
Abstract
Keywords
Introduction
As a rare tumor of the urinary system, upper tract urothelial carcinoma (UTUC), including renal pelvic cancer and ureteral cancer, accounts for 5% to 10% of all urinary tract epithelial cancers. 1 UTUC has a relatively high degree of malignancy. Approximately 60% of patients are already in the advanced stage at the time of diagnosis, while this proportion is only 15% to 25% among patients with bladder tumors. 2 Although conservative treatment can be used for some patients, radical nephroureterectomy (RNU) with bladder sleeve resection is still the current standard of UTUC treatment. 3 For patients undergoing RNU, the postoperative prognosis is not ideal and is accompanied by a high recurrence rate. 4 Thus, recognizing the influencing factors of prognosis is of great significance for early screening, individualized treatment, and prognostic evaluation of UTUC patients.
The present literature shows that pathologic tumor stage, tumor grade, and lymph node status are good prognostic predictors of UTUC.5,6 However, these factors are all obtained pathologically after surgery, intervention in patients is limited, and the effect is unknown. The current prognostic model based on these factors has low accuracy and limited prognostic value, which limits its clinical application in UTUC patients. 7 Systemic inflammation and the inflammatory microenvironment play an important role in tumor occurrence and development. 8 Recently, some studies reported blood-based inflammation biomarkers, including the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-monocyte ratio (LMR), are associated with the survival time and disease progression of cancer patients.9–11 Actually, most research has focused on the impact of a single biomarker, and much less research has explored the combined effect. Due to the limited number of high-quality studies and relatively small sample sizes, there is no reliable evidence to confirm the predictive value of blood-based inflammation biomarkers in the prognosis of UTUC.
In this study, we aimed to investigate the prognostic significance of preoperative NLR, PLR, and LMR in UTUC patients undergoing RNU and assess the clinical application value of these inflammation biomarkers. Furthermore, we attempted to construct a simple risk classification model based on biomarkers and explore the potential for clinical guidance.
Methods
Patient Selection
This retrospective study was approved by the China-Japan Friendship Hospital Research Ethics Board (2021-40-K24). The requirement for written informed consent from the patients were waived owing to the retrospective study design. We retrospectively included patients diagnosed with UTUC who received RNU treatment at our hospital from 2008 to 2018, all patients details have been de-identified. Patients with missing data, a history of preoperative neoadjuvant radiotherapy and chemotherapy, preoperative local treatment (such as segmental ureterectomy and endoscopic tumor resection or ablation, etc), the presence of other concomitant tumors, combined infections, blood or immune system diseases that have a significant impact on NLR indicators, or a history of bladder tumors and radical bladder surgery before RNU were excluded. A total of 172 patients were analyzed in this study. These patients underwent laparoscopic RNU surgery. Only patients who had preoperative images with suspected lymph node metastasis or enlarged lymph nodes during the operation were treated with local lymph node dissection.
Data Collection
We collected the following clinical and pathological data for the analysis: sex, age, tumor side, tumor location, pathologic tumor stage (pT), lymph node status (pN0, pNx or pN + ), tumor grade, tumor architecture, tumor multifocality, lymphovascular invasion (LVI), surgical margin status, distant metastasis and related laboratory examination parameters. All postoperative tissue samples were sent for pathological examination by senior pathologists. Pathologic tumor stage and grade were evaluated by the 2009 International Union Against Cancer (UICC) TNM classification system 12 and the 2016 World Health Organization (WHO) grading system. 13 NLR, PLR, and LMR was obtained from routine blood examination performed 1 week before surgery. X-tile software (version 3.6.1) was applied to determine the optimal cut-off for inflammation biomarkers classified as low level and high level. 14 The cut-off values of NLR, PLR, and LMR were 2.2, 115.3, and 3.6.
Follow-up
Patients were followed up every 3 months during the first year after surgery, every 6 months through the third year, and once a year thereafter. Follow-up data included blood tests, cystoscopic examination, urinary system ultrasound, chest and abdomen CT, urine exfoliated cytology and urography. If clinically indicated, selective bone scan, PET/CT or magnetic resonance (MRI) examination was performed. Overall survival (OS) was defined as the time from the date of RNU to death from any cause. Cancer-specific survival (CSS) was defined as the time from the date of RNU to the date of cancer-specific mortality. Recurrence-free survival (RFS) was defined as the time from the date of RNU to the date of first recurrence on imaging examination to death from any cause. Metastasis-free survival (MFS) was defined as the time from the date of RNU to the date of tumor metastasis according to imaging examination.
