
Abstract
With the improvement of diagnostic techniques, numerous uncommon metastases derived from breast cancer were reported. However, very few studies explored the clinical characteristics and prognostic patterns of these patients. A total of 82 cases of uncommon metastatic breast cancer (MBC) registered at our hospital from January 1, 2010, to July 1, 2022, were selected for this retrospective study. The diagnoses of uncommon metastases were based on pathology, and the potential prognostic indicators (overall survival [OS], uncommon disease-free interval [uDFI], and remaining survival [RS]) were estimated. The uncommon metastases involved distant soft tissue, parotid gland, thyroid, digestive system, urinary system, reproductive system, bone marrow, and pericardium. Stepwise multivariate Cox regression analysis indicates age ≤ 35 is an independent risk factor of poor outcome of OS, uDFI, and RS in uncommon MBC patients. Meanwhile, uncommon metastasis combined with common visceral metastasis is an independent risk factor for poor RS of uncommon MBC patients, with a hazard ratio of 6.625 (95% confidence interval = 1.490-29.455, P = .013). Post hoc pairwise comparisons showed that uncommon MBC patients who developed bone-only metastasis survived longer than those concomitant with common visceral metastasis (P = .029). Although the incidence is low, uncommon MBC may involve multiple metastatic sites. The delayed diagnosis of uncommon metastases could lead to systemic progression of the disease. However, patients who only develop uncommon metastasis have a significantly better prognosis than that of those combined with common visceral metastasis. Even for those complicated by bone-only metastasis, active treatment of bone metastases can still achieve substantially longer survival.
Keywords
Introduction
According to global cancer statistics, breast cancer is the most prevalent malignancy and the leading cause of mortality among women worldwide. 1 Among breast cancer patients, metastasis, rather than growth of the primary tumor, 2 is responsible for approximately 90% of deaths related to the disease. Metastatic breast cancer (MBC) is an incurable disease with a limited median survival time of 2 to 3 years, and bone, lung, liver, and brain are the most common metastatic sites.3,4 Advancements in treatment and imaging technology have led to an increasing number of patients with common metastatic breast cancer (MBC) achieving remission and stability. Meanwhile, there has been a notable uptick in the identification of uncommon metastatic sites in recent years.5,6 Due to the lack of treatment guidelines, there are varying treatment goals and treatment decisions (systemic treatment alone or combined with locoregional treatment) for this uncommon metastatic disease depending on individual physicians, potentially leading to either overtreatment or inadequate treatment. To the best of our knowledge, there are very few studies investigating the clinical characteristics, treatment, and prognosis of uncommon MBC. Our current perception of uncommon MBC mostly comes from case reports and literature reviews. However, substantial heterogeneity in patient characteristics and medical decisions appeared across these case reports, resulting in a marked variation in prognoses. Herein, we reviewed all MBC patients registered in our hospital from January 1, 2010, to July 1, 2022, and 82 patients with pathological diagnoses of uncommon MBC were retrospectively analyzed. The epidemiological characteristics, clinical features of interest, treatment, and prognosis of the primary and metastatic sites were reported. The objective of this study was to assess the potential risk factors affecting survival outcomes and provide additional evidence to inform treatment strategies and enhance prognosis for uncommon metastases derived from breast cancer.
Materials and Methods
Definition
In this study,
Uncommon metastases were defined as metastatic sites of breast cancer exclusive of distant lymph nodes, chest wall, breast, brain, bone, lung, liver, pleura, and peritoneum. Uncommon metastases with bone-only metastasis were defined as primary breast cancer that developed both uncommon metastases and bone metastases, but not occurred common visceral metastases. Uncommon metastases with common visceral metastases were defined as metastatic sites of breast cancer including brain, lung, liver, pleura, and peritoneum.
