
Abstract
Background:
Effective asthma management requires a multidisciplinary approach that includes; the physician, the patient, and the patient’s family.
Objectives:
The current study aimed to assess the roles played by community pharmacists toward asthma control together with the barriers hindering their practice and possible strategies to overcome those barriers.
Methods:
A multi-centered cross-sectional study was conducted. Data was collected using a structured, self-administered questionnaire adapted from previously conducted studies and customized to fit with the current study setup. The collected data was cleaned, coded, and entered into Statistical Package for Social Sciences (SPSS) version 21 for analysis. Descriptive analysis of the collected data was conducted and the results were presented using frequency tables and graphs.
Results:
A total of 122 community pharmacy professionals; 63 from Gondar, 26 from Bahir Dar, 15 from Debre Markos, 14 from Woldia, and 4 from Debre birhan participated in the study. About 96 (78.7%) of the participants reported that they teach their patients the basic facts about asthma. More than two-thirds of the participants 85 (69.7%) also reported that they were able to identify and manage the triggering factors of asthma for their patients. Lack of pharmacist time was reported by 78 (63.9%) of the study participants as a major reason for the inadequacy of the counseling service provided.
Conclusion:
It appears evident that there is a need for continuing professional education and pharmacists to receive additional training to improve their ability to go beyond identifying a problem and suggesting therapeutic options.
Introduction
Asthma is a chronic inflammatory disorder of the airways characterized by paroxysmal or persistent symptoms, such as dyspnea, cough, wheezing, chest tightness, and sputum production. 1 It is a significant public health disorder affecting 1%–18% of the world’s population. 2
International guidelines were published to optimize the management of asthma. 3,4 However, asthma-related morbidity and mortality have remained high despite all these progressions. 5 These days, Asthma can be considered a condition that is not adequately managed, since death from its complications usually arises from preventable causes, such as poor treatment and observation. 6 Evidence showed that asthmatic patients do not take their preventive medications regularly. 7 The most commonly reported reasons for these were due to side effects, 7 socioeconomic factors, and low awareness. 8,9 Besides, regardless of regular utilization, evidences are suggesting that asthmatic patients fail to achieve the correct inhaler technique, health-care workers do not usually check inhaler technique, and inhaler technique declines over time. 10,11
Effective asthma management requires a multidisciplinary approach that includes; the physician, the patient, and the patient’s family. When asthmatic patients participate in their disease management, they attain better health outcomes. 12 –15 Asthma self-management was found an effective strategy to reduce asthma-related hospitalizations and emergency room visits, spontaneous physician visits, lost workdays, nocturnal asthma incidents, and improved use of beta-2-agonists and oral or inhaled corticosteroids. 16,17
Community pharmacists are the most accessible health-care professionals in the health-care system with their regular contact with patients due to the need for prescription refills, and their medication expertise, make them in an optimal position to positively impact on asthma management. 18,19 Many studies have shown the important roles that community pharmacists have played in the management of asthma 18,20 –25,26 –28 while others have identified barriers to pharmacists’ interventions, such as time constraints, physician cooperation, and patient awareness. 27,29,30 An insufficient number of skilled pharmacists and technicians, impediments to access physicians, and lack of reimbursement of money for certain interventions were also identified by other studies outside the field of asthma as common barriers to community pharmacists’ interventions. 31 –39
Pharmacists need to have the necessary knowledge and skills to teach patients to self-manage their asthma. Some of these skills include; how to recognize whether a patient’s asthma condition is controlled or uncontrolled, identify factors that are impeding a patient’s asthma control, identify patients with no emergency action plan, and discuss with the patient and his/her physician to develop a strategy to help improve the patient’s asthma control. Therefore, the present study aimed to assess the roles played by community pharmacists working in Gondar, Bahir Dar, Debre Markos, Woldia, and Debre birhan city toward asthma control together with the barriers hindering their practice and possible strategies to overcome those barriers.
