
Abstract
Background:
The plasminogen activator inhibitor-1 (PAI-1) was found in many types of tumor cells, which involved in tumorigenesis. Some studies investigated the associations between PAI-1 polymorphisms and various cancers, but the results were inconsistent. So this study did a meta-analysis to assess the strength of relationship between PAI-1 and cancer.
Methods:
Articles that meet the requirements were searched from PubMed, EMBASE, MEDLINE, Scopus, CNKI, Wanfang and SinoMed electronic databases before June 17th 2021. Stata version 11.2 was performed to merge the odds ratios (ORs) values and calculate 95% confidence intervals (CIs). Stratified analyses were assessed on the basis of types of cancer, ethnicity and source of the control group. Heterogeneity and sensitivity analysis were tested, and publication bias was also estimated. A meta-regression analysis was applied to explore sources of heterogeneity. The false-positive report probabilities (FPRP) and the Bayesian False Discovery Probability (BFDP) test were used to assess the credibility of statistically significant associations.
Results:
Ultimately, in this study, 33 eligible reports were included with 9550 cases and 10431 controls for the rs1799889 polymorphism, 5 reports with 2705 cases and 3168 controls for the rs2227631 polymorphism, and 4 reports with 2799 cases and 4011 controls for the rs2227667 polymorphism. The ORs and 95% CIs showed a statistically significant relationship between rs1799889 4G>5G polymorphism and cancer risk, especially in feminine cancer. The term refers to cancers that occur in the female reproductive system, such as ovarian, breast, endometrial and cervical cancer. Moreover, there was no association observed for the PAI-1 promoter A>G polymorphism (rs2227631 and rs2227667). In further subgroup analyses of 4G>5G polymorphism (rs1799889), an increased susceptibility to cancer was observed in Caucasians group and some types of cancer groups.
Conclusions:
This article comes to a conclusion that the rs1799889 polymorphism might help to increase the risk of cancer; moreover, the susceptibility to feminine cancer is more evident.
Introduction
Cancer is a primarily public health issue and global problem with high mortality rates. Substantial and convincing evidences suggested that genetic factors were indispensable factors of the pathogenesis of cancer. The study of genetic variation has had an enormous impact on the belief within the last 30 or so years that could directly or indirectly link specific variants with specific traits or diseases. The commonest type of gene mutation is single nucleotide polymorphism (SNP) at the genomic level, accounting for more than 90% of all known polymorphisms. SNPs could be applied to detect alleles at polymorphic sites for indirectly or directly physiological correlation with traits or disease. 1 In other words, researchers have found that some sorts of cancers, such as ovarian, breast and lung, were associated with genetic polymorphism via SNPs test.
Plasminogen activator inhibitor type 1 (PAI-1) made a critical difference in tumor progression, involving in degradation of the basement membrane and tumor stroma. 2 PAI-1 could inhibit the expression of active plasmin which degraded the fibrin. Hence overexpression of PAI-1 might lead to fibrinolytic system dysfunction, thereby further increasing thrombosis risk. 3,4 Therefore, PAI-1 regulated the growth, invasion and angiogenesis of many types of cancer cell in a dose-dependent manner. 5,6 The level of PAI-1 expression had been found to be modulated by its own genetic polymorphism, of which the most relevant SNP was a single guanosine nucleotide insertion/deletion variation (4G>5G). The location of 4G allele of 4G>5G polymorphism was the promoter region −675 base pairs upstream, PAI-1 gene (rs1799889) could cause an increase in expression levels of PAI-1 in plasma, which suggested that PAI-1 gene (rs1799889) had an effect on the binding of nuclear proteins. This nuclear proteins participated in the regulation of PAI-1 gene transcription and conditioned a clear hypo-fibrinolytic state. 7 In addition, the single nucleotide polymorphism identified in the promoter region −844 G/A (rs2227631) was be investigated. 8 Up to now, the studies that have been published frequently focused on 3 variants of the PAI-1 gene including the rs1799889/rs2227631/rs2227667 polymorphisms.
In order to get a farther understanding of the PAI-1 gene, many case-control reports have explored the correlation between the rs1799889/rs2227631/rs2227667 polymorphisms and the risk of different types of cancers. Nevertheless, these reports also showed inconsistency findings. To address these issues, this meta-analysis was conducted to obtain a more precise verdict about the relationship between the rs1799889/rs2227631/rs2227667 polymorphisms and cancer risks.