Data Collection and Patients’ Selection Criteria
From January 1, 2010, to July 1, 2022, all patients diagnosed with uncommon metastases from 6274 consecutive breast cancer patients with stage IV disease registered in our hospital were enrolled in this retrospective study. This retrospective study was conducted in accordance with the Declaration of Helsinki (approval number: XMFHIIT-2022SL025). We have de-identified all patient details. The reporting of this study conforms to the REMARK guidelines. 7 All uncommon metastatic sites were confirmed by corresponding pathological examination reports.
Clinical characteristics; prognostic factors of overall survival (OS); interval to progression from primary breast sites to initial diagnosis of uncommon metastases, also known as uncommon disease-free interval (uDFI); and remaining survival (RS) of these patients were investigated. Therefore, the relevant medical records of these 82 patients, including the date of diagnosis of primary breast cancer, initial diagnosis date of uncommon metastases, and latest survival status, were collected. The following baseline features were also collected: age, menstrual status, primary histology (including invasive ductal carcinoma, invasive lobular carcinoma, and other invasive breast carcinoma of special type), primary molecular subtype (hormone receptor-positive/human epidermal growth factor receptor 2 negative [HER2-] breast cancer vs hormone receptor-negative breast cancer), pathological stage of local lymph node metastasis (N0 vs N1 vs ≥N2), presence or absence of blood vessel invasion, concomitant metastasis (developing uncommon metastasis only, uncommon metastases combined with bone-only metastasis, uncommon metastases combined with common visceral metastasis), molecular subtypes of uncommon metastatic sites, and treatment regimens (systemic therapy alone or locoregional treatment combined with systemic therapy). Patients were excluded at the last follow-up date if they were lost to follow-up or chose not to provide the latest information.
Statistical Analysis
OS, uDFI, and RS were estimated using the Kaplan-Meier method, and the difference in survival between the subgroups was compared by using a log-rank test. To estimate the potentially relevant risk factors of survival indicators (OS, uDFI, and RS) in the cohort of 82 patients, the baseline characteristics (age, histology, molecular subtype, pathological stage of local lymph node metastasis, blood vessel invasion, hormone receptor expression conversion, combined common metastasis, and treatment regimens) were used as covariates in multivariate Cox regression models (forward stepwise regression). The SPSS statistical software (version 25.0, IBM Corporation, Armonk, NY, USA) was used for data analysis. P<.05 was considered to be statistically significant, and all statistical tests were two-sided.
Results
Characteristics of Uncommon Metastasis
Overall, 91 cases were identified as having uncommon metastases among 6274 consecutive stage IV breast cancer cases from Jan 1, 2010, to July 1, 2022. After exclusion of 9 patients due to lack of basic information, a total of 82 patients with uncommon MBC were retrospectively reviewed in this study (Figure 1).

Flowchart of the patient selection and survival status of 82 patients with uncommon metastatic breast cancer.
The median age at initial diagnosis of the primary neoplasm was 45 years old (30-79 years). The median follow-up period was 113.5 months (95% confidence interval [CI] = 93.58-133.42 months). Among them, 11 patients lost follow-up before the end of the follow-up date, and the lost-to-follow-up rate was 13.4% (11 of 82). The baseline characteristics of the 82 patients included in the analysis are shown in Table 1.
Clinical Characteristics and Univariate Analysis of Initially Diagnosed Patients with Uncommon Metastatic Breast Cancer.

Abbreviations: OS, overall survival; uDFI, uncommon disease-free interval; RS, remaining survival after uncommon metastases; NR, not reach; NA, not available; AJCC, American Joint Committee on Cancer; TNBC, triple-negative breast cancer; pLN stage, pathological lymph nodes stage.
Luminal B subtype included hormone receptors positive and HER2 negative only.
Others included invasive breast carcinoma of special type, such as invasive micropapillary carcinoma, invasive metaplastic carcinoma, and invasive cystosarcoma phyllodes.
