
Abstract
While chronic lung disease causes substantial global morbidity and mortality, global estimates have primarily been based on broad assumptions. Specific country data from low-income countries such as Nepal are limited. This review assessed primary evidence on chronic respiratory disease burden among adults in Nepal. A systematic search was performed in June 2019 (updated May 2020) for studies through nine databases. High levels of heterogeneity deemed a narrative synthesis appropriate. Among 27 eligible studies identified, most were low-moderate quality with cross-sectional and retrospective study design. Chronic lung diseases identified were chronic obstructive pulmonary disease (COPD), asthma, bronchiectasis and restrictive lung diseases. Studies were categorised as: (i) community-based, (ii) hospital-based and (iii) comorbidity-related and disease burden. Reported disease prevalence varied widely (COPD, 1.67–14.3%; asthma, 4.2–8.9%). The prevalence of airflow obstruction was higher among rural dwellers (15.8%) and those exposed to household air pollution from domestic biomass burning as opposed to liquid petroleum gas users (Odds Ratio: 2.06). Several comorbidities, including hypertension and diabetes mellitus added to the disease burden. The review shows limited literature on lung disease burden in Nepal. Publications varied in terms of overall quality. Good quality research studies with prospective cohorts related to respiratory conditions are required.
Introduction
The burden of chronic lung disease worldwide is huge, both in terms of morbidity and mortality. It is increasing and the current COVID-19 pandemic is likely to add further. Just one lung non-communicable disease (NCD), chronic obstructive pulmonary disease (COPD), causes >3 million deaths per year globally, >90% of these occurring in low to middle-income countries (LMICs). 1,2 Globally identified risk factors in LMICs include tobacco smoke, household and ambient air pollution, and occupational exposure. 3 –8 The risk factors for developing chronic lung diseases will vary from country to country. The Himalayas contain several LMICs, many of which share geographical and cultural features. We chose Nepal as an exemplar Himalayan LMIC, with a population of circa 30 million and the 16th poorest country worldwide. Figures on disease prevalence for Nepal have been reported as part of the Global Burden of Disease project, these are primarily based on modelled data and are therefore dependent upon broad assumptions that may lack accuracy. 9 Reportedly, NCDs in Nepal account for 66% of mortality, of which chronic respiratory diseases are ranked as the second highest cause of death (10%), alongside cardiovascular diseases (30%) and cancer (9%). 10 The gravity of chronic respiratory diseases in Nepal was highlighted recently, with estimates second worse only to Kazakhstan for global mortality (Kazakhstan: 114.28 versus 100.75 deaths in Nepal per 100,000). 11,12
Respiratory disease greatly impacts health service demand in Nepal through hospitalisations. 13 –15 According to the 2016–2017 Department of Health services in Nepal, bronchial asthma and COPD were the second and third most common causes of outpatient department morbidity, with cardiovascular conditions as the leading cause. 12 Many patients reported having more than one long-term health condition.
Within Nepal, risk factors for chronic respiratory diseases vary according to gender and geographical location. Over 80% of the population lives in rural settings where a large proportion uses biomass as a source for heating and cooking fuel within poorly ventilated living quarters, with exposure to high levels of household air pollution. 16,17 As women generally do the cooking, this disproportionately affects them. Smoking is common, particularly in men (27% vs 6% in women) and in urban areas (30% of households); in addition, there is significant ambient, agricultural, and industrial pollution. 17 –20 These exposures do not only affect respiratory disease but also contribute to other health complications and socioeconomic burdens. 6,21 The remoteness of some rural locations hinders alternative energy sources and restricts fuel choices. Other socio-demographic factors, including illiteracy, poverty, distance and remote access to healthcare facilities, also have an adverse impact on health. 8,22
The government of Nepal has begun taking action with policies including the development of the Integrated NCDs Prevention and Control Policy of Nepal and the Multisectoral Action Plan for the Prevention and Control of Non-Communicable Diseases (2014–2020). 23 However, innovative health systemic structures and a comprehensive understanding of the burden of diseases are required for effective implementation. 24 This systematic review aims to synthesise the current available evidence across community and hospital settings on the prevalence of chronic respiratory disease (excluding cancer), respiratory symptoms, lung function and lung-related burden in Nepal.