Materials and Methods
Strategy for Retrieving Qualified Articles in the Database
The studies about the relation between rs1799889, rs2227631, or rs2227667 polymorphisms and cancer risks were identified and the databases used in this study were PubMed, EMBASE, MEDLINE, Scopus, CNKI, Wanfang and SinoMed electronic databases. The searches identified the eligible publications using the following terms and keywords in the variety of ways: (1) “PAI-1”/“plasminogen activator inhibitor-1”/“SERPINE1”; (2) “polymorphism”/“geneotype”/“gene mutation”/“variant”/“variation”; (3) “carcinoma”/“cancer”/ “tumor.” The time cut-off point for this searching work was June 17th, 2021.
In order not to miss relevant important articles, we searched carefully and manually all qualified articles, review articles and other relevant studies and the search was repeated several times. Unpublished articles were not under discussion. We had registered our study with INPLASY. The registration number was INPLASY202160026, and the DOI number was 10.37766/inplasy2021.6.0026.
The Selection Criteria of Eligible Articles and Quality Assessment
The criteria of eligible articles: (1) evaluation of the link between at least one of these 3 polymorphisms (SERPINE1 rs1799889, rs2227631, rs2227667) and cancer risk; (2) published language: English, Chinese; (3) enough data to be available for odds ratios (OR) with the 95% confidence interval (95% CI) calculation; (4) study design: case-control; (5) If many studies from the same datum were available, only the studies with larger sample size or most recent studies were included in this study.
The studies were excluded according to the following criteria: (1) duplicate of previous published articles; (2) studies without essential data; (3) reviews, only abstracts, and studies with none of these 3 polymorphisms (SERPINE1 rs1799889, rs2227631, rs2227667).
This meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 9
The Newcastle-Ottawa scale (NOS) was proposed by Wells et al in the website (http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm), which was used to assess the quality of eligible articles. The checklist of NOS had 3 parts: selection, comparability and exposure, as well as a score range of 0 to 9.
Data Extraction
Two independent researches (Jiaxi Wang, Yuanyuan Peng) carefully selected relevant studies separately according the inclusive criteria. Another researches (Cuiping Li, Hejia Guo) checked the extraction of original data. If any controversial issue remained, all researches reached a consensus after discussions. The data collected from each article included first author’s last name, the published time of papers, ethnicity, country, the types of cancer, source of control and number of genotypes. Ethnicities were generally categorized as Caucasian and Asian. If some articles included more than one ethnic descent or had difficulty in distinguishing participants form original literature, the ethnicity in these kinds of articles was categorized as mixed ethnicity.
Data Calculation
Crude ORs and 95% CI were applied to calculate and analyze the relationship between rs1799889 polymorphisms and cancer risk in 4 models (homozygous model: 4G4G vs 5G5G; heterozygous model: 4G4G vs 4G5G; recessive model: 4G4G vs 5G4G+5G5G; dominant model: 4G4G+5G4G vs 5G5G). Subgroup analyses were calculated by ethnicity, source of controls and cancer types respectively. Crude ORs and 95% CI were applied to calculate and analyze the association between rs2227631/rs2227667 polymorphisms and the susceptibility to cancer in homozygous model (AA vs GG), heterozygous model (AA vs AG), recessive model (AA vs AG+GG) and dominant genetic model (AA+AG vs GG).
Heterogeneity was calculated and analyzed by using I 2 value and P value. I2 statistic indicated the proportion of total variation which was caused by the variation between study and study. The random effects model was used when there were statistical differences found in heterogeneity (P < 0.05, I 2 > 50%), or else the fixed effects model was conducted (P > 0.05, I 2 < 50%). Publication bias was used to calculate statistically by the Egger’s linear regression test. STATA version 11.2 (Stata Corp, College Station, TX, USA) counted all the results, using the P values of 2-sided (P < 0.05: statistical significance; P ≥ 0.05: no statistical significance). Meta-regression analysis were applied to the predefined sources of heterogeneity on the base of year of population, and ethnicity. Sensitivity analyses were carried out to check the rationality of our meta-analysis results by eliminating studies that deviated from HWE. Sensitivity analysis was to exclude 1 study at a time and combined the remaining studies to detect whether there was any influence on the results, if the original synthetic results included at least 5 studies.
