
Abstract
Background
Chronic respiratory diseases (CRDs) are leading causes of morbidity and mortality worldwide, yet simple prognostic biomarkers are lacking. The systemic inflammation response index (SIRI) integrates neutrophil, monocyte and lymphocyte counts and has shown prognostic value in malignancies and cardiovascular disease, but its role in CRDs remains unclear. We hypothesized that higher baseline SIRI is independently and dose-dependently associated with increased all-cause mortality across the spectrum of CRDs.
Methods
We analyzed data from the National Health and Nutrition Examination Survey (NHANES) 2001–2018, including 7923 adults with CRDs (asthma, emphysema or chronic bronchitis). SIRI was calculated from a single baseline complete blood count. Participants were followed until death or 26 April 2022 (median 7.4 years). Cox proportional-hazards models (three levels of adjustment) evaluated the association between SIRI tertiles and all-cause mortality. Sensitivity analyses included continuous SIRI, a clinically derived cut-off (12.98) and CRD-specific sub-cohorts.
Results
Higher SIRI tertiles were progressively associated with increased mortality: fully-adjusted hazard ratios (Model 3) were 1.19 (95% CI 1.02–1.39) and 1.88 (1.63–2.16) for tertiles two and three versus tertile 1 (P-trend <0.001). Each 1-unit rise in continuous SIRI conferred an 1.01% excess risk (HR 1.0101, 95% CI 1.0082–1.0121). The unitless cut-off value of ≥12.98 identified a high-risk group with an increased risk of all-cause mortality (HR 1.69, 95% CI 1.51–1.89). This association was consistent for all-cause mortality across the asthma (HR 1.83), emphysema (HR 1.70), and chronic bronchitis (HR 1.89) sub-cohorts.
Conclusions
SIRI is an independent, dose-dependent predictor of all-cause mortality in patients with CRDs, performing robustly across asthma, emphysema and chronic bronchitis. These findings support the use of SIRI as a readily available prognostic tool in CRD management.
Introduction
Chronic respiratory diseases (CRDs) encompass a range of pulmonary and airway pathologies, most notably chronic bronchitis, emphysema, and asthma. 1 The global health burden of CRDs is substantial, contributing significantly to worldwide morbidity and mortality. 2 Data from the Global Burden of Disease study reveals that CRDs are responsible for nearly nine million deaths annually, accounting for 7% of global deaths. 3 The prevalence of these conditions has shown a marked increase, with an estimated 454.6 million cases diagnosed in 2019.1,4 This growing epidemic not only has serious adverse effects on patients’ quality of life and mortality risks but also imposes a considerable strain on global healthcare systems, society, and economic resources.5,6
The systemic inflammation response index (SIRI), a composite inflammatory biomarker calculated from peripheral blood neutrophil, monocyte, and lymphocyte counts, 7 has been increasingly utilized as a prognostic indicator for survival and mortality across numerous diseases. The prognostic value of complete blood count (CBC)-derived cellular ratios, such as the neutrophil-to-lymphocyte ratio (NLR), is well-established in respiratory conditions.8,9 In a prospective cohort of 298 postoperative colorectal patients, SIRI exhibited superior predictive performance for survival outcomes when compared to other conventional serum inflammatory markers. 10 Similarly, a study by Wang et al. involving 52 patients with advanced lung adenocarcinoma demonstrated that low SIRI levels were associated with a prolonged progression-free survival. 11 This finding is supported by a meta-analysis which concluded that high SIRI levels are predictive of poor survival outcomes in breast cancer patients. 12 Furthermore, not only in chronic heart failure patients, SIRI can provide better prognostic discrimination correlating with mortality risk in CHF patients, 13 but also in cardiovascular and cerebrovascular diseases.14–17 Besides, elevated SIRI levels are also associated with the incidence and mortality rates of chronic kidney disease (CKD). 18 SIRI integrates neutrophil, monocyte, and lymphocyte counts–key cellular mediators of chronic airway inflammation. In CRDs like asthma and COPD, neutrophils drive tissue damage through protease release and oxidative stress, while monocytes differentiate into alveolar macrophages that perpetuate inflammation and remodeling. Lymphopenia, conversely, reflects impaired immunoregulation. Thus, SIRI quantifies the net burden of these pathophysiological processes central to CRD progression.