Methods
Search strategy
Initial scoping in May 2019 through MEDLINE, Embase, Cochrane library and manually, identified no existing systematic reviews on this area.
The protocol was registered with PROSPERO (CRD42019138552). 25 Database searches were conducted in June 2019 and updated in May 2020 for publications, with no date restrictions. Nine electronic databases were searched: Ovid (MEDLINE, Embase, Global Health, CAB Abstracts), CINAHL, Scopus, Web of Science, Cochrane Library and Nepal Journal Online (NEPJOL). Grey literature searches were conducted, including Nepal Government/Health Ministry reports, World Health Organisation (WHO) data and OpenGrey. Searches were supplemented by contact with study authors where additional information was required as well as forward and backward citation tracking from included studies. A sample search strategy is shown, Appendix 1.
Study screening and selection
Study designs reporting quantitative population-level prevalence or incidence of chronic respiratory disease, lung function, respiratory symptoms or burden of lung disease in adults (individuals aged 16 years and older) living in Nepal were considered. The review included only peer reviewed publications, but grey literature set the scene in the introduction. Language was not an exclusion criterion. For this review, publications studying specific occupational exposure were excluded. Conference abstracts were excluded following screening for full-text peer-reviewed publications.
Study records identified were exported into Mendeley (London, UK), with duplicates removed. Titles and abstracts were screened by two independent reviewers (WE, CEB). Full texts of potentially eligible papers were retrieved and assessed independently by two reviewers with discrepancies resolved through discussion. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 26 flow diagram of the search and screening process is shown in Figure 1.

PRISMA flow chart of included studies.
Data extraction and quality assessment
A standardised data extraction form was used for the final selection of studies. Data were extracted by one reviewer and checked for accuracy by a second reviewer. Quality of the included studies was independently assessed by two researchers from WE, ARJ and CEB using the AXIS critical appraisal checklist for cross-sectional studies. 27 In keeping with the AXIS method, the quality is not judged as a numerical scoring of the component parts and therefore has a subjective element.
Data synthesis
Studies were highly heterogeneous with huge variation used for data acquisition, analysis and reporting. Therefore the pre-planned meta-analysis was not possible (see PROSPERO: CRD42019138552), and the findings were synthesised narratively. 28 Early on, it became apparent that the review would be in three distinct sections, given the heterogeneity of sites in the manuscripts: i) community setting, ii) hospital (mostly inpatients) setting and then iii) comorbidity-related and lung-related burden of disease.
Results
Study selection
A total of 6,393 papers were identified. Followng removal of duplicates, 4,252 studies were screened by titles and abstracts, and 121 full-text studies reviewed (Figure 1), with 27 articles included (Tables 1 –3).
Community-related chronic respiratory disease prevalence studies.

Airway Obstruction (AO), Confidence Interval (CI), Chronic Obstructive Pulmonary Disease (COPD), Indoor Air Pollution (IAP), Lower Limit of Normal (LLN), Peak Expiratory Flow Rate (PEFR), Forced Expiratory Volume in one second (FEV1 ), Forced Vital Capacity (FVC), Forced Expiratory Flow at 25–75% of FVC (FEF, Standard Error (SE)).
Hospital-related chronic respiratory disease studies.

Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD), Chronic Obstructive Pulmonary Disease (COPD), Non-Communicable Disease (NCD), Interstitial Lung Disease (ILD), Idiopathic Pulmonary Fibrosis (IPF).
Comorbidity-related and burden of chronic respiratory disease studies.
