
Abstract
Introduction
Esophageal cancer stands at the eighth most common cancer with significant morbidity and mortality.1 Due to late diagnosis, rapid progression, and high rate of recurrence, treatment results of patients with esophageal cancer are usually less optimistic. To take timely and effective treatment strategies against esophageal cancer, it is important for us to explore available predictive factors for prognosis and clinicopathologic characteristics of esophageal cancer patients.
Host inflammatory responses had been reported as correlating with tumor initiation and development, and increased inflammatory response often indicates poor prognosis.2 Inflammatory response may alter the relative levels of circulating white blood cells. In particular, the level of neutrophils increases, while that of lymphocytes declines.3
In previous studies, neutrophil-to-lymphocyte ratio (NLR) was proven to be a useful indicator in prostate cancer, gastric cancer and lung cancer.4–6 There were also studies that examined the relation between NLR and prognosis in patients with esophageal cancer.7–9 However, these studies were all limited to small study numbers and had different results. Recently, more and more clinical trials have been done to evaluated the relationship of NLR and esophageal cancer. We have a chance to systematically assess the prognostic role of NLR on oncologic outcomes of esophageal cancer. Oncologic outcomes include overall survival (OS), cancer-specific survival (CSS), progression-free survival (PFS), and disease-free survival (DFS). Clinicopathologic parameters include tumor length, tumor differentiation, tumor invasion depth, lymph node metastasis, metastasis stage and tumor-node-metastasis (TNM) stage.
Materials and Methods
This study followed the guidelines of the Meta-analysis of Observational Studies in Epidemiology group (MOOSE).10 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines11 were used for study design, search strategy, screening and Reporting. Our protocol for this study has been registered with INPLASY (registration number: INPLASY2021100111).
Literature Search
A systematic literature search was performed using PubMed, Cochrane Library, Embase, Web of Science, MEDLINE, and CNKI up to January 12, 2020. Terms “NLR” (or “neutrophil lymphocyte ratio,” “neutrophil to lymphocyte ratio,” “neutrophil-to-lymphocyte ratio”) AND “esophageal cancer” (or “esophageal Neoplasm,” “esophageal carcinoma”) AND “prognosis” (or “prognoses,” “prognostic,” “survival”) AND “inflammation” were used in the literature search. Related articles and reference were also reviewed.
Inclusion and Exclusion Criteria
Studies were selected according to the following criteria: 1) esophageal cancer was diagnosed with pathology; 2) NLR was measured before treatment from serum with a clear cutoff value; 3) the association between NLR and prognosis (OS, CSS, PFS, and DFS) or clinicopathologic parameters was evaluated.
Articles were excluded when the following situations existed: 1) abstract, letter, editorial, expert opinion, review, case report, concerned nonhuman research, or full text was not available; 2) studies did not directly report hazard ratios (HRs) or odds ratio (OR) or corresponding 95% confidence intervals (CIs), and there was no sufficient data to estimate; and 3) studies contained duplicate data or repeated analysis.
Assessment of Study Quality and Risk of Bias
The Newcastle-Ottawa Scale (NOS) was used for assessing quality of the non-randomized studies. NOS includes three aspects of evaluation: selection, comparability, and outcome in the case and control groups.12 A star system was used with a total score ranging from zero to nine stars. Studies with a score of 7 stars or greater were regarded as high-quality researches.
Data Extraction
Data were collected and extracted independently by two reviewers to avoid inconsistent evaluation and extractor bias. If the reviewers had any disagreements, those disagreements were resolved by a third reviewer. The following items were recorded for each study: authors, year of publication, country, study period, number of participants, gender, mean age, survival type, cutoff value for NLR, treatment strategy, pathological type, TNM stage, hazard ratio (HR) or OR with corresponding 95% CI (confidence interval) and its statistical method.