Although there is emerging evidence that risk of all-cause mortality in asthma depends on the highest quartile of SIRI compared to the lowest, 19 the research on the relationship between SIRI and mortality risk in CRDs has not been evaluated as far as we know. This gap is critical because CRDs exhibit unique immune phenotypes (e.g., neutrophilic vs eosinophilic inflammation) that may differentially influence SIRI’s predictive capacity. Therefore, the primary objective of this study was to determine the association between SIRI and all-cause mortality in a large, nationally representative cohort of US adults with CRDs. We hypothesized that a higher SIRI would be independently associated with increased mortality risk and that this association would be consistent across different types of CRDs, including asthma, chronic bronchitis, and emphysema.
Research design and methods
Study population
The NHANES provided cross-sectional data to assess nutritional and health status among the US non-institutionalized civilian population. Our study utilized data from the continuous NHANES survey from 11 survey cycles, conducted from 2001 to 2018 with a total of 91,351 participants. A total of 53,756 eligible participants aged 18 years and older were included in the study population. We next excluded patients without SIRI or CRDs disease data. Additionally, participants without records of age, sex, race, marital status, education level, body mass index, and family income-poverty ratio were excluded. Ultimately, there were 7923 participants were included in this study (Figure 1). Flow chart of study population selection.
This retrospective cohort study used the 2001–2018 NHANES cycles. SIRI was computed from the complete blood-count differential obtained at each participant’s single baseline mobile-examination-center visit; no repeated measurements were available. Mortality was ascertained via linkage to the National Death Index through 26 April 2022, yielding a median follow-up of 7.4 years (IQR 4.1–11.2) from blood draw to death or censoring.
Statistical analysis
SIRI was (neutro-phil count × monocyte count)/lymphocyte count. Participants were equally classified into three groups based on the values of SIRI. The adjusted hazard ratios (HRs) and 95% confidence intervals (95% CIs) were calculated through using Cox proportional hazards regression model. This observational study used three models based on the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guideline. 20 Model I was adjusted for non. Model II was adjusted for age, sex, and race. Model III was adjusted for all variables in model II and included other risk factors for marital status, education level, body mass index, and family income-poverty ratio. Furthermore, Kaplan–Meier survival curves for all-cause mortality stratified by the values of SIRI index was generated. Smooth curve fitting (penalized spline method) examined the nonlinearity association between SIRI index and all-cause mortality was to be used. All data analyses were performed using R version 4.2.2, and p values less than 0.05 indicated statistical significance.
Results
Subject characteristics
Demographic and clinical characteristics according to systemic inflammation response index.
