
Abstract
Objective:
The aim of the study was to investigate the prognostic role of neutrophil to lymphocyte ratio in ovarian cancer. Growing number of articles reported the relationship between neutrophil to lymphocyte ratio and prognosis in ovarian cancer, but the results remains inconclusive. The meta-analysis was conducted to analyze the association of pretreatment neutrophil to lymphocyte ratio with overall survival and progression-free survival.
Methods:
We performed a systematic literature research of PubMed, EMBASE, Medline, and Cochrane library for relevant studies up to October 8, 2017. The quality of included studies was assessed by the Newcastle-Ottawa Quality Assessment Scale. The hazard ratio and corresponding 95% confidence intervals were calculated. We checked the heterogeneity by the Q test and Higgins I-squared statistic. Begg funnel plot and Egger linear regression test were also applied for ascertain publication bias. All of the statistical analyses were performed using STATA version 12.0.
Results:
A total of 12 studies with 4046 patients were included in our study. The results indicated that depressed neutrophil to lymphocyte ratio was significantly correlated with higher overall survival (hazard ratio = 1.409, 95% confidence intervals = 1.112-1.786, P = .005) and progression-free survival (hazard ratio = 1.523, 95% confidence intervals = 1.187-1.955, P = .001) in ovarian cancer. Subgroup analysis by ethnicity of overall survival and progression-free survival showed that the prognostic effect of neutrophil to lymphocyte ratio was found both in Asians and Caucasians.
Conclusion:
Patients with depressed neutrophil to lymphocyte ratio had a higher overall survival and progression-free survival in ovarian cancer. This meta-analysis provided neutrophil to lymphocyte ratio as an available predictor of overall survival and progression-free survival for patients with ovarian cancer.
Keywords
Introduction
As the most lethal gynecologic malignancy, ovarian cancer is the seventh leading cause of cancer death in women worldwide. 1 Ovarian cancer accounted for 14 080 deaths in United States alone in 2017. 2 The early diagnosis of ovarian cancer is difficult because of insidious onset. Sixty percent of patients are diagnosed at the distant stage with survival of only 29%. 2 In addition to the high-mortality rate, the recurrence rate of ovarian cancer is as high as 80%. 3 Thus, it is imperative to run some tests to predict prognosis.
Prognostic variables in ovarian cancer include age at diagnosis, International Federation of Obstetricians and Gynecologists (FIGO) tumor stage, histological type, tumor grade, and presence of residual disease after initial surgery. 4 Ovarian cancer’s gene detection is also a way to predict the prognosis, including BRCA1, BRCA2, CYP1B1, ARID1A, and p53, but it is expensive and time consuming. 5 -9
Systemic inflammation is associated with tumor progression.
10
Recent epidemiological investigations showed that chronic inflammation, including infection, is involved in 15% and 20% of all human malignancies.
11
Inflammation activity is an important risk factor for the prognosis of patients with cancer. The state of inflammation can be reflected by the corresponding biological indicators such as CA-125, soluble cytokeratin, serum human kallikreins, serum cytokines, serum vascular endothelial growth factor, plasma
Materials and Methods
Search Strategy
We conducted a systematic literature retrieval on PubMed, EMBASE, Medline, and Cochrane library for relevant studies up to October 8, 2017. The following search terms were used: (“neutrophil to lymphocyte ratio” OR “neutrophil-to-lymphocyte ratio” OR “neutrophil-lymphocyte ratio” OR NLR) AND (“ovarian cancer” OR “ovary cancer” OR “ovarian tumor” OR “ovary tumor”). Besides, references listed in the retrieved articles were reviewed to trace additional relevant studies missed by the search.
Inclusion and Exclusion Criteria
All articles were identified independently by 2 investigators. Included studies satisfied all of the following criteria: (1) studies in ovarian cancer reporting the prognostic value of the peripheral blood NLR; (2) studies investigated correlation of pretreatment NLR with overall survival (OS) or progression-free survival (PFS); and (3) sufficient data to estimate hazard ratio (HR) with 95% confidence interval (95% CI). Excluded studies met any of the following criteria: (1) overlapping or duplicate publications; (2) abstracts, reviews, letters, case reports, case series, editorials, and commentaries; (3) non-English articles; (4) nonhuman research; (5) unpublished trials; (6) insufficient data to assess HR with 95% CI; and (7) without full text.
Data Extraction
Data were extracted independently by 2 investigators. For each study, the following characteristics were collected: first author, publication year, study type, country of the study, sample size, age, FIGO stage, treatment, cutoff value, survival analysis data including OS and PFS, duration, and follow-up time.