Outcome Measures
NLR was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count. OS was defined as the time between curative treatment and patient death or date of last follow-up. CSS was defined as the percentage of people who have not died from esophageal cancer in a defined period of time; which usually begin at the time of diagnosis or at the start of treatment and ended at the time of death (patients who died from causes other than the esophageal cancer being studied are were not counted in this study). PFS was defined as the length of time during and after the treatment of esophageal cancer. DFS was estimated from the day of treatment until the detection of cancer recurrence.
Statistical Analysis
HRs and 95% CIs were used to analyze the relation between NLR and prognosis (OS, CSS, PFS, and DFS). If univariate and multivariate analysis were both reported in the same study, multivariate-adjusted HRs and 95% confidence intervals were used with priority. ORs and 95% CIs were used to evaluate the relation between NLR and clinicopathologic factors. Between-study heterogeneity was assessed by χ2-based Q test and Higgins’ I2 statistic. P-value for Q test was >.10 and I2 was <50%. These suggested that there was no significant heterogeneity and therefore fixed-effects model was used to calculate overall estimate of effect. If there was any heterogeneity, random-effects model would be used instead. Subgroup analysis was used to explore possible heterogeneity. Robustness of data included was tested by sensitivity analysis. Publication bias was assessed by Begg's funnel plot and Egger's linear regression test. Differences were considered statistically significant for P-values <.05. Statistical analysis was conducted with Stata version 14.1 (Stata Corporation). All P-values were two-sided.
Results
Study Characteristics
A total of 154 abstracts were selected in the initial search. After discarding duplicates, 137 abstracts remained, and then 68 articles were excluded after reading the titles and abstracts, as they were views, letters, abstracts, case reports, or nonclinical types. The remaining 69 articles were further reviewed with full texts. After that, 37 studies were excluded as theyfor the following reasons: did not providing provide sufficient data, involved continuous NLR without a clear cutoff point, or were repeated repeated reporteds. Figure 1 showed the detailed screening process. Finally, 32 studies were included in this meta-analysis.13–44 All those studies were retrospective observational cohort studies, all reports were published between 2011 and 2017. The 32 articles involved a total of 8431 patients. Among them, 6569 suffered from squamous cell carcinoma, and 1862 suffered from adenocarcinoma and other malignant tumors. NLR cutoff values in these studies varied, ranging from 1 to 5. Of all those studies, 15 had a cutoff value ≤2.5, and 17 had a value ˃2.5. Detailed information on the selected studies was summarized in Table 1. All the studies had an NOS score ≥7.

Flow diagram of search strategy and study selection.
Main Characteristics of Relevant Studies.

M: HR from multivariate analysis; U: HR from univariate analysis; Mix: mixed treatment with at least two anticancer methods including chemotherapy, surgery, radiotherapy, or chemoradiotherapy; the dashes represent no data.
Abbreviations: CV, cutoff value; HR, hazard ratio; NR, not reported; OS, overall survival; DFS, disease-free survival; PFS, progression-free survival; CSS, cancer-specific survival; SD, standard deviation; TNM, tumor node metastasis; NLR, neutrophil-to-lymphocyte ratio; CRT, chemoradiotherapy; ESCC, esophageal squamous cell carcinoma; EC, esophageal cancer including adenocarcinoma, esophageal squamous cell carcinoma and other types esophageal carcinoma; No, number.
Overall Survival of Esophageal Cancer
21 Studies involving 5630 patients evaluated the association between NLR and OS (Table 2). High pretreatment NLR predicted a poor OS with a pooled HR of 1.57 (95% CI = 1.40-1.75, P < .001, Figure 2). Significant between-study heterogeneity was found (I2 = 42.7%, P = .021) and random-effect model was used.