Methods and materials
Study area and period
The study was conducted in five cities; Gondar, Bahir Dar, Debre Markos, Woldia, and Debre birhan which are all located in the Amhara regional state, Ethiopia. The Amhara regional state is the second most populous region of the 9 regions and two administrative cities in the country that covers an area of 154,709 km2. Bahir Dar is the capital of the region and is located at 565 km away from Addis Ababa (the capital city of the country) and the other study areas are located; Gondar 727 km, Debre Markos 302 km, Woldia 503 km and Debre Berhan 130 km away from the country’s capital. During the time of the study, there were 54 community pharmacies in Bahir Dar, 52 in Gondar, 30 in Debre Markos, 22 in Debre birhan, and 15 in Woldia respectively. The study was conducted from January 1 to March 30, 2019.
Study design
A multi-centered cross-sectional study was conducted to assess the roles played by community pharmacists toward asthma control together with the barriers hindering their practice and possible strategies to overcome those barriers.
Population
Source population
The source population includes all community pharmacists working in the five cities, namely; Gondar, Bahir Dar, Debre Markos, Woldia, and Debre birhan.
Study population
These include all community pharmacists working in the five cities that fulfill the inclusion criteria for the study.
Eligibility criteria
Inclusion criteria
Pharmacy professionals that had at least 6 months of work experience in a community pharmacy.
Exclusion criteria
Community pharmacy professionals that were not willing to participate in the study and those unavailable during the data collection period.
Sampling technique and sample size determination
As there was no recent data on the proportion of community pharmacists working in the five cities, the questionnaire was distributed based on the proportional number of community pharmacies found in the cities. In doing so, 5 pharmacies from each city were taken for the pilot study and thus were excluded. As such a total of 148 community pharmacies (49 pharmacies from Bahir Dar, 47 from Gondar, 25 from Debre Markos, 17 from Debre birhan, and 10 from Woldia) were taken. Based on these proportions a total of 200 questionnaires were distributed (66 to Bahir Dar, 64 to Gondar, 34 to Debre Markos, 22 to Debre birhan and 14 to Woldia City respectively.
Study variables
The major study variables in the current study were the major roles played by community pharmacists in educating asthmatic patients visiting their facility and these were analyzed with the different socio-demographic and professional related characteristics of the pharmacists.
Data collection procedures
Five data collectors were involved in the data collection procedure, each of them after being clarified on the purpose of the study as well as the data collection procedures. Data was collected using a structured, self-administered questionnaire adapted from previously conducted studies and customized to fit with the current study setup. 40 As there was no available data on the proportion of community pharmacists that were practicing in each of the five cities, all of the community pharmacists working in the abovementioned cities that fulfilled the inclusion criteria were invited to participate in the study after securing their verbal consent.
The questionnaire contained four parts and they were administered in the same manner to all of the study participants. The first part of the questionnaire includes the basic demographic characteristics of the respondents that are important factors to the current study (sex, educational qualification, and work experience). The second part contains dichotomous questions (“yes” or “no” questions) and multi-item questions; Do you educate patients on the basic facts about asthma? Can you identify and manage the triggers of asthma for the patients? Which asthmatic medications are widely prescribed (short-acting beta-2 agonist & Bronchodilator, Corticosteroid, Leukotriene modifiers, Anti-inflammatory)? Do you follow effective asthma management plan to ensure the patient is given written and verbal instructions that describe: When the patient should take his/ her drug, how the patient should take the drug, how much he/she should take? Do you educate asthmatic patients about the role of each medication? Do you explain the side effects and adverse drug reactions of a particular drug to patients? Do you ask patients about the medications other than the asthma medications he/she may be taking? Do you educate patients about the proper techniques of inhaled medications? The third and fourth part of the questionnaire includes questions that ask respondents the possible factors/barriers that could potentially influence their ability to counsel their asthma patients and possible strategies to overcome those barriers.
The questionnaires were distributed across the cities based on the number of community pharmacies in each of the cities as there was no available data on the proportion of pharmacists currently practicing in each of the cities. The five cities were found in the same region (Amhara National regional state) and thus they possess similar socioeconomic status.
Data processing and analysis
The collected data was cleaned, coded, and entered into SPSS version 21 for analysis. Descriptive analysis of the collected data was conducted and the results were presented using frequency tables and graphs.
Data quality assurance
One day of training was provided to all the data collectors. The data collection tool was pretested on 25 community pharmacy professionals (5 professionals in each of the five cities) to check the applicability of the tool and make necessary adjustments. Those pharmacy professionals that participated in the pre-test were excluded from the main study. The collected data were checked daily for its completeness, accuracy, and consistency before entering into software for analysis.