In our analysis, the multiple uncommon metastatic sites involved can be divided into 9 subtypes of classifications (Supplement 1), which were distant skin metastasis in 19 patients (including abdominal wall, back, buttock, elbow, temporal, scalp, and nose), reproductive system metastasis in 15 patients (including the uterus and ovaries), pericardial metastasis in 14 patients, digestive system metastasis in 12 patients (including esophagus, stomach, duodenum, jejunum/ileum, pancreas, colon, and rectum), adrenal gland metastasis in 6 patients, thyroid metastasis in 3 patients, urinary metastasis in 2 patients (including kidney and bladder), bone marrow metastasis in 21 patients, and parotid gland in 1 patient. Specifically, the 82 patients were stratified based on the concomitant common distant metastatic lesions for subgroup analysis, as shown in Table 2. Patients who only developed uncommon metastatic sites accounted for 22% (18 of 82). Patients who were complicated with bone metastasis but without the involvement of common visceral sites accounted for 30.5% (25 of 82). Patients with common visceral metastasis accounted for 47.5% (39 of 82).
Characteristics and Univariate Analysis of Uncommon MBC Patients.

Abbreviations: OS, overall survival; RS, remaining survival after uncommon metastases; NR, not reach; NA, not available.
Diagnosis and Treatment Patterns
Among 82 patients, 41 cases (50.0%) were confirmed by needle aspiration/core needle biopsy or endoscopic biopsy, and 41 cases (50.0%) were confirmed by surgical resection including salpingo-oophorectomy, hysterectomy adrenalectomy, nephrectomy, thyroidectomy, partial colectomy, or removal of the suspected lesions. All the patients with ovarian metastasis received confirmation of diagnosis after ovarian castration with no relevant preoperative imaging abnormality of the ovary. The immunohistochemical results of the primary and metastatic lesions were divided into 2 groups: hormone receptor expression converted from ER + or PR + to ER-/PR- and the hormone receptor expression was consistent or converted from ER-/PR- to ER + or PR + . Detailed results are shown in Table 2. The univariate survival analysis of the OS (P = .160) and RS (P = .578) showed no significant difference between the 2 groups.
After the diagnosis of uncommon metastasis, 31 (37.8%) patients received a systemic treatment combined with locoregional treatment, 48 (58.5%) patients received systemic treatment only, and 3 patients lost follow-up due to personal reasons. Systemic therapy included palliative chemotherapy, anti-HER2 targeted therapy, and endocrine therapy. Locoregional treatment included surgical resection, local radiotherapy, and thoracic/intraperitoneal lavage of chemotherapy drugs. Detailed results are shown in Table 2. The univariate survival analysis on the OS (P = .783) and RS (P = .881) showed no significant difference between the 2 groups.
Survival
As shown in Figure 1, a total of 31 (37.8%) patients with uncommon MBC died during the follow-up period. In this study, the median OS (mOS) from primary breast cancer to death was 170.2 months (95%CI = 43.03-197.37), and the median time from primary breast cancer to initial diagnosis of uncommon metastasis (muDFI) was 121.3 months (95%CI = 56.88-185.72). The median RS (mRS) from the initial diagnosis of uncommon metastasis to death was 66.8 months (95%CI = 26.42-107.19). The 5 characteristics listed in Table 1 related to primary breast cancer were analyzed for patients’ uDFI. Univariate analysis showed that age ≤ 35 was an independent predictor of poor prognosis in uncommon MBC patients, with OS (P = .016) and uDFI (P = .009) and RS (P = .049) (shown in Table 1). The presence of blood vessel invasion (P = .032) was associated with tumor metastasis from the breast to an uncommon site. Uncommon MBC patients with common visceral metastasis showed a shorter RS than that of patients who only developed uncommon metastasis without metastasis to any common metastatic sites and uncommon MBC patients who had bone-only metastasis (P = .037).
Multivariate Cox regression analysis by using forward stepwise yielded prognostic factors for survival is shown in Table 3. Patients with age > 35 and luminal A/B (HER-2 negative) subtype showed longer mOS than that of patients with age ≤ 35 (hazard ratio [HR] = 0.336 95%CI = 0.145-0.779, P = .011) and HER-2 positive/TNBC subtype (HR = 2.549 95%CI = 1.126-5.772, P = .025) (see Figure 2).