The false positive report probability (FPRP) was calculated to evaluate significance findings. We set the threshold for FPRP at 0.2 and specified a prior probability of 0.25, 0.1, 0.01, 0.001 and 0.0001 to detect that a odds ratio (OR) of 1.5 was associated with cancer risk in the study. The results were considered noteworthy only if the FPRP value is less than 0.2. 10
Bayesian false discovery probability (BFDP) was estimated using Excel calculation spreadsheet to assess the credibility of statistically significant associations. 11 BFDP values below 0.8 were considered to be noteworthy.
Results
Study Characteristics
Totally, 373 possibly relevant articles were selected after duplicates were removed by searching online databases, according to the search criteria (Figure 1). A total of 252 irrelevant studies were deleted after reading the titles and abstracts of every single article in detail. A total of 121 potential reports were checked with the reference criteria from the mention above. After reading the full text, 84 articles were removed (58 articles: no sufficient data + 26 articles: review). No other articles were found from the references manually. A total of 37 articles were identified in this article, which included 33 articles with 9550 cases and 10431 controls samples for the rs1799889 polymorphism, 8,12 -43 5 articles with 2705 cases and 3168 controls samples for the rs2227631 polymorphism 23,38,41,44,45 and 4 articles with 2799 cases and 4011 controls samples for the rs2227667 polymorphism. 44 -47

The whole flow diagram of filtering the available articles in this study.
Concerning rs1799889 polymorphism, among the 33 case-control studies, there were 9 studies on breast cancer, 5 studies on colorectal cancer, 3 studies on ovarian cancer, 3 studies on endometrial cancer, 3 studies on hepatocellular cancer, 2 studies on oral cancer, 2 studies on leukemia cancer and 6 studies on other cancers (cervical cancer, lung cancer, glioblastoma, nasopharyngeal cancer); there were 9 hospital-based studies and 9 population-based studies; there were 22 studies for Caucasian, 10 studies for Asian and 1 study for mixed ethnicity. Concerning rs2227631 polymorphism, among the 5 case-control studies, there were one each studies consisted of the studies on ovarian cancer, breast cancer, gastric cancer, colorectal cancer and glioblastoma. Concerning ethnicity, 3 studies were subjects of Asian descent, 1 study was subjects of Caucasian descent and 1 study was a mixed population. Concerning rs2227667 polymorphism, among the 4 case-control studies, there were 2 studies on myeloma, one each studies on breast cancer and gastric cancer. Concerning ethnicity, there were 2 studies for Caucasian and 2 studies for Asian. The main characteristics of the eligible studies for rs1799889, rs2227631 and rs2227667 polymorphism were showed respectively in Table 1.
The Main Characteristics of the Eligible Studies for Rs1799889, Rs2227631 and Rs2227667 Polymorphism.a

Abbreviations: NA, not available; PB, population-based; HB, hospital-based; HWE, Hardy-Weinberg equilibrium; NOS, Newcastle-Ottawa scale.
a Mixed ethnicity: those studies with more than one ethnic group or those difficult to separate participants.
The NOS score of eligible articles was between 6 to 9, which indicated that the quality of included literatures were relatively high. Detailed scores were summarized in Table 1.
Quantitative Synthesis
Table 2 showed the overall OR with its 95% CI regarding the relationship between SERPINE1 rs1799889 polymorphism and cancer risk. When 33 studies were analyzed in all models, the rs1799889 polymorphism statistically increased cancer susceptibility (4G4G vs 5G5G: OR (95%CI) = 1.297(1.107-1.519), P = 0.001; 4G4G vs 4G5G, OR (95%CI) = 1.095(1.025-1.170), P = 0.007; 4G4G vs 4G5G+5G5G, OR (95%CI) = 1.104(1.038-1.176), P = 0.002; 4G4G+4G5G vs 5G5G, OR (95%CI) = 1.072(1.000-1.150), P = 0.049, (Figure 2 and Table 2). There were statistically increased risks among Caucasian populations in 4 models when conducting a stratified analysis based on ethnicity (4G4G vs 5G5G: OR (95%CI) = 1.435(1.159-1.778), P = 0.001; 4G4G vs 4G5G, OR (95%CI) = 1.113(1.029-1.203), P = 0.007; 4G4G vs 4G5G+5G5G, OR (95%CI) = 1.302(1.118-1.516), P = 0.001;4G4G+4G5G vs 5G5G, OR (95%CI) = 1.217(1.038-1.427), P = 0.016, Table 2). However, the increased risk was not found in all models of Asian populations. Moreover, there were statistical significances in some comparison models for hospital-based groups (4G4G vs 5G5G: OR (95%CI) = 1.429(1.061-1.925), P = 0.019; 4G4G vs 4G5G+5G5G, OR (95%CI) = 1.352(1.07-1.708), P = 0.012, Table 2). However, the increased risk was not found in all models of population-based groups.
