced MRI, including circulatory system failure, liver and kidney dysfunction, or contrast agent allergy; and (5) patients with cognitive dysfunction (Figure 2). Clinical data included tumor diameter, tumor volume, age, gender, BMI, PLR, NLR, oral sex, clinical stage, primary site, depth of invasion (DOI), betel nut, spicy hot pot or pickled food, drug use, poorly differentiated, etc.5,6,14

The inclusion and exclusion criteria and case grouping method of this study.
This is an exploratory, single-center, and retrospective study. This study was approved by the Xiangyang No. 1 People's Hospital Institutional Review (Issue No. 3012 [2012]) conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from individual or guardian participants. The reporting of this study conforms to STROBE guidelines. 15 We have de-identified patient details such that the identity of any person may not be ascertained in any way.
Equipment Parameters
MRI: Philips Achieva 1.5 T Nova Dual MRI and GE discovery MR750 W 3.0 T MRI were used, equipped with appropriate head and neck coil arrays. Patients were placed in a supine position. Routine scanning sequences included axial and coronal T2WI sequences (fast spin echo sequence) of the oral pharynx; scanning parameters: TR 4890 ms, TE 70 ms, FOV 210 × 246 mm, matrix 384 × 384, slice thickness 3/5 mm, slice spacing 1.0 mm. Axial DWI scanning, b values of 0 and 1000 s/mm2, slice thickness 3 mm, slice spacing 1 mm, TR 7500 ms, TE 80 ms, FOV 300 × 356 mm, matrix 256 × 256, and apparent diffusion confficient (ADC) images were obtained on the workstation. T1WI-enhanced scanning, TR 220 ms, TE 2.46 ms, slice thickness 3.0 mm, slice spacing 0.6 mm, field of view 230mm × 230 mm, and matrix 320 × 240, using a Bayer high-pressure injector through the elbow central vein at an injection rate of 2 ml/s and a dose of 0.2 mmol/kg of contrast agent gadolinium-DTPA (Gd-DTPA), followed by intravenous injection of 20 ml of saline at the same flow rate. T2WI, DWI, ADC, and T1WI-enhanced images were exported as DICOM files and imported into 3D Slicer 4.13 software for volume of interest (VOI) delineation and feature extraction. Volume of interest delineation was performed manually by 2 experienced radiologists who were blinded to the pathological results. Volume of interest was delineated in the maximum axial section of the entire mass, away from surrounding tissues such as blood vessels and dental crowns. Texture parameters, including shape, first order, glcm, glrlm, glszm, ngtdm, and gldm parameters, were obtained using the Slicer radiomics module. The consistency between 2 repeated VOIs was evaluated by intra-class correlation coefficient (ICC) (ICC ≥ 0.7 indicates good consistency, and ICC ≥ 0.75 was required in this study). For each MR sequence, 879 features were obtained. These features were introduced into R software or Python to screen valuable texture parameters using LASSO and generate Radscore9,11,16 (Figure 3).

The simple schematic diagram of tongue squamous cell carcinoma (TSCC) MR lesion delineation and radiomics extraction in this study.
Therapeutic Method and Follow-Up Data
All TSCC patients underwent radical surgery, and cervical lymph node dissection or local radiotherapy was performed on patients with confirmed cervical lymph node metastasis through biopsy. The follow-up period is from the day of surgery to the patient's death or the end of the follow-up period, which is until April 30, 2023. Five patients were lost to follow-up, but there were no early losses. All patients were followed up after surgery through outpatient, inpatient, and regular telephone methods. The endpoint of follow-up was tumor recurrence or metastasis, which is the time from surgery to tumor recurrence or metastasis. Patients who did not experience recurrence or metastasis were followed up until their last follow-up. The observation time was measured in months, and comprehensive specialty examinations and imaging reviews (such as CT and MR) were conducted. If new lesions were found in the primary site or distant organs, it was diagnosed as a recurrence.17,18
Statistical Analysis
Jamovi 3.23 software was applied for statistical analysis. A training set and a test set were established based on a ratio of 7:3 and a time point. All continuous variables were calculated via homogeneity of variance and normal distribution. The measurement data in both groups (correspond to normal distribution) was expressed as X ± S, and compared via the t-test. The measurement data (nonnormal distribution) was expressed as range (A1–A2) and compared via the rank sum test. The categorical variables were expressed as percentage of case (%) and compared via the chi-square test. In addition, the optimal texture features were selected using LASSO algorithm with 10-fold cross-validation to adjust the elastic network parameters and select the best combination of feature parameters (Radscore) to avoid overfitting according to many previous studies. The differences of clinical data, general imaging features, and radiomics characteristics between groups were analyzed via logistic regression. Then, 3 prediction models (clinical data model, imaging model, and combined model) were established, and the different area under curves (AUCs) were calculated to test and verify the diagnostic performance of 3 models above. Then decision curve analysis (DCA) was conducted to evaluate the clinical net benefit of the valuable model. Finally, the nomogram was established and subjected to corresponding clinical testing and application. P < .05 was confirmed statistically significant.8,10,19
Result
We extracted 4 sets of Radscores based on T2WI, T1WI-enhanced images, DWI, and ADC, namely, T2WI (Radscore1), T1WI enhanced images (Radscore2), DWI (Radscore3), and ADC (Radscore4). ADC image VOI delineation was difficult, ICC < 0.60 was discarded, and DWI Radscore3 was not significantly different between the 2 groups (P > .05) and was discarded.