Ethical consideration
Ethical clearance was obtained from the ethical review committee of the School of Pharmacy (SoP), College of Medicine and Health Sciences, University of Gondar, and this was administered to each study participant before the data collection procedure. The purpose of the study was clearly described to each of the study participants and oral consent was obtained before the commencement of the study. Confidentiality was also assured by removing any personal identifiers from the questionnaire and the collected data was used only for the study.
Result
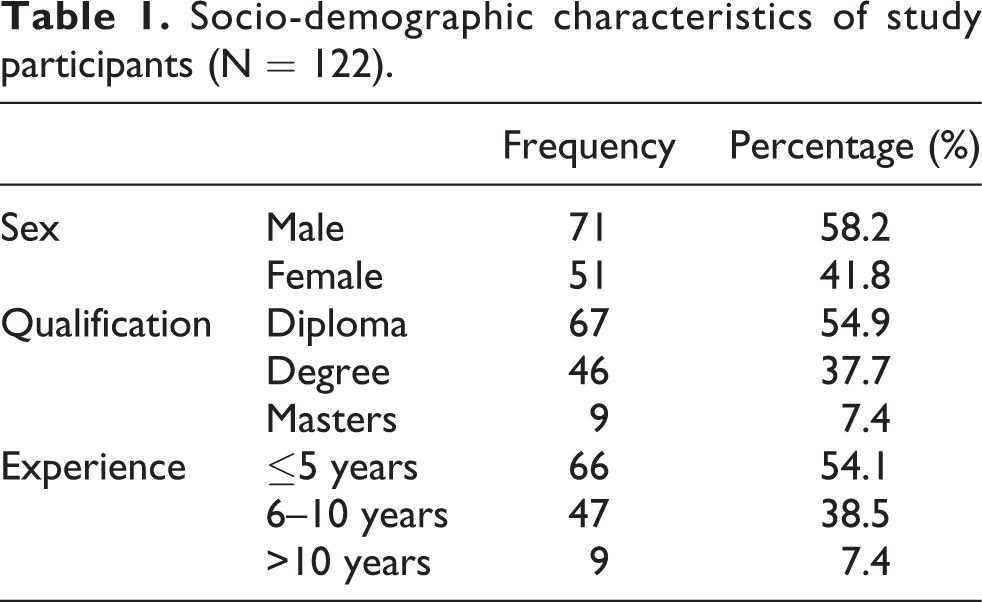
A total of 122 community pharmacy professionals; 63 from Gondar, 26 from Bahir Dar, 15 from Debre Markos, 14 from Woldia, and 4 from Debre birhan participated in the study providing a response rate of 61%. The majority of the respondents were male 71 (58.2%) in which 35 (49.3%) of them had ≤5 years of work experience. Concerning professional qualification, the majority were diploma holders 67 (54.9%) (Table 1).
Socio-demographic characteristics of study participants (N = 122).
About 96 (78.7%) of the participants reported that they teach their patients the basic facts about asthma. More than two-thirds of the participants 85 (69.7%) has also reported that they were able to identify and manage the triggering factors of asthma for their patients. Groups of drugs classified as short-acting B-receptor agonists were reported as the most commonly utilized single-drug therapy anti-asthma drugs in community pharmacies followed by bronchodilators; 33 (27%) and 13 (10.7%) respectively (Figure 1).

Commonly used anti-asthma drugs in community pharmacies.