Stratified Analyses of the Rs1799889 Polymorphism on Cancer Risk.a

Abbreviations: OR, odds ratio; CI, confidence interval; PB, population-based; HB, hospital-based; FPRP, false positive report probability; BFDP, Bayesian False Discovery Probability.
a The results in bold represented there was statistically significant noteworthiness at 0.2 level by FPRP or 0.8 level by BFDP calculations.
bChi-square test was used to calculate the genotype and haplotype frequency distributions.
cStatistical power was the power to detect an odds ratio of 1.5 for the homozygotes with the rare genetic variant and 1 for the heterozygotes and for the homozygote with the common variant.
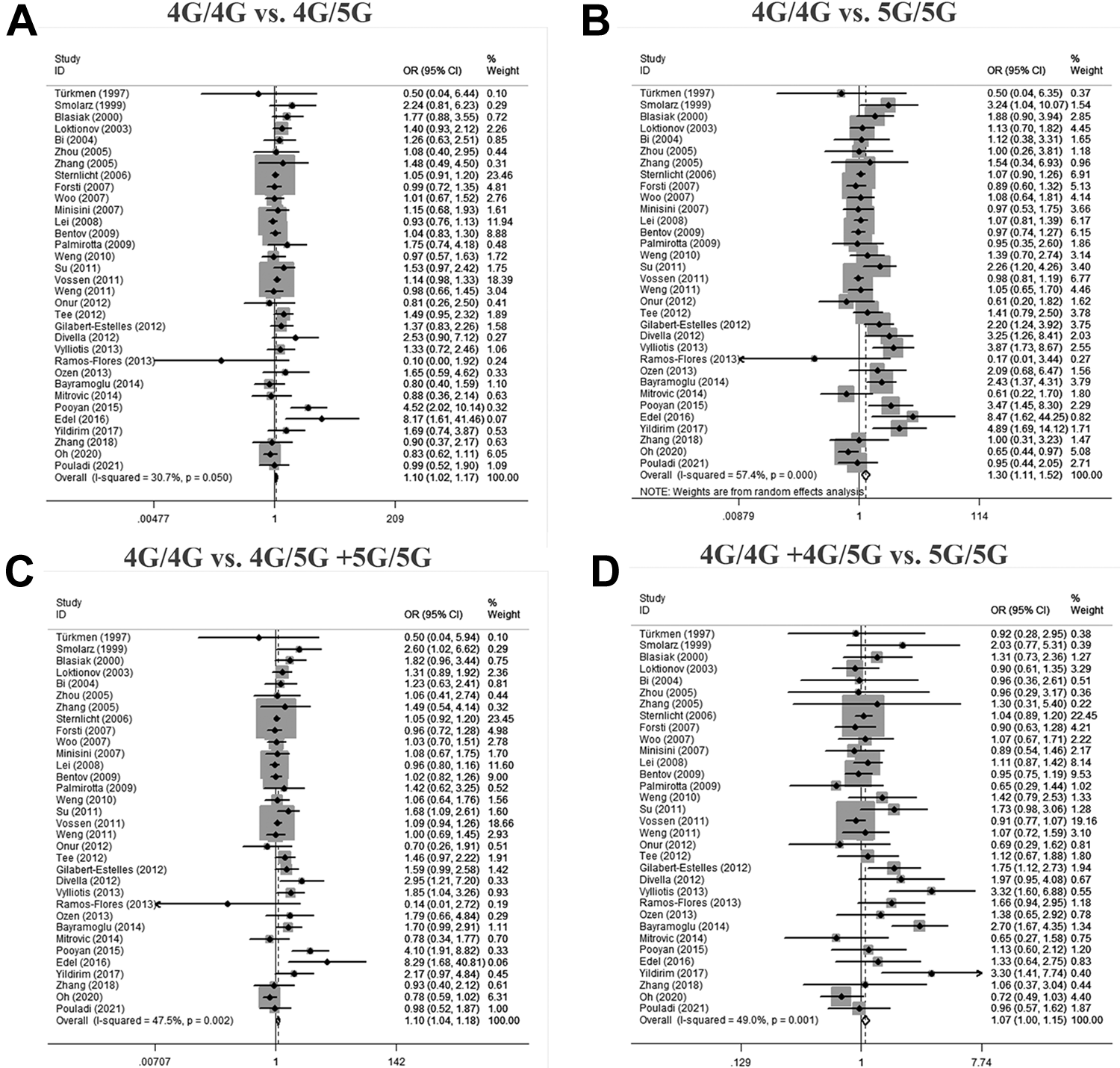
Forest plot of the statistical correlation between rs1799889 polymorphism and cancer susceptibility in all models (A: 4G4G vs 4G5G; B: 4G4G vs 5G5G; C: 4G4G vs 4G5G + 5G5G; D: 4G4G + 4G5G vs 5G5G). Data were pooled odds ratios (OR) with 95% confidence intervals (CI) determined using random-effects models or fixed-effects models according to I 2 values.
The increased susceptibility to feminine cancer were observed (4G4G vs 5G5G: OR (95%CI) = 1.157(1.036-1.291), P = 0.009; 4G4G vs 4G5G+5G5G, OR (95%CI) = 1.107(1.018-1.204), P = 0.017; and 4G4G+4G5G vs 5G5G, OR (95%CI) = 1.106(1.008-1.214), P = 0.033, (shown in Figure 3 and Table 3). Feminine cancer is specific to women, including ovarian, breast, endometrial and cervical cancer in this study. The term refers to cancers that occur in the female reproductive system. The results of the stratified analysis based on ethnicity showed that the increased risk was detected among Asian populations in 3 models (4G4G vs 5G5G: OR (95%CI) = 1.586(1.087-2.314), P = 0.017; 4G4G vs 4G5G, OR (95%CI) = 1.426(1.08-1.884), P = 0.012; and 4G4G vs 4G5G+5G5G, OR (95%CI) = 