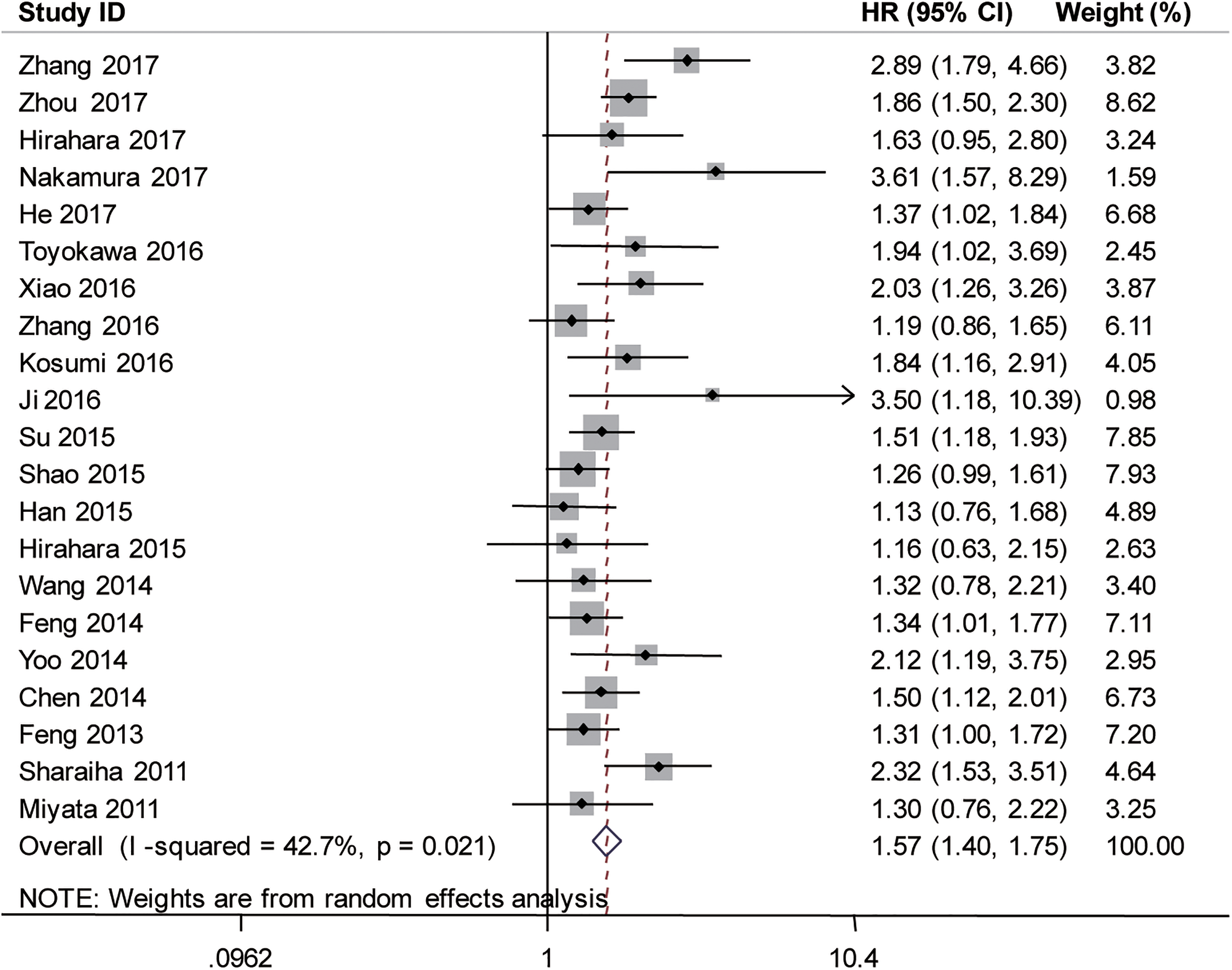
Forest plots of studies evaluating hazard ratios of NLR for OS.
Summary and Subgroup Analysis of the Association Between NLR and Prognosis of EC.