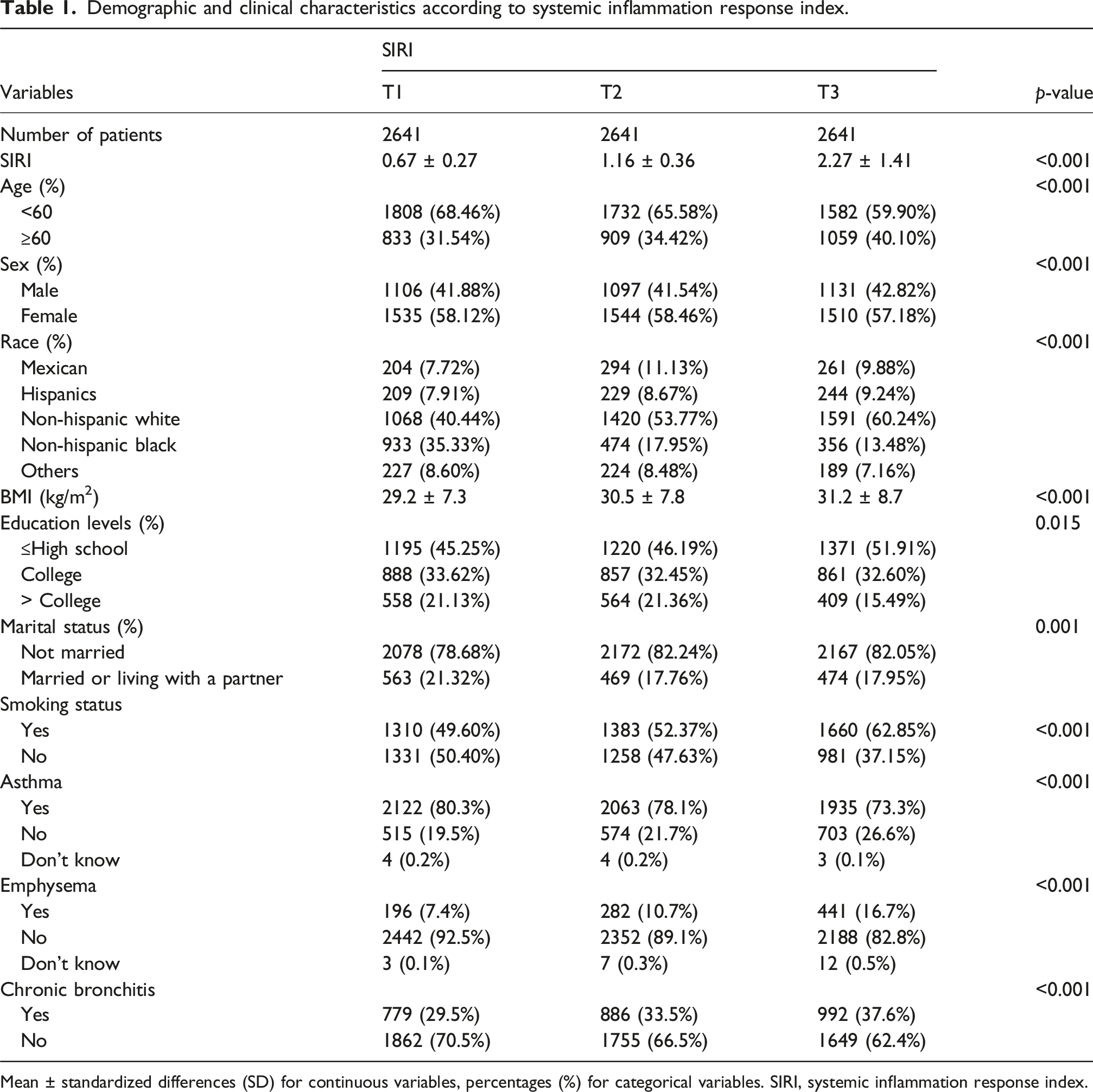
Mean ± standardized differences (SD) for continuous variables, percentages (%) for categorical variables. SIRI, systemic inflammation response index.
Association between SIRI index and mortality
Multivariate cox regression analysis of SIRI with all-cause mortality.