1.462(1.123-1.903), P = 0.005, shown in Table 3). On the contrary, the increased risk was detected among Caucasians in 2 models (4G4G vs 5G5G: OR (95%CI) = 1.159(1.020-1.315), P = 0.023; and 4G4G+4G5G vs 5G5G, OR (95%CI) = 1.126(1.013-1.252), P = 0.028, shown in Table 3). However, the increased risk was not found in all models of hospital-based groups and population-based groups.

Forest plot of the statistical correlation between rs1799889 polymorphism and the susceptibility of feminine cancer in all models (A: 4G4G vs 4G5G; B: 4G4G vs 5G5G; C: 4G4G vs 4G5G + 5G5G; D: 4G4G + 4G5G vs 5G5G). Data were pooled odds ratios (OR) with 95% confidence intervals (CI) determined using random-effects models or fixed-effects models according to I 2 values.
Stratified Analyses of the rs1799889 Polymorphism on Feminine Cancer Risk.a

Abbreviations: OR, odds ratio; CI, confidence interval; PB, population-based; HB, hospital-based; FPRP, false positive report probability; BFDP, Bayesian False Discovery Probability.
a The results in bold represented there was statistically significant noteworthiness at 0.2 level by FPRP or 0.8 level by BFDP calculations.
bChi-square test was used to calculate the genotype and haplotype frequency distributions.
cStatistical power was the power to detect an odds ratio of 1.5 for the homozygotes with the rare genetic variant and 1 for the heterozygotes and for the homozygote with the common variant.
The increased or reduced susceptibility to masticatory and gastrointestinal cancer were not observed (shown in Figure 4 and Table 4). The increased risk was detected among Caucasian populations (4G4G vs 4G5G: OR (95%CI) = 1.142(1.005-1.297), P = 0.042, shown in Table 4). On the contrary, moreover, these results were similar among Asians, hospital-based groups and population-based groups.