Quality Assessment of Primary Studies
The quality of included studies was assessed by 2 reviewers independently using the Newcastle-Ottawa Quality Assessment Scale (NOS). 19 Newcastle-Ottawa Quality Assessment Scale scores of ≥6 were considered to be of high quality. Discrepancies were resolved by consensus after discussion.
Statistical Analysis
We assessed the relationship between NLR and prognosis (OS and PFS) using pooled HR and 95% CIs based on methods of Parmer et al 20 The significance of the pooled HRs was determined using a Z test, and the level of statistical significance was established as P < .05. The heterogeneity among studies was checked by the Q test and Higgins I-squared statistic. 21,22 If the P value for the heterogeneity test was >.05, we performed the Mantel-Haenszel method-based fixed effects model to calculate the pooled HR. 23 Otherwise, the DerSimonian and Laird method-based random effects model was performed. 24 An Egger linear regression test was also applied (P < .05 was considered a significant publication bias). 25 All of the statistical analyses were carried out using a software program, STATA version 12.0 (Stata, College Station, Texas).
Results
Extraction Process and Study Characteristics
A total of 190 full-text articles were identified according to the search strategy. Our initial search and the process of study selection are summarized in Figure 1. Eventually, 12 studies 26 -37 published from 2009 to 2017 were included in our meta-analysis, containing 4046 patients. The main characteristics of included studies are shown in Table 1.

Flow diagram of the included studies.
Characteristics of Included Studies.

Abbreviations: CRT, chemoradiation therapy; FIGO, International Federation of Obstetricians and Gynecologists; m, months; NOS, Newcastle-Ottawa Quality Assessment Scale; NR, not reported; OS, overall survival; PFS, progression-free survival; S, surgery.
a Cases in this study were enrolled from 2 protocols—one that recruits patients before surgery for a pelvic mass and a second after a diagnosis of cancer has already been made.
Neutrophil to Lymphocyte Ratio and OS in Ovarian Cancer
There were 12 cohorts presenting the data of pretreatment NLR and OS in ovarian cancer. Our results revealed that patients with depressed NLR were expected to have higher OS after treatment (HR = 1.409, 95% CI = 1.112-1.786, P = .005; Figure 2). Subgroup analysis showed that the prognostic effect of NLR for OS was found both in Asian population (HR = 1.807, 95% CI = 1.084-3.014, P = .023) and in Caucasians (HR = 1.205, 95% CI = 1.014-1.432, P = .035). Remarkable heterogeneity (Ph = 0.000, I2 = 81.3%) was observed in the overall study. After subgroup analysis, we determined that Asian studies contribute to substantial heterogeneity because heterogeneity was significantly decreased in Caucasian (Ph = 0.066, I2 = 58.3%) but not in Asian (Ph = 0.000, I2 = 84.6%). The test of Galbraith Plot showed that the studies by Wang et al 29 and Kim et al 37 could contribute to substantial heterogeneity. The results also reminded us that ethnicity may be one of the reasons for significant heterogeneity.

Forest plots of studies evaluating HR with 95% CI of NLR for OS in subgroup analysis by ethnicity. The center of each square represents the HR, the area of the square is the number of sample and thus the weight used in the meta-analysis, and the horizontal line indicates the 95% CI. CI indicates confidence interval; HR, hazard ratio; NLR, neutrophil to lymphocyte ratio; OS, overall survival.
Neutrophil to Lymphocyte Ratio and PFS in Ovarian Cancer
Three cohorts presented the data of pretreatment NLR and PFS in ovarian cancer. The pooled HR demonstrated a significant association between depressed pretreatment NLR and higher PFS after treatment (HR = 1.523, 95% CI = 1.187-1.955, P = .001; Figure 3) with significant heterogeneity (P = .000, I2 = 78.8%). Subgroup analysis showed that the combined HR was 1.628 (95% CI = 1.160-2.284, P = .005) in Asian population, with significant heterogeneity (P = .000, I2 = 79.4%). With only 1 study included in Caucasian subgroup, there was no need to combine HRs and assess heterogeneity in this group. The test of Galbraith Plot indicated that the study by Wang et al 29 and Kim et al 37 could contribute to substantial heterogeneity.