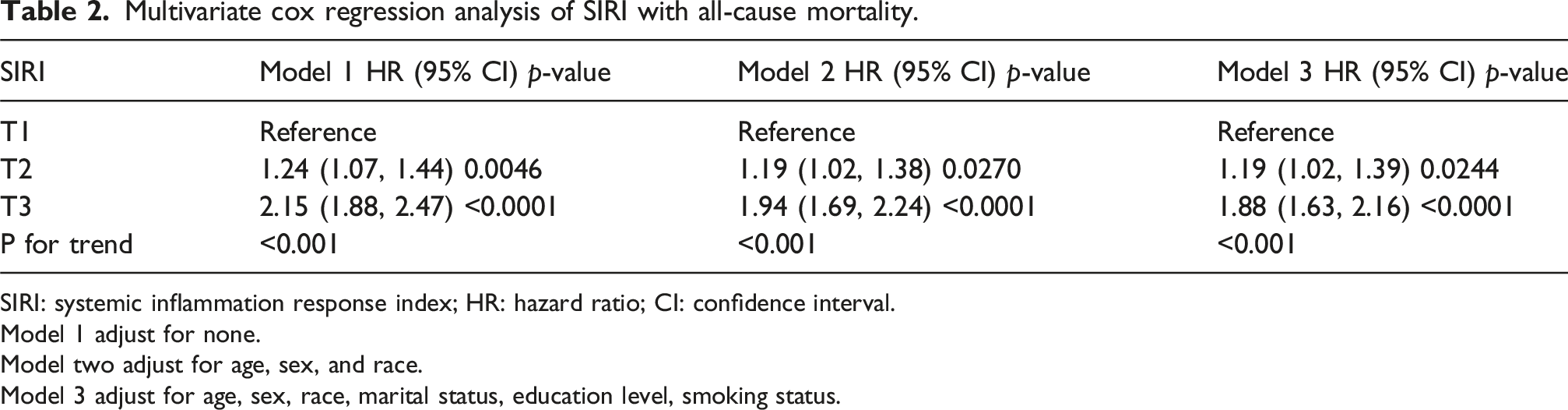
SIRI: systemic inflammation response index; HR: hazard ratio; CI: confidence interval.
Model 1 adjust for none.
Model two adjust for age, sex, and race.
Model 3 adjust for age, sex, race, marital status, education level, smoking status.

Restricted cubic spline analysis of the association between SIRI and all-cause mortality.
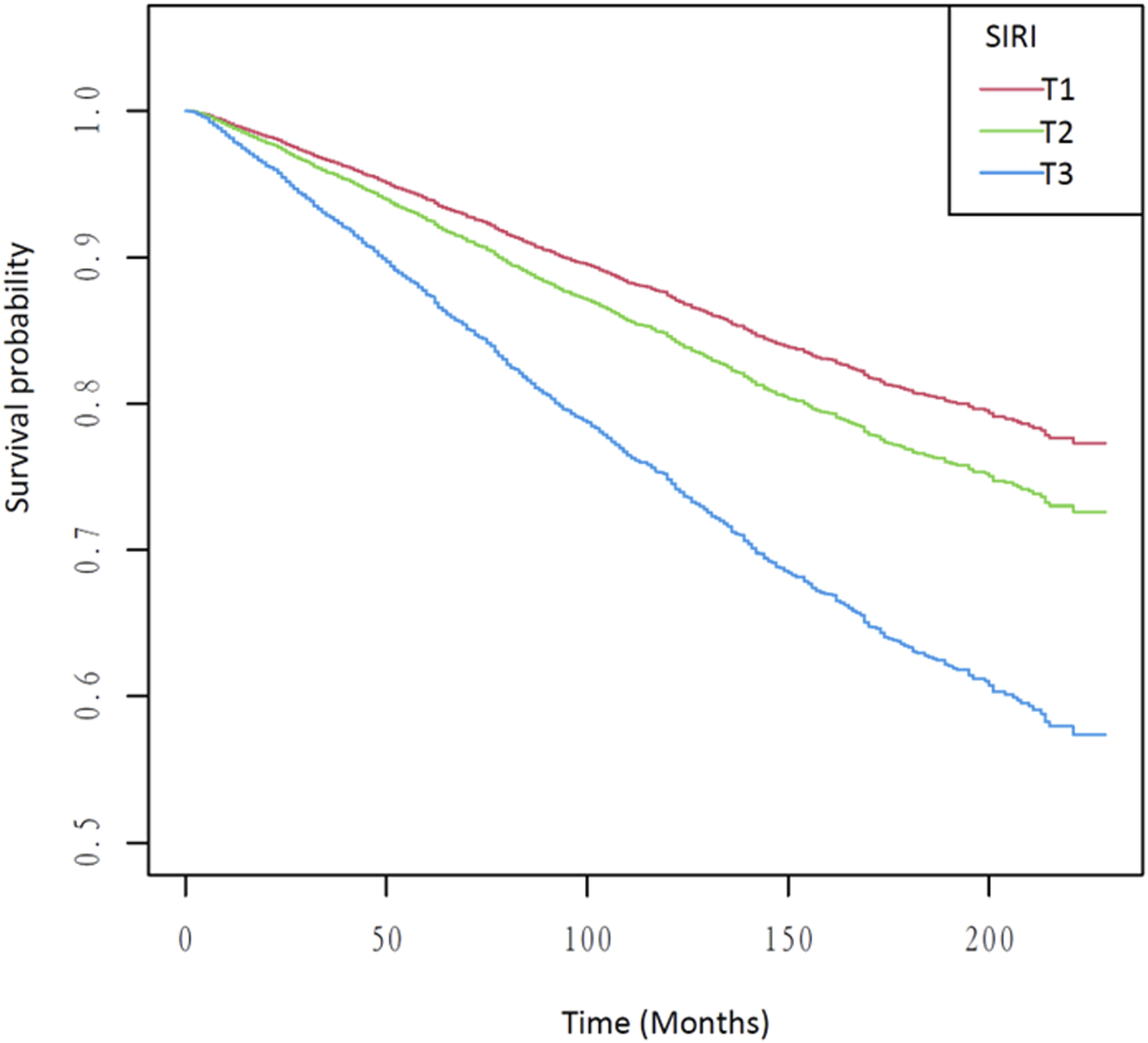
Kaplan–meier survival analysis plot for all-cause mortality with SIRI categories.
Subgroup of association between systemic inflammation response index and all-cause mortality.

Association between SIRI (tertiles) and all-cause mortality in patients with asthma, emphysema, and chronic bronchitis.

Model 1 adjust for none.
Model 2 adjust for age, sex, and race.
Model 3 adjust for age, sex, race, marital status, education level, smoking status.
As detailed in Supplemental Table 1, we evaluated the prognostic performance of systemic immune-inflammation index (SII), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and monocyte-to-lymphocyte ratio (MLR) through multivariable Cox regression. In unadjusted analyses (Model 1), all inflammatory indices exhibited significant associations with mortality, with MLR showing the strongest effect (T3 HR = 3.05, p < 0.001). However, after adjustment for age, sex, race, and sociodemographic confounders (Model 3), NLR (T3 HR = 1.88, 95% CI: 1.63–2.17) and MLR (T3 HR = 1.80, 95% CI: 1.55–2.09) retained significant but attenuated risks, while PLR demonstrated weaker predictive capacity (T3 HR = 1.24, 95% CI: 1.09–1.42). Then, we determined the optimal prognostic cut-off for SIRI by maximally selected rank statistics, identifying a single threshold of 12.98 that best stratified mortality risk. Participants with SIRI ≥12.98 exhibited a consistently higher hazard of all-cause death—HR 1.97 (95% CI 1.76–2.19) unadjusted, attenuating to HR 1.69 (95% CI 1.51–1.89) after full adjustment—confirming the clinical relevance of this cut-off (Supplemental Table 2). Beyond tertile stratification, treating SIRI as a continuous variable yielded a consistent dose-response pattern: each 1-unit increase in SIRI was associated with an 1.01% rise in all-cause mortality after full adjustment (Model 3 HR 1.0101, 95% CI 1.0082–1.0121, p < 0.001; Supplemental Table 3).