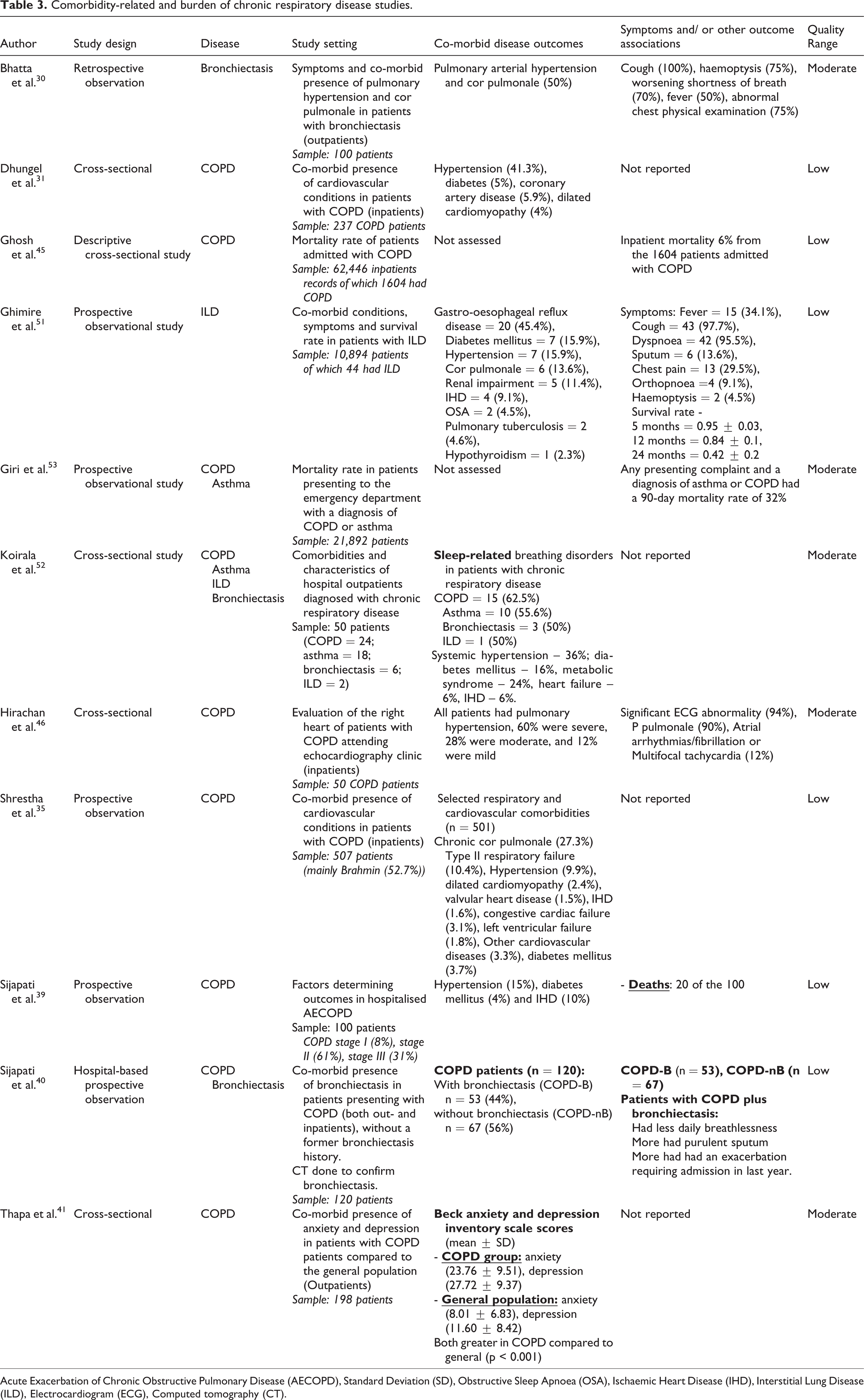
Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD), Standard Deviation (SD), Obstructive Sleep Apnoea (OSA), Ischaemic Heart Disease (IHD), Interstitial Lung Disease (ILD), Electrocardiogram (ECG), Computed tomography (CT).
Overview of included studies
Years of publication ranged from 1984 to 2019, and all were published in English. One was published in the 1980s, 29 7 between 2000 and 2010, 30 –36 and 19 after 2011. 20,37 –54 All included studies were cross-sectional, direct observations of clinical notes, comparative and single point survey designs. 20,29 –54 The studies reported on diseases (usually self-reported), symptoms, related health conditions and lung function. Most of the studies were either of low (n = 13) or moderate (n = 12) quality, with two classed as high quality.