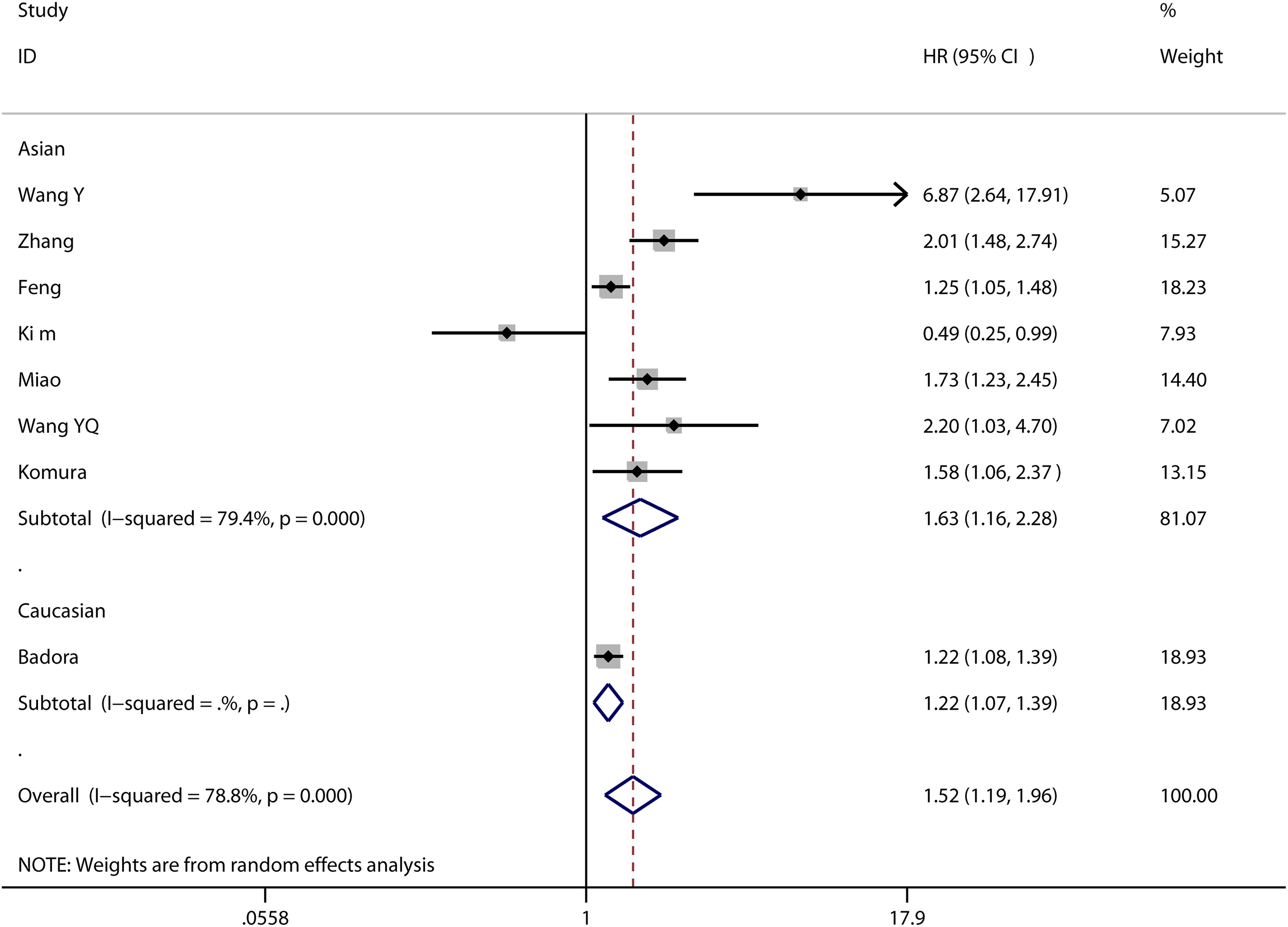
Forest plots of studies evaluating HR with 95% CI of NLR for PFS in subgroup analysis by ethnicity. The center of each square represents the HR, the area of the square is the number of sample and thus the weight used in the meta-analysis, and the horizontal line indicates the 95%CI. CI indicates confidence interval; HR, hazard ratio; NLR, neutrophil to lymphocyte ratio; OS, overall survival; PFS, progression-free survival.
Sensitivity Analyses
Sensitivity analyses were performed to assess the influence of each individual study on the pooled HRs. A single study involved in the pooled meta-analysis was excluded each round of analysis, and the corresponding HRs were not changed considerably, suggesting that the results of this meta-analysis are credible (data also not shown).
Publication Bias
Begg funnel plot (Figures 4 and 5) and Egger test were performed to assess the publication bias of the included studies. Funnel plot shapes did not reveal any obvious evidence of asymmetry. The P value for Egger test in the NLR and OS was .161, respectively. The P value for Egger test in the NLR and PFS was .230. Thus, the results above suggest that publication bias was not evident in this meta-analysis.

Begg funnel plot of potential publication bias for OS. OS indicates overall survival.

Begg funnel plot of potential publication bias for PFS. PFS indicates progression-free survival.