Kaplan-Meier curves of overall survival (OS) in age ≤ 35 versus age>35 patients with rare metastatic breast cancer (left) and in luminal A/B (HER-2 negative) versus HER-2 positive/TNBC patients with rare metastatic breast cancer (right).
Multivariable Cox Models to Determine Factors Associated with Survival in Patients with Uncommon Metastatic Breast Cancer.

Abbreviations: HR, hazard ratio; CI, confidence interval.
Similarly, in the analysis of uDFI, patients with age > 35 and luminal A/B (HER-2 negative) subtype showed longer mOS than that of patients with age≤35 (HR = 0.315 95%CI = 0.186-0.834, P = .004) and HER-2 positive/TNBC subtype (HR = 2.301 95%CI = 1.039-5.094, P = .040) (Figure 3). Using multivariate Cox regression analysis of the factors associated with RS, the baseline characteristics such as the age of primary disease, molecular subtype, hormone receptor expression conversion, and treatment regimens after uncommon metastasis occurrence were not associated with RS of uncommon MBC patients. Using patients who only developed uncommon metastasis (mRS = 95.6 months, 95%CI = 66.68-124.57) as a reference, those combined with common visceral metastasis (mRS = 49.5months, 95%CI = 29.52-69.42) had a shorter RS (HR = 6.625 95%CI = 1.490-29.455, P = .013). However, no obvious survival difference was observed in those uncommon MBC patients with bone metastasis only (mRS = 90.0 months, 95%CI = 63.75-116.29). Post hoc pairwise comparisons showed those with bone metastasis had a better survival performance than that of those with common visceral metastases (P = .029) (Figure 4). (Note: Since less than half of patients who only developed uncommon metastases died, we chose to report the mean survival time for RS.)
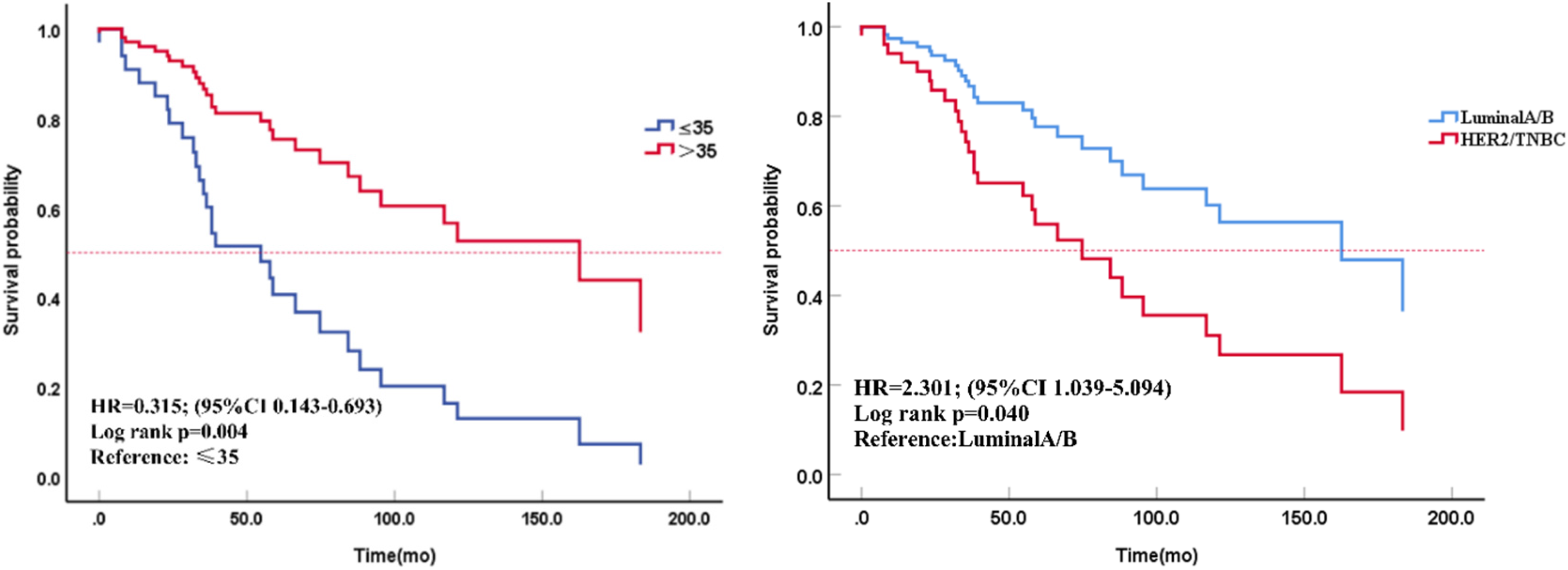
Kaplan-Meier curves of uncommon disease-free interval (uDFI) in age ≤ 35 versus age > 35 patients with rare metastatic breast cancer (left) and in luminal A/B (HER-2 negative) versus HER-2 positive/TNBC patients with rare metastatic breast cancer (right).