Some studies reported on more than one condition, with the major diseases identified being: COPD (22 studies), 31,32,34 –36,38 –54 asthma (8 studies), 20,32,36,37,49,52 –54 bronchiectasis (2 studies and as a co-morbidity in one), 30,40,52 restrictive lung diseases (3 studies), 49,51,52 and ‘chronic bronchitis’ (1 study). 29
Symptoms reported included chronic cough, phlegm or sputum production, breathlessness or shortness of breath, chest tightness, wheezing, dyspnoea and sore throat. Reporting included presence of pulmonary arterial hypertension 30 and cor pulmonale. 29,30,35,51,52
Lung function was reported in seven studies, 29,32,33,38,47,48,51 and data presented across different spirometric measures, with one reporting proportions only of patients categorised as ‘normal’, ‘obstruction’ and ‘restriction’. 51
Community-based prevalence studies
Studies included over 18,000 participants across diverse population groups (Table 1). COPD and asthma, (usually self-reported), were covered across small-medium sized studies of 78 to 401 participants, 20,32,36 –38 with one large-scale study of 12,557 participants (prevalence determined in 11,277). 50 A study of chronic bronchitis, according to the Medical Research Council definition, was based on 2,826 participants. 29
One study on both rural and urban households reported a COPD prevalence of 14.3%. 36 This was comparable with the findings of Dhimal et al., 50 which reported a nationwide prevalence of COPD of 11.7%. These findings differed from other studies, where reported COPD prevalence was 1.67% in rural adult kitchen dwellers (reported in the paper as adults who spend a large amount of the day in the kitchen), 32 and 6% COPD prevalence in rural community residents using biomass fuels. 38 Meanwhile, prevalence of chronic bronchitis of 18.3% was reported in a study with an additional 3.1% with emphysema too. 29 Asthma prevalence ranged from 4.2% to 8.9% 20,32,36 but one study reported 25.4% in adults ≥60 years. 37 Generally, chronic respiratory diseases were more prevalent in adults aged over 40 years. 37,38,50
In a general representative population, symptom-wise, one study reported cough, phlegm, breathlessness and wheezing to each have a prevalence of over 20%, and greater among populations using unprocessed fuels and living in rural regions, than in those using processed fuels and living in urban households. 36 This agreed with Ranabhat et al., 20 where reported breathlessness and productive cough were 27.3% and 19.7% of individuals living in rural communities exposed to household air pollution. Kurmi et al. 47 reported that wheeze (male, 23.5% vs 8.7%; female, 32% vs 10.3%) and dyspnoea (male, 12% vs 2.5%; female, 17.8% vs 7.6%) were more prevalent symptoms in the rural environment as a whole, whereas chronic phlegm (male, 4.7% vs 5.3%; female, 4.4% vs 4.2%) and cough (male, 3% vs 12.9%; female, 4% vs 5.8%) were more comparable between rural and urban environments. 48 Symptom reporting was also greater in current and past smokers than never smokers, with the prevalence of cough, phlegm, breathlessness and wheezing all above 11% in rural community kitchen dwellers as a whole. 32
Kurmi et al., 47,48 a large study, reported across two publications that the odds ratio of having airflow obstruction with exposure to biomass was two times higher (OR: 2.06) 47,48 compared to liquid petroleum gas users. Males (OR: 1.94; p = 0.035) were more at risk of suffering airflow obstruction after exposure to biomass (OR: 1.30; p = 0.436) when the threshold of FEV1/FVC < 0.70 was utilised but not for a threshold of FEV1/FVC < lower limit of normal (Males, OR: 1.11, p = 0.840; Females, OR: 1.67, p = 0.281). Airflow obstruction was reported in 15.8% of rural community residents using a subset representative of the overall study population, with airflow obstruction prevalent in 57.4% among those meeting the study criteria for chronic bronchitis. 29 Smokers had lower lung function in one study compared to those who reported to not smoke, although it was unclear whether this comparator group were ex- or never smokers 33 . Pratali et al. 38 found that 54% of rural community residents using biomass fuels had a FEF25 – 75 < 80% predicted. Joshi et al. 32 reported absolute peak flow and not % predicted, and therefore is largely uninterpretable.
