
Abstract
Objective
To investigate markers of systemic inflammation and the effect of thyroid dysfunction on these parameters in patients with Hashimoto’s thyroiditis (HT).
Methods
Patients with HT and volunteer healthy individuals admitted to the general surgery outpatient clinic between January 2020 and June 2023 were enrolled into the study. Patients with HT were divided into euthyroid, hypothyroid, and hyperthyroid subgroups. All participant data were retrospectively extracted from the hospital database.
Results
A total of 268 patients (euthyroid, n = 131; hypothyroid, n = 83; and hyperthyroid, n = 54) and 124 controls were included. The platelet-to-lymphocyte ratio was lower in the euthyroid group versus control group, and the neutrophil-to-lymphocyte ratio was lower in controls than the three patient subgroups. Euthyroid and hypothyroid patients with HT exhibited a higher systemic inflammation index than the control group. The pan-immune inflammation index was lower in controls than in euthyroid, hypothyroid, and hyperthyroid patients with HT. In patients with HT, inflammation markers did not significantly differ between subgroups.
Conclusions
Markers of systemic inflammation provide meaningful and reliable information in patients with HT, but do not differentiate between euthyroid, hypothyroid, or hyperthyroid patients.
Keywords
Introduction
Hashimoto’s thyroiditis (HT), also known as chronic lymphocytic thyroiditis, autoimmune thyroiditis, or struma lymphomatosa, is a chronic organ-specific inflammatory, autoimmune disease that was first described in 1912, and is among the most common causes of hypothyroidism. 1 HT is more prevalent in women, with approximately 2–4% of women and up to 1% of men being affected worldwide, and the prevalence increases with age. The rate of new cases is 0.3–1.5/1000 per year and HT is mostly observed in women between 30 and 50 years of age. 2
Hashimoto’s thyroiditis is an inflammatory condition that affects the thyroid gland, with patients developing clinical thyroid dysfunction according to the duration of disease. HT causes atrophy of the thyroid parenchyma through autoimmune processes and chronic inflammation. 3 Hemogram-derived inflammatory indices are associated with the inflammatory burden in various inflammatory conditions, such as autoimmune disorders and thyroid disorders. Therefore, it is reasonable to examine markers of systemic inflammation in HT. Studies have shown that HT-related inflammation may not be limited to the thyroid gland and may trigger a systemic inflammatory process, even in patients with normal thyroid function. It has also been revealed that there is a significant relationship between HT and systemic inflammatory load. Platelet-to-lymphocyte ratio (PLR), neutrophil-to-lymphocyte ratio (NLR) and C-reactive protein levels have been investigated as markers of systemic inflammation in HT. In recent years, new markers have emerged for evaluating systemic inflammation, such as the systemic inflammatory index (SII) and pan-immune inflammation index (PII), however, studies examining the relationship between SII and PII in HT are limited.4–10
The aim of the present study was to investigate NLR, PLR, SII and PII as markers of systemic inflammation in HT, and to compare systemic inflammation markers in euthyroid, hypothyroid and hyperthyroid patients with HT.
Patients and methods
Study population and design
This cross-sectional observational study was approved by Firat University Non-Interventional Research Ethics Committee (Date: 21 April 2022; Session No. 2022/06-04), and the study was conducted according to the guidelines of the Declaration of Helsinki. All participants provided written informed consent. STROBE guidelines were followed in preparing this article. 11 Consecutive patients diagnosed with HT, who were admitted to the hospital general surgery outpatient clinic between January 2020 and June 2023 were enrolled into the study. Healthy volunteers were recruited from patients attending the outpatient clinic for other reasons.
The diagnosis of HT was confirmed in all patients by an endocrinologist, and patients with HT were divided into euthyroid, hypothyroid, and hyperthyroid subgroups according to thyroid-stimulating hormone (TSH) and free thyroxine (T4) levels. Thyroid function and thyroid autoantibodies (anti-thyroid peroxidase antibody [TPO-Ab], and anti-thyroglobulin [Tg-Ab] antibodies) of healthy controls were assessed by an endocrinologist to exclude thyroid disease. Normal thyroid values in our laboratory were as follows: TSH, 0.25–4.2 IU/ml; free triiodothyronine (T3), 2.0–4.4 pg/ml; free T4, 0.86–1.76 ng/dl; Tg-Ab, 0–4 IU/ml; and TPO-Ab, 0–10 IU/ml.