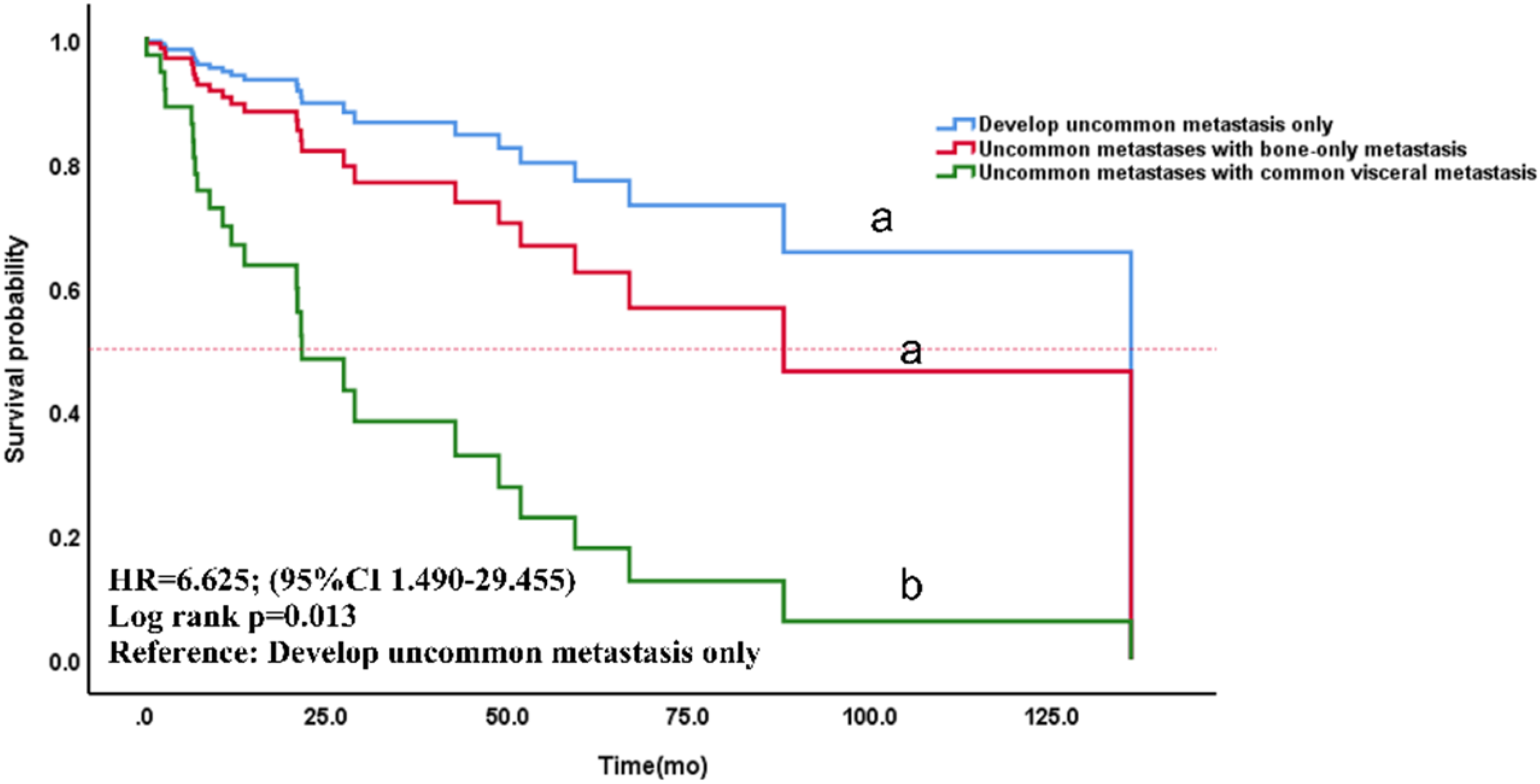
Kaplan-Meier curves of remaining survival (RS) in breast cancer patients only developed uncommon metastasis versus uncommon breast cancer metastasis with bone-only metastasis versus uncommon breast cancer metastasis with common visceral metastases.
Discussion
Despite considerable progress in treatment modalities, survival rates of MBC are still only 27% on average. 8 There is limited evidence on the diagnosis and treatment of uncommon MBC compared with common metastatic disease. Clinicians typically depend on sporadic case reports and case series to make their clinical decision-making. However, such reports only marginally enhance our comprehension of the clinical features of rare metastatic sites in MBC. Meanwhile, patients’ outcomes are highly heterogeneous due to individual differences and physicians’ decision. To our knowledge, this is as of now the largest cohort of pathologically diagnosed uncommon MBC.
As shown in Table 1, the median age at diagnosis for primary breast cancer of these 82 women was 45, similar to the peak age of breast cancer diagnosis for Asian women. 9 In Asian women, breast cancer tends to develop earlier in life, so it affects more premenopausal women than Western women. 9 Young breast cancer patients (mostly defined as age at initial diagnosis ≤ 35 years) have the propensity to develop phenotypes that are more malignant, leading to more aggressive biologic behaviors. So, young age seems to be an independent risk factor for local recurrence and even OS. 10 The univariate analysis conducted in the present study demonstrated that age ≤ 35 was one of the major predictors of