Discussion
Inflammation plays a crucial role in the occurrence and development of cancer, providing a favorable microenvironment for tumor initiation, invasion, and metastasis. 10,38,39 Inflammatory cells and cytokines promote tumor development by facilitating cancer cells’ proliferation, angiogenesis, and apoptosis inhibition, and in turn the tumor-induced inflammation creates a “snowball” effect. 40,41 Inflammation infiltration can be evaluated by performing laboratory examinations. As one of representative inflammatory parameters, NLR is a promising index to predict the prognosis of cancer. Neutrophil to lymphocyte ratio is accessed easily from peripheral blood test results and relatively inexpensive. A growing number of studies show the correlation between high pretreatment NLR and poor prognosis in different cancer types. 42 -46
This study aimed at exploring the prognostic significance of pretreatment NLR in ovarian cancer, including 12 studies with 4046 patients. According to the results, we found that patients with depressed NLR had higher OS and PFS although with heterogeneity. Both in Asian and in Caucasian population, the prognostic effect of NLR is dependable. The results indicated that reduced NLR predicted good prognosis in ovarian cancer, in accordance with meta analyses of pretreatment NLR and other cancer types. Sufficient ovarian cancer types were included. Sensitivity analyses and publication bias showed that our results were credible. Therefore, NLR is a reliable and satisfactory indicator to predict prognosis of patients with ovarian cancer. Neutrophil to lymphocyte ratio assessing is an ideal prognostic test of ovarian cancer, which is widely available in all hospitals and saves money for patients.
We checked out sources through subgroup analysis and Galbraith Plot test. Subgroup analysis indicated that heterogeneity of OS significantly decreased in Caucasian but not in Asian, which meant the Asian studies were the primary cause of heterogeneity. The Galbraith Plot test revealed that the studies of Wang et al and Kim et al contribute to substantial heterogeneity, which are both Asian studies. It also reminds us that ethnicity may be one of the reason for heterogeneity. As for PFS, Galbraith Plot test revealed that the studies of Wang and Kim et al could contribute to substantial heterogeneity. There could be 3 reasons through analysis about Wang’s study. First, the strict exclusion criteria were most likely the major cause. Wang excluded patients with malignancies or multiple primary malignancies, hematological disease, inflammatory disease, hematology, influenced drugs use, missing preoperative complete blood cell count prior to surgery or prior chemotherapy or radiotherapy. Second, the study object was serous ovarian cancer, which had a high malignant potential. Third, the sample size of this study was only 126, which may cause the result not accurate enough like the studies of large sample size. As for the study of Kim, first, their inclusion criteria were strict, and Kim only included patients with clear cell ovarian carcinoma (CCOC) who did not have any inflammatory conditions except endometriosis and underwent primary debulking surgery. As we all know, CCOC is a unique histologic type of epithelial ovarian cancer, which is characterized by being a more aggressive histologic subtype 47,48 and has poor response rate to platinum-based chemotherapies. 49 Second, the sample size of Kim study was the smallest in 12 studies.
All of the 12 included studies treated NLR as a categorical variable. However, the cutoff values of NLR are different in these studies due to different methods. For instance, 7 of the included studies optimized NLR cutoff values for outcoming Receiver Operating Curve (ROC) values from 2.6 to 4.0. 26,30,31,34 -37 In contrast, one study used a median level (3.24), 32 one used the log-rank test (4), 27 and one used an interquartile level (1.86-3.77, from the lowest to highest category). 29 We didn’t find enough evidence to prove which method provides the most accurate value. Further researches are needed to clarify which cutoff method is the best one to assess the prognosis risk of patient with ovarian cancer.
Some limitations exist in this meta-analysis. First, the number of articles meeting our criteria was only 12, causing limited data for analysis. Second, the cutoff values of NLR in 12 studies were not the same, which may be the major cause to the heterogeneity. Third, only English articles were involved, leading to language bias and publication bias. Fourth, only 2 included articles were cohort studies. We need more prospective studies to confirm our conclusion. More scientifically designed clinical trials and further investigation are imperative to draw accurate conclusions.
In summary, our study demonstrated that depressed NLR was associated with higher OS and PFS in patients with ovarian cancer by meta-analysis. The association was both dependable in Asians and Caucasians. The findings could provide suggestions for clinical management of patients with ovarian cancer.
Footnotes
Authors’ Note
Gaowen Chen, Lin Zhu, and Yulu Yang contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the work was supported by the Science and Technology program of Guangdong province, China (2013B021800307), the National Natural Science Foundation of China (81773291), the Natural Science Foundation of Guangdong Province, China (2015A030313308), and the Wu Jieping Medical Foundation (320.6755.15010).