Abbreviations: NLR, neutrophil-to-lymphocyte ratio; EC, esophageal carcinoma including adenocarcinoma, esophageal squamous cell carcinoma and other types esophageal carcinoma; HR, hazard ratio; CI, confidence interval; OS, overall survival; CSS, cancer-specific survival; DFS, disease-free survival; PFS, progression-free survival; Mix: mixed treatment with at least two anticancer methods including chemotherapy, surgery, radiotherapy, or chemoradiotherapy; CRT, chemoradiotherapy; ESCC, esophageal squamous cell carcinoma; CV, cutoff value.
For further investigation, subgroup analysis of OS was performed, and the detailed information was shown in Table 2. Subgroup analysis by country showed that the combined HR was 1.49 (95% CI = 1.31-1.69, P < .001, I2 = 47.2%, Pheterogeneity = 0.030, Figure S1A within Supplemental) for China and 1.68 (95% CI = 1.30-2.17, P < .001, I2 = 14.8%, Pheterogeneity = 0.319) for Japan. Subgroup analysis according to sample size revealed that the combined HR was 1.52 (95% CI = 1.34-1.71, P < .001, I2 = 37.2%, Pheterogeneity = 0.121) for sample size >250 and 1.68 (95% CI = 1.35-2.09, P < .001, I2 = 49.8%, Pheterogeneity = 0.025) for sample size ≤250 (Figure S1B within Supplemental). Subgroup analysis also showed that high NLR was correlated with poor OS for different therapy, different cutoff values, different survival analyses (univariate or multivariate analysis) and different histology (Table 2, Supplemental Figure S1C-S1F).
Because of the significance heterogeneity, sensitivity analysis was done to estimate the influence of each individual study on the overall estimate of effect, and the data proved that the results calculated were reliable and stable (Figure 3A).

Sensitivity analysis (A) and publication bias of Begg's funnel plot (B) and Egger's linear regression test (C) on the relationship between NLR and OS, using Metaninf function in Stata 14.1.
Other Survival Indicators of Esophageal Cancer
The association between NLR and CSS, PFS and DFS were evaluated and shown in Table 2. Patients with elevated NLR was notably correlated with poorer CSS (HR = 1.28, 95% CI = 1.09-1.49, P < .001, Figure S2A), without between-study heterogeneity (I2 = 3.8%, P = .397). Impact of NLR on PFS was also examined. The results revealed that higher NLR was related with poorer PFS (HR = 1.45, 95% CI = 1.29 −1.72, P < .001, Figure S2B), and no significant heterogeneity was found (I2 = 0.0%, P = .464). The meta-analysis also revealed that NLR had prognostic role for DFS of esophageal cancer; the combined HR was 1.58 (95% CI = 1.27-1.97, P < .001, Figure S2C) with high heterogeneity (I2 = 50.2%, P = .074).
Sensitivity analysis was done to evaluate the influence of single study on overall estimate of effect, and the results showed that the pooled HR was reliable (Supplemental Figure S3).
Tumor Length of Esophageal Cancer
Significant association was observed between high NLR and large tumor size (OR = 2.85, 95%CI = 2.32-3.50, P < .001). No statistical heterogeneity was found among these studies (I2 = 37.7%, P = .141, Figure 4A).