poor prognosis affecting OS, uDFI, and RS in uncommon MBC patients. When adjusting for all prognostic variables, age ≤ 35 was still significantly related to mortality with an HR of 2.822 (95%CI = 1.227-6.490) and uncommon disease progression with an HR of 3.178 (95%CI = 1.443-6.996) compared to older women. As shown in our study, younger age has been generally accepted as an independent adverse prognostic indicator of survival in breast cancer.11,12
It is worth noting that young women are usually in premenopausal status at the initial diagnosis of breast cancer, and patients need to be treated with ovarian function suppression (OFS) in the process of subsequent endocrine therapy. Now, most women choose to receive drug-induced ovarian function suppression. In this study, 12 patients with ovarian metastasis were diagnosed by pathological examination after surgical castration, and no abnormal imaging findings of the ovaries were found in preoperative imaging evaluation. This finding suggests that for premenopausal patients with a high-risk of recurrence, the risk of ovarian metastasis should be considered in the subsequent selection of the approach of ovarian castration in order to detect ovarian metastasis early and improve survival. At present, the subsequent follow-up principle of young breast cancer patients follows the same principles as elderly patients. 13 Our study raised the question that age, an independent risk factor for poor prognosis associated with uncommon metastasis, should be a focus of follow-up of young breast cancer. Further research is still needed to specifically address this concern for young breast cancer patients.