Hospital-based studies
Ten studies, including a total of 111,188 subjects reported on the prevalence of chronic respiratory diseases in a hospital setting (Table 2). 31,34,42 –45,49,51,53,54 The majority of studies reported on COPD among hospitalised patients, 31,34,42 –45 with other studies reporting on interstitial lung disease (ILD), 51 both COPD and asthma, 53,54 and outpatient spirometry referrals. 49
Overall estimates for the proportion of admissions due to COPD varied widely from 2.6% to 14% in studies including all hospital admissions and up to 17.3% in medical wards. 31,42,43,45 Two studies reported that among hospitalised participants with an NCD, 43–45% were COPD patients. 42,43 In two studies, the majority of hospitalised COPD patients were females (60%). 42,44
One study reporting on dyspnoea admissions (this being 9% of all the admissions) at one hospital, identified that 52.3% received a respiratory diagnosis for that presentation, another 13% had a combined respiratory and cardiovascular cause, and 9.3% received a diagnosis of respiratory accompanied with other complications. 54 However, dyspnoea was also due to metabolic (11.2%), neuropsychiatric (6.7%) and cardiovascular alone (3.7%). 54 In a study where the majority of hospital admissions were attributed to injuries in young adults, respiratory complaints still accounted for 9.2% of total hospital admissions, with COPD or asthma accounting for 0.5% of total hospital admissions. 53
Ghimire et al. 51 reported a prevalence of 0.4% for ILD among patients treated in hospital for pulmonary disorders. The majority of these ILD’s were attributed to idiopathic pulmonary fibrosis (79.5%), and 68.1% of the patients were over the age of 60 years. 51
There was only one hospital-based study with spirometry for outpatients: the final diagnoses being bronchial asthma (24.2%), COPD (31.4%), and restrictive lung disease (8.1%) of those referred for testing. 49
Comorbidity-related and burden of disease
Eleven studies, with a total of 96,594 patients reported on comorbidity and burden of chronic respiratory disease. 30,31,35,39 –41,45,46,51 –53 The major chronic respiratory diseases were COPD (seven studies), 31,35,39 –41,45,46 bronchiectasis (one study), 30 ILD (one study), 51 COPD or asthma (one study), 53 or they assessed COPD, asthma, bronchiectasis and ILD together (one study) (Table 3). 52 Reported comorbidities covered other respiratory conditions, endocrine, cardiovascular disease, sleep and mental health disorders.
Common comorbidities reported in patients with COPD were hypertension ranging 9.9–41.3% of subjects, 31,35,39 diabetes mellitus: 3.7–5%, 31,35,39 ischaemic heart disease/coronary artery disease: 1.6–10%, 31,35,39 dilated cardiomyopathy: 2.4–4%, 31,35 chronic cor pulmonale: 27.3%, 35 and type II respiratory failure: 10.4%. 35 One study in patients with COPD who had echocardiography reported that all had echocardiography evidence of pulmonary hypertension, of which 60% were severe. 46 Another study reported a co-morbid presence of bronchiectasis in 44% of COPD patients. 40 Anxiety and depression were almost three times more common in COPD patients compared to the general population. 41
One study reported that patients with an initial diagnosis of ILD had a 45.4% prevalence of gastro-oesophageal reflux disease, 15.9% diabetes mellitus, 15.9% hypertension, 13.6% cor pulmonale, 11.4% renal impairment, and 9.1% ischaemic heart disease. 51 Systemic hypertension (36%), diabetes mellitus (16%), metabolic syndrome (24%), ischaemic heart disease (6%) and heart failure (6%) were prevalent across multiple chronic respiratory diseases (COPD, ILD, bronchiectasis and asthma). 52 Two studies reported on sleep disorders with Ghimire et al. 51 reporting obstructive sleep apnoea prevalence in 4.5% of ILD patients, while Koirala et al. 52 reported that 62.5% of COPD and 55.6% of asthma patients had sleep-related breathing disorders.
Two studies reported mortality rates ranging from 6–20% in patients admitted to hospital with COPD. 39,45 Another study reported a 90-day mortality rate of 32% for patients admitted to the hospital with any complication with an accompanying diagnosis of COPD or asthma. 53 The prevalence of an exacerbation requiring hospitalisation was nearly double in COPD patients with coexistent bronchiectasis compared to those without (56.6% vs 26.8%). 40 Ghimire et al. 51 reported survival rates of 95% at 5 months, 84% 1-year, and 42% 2-year following ILD diagnosis.