Forest plot of the correlation between rs1799889 polymorphism and the susceptibility of masticatory and gastrointestinal cancer in all models (A: 4G4G vs 4G5G; B: 4G4G vs 5G5G; C: 4G4G vs 4G5G + 5G5G; D: 4G4G + 4G5G vs 5G5G). Data were pooled odds ratios (OR) with 95% confidence intervals (CI) determined using random-effects models or fixed-effects models according to I 2 values.
Stratified Analyses of the Rs1799889 Polymorphism on Masticatory and Gastrointestinal Cancer Risk.a

Abbreviations: OR, odds ratio; CI, confidence interval; PB, population-based; HB, hospital-based; FPRP, false positive report probability; BFDP, Bayesian False Discovery Probability.
a The results in bold represented there was statistically significant noteworthiness at 0.2 level by FPRP or 0.8 level by BFDP calculations.
bChi-square test was used to calculate the genotype and haplotype frequency distributions.
cStatistical power was the power to detect an odds ratio of 1.5 for the homozygotes with the rare genetic variant and 1 for the heterozygotes and for the homozygote with the common variant.
Table 5 showed the overall OR with its 95% CI regarding the relationship between SERPINE1 rs2227631 polymorphism and cancer risk. No association between the rs2227631 polymorphism and cancer risk was detected (AA vs GG: OR (95%CI) = 0.925(0.65-1.316), P = 0.665; AA vs AG: OR (95%CI) = 0.975(0.686-1.386), P = 0.888; AA vs AG+GG: OR (95%CI) = 0.956(0.686-1.332), P = 0.789; and AA+AG vs GG: OR (95%CI) = 0.932(0.832-1.043), P = 0.220).
Stratified Analyses of the Rs2227631 and Rs2227667 Polymorphism on Cancer Risk.

Abbreviations: OR, odds ratio; CI, confidence interval; PB, population-based; HB, hospital-based; FPRP, false positive report probability; BFDP, Bayesian False Discovery Probability.
aChi-square test was used to calculate the genotype and haplotype frequency distributions.
bStatistical power was the power to detect an odds ratio of 1.5 for the homozygotes with the rare genetic variant and 1 for the heterozygotes and for the homozygote with the common variant.
Table 5 showed the overall OR with its 95% CI regarding the SERPINE1 rs22276367 polymorphism and cancer risk. The results showed that no association between the rs2227667 polymorphism and cancer risk was detected (AA vs GG: OR (95%CI) = 0.649(0.393-1.071), P = 0.091; AA vs AG: OR (95%CI) = 0.980(0.687-1.398), P = 0.911; AA vs AG+GG: OR (95%CI) = 0.889(0.701-1.128), P = 0.333; and AA+AG vs GG: OR (95%CI) = 0.687(0.409-1.155), P = 0.157).
Publication Bias
Begg’s test and Egger’s test were used to assess about possible publication bias. According to the SERPINE1 rs1799889 polymorphism, some results showed the evidence of publication bias (Egger’s test for 4G4G vs 5G5G, 4G4G vs 4G5G, 4G4G vs 4G5G+5G5G, 4G4G+4G5G vs 5G5G: P = 0.016/0.038/0.009/0.035, Table 2). According to the SERPINE1 rs2227631/rs2227667 polymorphism, the results showed no evidence of publication bias (Table 5).
Sensitivity Analysis
None of the comparisons in the sensitivity analysis detected a change in the outcome of PAI-1 gene polymorphism, indicating that our results were statistically stable and reliable. The meta-regression found that ethnicity was the potential source of heterogeneity regarding the relationship between SERPINE1 rs2227631 polymorphism and cancer risk.
FPRP and BFDP Test
The FPRP values of statistical power for significant findings about the SERPINE1 rs1799889 polymorphism were shown in Table 2. According to the results of the FPRP analyses, almost all models of rs1799889 polymorphism were found to be noteworthy by FPRP estimation at the OR of 1.5 with the prior probability of 0.25 and 0.1, but there were no noteworthy by BFDP test at the OR of 1.5 with the prior probability of 0.01, 0.001 and 0.000001, which suggested that the results of this study should be interpreted with caution.
Discussion
Cancer was a significant economic burden for public health systems worldwide. Up to now, a great deal of research has shown that cancer might be closely related to genetic factors. PAI-1 polymorphisms were considered to be closely related to cancer development and outcome among different individuals, 2,48 since genetic variations had an essential impact on the activities of PAI-1. In regard to the PAI-1 gene, the polymorphism about rs1799889, rs2227631 and rs2227667 have been the most frequently studied, but the conclusion was controversial about judging the relationship between PAI-1 polymorphism and cancer risk which was estimated in our present study by aggregating the findings of overall qualified case-controlled studies.