Discussion
This study is the first to establish the SIRI as a novel, independent, and dose-dependent predictor of all-cause mortality in a large, nationally representative cohort of patients with CRDs. Utilizing data from the NHANES database (2001–2018), we identified a significant linear association between elevated SIRI levels and increased risk of all-cause mortality. Crucially, this association remained robust after extensive adjustment for sociodemographic and clinical confounders, indicating that SIRI may serve as a readily available and potent prognostic tool for risk stratification in CRD patients. A key novel insight from our analysis is the consistency of this association across the major CRD entities—asthma, emphysema, and chronic bronchitis—suggesting SIRI captures a universal inflammatory risk pathway common to these diseases. Recent studies by Buonacera et al. and Regolo et al. further highlight that sustained neutrophilia and systemic inflammation—core components of SIRI—are key drivers of respiratory failure and mortality, thereby reinforcing its prognostic relevance across chronic respiratory diseases.21–23
The prognostic value of complete blood count (CBC)-derived inflammatory biomarkers, such as the neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), platelet-to-lymphocyte ratio (PLR), and systemic immune-inflammation index (SII), has been increasingly recognized in CRDs. 19 The prognostic significance of these indices has been well-documented. A cross-sectional NHANES study by Zhu et al. linked elevated NLR levels with higher all-cause mortality in asthma. 24 This association was corroborated by Shi et al., who confirmed a correlation between NLR and the severity and prognosis of asthma in both adults and children.25,26 Furthermore, Xuanqi et al. showed that PLR can predict the frequency of acute exacerbations in patients with stable chronic obstructive pulmonary disease (COPD), 27 and both NLR and PLR have been identified as prognostic predictors for mortality in COPD. 28 A higher SII has been associated with a poorer prognosis in combined cohorts of COPD and asthma patients. 29 While these studies lay a foundation for the role of systemic inflammation, our findings uniquely demonstrate that SIRI—integrating three key immune cell lineages (neutrophils, monocytes, and lymphocytes)—provides a superior and more holistic reflection of the dysfunctional immune response in CRDs, which is strongly predictive of mortality.
Although asthma, COPD, chronic bronchitis, and other major CRDs have distinct pathophysiological mechanisms, they all share a common feature: unresolved chronic inflammatory responses.30–32 Evidence suggests that elevated and activated neutrophil levels are linked to symptom relief and treatment outcomes in symptomatic asthma patients. 33 Furthermore, monocytes in the peripheral blood are also activated in asthma patients. 34 On one hand, these monocytes can differentiate into macrophages or dendritic cells, thereby promoting the inflammatory process and contributing to lung function destruction.35–37 On the other hand, lymphocytes, which play a regulatory role in allergic inflammation associated with asthma, 38 may have a diminished response due to the increase in neutrophil and monocyte counts. In COPD patients, the levels of CD8 + T lymphocytes in the blood are elevated compared to healthy individuals.39,40 However, studies also indicate that T cell-mediated immune responses may be diminished in severe COPD patients. 41 Tzu-Tao et al. further confirmed that the percentage of peripheral blood lymphocytes is related to the worsening of COPD symptoms. 42 Additionally, research has shown a relationship between an increased peripheral blood neutrophil count and higher rates of COPD exacerbation and mortality.43,44 Moreover, reactive oxidative stress (ROS), which is closely linked to acute exacerbation of COPD,45–47 can induce chemotaxis and increase the count of peripheral blood monocytes. This suggests that an increased peripheral blood monocyte count may also be associated with acute exacerbations of COPD. Based on these findings, it is reasonable to speculate that other CRDs may exhibit similar changes in peripheral blood inflammatory cells. Therefore, utilizing the SIRI, which incorporates these cell counts, is a suitable approach for predicting the mortality rate of CRD patients.
This study has several notable strengths. First, to our knowledge, this is the first study to investigate the association between SIRI levels and mortality risk specifically in patients with CRDs. Second, with 7923 participants included in our analysis, the large sample size provides robust statistical power and enhances the credibility of our findings. Third, our statistical models were adjusted for several potential confounders and risk factors, which further strengthens the reliability of our results.