According to the American Joint Committee on Cancer (AJCC) eighth edition tumour, node and metastases staging criteria for oral cancer in 2017, there were 46 cases in stage I, 67 cases in stage II and 98 cases in stage III (P < .05). The tumor sites were 42 cases on the tip and edge of the tongue, 76 cases on the body of the tongue, and 93 cases on the base of the tongue (P > .05). The degree of differentiation was high in 68 cases and moderate to low in 143 cases (P < .05) (Figure 4). Adjacent cervical lymph node metastasis was present in 48 cases and absent in 163 cases; after undergoing radical surgery and cervical lymph node dissection or local radiotherapy, the prognosis of TSCC was not affected (P > .05).

Male, 59 years old, with poorly differentiated tongue squamous cell carcinoma (TSCC). Pathological findings suggested that the tumor tissue was squamous differentiated and lacks of keratinizing beads (a). Female, 62 years old, with highly differentiated tongue squamous cell carcinoma. Pathology suggested squamous differentiation of the tumor tissue, with obvious keratinized beads visible (b).
Single-factor analysis confirmed that there was a statistically significant difference in the betel nut consumption, spicy hot pot or pickled food, unclean oral sex, drug use, DOI, PLR, NLR, MR enhancement pattern, low differentiation, clinical stage, and Radscore between the 2 groups (P < .05), while there was no statistically significant difference in age, hypertension, diabetes, history of smoking, history of alcohol use, tumor volume, BMI, and other clinical characteristics between the 2 groups (P > .05).
Based on the above risk factors, we have established clinical data models, imaging models, and combination models, respectively. In the training set, the combination model has the highest predictive performance (AUC: 0.907, 95% CI (0.849-0.948]), which is significantly better than the clinical data model (AUC: 0.817, 95% CI [0.745-0.875], P = .001) and imaging model (AUC: 0.865, 95% CI [0.799-0.915], P = 0.023). The same results were verified in the test set, where the combination model had higher predictive performance (AUC: 0.870, 95% CI [0.761-0.942]) than the clinical data model (AUC: 0.730, 95% CI [0.602-0.835], P = .033) and imaging model (AUC: 0.765, 95% CI [0.640-0.863], P = .074). Decision curve analysis confirmed that the clinical net benefits of the combination models in both groups were higher. Subsequently, the nomogram based on the combination model also obtained clinical application and better clinical application value (Tables 1 to 3 and Figures 5 to 7).