Statistical Analysis
We presented the parameters as the frequency (percentage). Some results are shown as median values with ranges or interquartile ranges (IQRs). Pearson’s chi-square test was used to analyze categorical variables, the Mann–Whitney U test and Kruskal–Wallis H test were used to analyze continuous variables, and nonparametric tests were used to analyze nonnormally distributed variables. The Kaplan–Meier method and log-rank test were used to compare the survival rates among different risk groups. Pearson’s correlation analysis was implemented to assess the correlation between biomarkers. Univariate and multivariate Cox regression analyses models were used to assess prognostic factors related to OS, CSS, RFS, and MFS. These statistical outcomes were 2-sided tests, and P <.05 indicated that the difference was statistically significant. In addition, the receiver operating characteristic (ROC) analyses was performed, and the area under the ROC curve (AUC) and concordance index (C-index) were calculated to evaluate the discrimination ability. We also performed decision curve analysis (DCA) to evaluate the clinical net benefit of prognostic models. All analyses were performed with SPSS (version 24) and R software (version 4.1.2). The figures were generated by MedCalc (version 19.0) and R software (version 4.1.2).
Results
Association of Inflammation Biomarkers with Clinicopathological Variables
A total of 172 patients were ultimately included in this research. Table 1 shows their demographic and clinicopathological characteristics. There were 77 males and 95 females. The median age of the whole cohort was 69 (range: 38-86) years. We divided the group based on the cut-off values of NLR, PLR, and LMR. Table 2 summarizes the association of inflammation biomarkers and clinicopathologic characteristics of the cohort. No significant differences were observed in terms of age, tumor location, lymph node status, tumor architecture, or tumor multifocality among the subgroups of 3 biomarkers (all P > .05). Patients with an elevated NLR had higher rates of a higher pathologic tumor stage (pT3-4), high-grade tumor, positive surgical margin status, and LVI (all P <.05). In addition, obvious differences were found in the PLR groups regarding distant metastasis, tumor side and grade (all P <.05). In contrast, the results showed that patients with a low LMR had a higher rate of pT3-4 (all P <.05).
Demographic and Clinicopathological Characteristics of 172 Patients With UTUC.

Abbreviations: NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-monocyte ratio; CIS, carcinoma in situ; LVI, lymphovascular invasion.
Association of Inflammation Biomarkers and Clinicopathologic Characteristics in 172 Patients With UTUC.

Abbreviations: NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-monocyte ratio; CIS, carcinoma in situ; LVI, lymphovascular invasion.
*P < .05.
Survival Analyses Based on Preoperative Inflammation Biomarkers