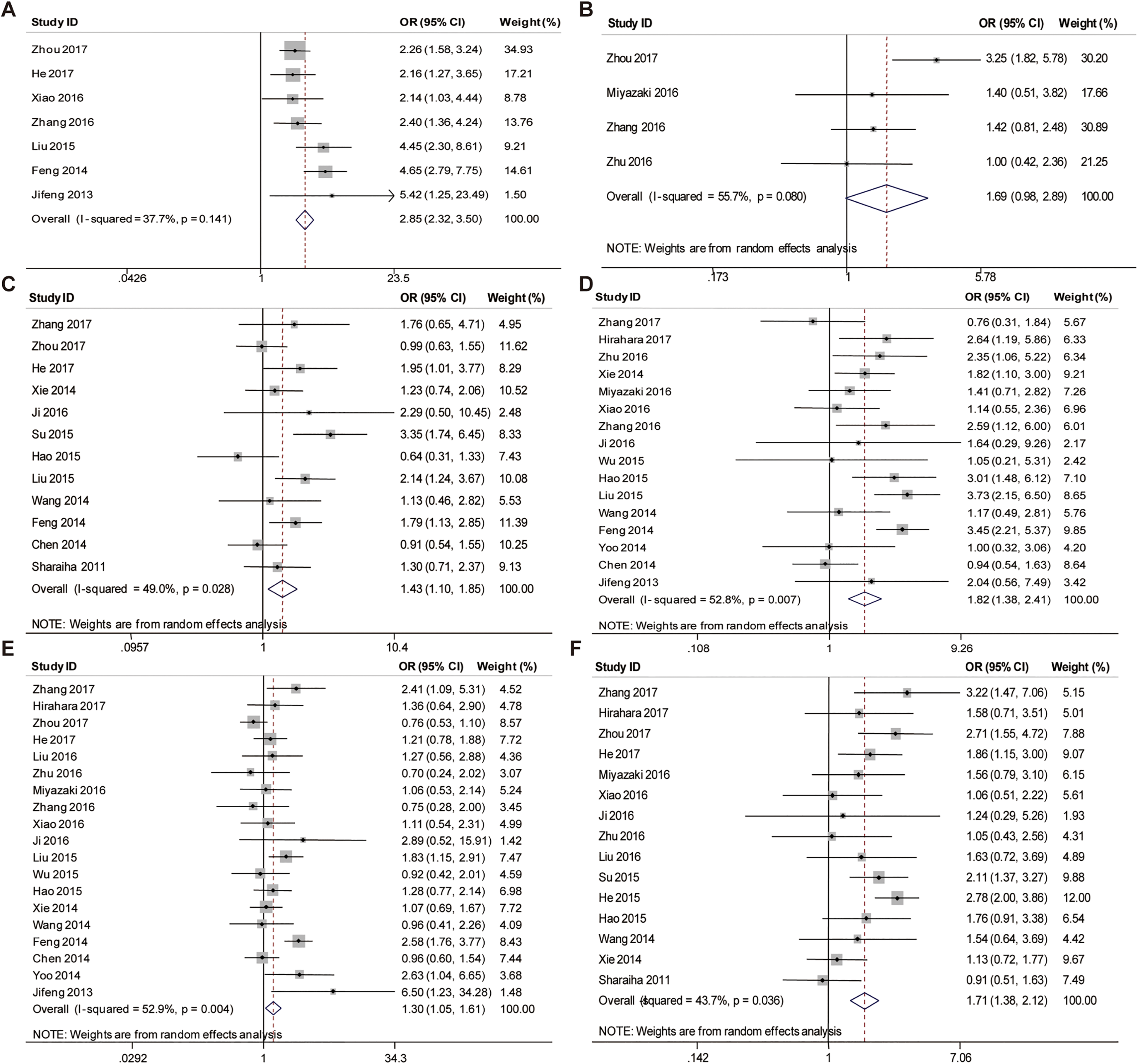
Forest plots of studies evaluating odds ratios of NLR for tumor length (A), metastasis stage (B), tumor differentiation (C), depth of invasion (D), lymph node metastasis (E), and TNM stage (F).
Subgroup analysis by tumor length cutoff value revealed that combined OR was 2.28 (95% CI = 1.72-3.01, P < .0001, I2 = 0.0%, Pheterogeneity = 0.960, Supplemental Figure S4) for tumor length cutoff value of 5, and 3.62 (95% CI = 2.66-4.94, P < .0001, I2 = 43.5%, Pheterogeneity = 0.150, Supplemental Figure S4) for tumor length cutoff value of 3.