In patients with bronchiectasis or ILD, common symptoms experienced included cough (bronchiectasis, 100%; ILD, 97.7%), haemoptysis (bronchiectasis, 75%; ILD, 4.5%), worsening shortness of breath (bronchiectasis, 70%; ILD, 95.5%), and fever (bronchiectasis, 50%; ILD, 34.1%). 30,51
Discussion
This study has identified and synthesised the available evidence on the prevalence of chronic respiratory diseases, symptoms, lung function, comorbidities and the overall burden of lung disease in Nepal. Overall, COPD is common, both in males and females, and is associated with frequent hospital admission and a range of comorbidities. Smoking and household air pollution were found to be common risk factors. Estimates of asthma prevalence varied widely and there was no good data on the ILD prevalence.
Community-based findings
The findings highlight the high prevalence of COPD and the varied prevalence of asthma in Nepal. The global prevalence of COPD has been reported to be approximately 9.2%, 55 with other estimates suggesting age-standardised figures for prevalence of males: 3.2% and females: 2.0%. 56 In comparison, large-scale and high quality studies assessing COPD prevalence in representative samples of the overall population in LMIC’s such as China and India have shown prevalence to be 8.6% 57,58 and 4.2% respectively. 59 The prevalence estimates of 1.67% to 14.3% in Nepal vary significantly on either side of these prevalence figures, making it challenging to draw meaningful comparisons. As with COPD, asthma prevalence figures for Nepal varied widely depending on the population, rendering it difficult to interpret alongside World Health Surveys and findings from other LMICs where prevalence of diagnosed asthma have been estimated at 4.3% 60 and 2.9% respectively. 59 However, both asthma and COPD prevalence figures could be impacted by the misclassification of disease and by the lack of quality studies. To date, most publications reporting COPD diagnosis in Nepal are not based on spirometry, and where they are, they did not assess post-bronchodilator measurements. 61 Similarly, the term ‘COPD’ is not universally recognised in Nepal, and therefore there is further misclassification of patients as having asthma or other terms for chronic lung disease. This review highlights that the large proportion of the prevalence studies were of moderate to low-quality evidence and utilised diverse populations and approaches.
Two publications from the same large project met the criteria for high quality. 47,48 The use of biomass fuels as a household energy source markedly increased the risk of airflow obstruction compared to liquefied petroleum, 47 in line with the Global Burden of Disease study and other studies. 62 –65 Further, symptoms are prevalent in both urban and rural community dwellers, but particularly in rural, where there is greater use of biomass fuels leading to household air pollution. 48 These observations agree with previous findings. 66,67 However, some recent evidence contradicts the lung function observations, whereby post-bronchodilator airflow obstruction was not associated with the use of biomass fuels. 68
Hospital-based findings
In the hospital setting, the estimates of COPD and asthma also varied across studies. The reporting of hospital admissions attributed to COPD and/or asthma in Asian LMICs is scarce in the literature providing challenges in making effective comparisons. Of the available evidence, a study looking into hospital admission causes in China reported that chronic respiratory disease contributed to 22.6% of total admissions. 69 Dagenais et al. 70 further suggested that respiratory disease patients accounted for around 8.5% of global hospital admissions, but the number of first admissions attributed to respiratory disease was higher (4.9%) in high income countries compared to LMIC (1.9%). It was suggested that this was due to higher diagnosis rates and earlier treatment in high income countries. 70
Of note, two studies highlighted that most hospitalised COPD patients were female. 42,44 This conflicts evidence from other LMICs whereby hospital admissions for COPD appear to be more males, 71,72 and prevalence rates of COPD are higher in males. 58,73 This finding is of potential importance in addressing the burden of COPD in Nepal and needs to be investigated further. One possibility is the greater exposure of women to household air pollution.
It is important to note that drawing comparisons with other countries based on the low to moderate quality data are hindered by the disparities in reporting of admissions, including whether total hospital admissions, select age groups or select hospital departments and also the hospital location and access. All these factors hinder interpretation, especially when the studies tend to include large hospital centres in urban areas. This creates challenges in providing evidence relating to rural environments.