The median follow-up was 45.5 (range: 1-143; IQR: 27-77) months. During the follow-up period, 57 patients (33.1%, 57/172) died, of whom 45 patients (26.2%, 45/172) died from UTUC, and 12 patients (6.9%, 12/172) died from all causes. The 5-year OS, CSS, RFS, and MFS were 66.5%, 72.5%, 47.7%, and 72.9%, respectively. We generated Kaplan–Meier curves to reveal the survival outcomes of the different groups. The results demonstrated that patients with a high NLR have a worse OS, CSS, RFS, and MFS. Similarly, an elevated PLR significantly decreased OS, CSS, RFS, and MFS. However, the curves show that MLR has no obvious effect on OS and CSS but significantly affects RFS and MFS (Figures 1 to 3).

Kaplan–Meier curves for OS (A), CSS (B), RFS (C), and MFS (D) of patients with UTUC according to NLR.
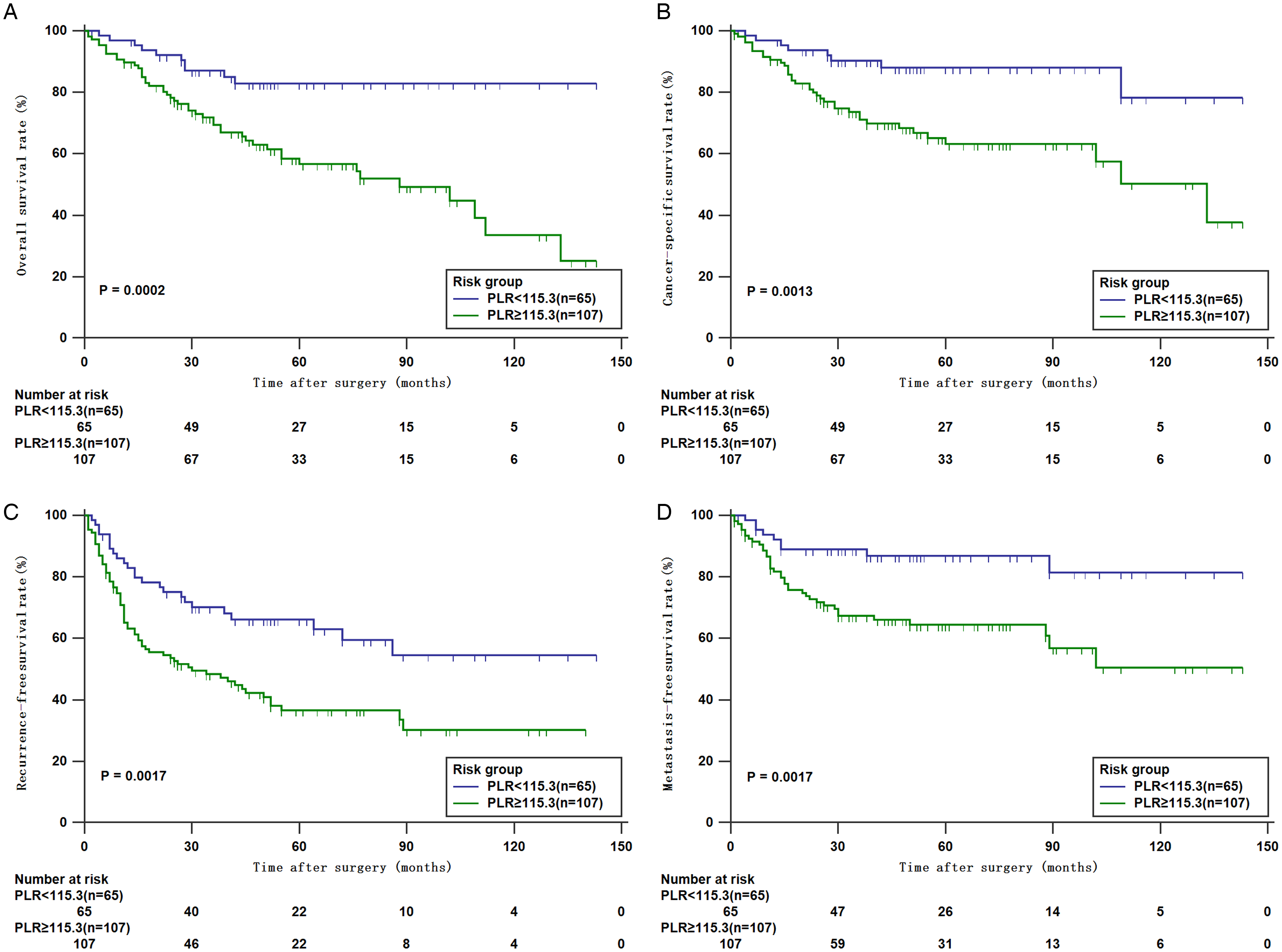
Kaplan–Meier curves for OS (A), CSS (B), RFS (C), and MFS (D) of patients with UTUC according to PLR.
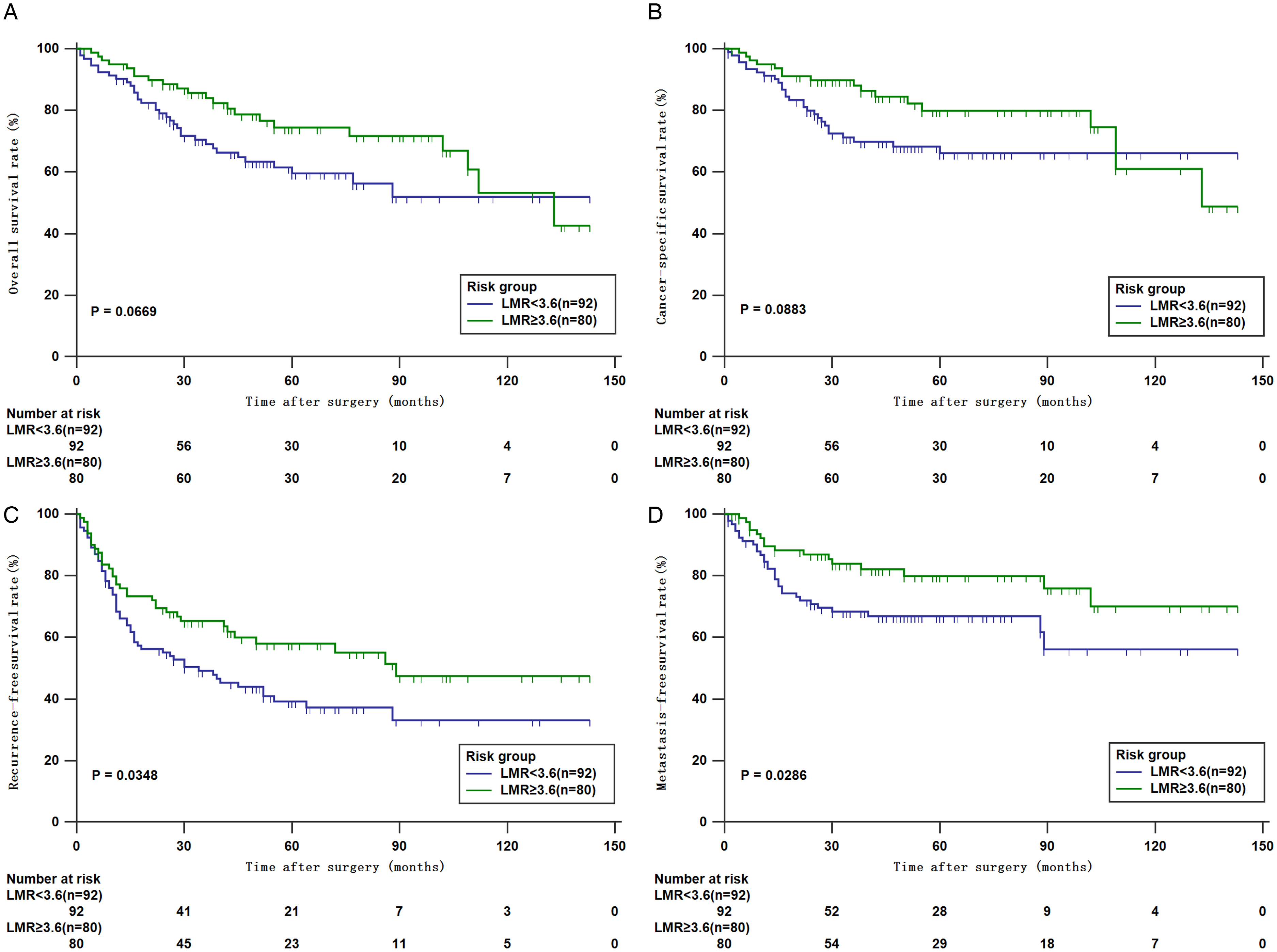
Kaplan–Meier curves for OS (A), CSS (B), RFS (C), and MFS (D) of patients with UTUC according to LMR.
Prognostic Significance of NLR and PLR
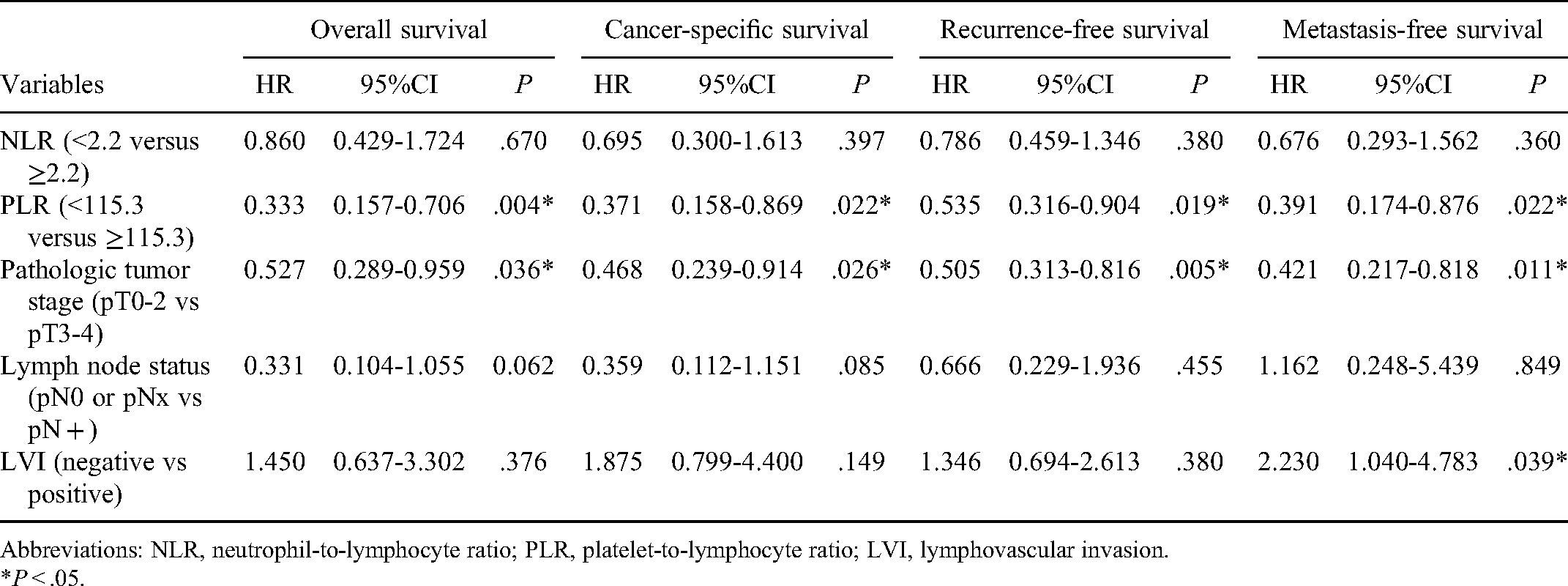
According to the univariate Cox analysis, the high NLR and PLR group had worse OS, CSS, RFS, and MFS. Pathologic tumor stage, lymph node status, and LVI also showed a strong relationship with oncological outcomes in the univariate analysis (all P <.05) (Table 3). After including these relative factors, multivariate Cox analysis demonstrated that PLR was an independent clinical risk predictor for survival outcome, but NLR had no significant effect (P <.05) (Table 4).