Tumor Differentiation of Esophageal Cancer
The associations between NLR and clinicopathologic parameters were shown in Table 3. Pooling data (from 12 studies with 3686 patients) showed that NLR was higher in patients with poor tumor differentiation (OR = 1.43, 95%CI = 1.10-1.85). The random-effects model was adopted to determine the significance of heterogeneity (P = .028, I2 = 49.0%, Figure 4C).
Summary and Subgroup Analysis of the Association Between NLR and Clinicopathologic Features of EC.

Abbreviations: NLR, neutrophil-to-lymphocyte ratio; CV, cutoff value; EC, esophageal carcinoma; OR, odds ratio; CI, confidence interval; TNM, tumor node metastasis.
We next investigated whether heterogeneity resulted from NLR cutoff value. The results suggested that elevated NLR was associated with high tumor differentiation for cases with NLR cutoff value ˃2.5 (OR = 1.41, 95% CI = 1.02-1.95, P = .037, I2 = 48.3%, Pheterogeneity = 0.071, Figure S5A within Supplemental), but not for those with NLR cutoff value ≤2.5 (OR = 1.47, 95% CI = 0.91-2.37, P = .119, I2 = 59.9%, Pheterogeneity = 0.041). Both subgroups showed high heterogeneity. Sensitivity analysis showed that the pooled OR was steady (Supplemental Figure S5B).
Depth of Invasion of Esophageal Cancer
A total of 16 studies were accessed to calculate a pooled OR and 95% CI for depth of invasion of esophageal cancer. As heterogeneity was detected (I2 = 52.8, P = .007), random-effect model was used. Significant associations were observed between high NLR and deeper invasion (T3-T4) (pooled OR = 1.82, 95% CI = 1.38-2.41, P < .001, Figure 4D).
Due to the presence of heterogeneity, we performed stratified analysis by NLR cutoff value. Combined OR was 1.29 (95% CI = 0.94-1.77, P = .111, I2 = 24.2%, Pheterogeneity = 0.244, Supplemental Figure S6A) for NLR cutoff value ≤ 2.5 and 2.73 (95% CI = 2.14-3.49, P < .0001, I2 = 0.0%, Pheterogeneity = 0.445) for NLR cutoff value ˃ 2.5. The results revealed that, NLR was associated with depth of invasion only for NLR cutoff value ˃ 2.5. Significant heterogeneity was not observed in both subgroups. Sensitivity analysis demonstrated that the combined OR was not markedly changed by omitting each study in turn (Supplemental Figure S6B).
Lymph Node Metastasis of Esophageal Cancer
Our pooled results showed that high NLR was associated with advanced lymph node metastasis (N1-N3). The combined OR was 1.30 (95% CI = 1.05-1.61, P = .018, I2 = 52.9%, Pheterogeneity = 0.004, Figure 4E), using a random-effects model.
To explore heterogeneity, subgroup analysis was done by NLR cutoff value, which revealed that the pooled OR was1.22 (95% CI = 0.97-1.55, P = .091, I2 = 2.8%, Pheterogeneity = 0.408, Supplemental Figure S7A) for NLR cutoff value ≤ 2.5 and 1.31 (95% CI = 0.93-1.83, P = .119, I2 = 67.4%, Pheterogeneity = 0.001) for NLR cutoff value ˃2.5. The results implied no significant correlation between lymph node metastasis of esophageal cancer and high- or low-NLR groups. Sensitivity analysis was done to investigate the influence of an individual study on the pooled results. The results indicated that the pooled OR showed no significant change (Supplemental Figure S7B).
Metastasis Stage of Esophageal Cancer
There were only four studies reported the correlation between NLR and metastasis stage of esophageal cancer. The pooled OR was 1.69 (95% CI = 0.98-2.98, P = .058, I2 = 55.7%, Pheterogeneity = 0.08, Figure 4B). This indicated that NLR was not an effective predictor for metastasis stage of esophageal cancer. But as there were only a few studies concerning this topic, sensitivity analysis was not carried out.