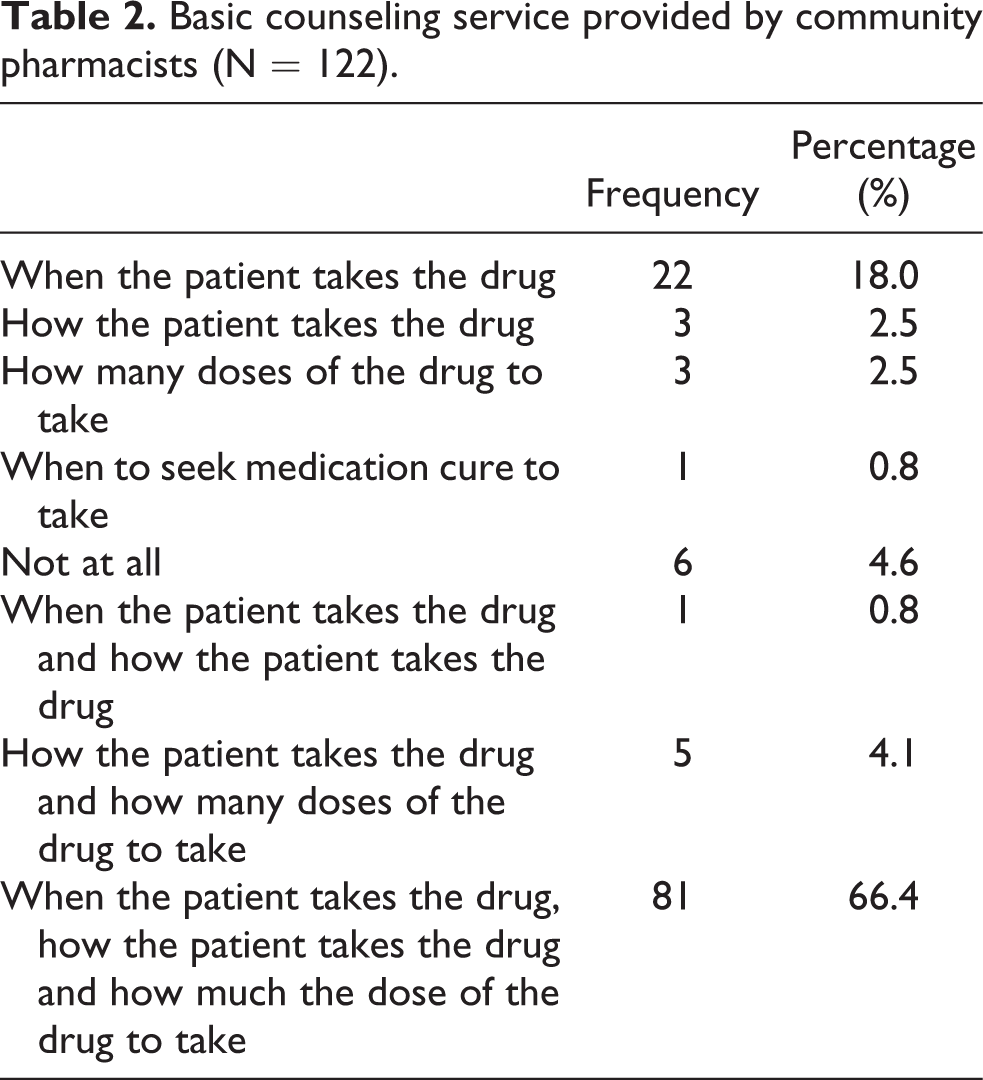
Concerning counseling patients about their medications, among the three basic medication-related information’s provided by the study (when to take, how much to take and how to take), 81 (66.4%) of the respondents reported that they provide all of the three information’s to their counseling service while dispensing medications (Table 2).
Basic counseling service provided by community pharmacists (N = 122).
About 84 (68.9%) of the respondents reported that they counseled their patients regarding the role of the dispensed medications in treating asthma while 71 (58.2) of the respondents have also reported that they counsel about the possible side effects of the medications (Table 3).
Additional counseling service provided by community pharmacy (N = 122).

About 78 (63.9%) of the pharmacists reported a lack of pharmacist time as a reason for the inadequacy of the counseling service provided whereas 74 (60.6%) of the respondents agreed with a lack of adequate knowledge about the disease and the medications as the possible reason. About 29 (23.8%) of the pharmacists also reported that it is not the responsibility of the pharmacist to counsel the patients (Figure 2).

Anticipated barriers for counseling asthmatic patients by community pharmacists.