Patients with acute and chronic infections, recent use of antibiotics and anti-inflammatory drugs within the last 1 month, pregnancy, chronic disease (diabetes, hypertension, autoimmune diseases), hematologic disease, malignancy, and/or recent steroid use within the last 6 months were excluded from the study. Data regarding participants’ biological sex and age were extracted, but smoking status was not included, as relevant data could not be extracted through the hospital registration system.
The sample size was calculated using open-access Web-Based Sample Size & Power Analysis Software (biostatapps.inonu.edu.tr/WSSPAS/). Onalan et al. 7 reported NLRs of 2.43 ± 0.94 and 2.11 ± 0.81 in patients with HT and healthy controls, respectively. The minimum sample size required to identify a significant difference using this test should be at least 119 in each group (238 in total), given a type I error of 0.05 (alpha), a power of 0.8 (1–beta), an effect size of 0.36 and a two-sided alternative hypothesis.
Biochemical assays
Peripheral blood samples were collected from all participants after overnight fasting. Blood parameters (complete blood count, white blood cells, hemoglobin, platelets, lymphocytes, neutrophils, and monocytes), and TSH, free T3, free T4, TPO-Ab, and Tg-Ab were determined using the ADVIA Centaur® XPT Immunoassay system autoanalyzer and associated reagents (Siemens Healthcare GmbH, Erlangen, Germany), according to the manufacturer’s instructions.
Inflammatory markers
The PLR, NLR, SII, and PII values were calculated from platelet, neutrophil, monocyte, and lymphocyte counts. The calculation formula for each indicator was as follows: PLR = platelet count (109/L)/lymphocyte count (109/L); NLR = neutrophil count (109/L)/lymphocyte count (109/L); SII = platelet count (109/L) × neutrophil count/lymphocyte count (109/L); PII =neutrophil count (109/L) × platelet count (109/L) × monocyte count (109/L)/lymphocyte count (109/L).
Statistical analyses
Categorical data are presented as frequency (percentage) and continuous data are presented as median (minimum–maximum). Statistical analyses were performed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA). Shapiro–Wilk test was used to examine the distribution of continuous data. Between-group differences in categorical data were assessed with Pearson’s χ2-test. Kruskal–Wallis test was used to compare more than two independent groups of continuous data that were not normally distributed. The relationship between two continuous variables was assessed with Spearman’s rank correlation coefficient. A P value < 0.05 was considered statistically significant.
Results
This study included a total of 392 participants, of whom 70 were male and 322 were female. Of the participants, 268 were patients with HT (45 male and 223 female), divided into euthyroid (n = 131), hypothyroid (n = 83), and hyperthyroid (n = 54) subgroups, and 124 were healthy controls. No difference was noted in median age between the control and patient groups (P = 0.314), however there was a statistically significant difference in gender between the groups, with a higher proportion of female participants, particularly patients in the euthyroid HT group (P = 0.004). Median TPO-Ab and Tg-Ab values were significantly higher in all patients with HT compared with the control group (P < 0.001). A comparison of the study population demographic, hematologic, and thyroid function data is presented in Table 1.
Baseline characteristics of 268 patients with Hashimoto’s thyroiditis (HT) and 124 healthy controls.

Data presented as frequency (percentage) or median (min–max).
Ab, antibody; TSH, thyroid-stimulating hormone; T3, triiodothyronine; T4, thyroxine; TPO, thyroid peroxidase; TG, thyroglobulin.
P = 0.002 versus control; bP < 0.001 versus control; cP < 0.001 versus euthyroid group; dP < 0.001 versus hypothyroid group; eP = 0.004 versus control; fP = 0.013 versus euthyroid group; gP = 0.001 versus control; hP = 0.023 versus control; iP = 0.018 versus control; jP = 0.009 versus euthyroid group; kP = 0.002 versus hypothyroid group; lP = 0.016 versus euthyroid group; mP = 0.008 versus control. Pearson’s χ2-test (categorical data) or Kruskal–Wallis test (continuous data).
NS, no statistically significant between-group differences.