TNM Stage of Esophageal Cancer
High NLR was found to be significantly associated with late TNM stage (III-IV) of esophageal cancer (OR = 1.71, 95% CI = 1.38-2.12, P < .0001, Figure 4F) with high heterogeneity among these studies (I2 = 43.7%, P = .036).
Stratified analysis by NLR cutoff value showed that OR was 1.62 (95% CI = 1.21-2.15, P = .001, Supplemental Figure S8A) for NLR cutoff value ≤ 2.5 and 1.76 (95% CI = 1.28-2.41, P < .0001) for NLR cutoff value ˃2.5. Significant heterogeneity was observed in the high-NLR group (I2 = 53.7%, Pheterogeneity = 0.034), not in the low-NLR group (I2 = 25.8%, Pheterogeneity = 0.232).
Meta-sensitivity analysis suggested no undue influence of any single study on the pooled effect (Supplemental Figure S8B).
Publication Bias
Begg's test and Egger's test were used to evaluate publication bias. Visual inspection of Begg's funnel plots and Egger's linear regression tests indicated no significant publication bias in this meta-analysis on relation between NLR and survival indicator and clinicopathologic characteristics (Figure 3B, Figure 3C, and Supplemental Figure S9-S15). P-values for Begg's text and Egger's test also failed to find evidence of publication bias (Supplemental Table S1). It was not necessary to carry out tests of publication bias test was not done on the outcomes of PFS and Metastasis stage, because there were only a few studies concerning these topics.
Discussion
The results of our analysis from 32 studies with 8431 esophageal cancer patients demonstrated that pretreatment NLR was an effective serum marker to predict prognosis and associated with various clinicopathological characteristics, including tumor length, tumor invasion, clinical stage, lymph node metastasis and differentiation, except metastasis stage. In addition, subgroup analyses and sensitivity analyses provided further support for the conclusions.
A number of studies reported that inflammatory responses play crucial roles in tumor development, including initiation, promotion, malignant conversion, invasion, and metastasis.2,6,45,46 Our finding are consistent with those in published reports, but the mechanisms on how elevated NLR causes poor outcomes remain elusive. It was reported that neutrophils may secrete vascular endothelial growth factor to promote tumor angiogenesis, and they can promote cell proliferation, mobility, and migration.37,47–49 On the other side, accumulating data have demonstrated that cancer produce various cytokines, such as circulating vascular endothelial growth factors, TNF-α (tumor necrosis factor-α), TGF-β (transforming growth factor-β), interleukin-1, and interleukin-6, which may contribute to tumor-infiltrating associated neutrophils.49,50 In view of these, pretreatment NLR may not only serve as an indicator to evaluate the level of inflammation response, but also have great potential for prediction of prognosis of patients. Measuring pretreatment NLR could guide clinical decisions for patients with esophageal cancer. Furthermore, NLR test is easy to perform, and the materials are cheap and readily available in oncological practice.
Our study showed that NLR could as an independent predictor of esophageal cancer. In addition, we should not ignore other important factors affecting the prognosis of esophageal cancer. Tumor TNM staging, which is related to doctors' judgment of the disease, guidance of treatment, prognosis estimation and screening of the best treatment plan for tumors of different stages. Other important factors include smoking,51 alcohol consumption,51 tumor length,52 tumor location,52 difficulty in swallowing,53 and genetic mutations.54 To esophagus cancer position, upper esophageal carcinoma patient is the most serious, followed by midpiece esophagus cancer, and lower esophageal cancer patients. The degree of tumor differentiation is also a key factor affecting prognosis. Poor tumor differentiation is associated with poor tumor prognosis. The results of this study showed that high NLR value predicted poor tumor differentiation. This finding is consistent with our results that high NLR values can predict poor outcomes in patients with esophageal cancer. In practice, clinicians are recommended to consider all those factors to make a reliable prediction on prognosis of patients with esophageal cancer.