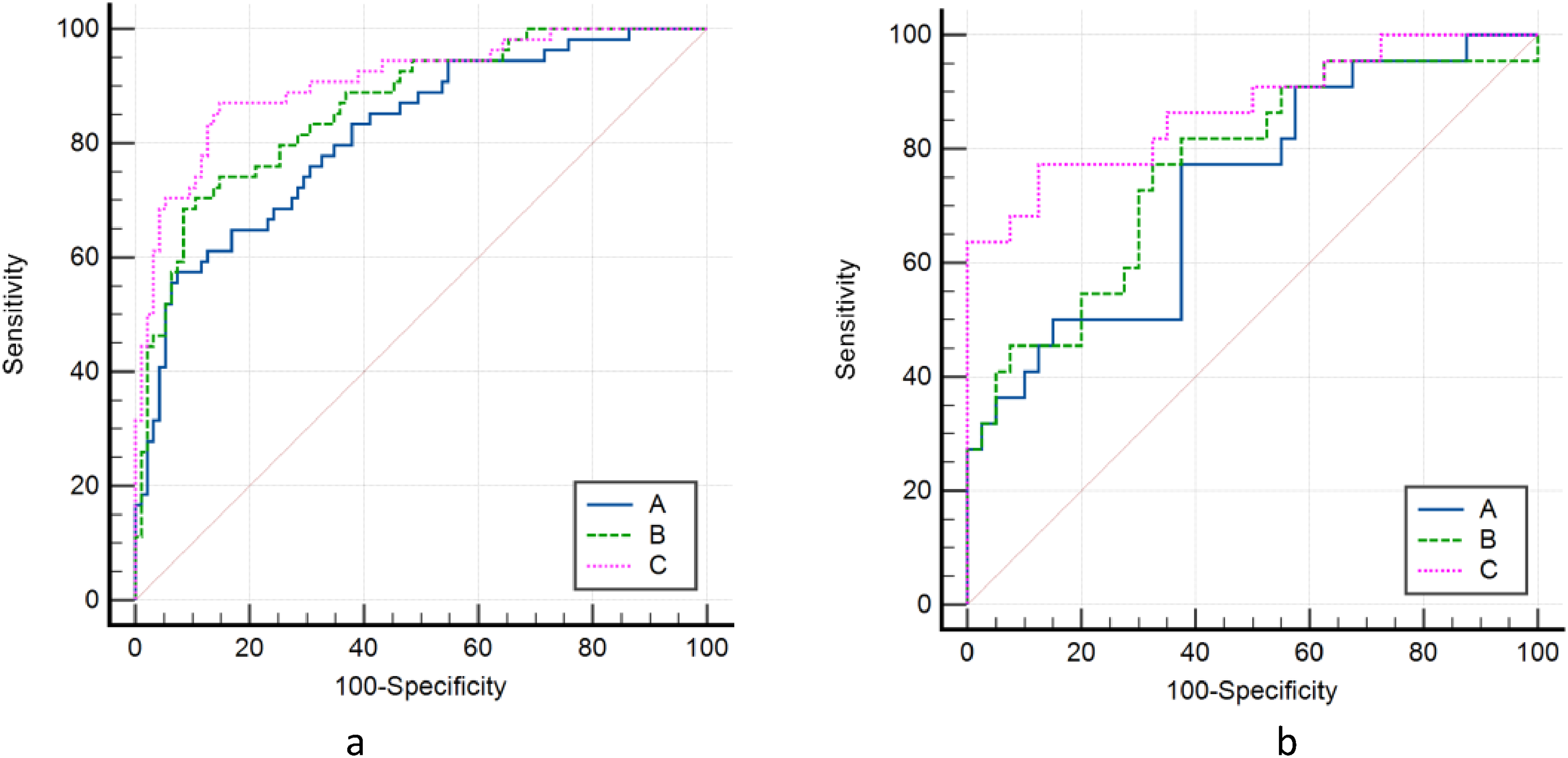
Delong nonparametric curves of the training set (a) and the test set (b). The area under the ROC curve of the combined model of the 2 groups is the largest, which confirms that the combined model has the best predictive performance. Clinical data model (A); imaging model (B); combined model (C).