Inflammation markers showed significant variations between healthy controls and subgroups of patients with HT. The median PLR value was higher in the control group than in euthyroid patients with HT (P = 0.001). The median NLR value was lower in the control group than in euthyroid (P < 0.001), hypothyroid (P < 0.001), and hyperthyroid (P = 0.013) patients with HT. Euthyroid and hypothyroid patients with HT had higher median SII values than the control group (both P < 0.001). The median PII value was lower in the control group than in euthyroid (P = 0.011), hypothyroid (P < 0.001), and hyperthyroid (P = 0.013) patients with HT. Inflammation markers did not differ significantly between the subgroups of patients with HT (Table 2).
Comparison of inflammation markers between patients with Hashimoto’s thyroiditis and healthy controls.
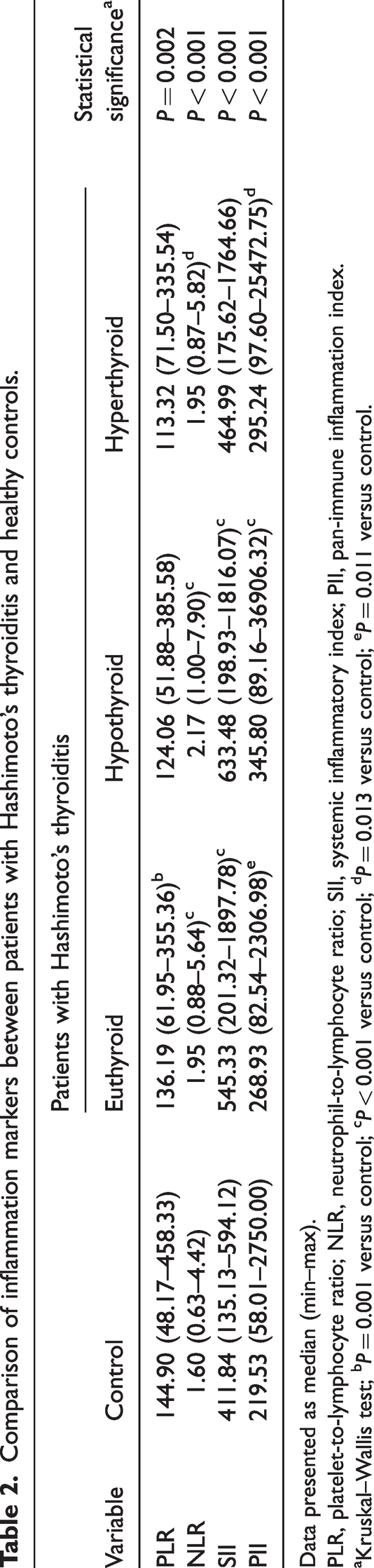
Data presented as median (min–max).
PLR, platelet-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio; SII, systemic inflammatory index; PII, pan-immune inflammation index.
Kruskal–Wallis test; bP = 0.001 versus control; cP < 0.001 versus control; dP = 0.013 versus control; eP = 0.011 versus control.
In the healthy control group, positive significant correlations were found between TPO-Ab values and PLR (r = 0.197; P = 0.028), SII (r = 0.180; P = 0.046) and PII (r = 0.327; P < 0.001). In addition, there was a significant positive correlation between PLR and TPO-Ab values in hypothyroid patients with HT (r = 0.231; P = 0.035). No correlations were found between TPO-Ab and TG-Ab levels and inflammatory markers in euthyroid and hyperthyroid patients with HT (Table 3).
Correlation between continuous variables in healthy controls and in euthyroid, hypothyroid and hyperthyroid patients with Hashimoto’s thyroiditis.

Ab, antibody; TPO, thyroid peroxidase; TG, thyroglobulin; PLR, platelet-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio; SII, systemic inflammatory index; PII, pan-immune inflammation index.
NS, no statistically significant correlation (P > 0.05; Spearman’s rank correlation coefficient).
Discussion
Many recent studies have reported that numerous, easily accessible and cost-effective hematological parameters, and the serum systemic inflammatory response markers calculated from them, may be used as clinical prognostic markers in a wide range of malignant and non-malignant diseases. 6 These markers express the systemic inflammatory burden of the disease in question. HT causes systemic inflammation at the cellular level leading to hypothyroidism in the long term, due to inflammation. Thyroid functions may be hyperthyroid, euthyroid or hypothyroid, and the status of inflammation parameters in patients during these processes is a matter of debate. 12 In the present study, no significant differences in inflammatory markers were observed between these three thyroid states.