Previous studies have shown that there are preferential metastatic sites for different molecular subtypes of primary breast cancer.11,14–16 However, it remains unclear whether this also applies to the different uncommon metastatic sites. As shown in Supplement 1, HER-2 positive/TNBC metastatic breast cancer patients accounted for a larger proportion of distant skin metastatic disease than that of those with hormone receptor-positive/HER2- (68.4% vs 31.6%). Previous studies have shown that distant skin metastasis usually has a relatively good prognosis after systemic treatment, and most patients eventually die due to visceral metastases. It is worth noting that Graziano et al 17 reported 2 HER2-positive advanced breast cancer patients combined with distant skin metastases received anti-HER-2 targeted therapy for visceral metastasis and obtained partial remission, while skin metastases progressed during treatment. The different responses between skin metastatic lesions and visceral organs treated with anti-HER2 targeted therapy may be related to the immunological effects on the skin. At this time, local radiation may help to relieve cutaneous metastatic lesions. 18 In addition, patients of luminal subtypes accounted for a higher proportion than HER-2 positive/TNBC patients with bone marrow metastasis (81.0% vs 9.5%) and pericardial metastasis (64.3% vs 35.7%). These data echo with the previous reports that the existence of disseminated tumor cells (DTC) in bone marrow metastasis was correlated with the adverse outcome of luminal A metastatic breast cancer patients (P = .008). 19 There is no report on the difference in pericardial metastasis influenced by different molecular subtypes of breast cancer. In this study, after multivariable adjustment, the HER-2 positive/TNBC subtype is associated with the occurrence of rare metastases (HR = 2.301 95%CI = 1.039-5.094, P = .040) and the worse OS of uncommon MBC patients (HR = 2.549 95%CI = 1.126-5.772, P = .025), similar to common metastatic breast cancer patients. However, when diagnosed with uncommon MBC, there was no correlation between the molecular subtypes and the RS of these patients (P = .743). The findings of this study indicate that subtype recognition using ER, PR, and HER-2 immunophenotypes may be helpful in estimating the occurrence of uncommon metastases, and the potential preference of different uncommon metastatic sites driven by various molecular subtypes warrants further studies.
It is suggested that uncommon MBC combined with common metastatic sites is usually highlighting a worsening systemic disease, 5 while the uncommon metastasis itself did not appear to affect the survival. 6 Previous studies on common MBC revealed that patients with bone-only metastasis have the best long-term prognosis, which is characterized by the long course of disease and slow progress. Patients combined with liver and brain metastasis have poor overall survival, while those combined with lung metastasis seem to have no effect on survival. 20 Studies have shown that diverse patterns of distant metastasis have varying impacts on the survival of patients even if they both exhibited stage IV breast cancer. In this study, when initially diagnosed as uncommon MBC, patients only with uncommon metastases accounted for 18 cases (22.0%), while uncommon MBC patients combined with bone-only metastasis and with common visceral metastasis accounted for 25 cases (22.0%) and 25 cases (47.5%), respectively. The mean RS of the patients in these 3 groups was 95.6, 90.0, and 49.5 months, respectively. There were significant differences among the three groups (P = .037). After multivariable adjustment, the common visceral metastasis of breast cancer was found to be an independent risk factor for poor RS of uncommon metastatic breast patients. Pairwise comparison showed that uncommon MBC patients combined with bone-only metastasis did not have a worse survival time in comparison to those only developed metastasis only at uncommon sites (P = .458) but had longer RS than those with common visceral metastases (P = .029). The results suggested that for certain stage IV breast cancer patients who only had uncommon metastases, the progression of bone metastasis seemed not to deteriorate the survival. Active anti-bone metastasis treatment can be still beneficial to yield a substantial survival period.
Hormone receptor expression is an important predictor of the efficacy and prognosis of endocrine therapy for breast cancer, and its expression affects subsequent clinical decision-making. 21 Based on patients with uncommon MBC in our study, there was no significant difference in OS (P = .160) and RS (P = .578) between the groups with the conversion of hormone receptor expression. However, it is worth noting our predesigned grouping is not detailed enough due to the sample size limitation, so the results should be interpreted with caution. Further studies with larger sample sizes are required to investigate the correlation between hormone receptor expression conversion, incidence, and survival of uncommon metastatic breast cancer.