Univariate Cox Regression Analyses Predicting Survival Outcome of Patients With UTUC.

Abbreviations: NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-monocyte ratio; LVI, lymphovascular invasion.
*P < .05.
Multivariable Cox Regression Analyses Predicting Survival Outcome of Patients With UTUC.
Abbreviations: NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LVI, lymphovascular invasion.
*P < .05.
Impact of the Combined use of NLR and PLR on Preoperative Risk Classification
The results of the correlation analysis showed that NLR was positively correlated with PLR (Supplemental Figure S1) (r = 0.633, P < .0001). Combining the analysis results, we developed a preoperative risk classification model based on the preoperative NLR and PLR. The high-risk group was defined with both high NLR and PLR. Those with either a high NLR or PLR were included in the intermediate-risk group. The low-risk group included patients with neither elevated NLR nor PLR. The Kaplan–Meier curves revealed a significant difference in OS, CSS, RFS, and MFS among the 3 groups (Figure 4). When including risk classification grade in univariate and multivariate Cox analyses, the results were significantly associated with all survival outcomes (Supplemental Table S1).

Kaplan–Meier curves for OS (A), CSS (B), RFS (C), and MFS (D) of patients with UTUC according to preoperative risk classification.
The Performance of the Prediction Model With the Addition of NLR and PLR
To verify whether the addition of NLR and PLR will improve the accuracy of the basal prediction model (pT, pN, LVI, tumor location, and architecture) on clinicopathological features. The new prediction model was defined as the basal model with the addition of NLR and PLR. We compared the new prediction model to the basal model by performing time-dependent ROC curve (Figures 5 and 6). The results revealed that the new model marginally improved its predictive accuracy for all 3-year and 5-year OS, CSS, RFS, and MFS compared with the basal model (Table 5). Moreover, we tested the C-index for the model of OS, CSS, RFS, and MFS before and after inclusion of NLR and PLR, and the C-index for 1- to 5-year increased obviously when including the NLR and PLR (Figure 7). Accordingly, the results of the relative analysis showed that the combination of NLR and PLR represented a more accurate prognostic ability and efficient potential for the discrimination of survival rates in patients with UTUC. In Figures 8 and 9, the DCA revealed that the net benefit of new model was better than that of the basal models for all 3-year and 5-year OS, CSS, RFS, and MFS. Consequently, prognostic models with NLR and PLR can improve the net clinical benefit for predicting survival probabilities.

ROC curves predicting 3-year OS (A), CSS (B), RFS (C), and MFS (D) of patients with UTUC according to prognostic models.

ROC curves predicting 5-year OS (A), CSS (B), RFS (C), and MFS (D) of patients with UTUC according to prognostic models.

C-index evaluating prognostic performance of OS (A), CSS (B), RFS (C), and MFS (D) of patients with UTUC according to prognostic models.
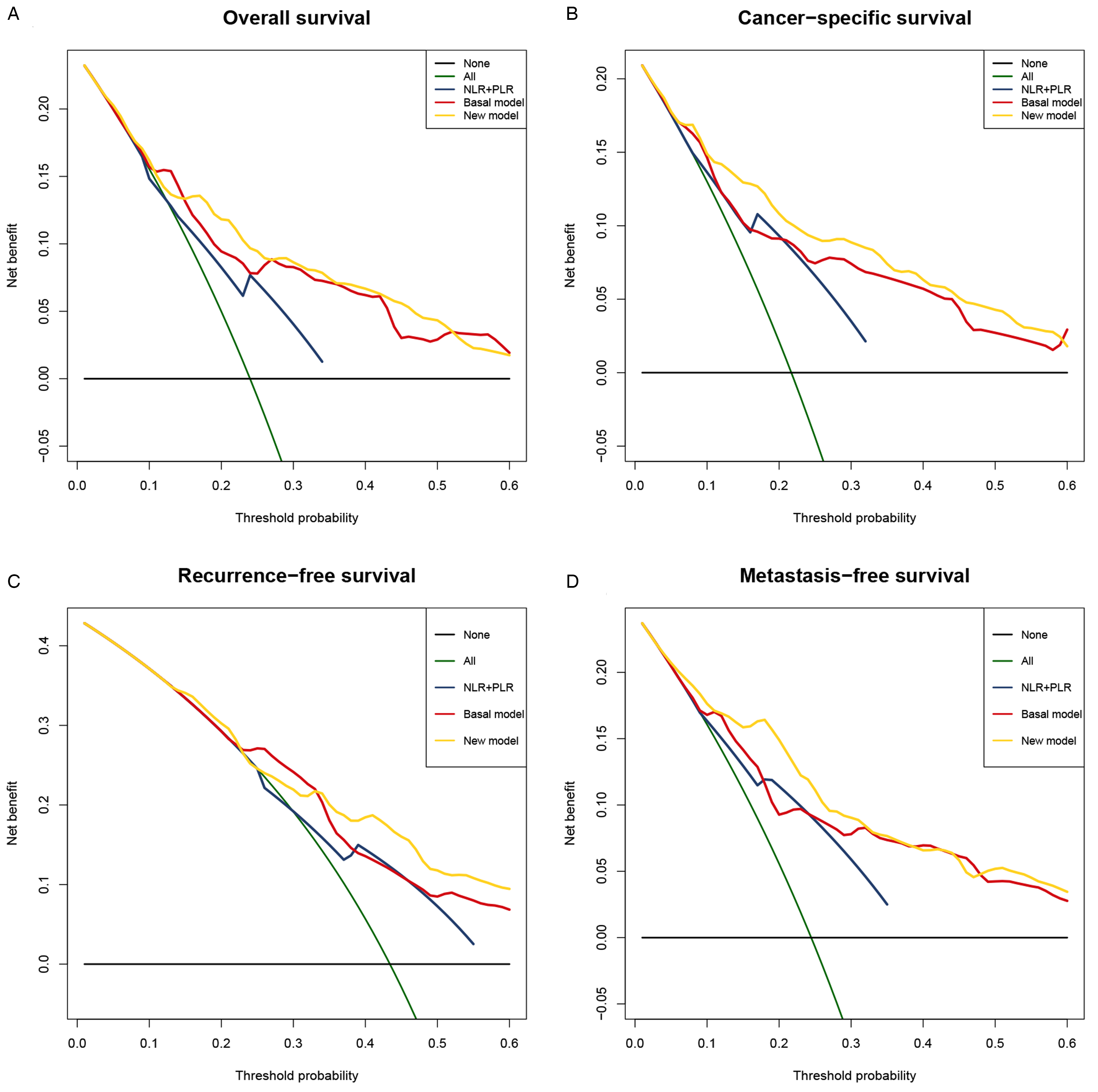
Decision curve analyses comparing the added benefit of NLR and PLR for 3-year OS (A), CSS (B), RFS (C), and MFS (D) of patients with UTUC.