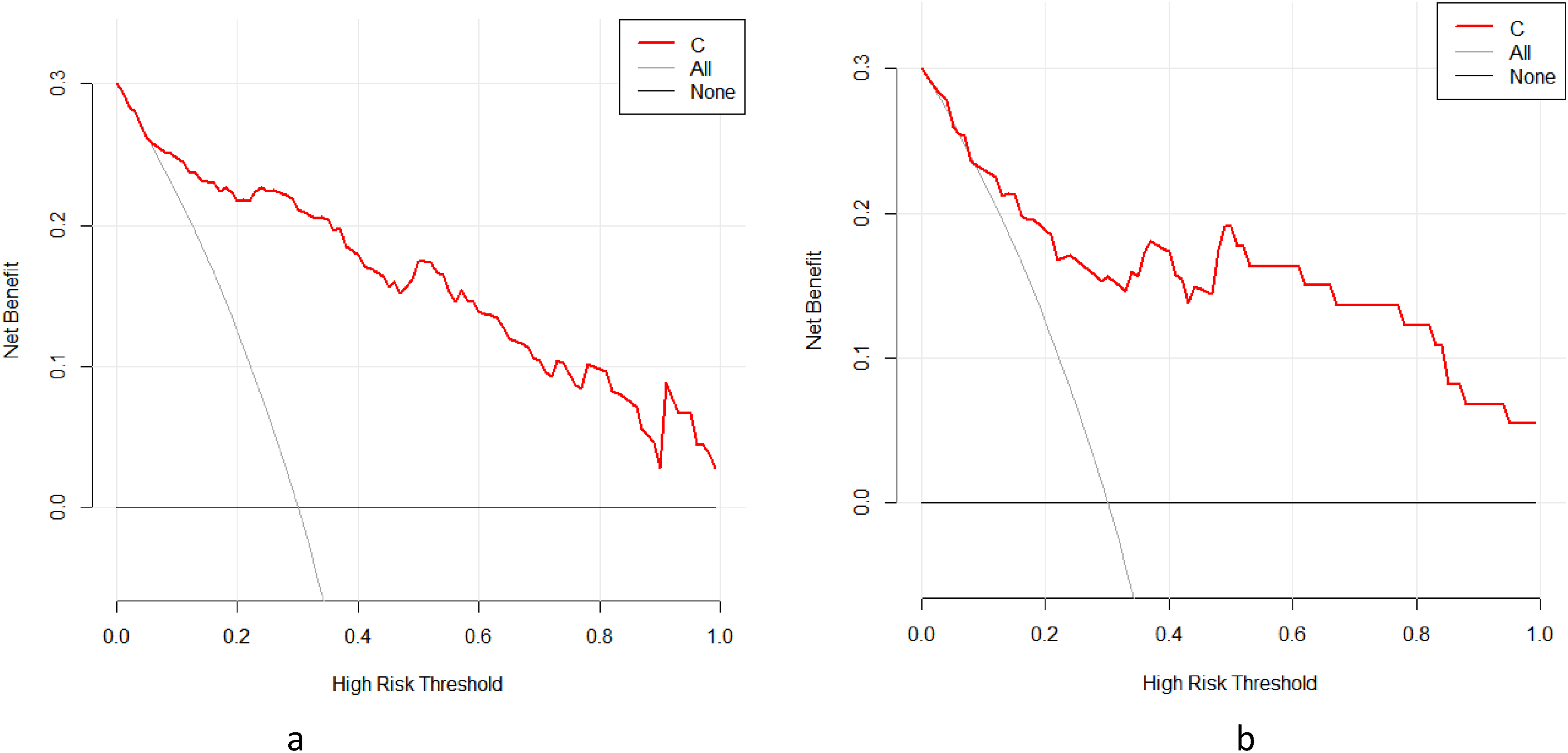
The higher clinical net benefits of the combined model was confirmed in the 2 groups by decision curve analysis (DCA) of training set (a) and test set (b) using R software.

The nomogram prediction tool based on the risk factors of the combined model was used clinically (a, nomogram; b, Calibration). Namely, each risk factor is scored, added together, and the final risk value is calculated.
Logistic Regression Analysis Results of Clinical Model Based on Clinical Characteristics for Predicting the TSCC Prognosis,*P < .05.