Comorbidity-related and burden findings
A high prevalence of concurrent comorbidities included other respiratory disorders, 35,40,51,52 cardiovascular disease, 31,35,39,46,51,52 diabetes, 31,35,39,51,52 anxiety and depression. 41 The estimates of prevalence varied markedly. Although these were small and discrete populations, the coexistent comorbidities concur with the literature in other countries and warrant further investigation and studies to delineate the additive burden, contribution to mortality, opportunity for earlier identification and prevention. 74,75
There was minimal literature on mortality associated with chronic respiratory disease. For COPD, in-hospital mortality rates ranged from 6–20%, 39,45 which is a wide variation in the estimate. Comparisons may be drawn with COPD in-hospital mortality rates in India, which are around 12%, 72 but further clarity is needed to distinguish a precise estimate in Nepal. Access to hospital and possible later presentation with symptoms, healthcare costs and the provision and access of core medications and treatment once at the hospital are factors. There was no population-level COPD or other chronic lung disease mortality data for Nepal.
Strengths and limitations
This review included self-reported and diagnosed lung disease, symptoms, lung function and comorbidity, allowing capture on the wider burden of respiratory disease. Outcomes needed to be contextualised to study setting, allowing for adequate reflection for future research and policy utilisation and a rounded view of respiratory disease burden in both the community and hospital while highlighting variation and a need for further research.
The main limitation was the considerable heterogeneity in the studies in terms of population sampling approach and data collection methods leading to a variety of outcome measures and a range of information. There were stark differences in study quality stemming from design and setting, which make it necessary to separate the study into three categories. The populations recruited to these studies should also be considered with several elements identified that infer heavy bias, potentially affecting the interpretation of results. For example, lack of segregated data based on the age of the population monitored meaning standardised results could not be produced, lack of spirometry especially including post-bronchodilator assessments to determine the overall prevalence, lack of reporting on medications, lifestyle factors, previous medical history (e.g. childhood respiratory complications), and socioeconomic status to help interpret the populations included. It is also important to note that no data on incidence of chronic respiratory diseases were available for reporting, and that reported symptom data were not consistent. As a result, the high variability required a narrative analysis approach with details of the population presented as opposed to a pooled estimate of prevalence and burden. Ultimately, these issues made it difficult to compare studies but have helped to provide an evidence base for future research needs assessing non-communicable lung disease burden in Nepal.
Implications for future health research and care
While unable to fully delineate the estimates of the true prevalence of respiratory disease in Nepal, the scale and burden of chronic lung disease are marked. Current research is taking a population approach to systematically identify the scale of COPD in urban Nepal. 76 Identifying the estimates and burden of disease drives the need for optimised healthcare strategies and subsequent implementation and dissemination. For example, smoking cessation to reduce tobacco exposure 77 –79 and pulmonary rehabilitation 77 have a strong evidence base in their effectiveness in managing lung diseases. Pulmonary rehabilitation takes a holistic approach to reduce breathlessness, improve function and treat multimorbidity. 80 Importantly, these are high value, low-cost interventions and will be of an increasing need for a country with an increasing life expectancy and a growing issue of NCD prevalence. Reducing exposures through smoking cessation and utilisation of alternative fuel sources alongside health promotion are key to the long-term management and prevention of chronic respiratory diseases in Nepal. However, any consideration and inclusion of public health interventions needs a full evaluation of their potential appropriateness and acceptability given the tremendous social, cultural, linguistic, economic and geographic diversity of Nepal. Important factors include the fact that a large proportion of people in Nepal live in very rural and often mountainous terrain, many are living in extreme poverty and illiteracy is high. 8,16,17,22
Conclusion
This systematic review demonstrated that there is limited published literature on the burden of lung disease and marked variation in outcome measures and populations studied. Nonetheless, chronic respiratory burden in Nepal is likely to be considerable. This is a priority area for future research. Based on the available information, there is a clear need for further studies and the need for healthcare professionals, providers and policymakers to develop effective strategies to tackle chronic respiratory diseases in Nepal. These findings are also likely to be relevant to other Himalayan LMICs.
Footnotes
Author contributions
WE and ARJ are joint first authors. The original study was devised by CEB, IPH and RK. Design of the study was by CEB, IPH and WE. WE, ARJ and CEB conducted literature review and main analysis. WE and ARJ wrote the first manuscript draft. All authors contributed and critiqued the manuscript and approved the article before submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The systematic review was supported by the “Global Challenges Research Fund”, University of Nottingham 2018-2019. CEB & IPH report grants from the Global Challenges Research Fund during the conducting of this review. WE, ARJ, CE, RK, & OPK declare to have no conflicts of interest relating to the production of this manuscript.