Decision curve analyses comparing the added benefit of NLR and PLR for 5-year OS (A), CSS (B), RFS (C), and MFS (D) of patients with UTUC.
Time-dependent ROC Analysis of the Prognostic Accuracy of NLR Plus PLR for Survival Outcome in the Overall Cohort.

Abbreviations: ROC, receiver operating characteristic; AUC, area under the curve; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio.
Discussion
In the present study, a cohort of 172 patients who underwent RNU were retrospectively analyzed. The results demonstrated that a high NLR and PLR were significantly associated with poor OS, CSS, RFS, and MFS in univariate analyses. However, the same result was not observed in the OS and CSS of LMR group. The high NLR represented a high predictive potential for survival outcomes. Interestingly, when the PLR was incorporated in multivariate analyses, the NLR failed to predict survival outcomes, but a high PLR was proven to be an independent predictor for worse survival outcomes. Zheng et al 15 reported a similar result; PLR was considered a significant risk factor for OS, but NLR had no contribution to survival outcome. In contrast, a recent meta-analysis with a large sample size concluded that an elevated NLR could significantly decrease survival rates. 16 Considering the different findings described in previous literature, we further analyzed the data and inferred the different risk classification grades based on NLR and PLR as the impact factors. As expected, the results from univariate and multivariate analyses validated that risk classification is an independent prognostic factor for patients with UTUC. The NLR combined with PLR has the largest AUC than NLR or PLR alone, which hinted that this index can improve the prognostic accuracy in patients with UTUC. Therefore, compared to a single biomarker, the combined use of biomarkers can reflect the optimal diagnostic value.
Some studies have shown that the tumor grade and pathological stage of UTUC are the most powerful indicators of prognosis.17,18 There are some other tumor-related factors, such as LVI, tumor necrosis, and carcinoma in situ, which can also be used as independent factors to predict the prognosis of UTUC. 19 In our study, the results revealed that the tumor pathological stage was associated with OS, CSS, RFS, and MFS. However, lymph node status and tumor grade had no effect on the prognosis outcome. Due to the small sample size in this study, there were fewer patients with pT4 stage disease, only 6 patients showed pN + status. Besides, we divided the patients into 2 groups (pT0-2 vs pT3-4) for better performance in the analysis, which may also have led to the difference. Factors such as specimen staining, accurate diagnosis of LVI, and patient selection bias do not support LVI as independent prognostic factors for survival outcome besides MFS in the present study. On the other hand, we hypothesize that the difference may be related to the race of the included population. Compared with patients in Western countries, the Chinese population is quite different in terms of race, ethnicity, eating habits, lifestyle choices, and common exposure to carcinogenic factors, especially aristolochic acid.20,21 Therefore, the pathological characteristics and prognostic indicators of UTUC in the Chinese population should also be different. Population characteristics should be taken into consideration when explaining these research results.