Previous meta-analysis has reported the relation between NLR and survival of patients with esophageal cancer.7–9 But those studies only enrolled small numbers of patients. To overcome such limitation, Different from previous studies, our research work(a) included rolled large numbers of patient with 8431 patients from 32 studies, and heterogeneity between the studies was minimized. In our work, a comprehensive analysis of the relation between NLR and esophageal cancer was made by analyzing important outcomes of esophageal cancer (CSS, PFS, lymph node metastasis, and metastasis stage). Apart from those, our work also confirmed that there is a relation between NLR and esophageal cancer. Such findings were in line with those of Yang et al..7 But some results of Yodying et al.8 and Huang et al.9 were negated in our work.
This meta-analysis had some limitations, which were intrinsic to the nature of included studies and provide basis for future research. First, most of the enrolled studies were retrospective, published in English, and from Asian countries, making results more susceptible to some bias. Second, the cutoff values of NLR were lack of uniformity, ranged from 2 to 5, which may lead to heterogeneity and influence clinical application of the index, and some subgroup analysis by NLR cutoff value showed that the pooled OR had no statistical significance when NLR cutoff value ≤2.5. Third, there were only four studies reported the correlation between NLR and metastasis stage of esophageal cancer, making their conclusions unreliable. Fourth, NLR-related ratios were affected by some diseases, including inflammation and infection, and certain medications, including antibiotics, which could undoubtedly reduce the prognostic value of NLR. In view of these, the pooled HR and OR should be interpreted with caution. Further meta-analysis on larger sample size and other geographic regions are needed.
In summary, this study revealed that NLR was negatively correlated with prognosis in patients with esophageal cancer (OS, CSS, PFS and DFS). Elevated pretreatment NLR was related to poor differentiation, large tumor size, advanced clinical stage, deep tumor invasion and serious lymph node metastasis. Metastasis stage of esophageal cancer showed nothing to do with NLR, which need more studies and evidence to confirm its reliability. Furthermore, farther research into cancer-related inflammation should be carried out, because it might be helpful for developing better diagnostics and treatments.
Supplemental Material
sj-docx-1-tct-10.1177_15330338211070140 - Supplemental material for Prognostic and Clinicopathologic Significance of Neutrophil-to-Lymphocyte Ratio in Esophageal Cancer: An Update Meta-Analysis
Supplemental material, sj-docx-1-tct-10.1177_15330338211070140 for Prognostic and Clinicopathologic Significance of Neutrophil-to-Lymphocyte Ratio in Esophageal Cancer: An Update Meta-Analysis by Binfeng Li, Fei Xiong, Shengzhong Yi and Sheng Wang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-2-tct-10.1177_15330338211070140 - Supplemental material for Prognostic and Clinicopathologic Significance of Neutrophil-to-Lymphocyte Ratio in Esophageal Cancer: An Update Meta-Analysis
Supplemental material, sj-docx-2-tct-10.1177_15330338211070140 for Prognostic and Clinicopathologic Significance of Neutrophil-to-Lymphocyte Ratio in Esophageal Cancer: An Update Meta-Analysis by Binfeng Li, Fei Xiong, Shengzhong Yi and Sheng Wang in Technology in Cancer Research & Treatment
Footnotes
Acknowledgments
There are no sources of any funding for this study. We thank for all the patients and clinical investigators who are involved in the selected studies in the meta-analysis.
Author Contributions
Binfeng Li and Sheng Wang conceived the study. Fei Xiong and Binfeng Li performed the literature search and collected the data. Binfeng Li drafted the manuscript. Fei Xiong, Shengzhong Yi and Sheng Wang assessed the study quality. Shengzhong Yi and Sheng Wang revised the manuscript and language. All authors approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.