In various studies, NLR and PLR levels have been evaluated primarily in terms of systemic inflammation. HT is characterized by inflammation, and NLR is reported to be increased in inflammatory conditions, including inflammatory bowel disease, diabetes, gastrointestinal diseases, and heart conditions. Similarly, high PLR levels have been reported in thyroiditis, cancer, diabetes, irritable bowel disease and Covid-19 infection. It has been suggested that these parameters may be used in diagnosing patients with HT and in determining the severity of disease.7,13–21 Comparable to these previously published data, NLR was found to be significantly increased in all three groups of patients with HT compared with healthy controls. The PLR value was statistically significantly lower in patients with euthyroid HT compared with the control group.
Some studies have shown no relationship between the above inflammation values and HT.12,22,23 For example, in a study that compared overt and subclinical hypothyroidism groups with controls, NLR values were found to be similar in all groups. 22 Another study reported that NLR and PLR levels were similar in patients with hypothyroidism and healthy controls, and that there was a positive correlation between these two markers. 23
In addition to NLR and PLR, two further inflammatory markers, SII and PII, have been identified, and a limited number of studies in the literature have evaluated these two markers in patients with HT. The SII is a composite index based on peripheral blood lymphocyte, neutrophil, and platelet counts (SII = platelet count ×neutrophil/lymphocyte count), and is considered a stable and comprehensive indicator of the body’s local immune response and systemic inflammatory status. The SII has been previously shown to predict the prognosis of tumor patients by reflecting the balance between the body’s inflammatory and immune responses. 24 Additionally, the SII has been linked to gestational diabetes and diabetic kidney disease. 25
The SII has been studied in differentiated thyroid cancer and was found to be significantly higher in patient than in controls, and the SII is higher in patients with differentiated thyroid cancer than in the healthy population. High SII values may be attributed to multifocalism.26,27 In a study conducted in patients with subacute thyroiditis, the SII was found to be significantly higher in these patients than in the control group. 28 The present study also showed that SII values were significantly higher in patients with subacute thyroiditis. The median SII values of patients with euthyroid and hypothyroid HT were statistically significantly higher than the control group.
Significant negative correlations have been found between the SII and free T3 and free T3/free T4, and significant positive correlations between the SII and total T4, 24 however, no such correlations were observed in patients with HT in the present study.
The PII was first described by Fuca et al. 29 as an immune-inflammatory biomarker in colorectal cancer that correlates strongly with the overall prognosis of patients with metastatic colorectal cancer and outperforms other well-established biomarkers. 29 The present authors found no published studies evaluating the effectiveness of the PII in patients with malignant or benign thyroid disease. In another meta-analysis including 4000 cancer patients with different localizations, the PII was reported to be a reliable prognostic marker.29,30 In the present study, PII values were higher in all three HT patient groups than in the control group, and this increase was statistically significant.
Conclusions
In conclusion, biomarkers of systemic inflammation in patients with HT, such as the recently identified SII and PII, offer more reliable information due to their derivation from a broader range of hematologic parameters. In the present study, even in HT patients with chronic inflammation resulting in hypothyroidism, no significant difference was observed in systemic inflammation parameters. Further prospective studies with larger study populations are required for these parameters to acquire a prognostic value.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241280049 - Supplemental material for Evaluation of systemic inflammation markers in patients with Hashimoto’s thyroiditis
Supplemental material, sj-pdf-1-imr-10.1177_03000605241280049 for Evaluation of systemic inflammation markers in patients with Hashimoto’s thyroiditis by Ahmet Bozdag and Pinar Gundogan Bozdag in Journal of International Medical Research
Footnotes
Author contributions
Conceptualization, AB and PGB; methodology, PGB; software, AB; validation, PGB.; formal analysis, AB; investigation, PGB; resources, AB; data curation, PGB; writing – original draft preparation, AB; writing – review & editing, PGB; visualization, AB; supervision, AB; project administration, PGB; and funding acquisition, AB. Both authors have read and agreed to the published version of the manuscript.
Data availability statement
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant form any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.