As the seventh hallmark of cancer, 22 cancer-related inflammation has recently been extensively researched with increasing appreciation. Chronic inflammation stimulates tumor growth in 2 ways: one is that external stimuli can promote malignant tumors, and the second is the activation of proto-oncogenes related to inflammation to maintain tumor growth. 23 In tumor tissues, malignant tumor cells grow in a microenvironment similar to that of chronic inflammation. In addition to tumor cells, they also include white blood cells, lymphocytes, macrophages, and some cytokines and chemical factors as mediators, thus reflecting a sustained period of inflammation. 24 Some systemic inflammation-based factors, including NLR, PLR, LMR, and albumin (ALB), have been considered potential markers for prognosis in multiple malignant tumors, including UTUC.9,25–27 In this study, the potential predictive value was observed in NLR and PLR for patients with UTUC. NLR is an indicator of systemic inflammation, and the occurrence and development of tumors are related to systemic inflammation. The enzymatic reaction caused by neutrophils helps tumor cells migrate into the extracellular space and the blood vessel wall, which is an important process for tumor metastasis and development. 28 In addition, an elevated NLR may indicate a decrease in lymphocytes, which have been shown to inhibit tumor growth under certain conditions. 29 Thus, the NLR represents the dynamic balance of the body’s inflammatory response between processes promoting tumor development and inhibiting tumor development. An increase in the NLR indicates that the inflammatory response has shifted toward promoting tumor development, indicating that the patient’s prognosis is poor. The exact mechanism by which PLR has prognostic value in tumor patients is still unclear, and the underlying mechanism of action may be related to the function of platelets and lymphocytes. Platelets are generally considered to be one of the key parts in the process of physiological hemostasis. However, studies have confirmed that platelets can not only promote the immune escape of tumor cells but also release cytokines, including prostaglandin E2 (PGE2) and platelet-derived growth factors, to promote the epithelial-mesenchymal transition (EMT) of tumor cells, and EMT is considered to be one of the key parts in the process of tumor metastasis.30,31 In addition, tumor cells induce platelet activation by secreting platelet agonists, including thromboxane A2 (TXA2), and activated platelets, as participants in the inflammatory response, can promote the immune escape of tumor cells and improve the survival rate of tumor cells by covering tumor cells, further promoting the growth and development of tumors. 32 Therefore, the increase in PLR not only represents a stronger inflammatory response in patients with malignant tumors but also reflects impaired cell-mediated immune function. Accordingly, combining the 2 inflammation biomarkers increases the predictive value for patients with UTUC. Some similar combinations, PLR-LMR, NLR-ALB, and fibrinogen level-PLR, have been described in recent study.33–35 To our knowledge, the present study is the first proposal to confirm that the combined preoperative NLR and PLR possess predictive value among UTUC patients.
The subgroup of inflammation biomarkers was divided depending on the cut-off value. Most studies selected the cut-off value of NLR from 2 to 5 and PLR from 120 to 200. 16 However, the cut-off value in our study was lower than that reported in previous research. Due to the differences in the study design, patient selection and ethnic diversity, there are no consensus on the best cut-off values for inflammation biomarkers. In our study, we used X-tile software, which has been cited in numerous studies, to determine the optimal cut-off values. We also performed time-dependent ROC curve analysis, revealing that the cut-off set was suitable during both short- and long-term periods. Although the NLR has been suggested as a prognostic factor for CSS in UTUC according to the EAU guidelines, 2 it has not been considered a risk factor due to the low level of evidence. The same is true for PLR, which also lacks strict and precise conclusions. Due to the complexity of the tumor microenvironment and cancer-related inflammation, the single biomarker may not truly reflect the situation of tumor development. Thus, the appropriate combination biomarker may improve the prognostic accuracy. Undoubtedly, further investigations with large samples are required to make reliable conclusions.
For patients with high-risk UTUC, RNU is the first choice. In contrast to other studies that included patients undergoing open nephroureterectomy (ONU),34,35 the patients included in the present study all underwent laparoscopic nephroureterectomy (LNU). Compared to ONU, LNU has some advantages, namely, less bleeding, less trauma, quick recovery after surgery, and fewer complications. However, no consensus exists on the survival differences between these 2 surgical approaches. 36 In addition, routine lymph node dissection for UTUC patients is not strongly recommended in the guidelines, 2 and only some patients with exact indications were included in our study. For patients with pT2-4 disease, lymphadenectomy can significantly improve the survival rate. 37 Some patients with worse pathological features receive adjuvant chemotherapy. There is no doubt that these factors contribute to potential bias in the results. Therefore, more studies with strict standards are needed to obtain more reliable findings regarding patient outcomes.