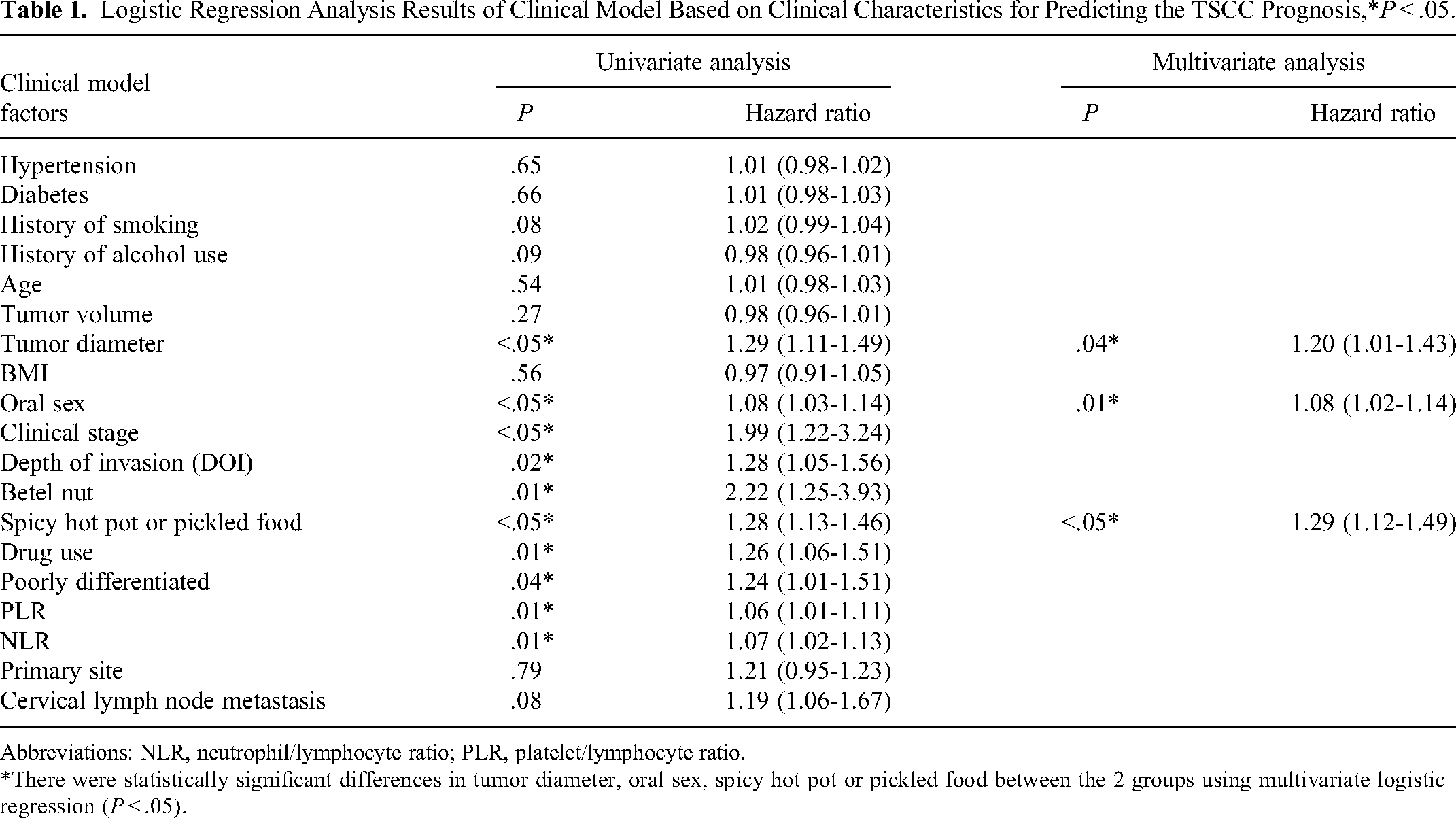
Abbreviations: NLR, neutrophil/lymphocyte ratio; PLR, platelet/lymphocyte ratio.
*There were statistically significant differences in tumor diameter, oral sex, spicy hot pot or pickled food between the 2 groups using multivariate logistic regression (P < .05).
Logistic Regression Analysis Results of Imaging Model Based on MR Characteristics for Predicting the TSCC Prognosis,*P < .05.

*There were statistically significant differences in MR enhancement pattern, Radscore1, Radscore2 between the 2 groups using multivariate logistic regression (P < .05).
Logistic Regression Analysis Results of Combined Model Based on Valuable Factors Mentioned Above for Predicting the TSCC Prognosis, *P < .05.

Abbreviations: NLR, neutrophil/lymphocyte ratio; PLR, platelet/lymphocyte ratio.
*There were statistically significant differences in oral sex, spicy hot pot or pickled food, MR enhancement pattern, and Radscore2, between the 2 groups using multivariate logistic regression (P < .05).