Our present study found that the SERPINE1 rs1799889 polymorphism was statistically related with cancer risk, but there was no association observed for rs2227631 and rs2227667 polymorphism. Furthermore, the rs1799889 polymorphism was found to have higher risks for breast, endometrial and colorectal cancer, but there was no effect on susceptibility to uterine cervical cancer. 19,22,31,34 However, the linkage disequilibrium analysis detected that both 4G for PAI-1 rs1799889 and A for TGF-β1 rs1800468 pair-haplotype was in strong linkage disequilibrium with a statistically increased risk to uterine cervical cancer. 34 Meanwhile, the linkage disequilibrium analysis detected that both 4G4G for PAI-1 rs1799889 and CC for uPArs 4065 pair-haplotype was in strong linkage disequilibrium with a statistically increased risk to cervical neoplasia. 30 The polymorphism of rs2227631 was found to have higher risks for breast cancer and glioblastoma, but there was no effect on susceptibility to ovarian and gastric cancer. 23,38,44,45 The polymorphism of rs2227667 was at higher risks for breast cancer and multiple myeloma, while no effect was found in gastric cancer. 44 -47 PAI-1 gene-polymorphism exerted different impacts on different organs, maybe thereby increasing the persons who had a specific inherited predisposition to cancer, but the mechanism was not entirely clear. According to our present meta-analysis, PAI-1 gene-polymorphism in different locations maybe have different distributions to different types of cancers.
Concerning stratified analysis by ethnicity about rs1799889, our present meta-analysis found an ascending risk in 4G carriers among the Caucasian and Asian population but not mixed population for these types of cancers. For masticatory and gastrointestinal cancer, no significantly increased risk was found. Moreover, there was a statistically increased risk of gynecological cancer in both Caucasian and Asian population, potential explanations for this result included 3 aspects: (1) wide difference in incidence rates of gene polymorphisms existed in disparate ethnic populations 49 ; (2) wide difference in susceptibility to different cancers existed in people in different parts of the world; (3) some objective factors might also have some effect such as sample size, selection bias, inclusion or exclusion criteria and so on. Therefore, a big population study with multiple analyses was needed to conduct and further prove the relationship between rs1799889 polymorphism and cancer risks.
When interpreting the pooled findings in our present meta-analysis, there were some restrictions that should be mentioned. Firstly, although we had detected a comprehensive and thorough search, the count of studies and participant studies were not adequate, especially for rs2227631 and rs2227667. Secondly, there was no further analysis of the underlying correlation between gene and behavior, environment, prognosis, or linkage disequilibrium and so on, because common raw data was missing. Thirdly, most research mainly focused on polymorphism (rs1799889) and tiny minority research focused on rs1799768, both of which located in the promoter region −675 bp. 50 However, rs1799768 polymorphism located in the SERPINE1 promoter was genotyped. 44 Based on the controversy above mentioned, we had to exclude the research about rs1799768. Finally, the meta-analysis revealed some statistically significant results in Egger’s test which suggested the existence of the publication bias, hence, the corresponding results should be interpreted cautiously.
Through a review of the literature, we found that 2 similar articles had been published in the past. 50,51 Compared with these articles, the following contents were added to our study: (1) relevant research literatures after 2013 were added; (2) the feminine, masticatory and gastrointestinal cancer subgroups were compared and analyzed; (3) 2 more sites of rs2227631 and rs2227667 polymorphisms were added.
Our study finally reached a conclusion that PAI genetic polymorphism (rs1799889) might be connected with the predisposition of cancer, especially feminine cancer. Moreover, the increased cancer risks were observed in Caucasians group. No significant association was identified for the rs2227631 and rs2227667 polymorphisms with cancer risk. Furthermore, rs1799889 polymorphism may be a potential marker genotyping to cancer susceptibility for clinical assessment.
Footnotes
Authors’ Note
Our study did not require an ethical board approval because it did not contain human or animal trials.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was supported in part by the Natural Science Foundation of Guangxi Province (Grant No.: 2018GXNSFAA138003).