Although the pathological stage of UTUC can predict clinical prognosis, it is dependent on the pathological specimen after surgery and is difficult to grade accurately. Moreover, RNU will cause nephron loss, and patients with high-risk UTUC may have difficulty with cisplatin-based adjuvant chemotherapy after surgery and miss the chance to receive neoadjuvant chemotherapy before surgery. Therefore, the patient’s postoperative treatment and survival outcomes can be affected. As blood-based inflammation biomarkers, the NLR and PLR can be conveniently obtained before surgery, and appropriate risk stratification of patients can guide further treatment. A preoperative risk classification model using NLR and PLR will be helpful for developing personalized treatment options and follow-up plans for UTUC patients. For patients with low-risk UTUC, nephron-sparing surgery can be used as the main treatment option to protect the patient’s renal function and avoid complications caused by radical surgery. Lymph node dissection and bladder infusion chemotherapy on the basis of RNU can avoid tumor recurrence and improve prognosis for patients with high-risk UTUC to the maximum extent.
There are several limitations to the present study that should be acknowledged. First, this was a retrospective study with a limited sample size on the basis of our strict inclusion criteria; therefore, power calculation was not performed in our study and selection bias was unavoidable. In addition, the time span was relatively long, and the relative standards of blood tests, urine exfoliated cytology, and pathological examination standards may have changed during this period, further affecting the reliability of the collected data. Moreover, due to the single center with limited small sample sizes, the validation cohort was not contrasted. For this reason, external validation in a future prospective study is warranted. Finally, some subjective factors, including surgical details and patient features, should be taken into consideration when discussing these results.
Conclusion
Our study suggested that the combination of preoperative NLR and PLR was an independent prognostic factor for UTUC patients after RNU. The addition of NLR and PLR will improve the accuracy of current prognostic models and help guide clinical strategies in the treatment of UTUC. These biomarkers may be recommended as routine references for urologists in the management of UTUC. We hope that the findings of this study will be confirmed by further external validation and prospective multicenter trials.
Supplemental Material
sj-tif-1-tct-10.1177_15330338221095667 - Supplemental material for What is the Role of the Preoperative Blood-Based Inflammation Biomarkers in the Prognosis of Upper Tract Urothelial Carcinoma With Radical Nephroureterectomy? A Single-Centre Retrospective Study
Supplemental material, sj-tif-1-tct-10.1177_15330338221095667 for What is the Role of the Preoperative Blood-Based Inflammation Biomarkers in the Prognosis of Upper Tract Urothelial Carcinoma With Radical Nephroureterectomy? A Single-Centre Retrospective Study by Zhenkai Luo, Binbin Jiao, Tao Huang, Hang Zhao and Guan Zhang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-2-tct-10.1177_15330338221095667 - Supplemental material for What is the Role of the Preoperative Blood-Based Inflammation Biomarkers in the Prognosis of Upper Tract Urothelial Carcinoma With Radical Nephroureterectomy? A Single-Centre Retrospective Study
Supplemental material, sj-docx-2-tct-10.1177_15330338221095667 for What is the Role of the Preoperative Blood-Based Inflammation Biomarkers in the Prognosis of Upper Tract Urothelial Carcinoma With Radical Nephroureterectomy? A Single-Centre Retrospective Study by Zhenkai Luo, Binbin Jiao, Tao Huang, Hang Zhao and Guan Zhang in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-monocyte ratio; UTUC, upper tract urothelial carcinoma; RNU, radical nephroureterectomy; AUC, area under the curve; C-index, concordance index; DCA, decision curve analysis; IQR, interquartile range; OS, overall survival; CSS, cancer-specific survival; RFS, recurrence-free survival; MFS, metastasis-free survival; LVI, lymphovascular invasion; UICC, International Union Against Cancer; WHO, World Health Organization; MRI, magnetic resonance; ROC, receiver operating characteristic; ALB, albumin; PGE2, prostaglandin E2; PDGF, platelet-derived growth factors; EMT, epithelial-mesenchymal transition; TXA2, thromboxane A2; ONU, open nephroureterectomy; LNU, laparoscopic nephroureterectomy.
Author Contributions
Study design: Guan Zhang, Zhenkai Luo, Binbin Jiao; data collection: Zhenkai Luo, Binbin Jiao, Hang Zhao; data analysis and interpretation: Zhenkai Luo, Binbin Jiao, Tao Huang; manuscript writing: Zhenkai Luo, Binbin Jiao.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Ethics
This retrospective study was approved by the China-Japan Friendship Hospital Research Ethics Board (2021-40-K24) on February 24, 2021. A formal consent is not applicable for this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.