Discussion
Currently, due to factors such as chewing betel nut, eating spicy hot pot, consuming pickled foods, and environmental pollution, the incidence of TSCC in China is increasing year by year, with a rate of 2.0 to 3.5/10 000. Postoperative complications such as dysphasia, eating disorders, psychological disorders, and recurrence and metastasis seriously affect the quality of life of patients.20,21 Tongue squamous cell carcinoma is a common pathological type of oral cancer, and usually when patients seek medical attention, TSCC has already infiltrated the surrounding tissues, making treatment difficult and prognosis poor, seriously affecting the life and health safety of patients. Tongue squamous cell carcinoma is often related to tongue squamous epithelial mutations caused by long-term mucosal irritation or injury, viral infections, immune suppression, ulcers, etc. Early symptoms often manifest as rough white patches on the oral mucosa, which develop into papillary or ulcerative types, or a combination of both, with ulcerative types being more common. In ulcerative types, TSCC cancer cells exhibit obvious dysplasia and more nuclear division and are highly malignant also named nonkeratinizing TSCC. Currently, surgery is the main treatment for TSCC, combined with radiotherapy, chemotherapy, and targeted therapy. According to statistics, about 90% of TSCC in China undergo radical resection, and 20% to 30% of TSCC experience recurrence or metastasis, and even death and other adverse events.14,22,23 Therefore, finding independent risk factors for TSCC prognosis can provide a basis for precise treatment management and improve prognosis and has important clinical significance. In this study, we used LASSO and 10-fold cross-validation to screen reliable MRI radiomics features and established a combined model of TSCC clinical and MRI radiomics features for noninvasive prediction of TSCC prognosis and improved prediction efficiency. The model does not require additional costs and has been proven to have good predictive effects, providing strong support for clinical decision-making for TSCC.
In this study, the rate of adverse events in TSCC surgery patients 1 to 6 years post-surgery was 36.02%, slightly higher than previous studies, which may be related to population differences, severe domestic environmental pollution, and long-term follow-up. Therefore, combining clinical imaging data and long-term follow-up is of great significance for the prognosis management and development of early prediction tools for TSCC. In order to find more effective predictive features for TSCC adverse events, we compared the clinical and radiological features of 2 groups, and single-factor regression analysis confirmed that chewing betel nut, spicy hot pot or pickled food, unclean oral sex, MR enhancement pattern, drug use, DOI, PLR, NLR, low differentiation, clinical stage, and Radscore are significant risk factors (P < .05). Multivariate regression confirmed that spicy hot pot or pickled food, unclean oral sex, MR enhancement pattern, and Radscore2 are independent risk factors for TSCC prognosis. The DOI of TSCC is closely related to cervical lymph node metastasis and pathology differentiation and also affects the surgical method and patient prognosis. It has been reported that the inflammatory environment of tumors can affect their malignant potential and patient prognosis, and an increase in PLR and NLR often indicates that liver and gastric tumors will develop toward pro-tumor growth inflammation, increasing the risk of tumor infiltration, invasion, and recurrence. Both are equally effective for TSCC prognosis. Poor differentiation and clinical staging are classic prognostic indicators for various tumors, which also apply to TSCC, but their specificity is poor because the prognosis of TSCC in this study is closely related to patients’ postoperative peripheral environment and dietary factors. Chewing betel nut, spicy hot pot or pickled food, unclean oral sex, drug use, and MRI-Radscore1/Radscore2 are new risk factors for TSCC prognosis discovered in this study. In China, most migrant workers in Guangdong, Guangxi, and Hunan provinces (about 60 million) love to chew betel nut, which usually causes: ① physical damage; when chewing betel nut, its fibers inevitably cause damage to the tongue mucosa. If there is a long-term habit of chewing betel nut, this physical damage will exist for a long time, causing chronic inflammation of the local tongue mucosa, inducing cancer formation; ② chemical damage: betel nut contains many alkaloids and polyphenols, such as arecoline and tannins, which are all biologically cytotoxic and can induce programmed cell death of epithelial cells on the tongue mucosa, interfering with the precipitation and degradation of extracellular matrix macromolecules and inducing cancer.24,25 However, many TSCC postoperative patients still insist on chewing betel nut, which is bound to lead to poor prognosis. Spicy hot pot is a common delicacy in Western China. With the spread of food culture, it has also been loved by many foreign friends. However, spicy hot pot often adds a lot of advanced red pepper (Scoville heat units > 2500 SHU), and the food temperature is high, which will cause strong stimulation, burns, and ulcers on the surface of the tongue mucosa, not to mention chemical damage. The probability of cancer transformation in the continuously repaired and thickened tongue mucosa will increase significantly. With