However, several limitations of our study should be considered. The data were sourced from the cross-sectional NHANES database, which, by its nature, provides only a snapshot of health status at a specific time point. This design limits our ability to establish causality or track the long-term relationship between CRDs and mortality. The limitations of the NHANES database also extended to key clinical and laboratory parameters. Inconsistent and incomplete measurement of CRP/hs-CRP across NHANES cycles precluded their inclusion in our models; future studies with standardized inflammatory markers are warranted to refine prognostic assessments. Additionally, the lack of data on critical clinical parameters such as oxygen therapy, pulmonary function tests, and disease-specific medications prevented further adjustment for these potential confounders. The absence of P/F ratio data also restricted our direct assessment of hypoxemic severity, suggesting that future studies should prioritize collecting arterial blood gas data to validate SIRI’s prognostic utility, particularly in respiratory failure subgroups. Future research could also validate SIRI against P/F ratios in mechanically ventilated patients. Lastly, the unavailability of comprehensive data on dyspnea and exercise capacity in NHANES prevented the use of established clinical indices, such as the BODE index, which could serve as a valuable complement to SIRI in assessing CRD prognosis.
In summary, our study provides evidence that higher SIRI levels are relevant to the increased all-cause mortality in patients with CRDs. However, Further research is warranted to confirm our findings.
Supplemental Material
Supplemental Material - Association between the systemic inflammation response index and all-cause mortality in patients with chronic respiratory diseases: A nationwide cohort study from the NHANES 2001–2018
Supplemental Material for Association between the systemic inflammation response index and all-cause mortality in patients with chronic respiratory diseases: A nationwide cohort study from the NHANES 2001–201 by Danyan Huang, Chunfeng Xing, Yongwen Feng, Pan Jiang, Jibo Li, Haoda Liang, Feng Xu and Dandan He in Chronic Respiratory Disease
Supplemental Material
Supplemental Material - Association between the systemic inflammation response index and all-cause mortality in patients with chronic respiratory diseases: A nationwide cohort study from the NHANES 2001–2018
Supplemental Material for Association between the systemic inflammation response index and all-cause mortality in patients with chronic respiratory diseases: A nationwide cohort study from the NHANES 2001–201 by Danyan Huang, Chunfeng Xing, Yongwen Feng, Pan Jiang, Jibo Li, Haoda Liang, Feng Xu and Dandan He in Chronic Respiratory Disease
Supplemental Material
Supplemental Material - Association between the systemic inflammation response index and all-cause mortality in patients with chronic respiratory diseases: A nationwide cohort study from the NHANES 2001–2018
Supplemental Material for Association between the systemic inflammation response index and all-cause mortality in patients with chronic respiratory diseases: A nationwide cohort study from the NHANES 2001–201 by Danyan Huang, Chunfeng Xing, Yongwen Feng, Pan Jiang, Jibo Li, Haoda Liang, Feng Xu and Dandan He in Chronic Respiratory Disease
Footnotes
Author contributions
Danyan Huang, Yongwen Feng and Jibo Li contributed equally to study conceptualization, data curation, and initial manuscript drafting. Pan Jiang and Haoda Liang performed additional statistical analyses, generated the figures and tables, and critically revised the manuscript. Chunfeng Xing led the sensitivity analyses, conducted all subgroup analyses, and substantially revised the Methods and Discussion sections during the revision phase. Dandan He, as the corresponding author, coordinated the response to reviewers’ comments, supplied missing data, refined the statistical models, and conducted the final scientific and linguistic review of the revised manuscript. Feng Xu and Dandan He jointly supervised the overall study and verified the accuracy of all revisions. All authors read and approved the final submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Supported by Sanming Project of Medicine in Shenzhen Guangming (szgmtd2025003) and grants from Shenzhen Science and Technology Program (JCYJ20240813152030039).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.