When uncommon metastasis occurs, it is usually difficult for clinicians to decide whether systemic therapy should be combined with locoregional treatment or not. This may lead to either overtreatment or inadequate treatment. Different from bone marrow metastasis and pericardial metastasis,22,23 when the rare metastatic sites involve the skin or solid/hollow organs (especially an isolated uncommon metastatic site), local radiotherapy or complete resection can be performed for local intensive treatment on the basis of systemic therapy.24–27 Different treatment patterns may lead to different prognoses for these patients with metastatic breast cancer. For selected patients with solitary adrenal metastases, laparoscopic adrenalectomy can provide a survival benefit. 26 When breast cancer metastasizes to the orbit and paranasal sinuses, surgical resection may be considered in the case of a single metastatic lesion. Palliative chemoradiotherapy and immunotherapy are considered for unresectable disease, which is associated with high rates (60%-80%) of clinical improvement of local symptoms and vision.24,27 The same decision is applicable to parotid metastasis of breast cancer, but attention should be paid to the protection of the facial nerve during operation.28,29 For digestive system metastasis, some researchers advocated that systemic treatment should be used as a first-line clinical decision 30 and surgical resection should be applicated only when presenting with obstruction symptoms. 31 But compared with the first-line application of systemic therapy combined with local resection, the improvement of median survival time of patients is still controversial, and there is no significant difference in OS. 32
There were some limitations in this study. Firstly, the sample size is modest, which led to an inevitable heterogeneity and made it unpractical to further explore different patterns of different uncommon metastatic sites. Secondly, a substantial proportion of the primary breast cancer patients were initially diagnosed and treated at outside facilities/hospitals, which might lead to potential recall bias in the description of the relevant characteristics of primary breast cancer. Despite these limitations, our study is currently the largest sample from a single center, which further suggested the relatively good survival of uncommon MBC patients with bone-only metastasis and the necessity of active treatment for bone metastasis. In addition, some potential prognostic predictors of uncommon MBC patients were provided for clinicians as a reference.
Conclusion
In conclusion, in addition to bone, liver, lung, and brain, systemic dissemination of breast cancer can also involve multiple other sites. Breast cancer patients who only developed uncommon metastasis have significantly better survival than those with common visceral metastasis. Even for uncommon MBC patients combined with bone-only metastasis, a substantially improved prognosis can still be achieved with active anti-bone metastasis therapy. At present, the uncommon MBC remains clinically under-recognized and undertreated. Further subdivision of the rare metastatic sites is needed to explore the prognostic model.33–35
Supplemental Material
sj-pdf-1-tct-10.1177_15330338231184990 - Supplemental material for Clinical Features and Prognosis of Uncommon Metastatic Breast Cancer: A Retrospective Analysis of 82 Cases
Supplemental material, sj-pdf-1-tct-10.1177_15330338231184990 for Clinical Features and Prognosis of Uncommon Metastatic Breast Cancer: A Retrospective Analysis of 82 Cases by Yusi Zhang, MD, Chenyu Sun, MD, Vicky Yau, MD, Shuanglong Chen, MD, Qingmo Yang, MD, Wenlin Chen, MD, Scott Lowe, MD, Rachel Bentley, MD, and Zhong Ouyang, MD in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Acknowledgments
Not applicable.
Authors’ Contributions
All authors contributed to the study's conception and design. Material preparation, data collection, and analysis were performed by YSZ, CYS, VY, and WLC. The first draft of the manuscript was written by YSZ and CYS, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the first author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This retrospective study was approved by the Ethics Committee of The First Affiliated Hospital of Xiamen University on the basis of the Declaration of Helsinki (approval number: XMFHIIT-2022SL025), with an exemption from informed consent. No specific consent is needed for statistical analyses of aggregated de-identified data. For this study, the raw data were first extracted from HIS, and patients’ identities, including names, screening IDs, patient IDs, and mobile phone numbers, were de-identified.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.