the opening up of the economy, domestic partner ideas have become more open. Excessive unclean oral sex can cause bacterial and viral infections and mechanical damage. However, due to conservative ideas in China, such people are reluctant to seek medical treatment even if they repeatedly have tongue infections and ulcers due to shame and other reasons, ultimately leading to adverse events. Drugs themselves contain a large number of harmful chemicals. Long-term use of methamphetamine can cause oral environmental disorders, tongue mucosal cell mutations, and immune deficiency. Pickled food is a characteristic delicacy in China. Its production process involves carbon fire smoking and pickling or fermentation, which can cause a large amount of nitrite and mycotoxin damage to the tongue mucosa, inducing cancer.26–28 In 2012, Lambin et al. first introduced the concept of radiomics and expanded it to MR and CT diagnosis. Currently, the imaging analysis of lung nodules has been applied clinically and has received good reviews. This study found that Radscore is an important influencing factor for TSCC prognosis. We extracted 2 reliable Radscores of the tongue MR in 2 groups to represent the comprehensive texture differences between lesions and obtained good predictive results, confirming that the underlying texture features of the tumor represented by Radscore can help distinguish the malignant potential of the tumor. Based on the above risk factors, we established 3 predictive models in the training set and obtained external validation of the test set, confirming the higher predictive performance and clinical net benefits of the combined model, and produced a reliable nomogram for prognosis prediction. The nomogram integrates the clinical and radiological information of TSCC, which can well mine clinical imaging data, reduce imaging interpretation bias, better reflect the population prognosis differences of TSCC, and provide important data support for TSCC clinical decision-making.29–31 The combined model and nomogram to some extent simplify the process of predicting TSCC prognosis. During the follow-up process, if oral sex (≥26.25 times/month), spicy hot pot or pickled food (≥9.75 times/month), MR enhancement pattern (≥5.25 TIC), and Radscore2 (≥6.75) exceed the threshold, adverse prognosis will be considered, treatment strategies will be timely changed and strengthened, and follow-up will be adopted.
Limitation
The sample size of included patients is relatively small in a single-center study. It is inevitable to consider the potential impact of small sample sizes on the validity and applicability of the results when interpreting the findings. The study only analyzed a total of 211 patients with TSCC, which may limit the generalizability and reliability of the findings. A larger sample size would strengthen the study's conclusions and increase the robustness of the predictive model in the future. The sample size also wasn’t calculated via stratified random sampling, whole group sampling, or other statistical methods. Moreover, The data analysis of this study only uses the Logistic regression method; high data discrepancy requirements (P all < .05) may overlook some potentially effective influencing factors (P≈.05); Therefore, in the future, we will collaborate with more medical centers to conduct multicenter studies and validate or supplement our research model using deep learning or artificial intelligence data analysis.32,33
Conclusions
In summary, the postoperative management and survival of TSCC in China still face many difficulties and challenges. The combined model based on clinical features and MR radiomics provides a new approach for TSCC treatment management, which can further improve clinical decision-making and postoperative survival rate of TSCC.
Footnotes
Abbreviations
Acknowledgments
We thank Graduate Education Research Project Fund of Hubei University of Medicine (YJ2022013), Xiangyang Science and Technology Plan Key Project Fund (2022YL34A), the “323” Public Health Project of the Hubei health commission and the Xiangyang No.1 People’s Hospital (XYY2022-323), and the Natural Science Foundation of Hubei Province (grant numbers 2022BCE021 and 2022CFD010), and Innovative Research Program of Xiangyang No.1 People’s Hospital (XYY2023QT04).
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Author Contributions
J.L., L.S., and P.A. conceived and drafted the manuscript. M.Y., Y.H., and J.Z. contributed to the literature review. Y.Y., X.L., P.S., and J.Z. is responsible for the quality control of article statistics. P.S., Y.Y., and J.W. revised the manuscript critically for important intellectual content. G.F.,H.G.,and P.A. approved the final version to be published and agreed to act as guarantors of the work. J.L., L.S., and J.Z. contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The experimental protocol was established, according to the ethical guidelines of the Helsinki Declaration and was approved by the Human Ethics Committee of Xiangyang No.1 People's Hospital affiliated to Hubei University of Medicine (Issue No. 3012 [2012]). And the date of approval to this manuscript: March 1, 2012; Written informed consent was obtained from individual or guardian participants.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Graduate Education Research Project Fund of Hubei University of Medicine (YJ2022013) (YingJian Ye), Xiangyang Science and Technology Plan Key Project Fund (2022YL34A).