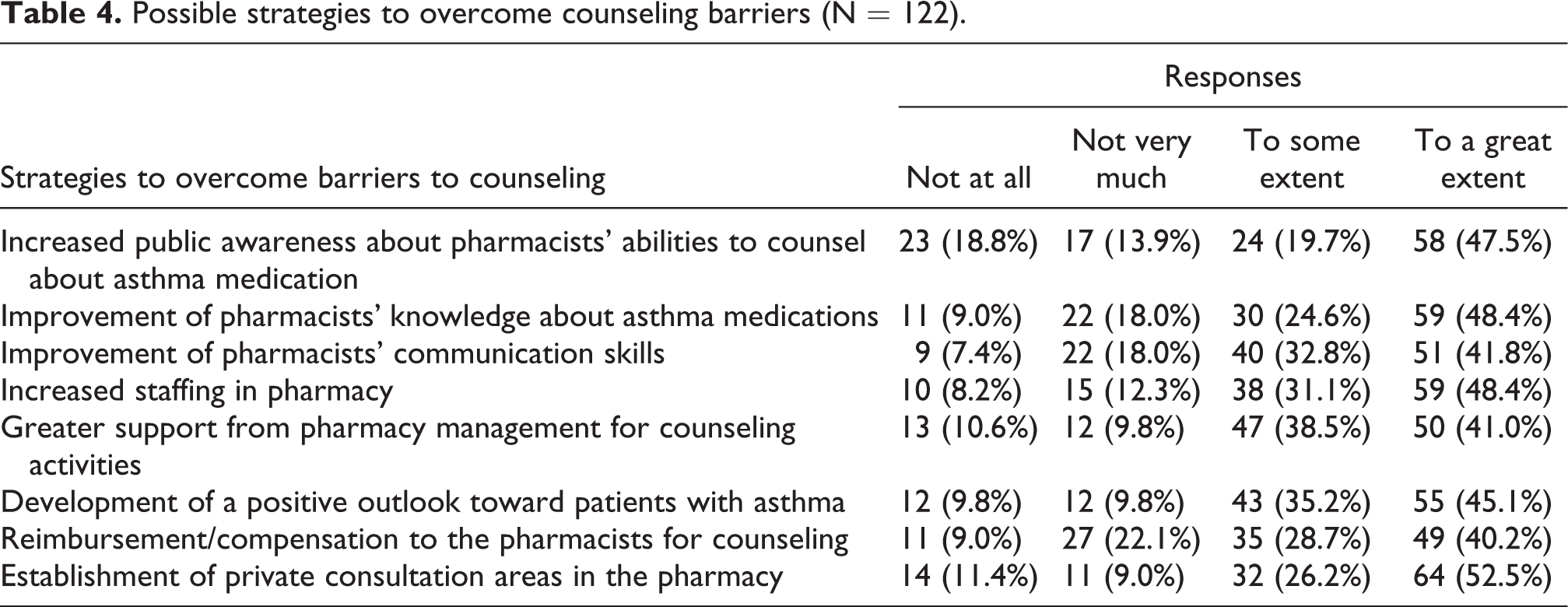
Regarding the possible strategies to overcome the barriers for counseling, the respondents were asked to put their response on a four-level Likert scale (not at all; not very much; to some extent; to a great extent). Establishment of private consultation areas in the pharmacy premises 64 (52.5%), improvement of pharmacists’ knowledge about asthma medications 59 (48.4%), and increasing the pharmacy staff 59 (48.4%) were the main strategies suggested by the study participants to overcome the barriers for counseling services (Table 4).
Possible strategies to overcome counseling barriers (N = 122).
Discussion
Community pharmacists’ involvement in asthma care has been shown to improve asthma control, as well as improve the quality of life for those with asthma. 41,18 This study showed that 78.7% of the participants reported that they teach their patients the basic facts about asthma. The finding of this study is comparable with a study done in Rabat in Morocco (75%) 42 and Saudi Arabia (85%), 43 but lower than a study done in Québec, where there are asthma education centers and pharmacists are more motivated to intervene in the care of patients with asthma (98%). 44 Educating asthmatic patients about their disease, medications they took, and the main triggering factors should be the mainstay of its management strategy as asthma is a chronic disease, and patients should be aware of how they can self-manage the diseases to improve its prognosis and prevent future attacks.
The current study also revealed that more than two-thirds of the participants (69.7%) were able to identify and manage the triggering factors of asthma for their patients. The result of this study was very low compared to the study conducted in Saudi Arabia (90%). 43 Some of the possible reasons for this finding could be, as the majority of our study participants were diploma holders, it is clear that they hold their pharmacy qualification from private colleges (government universities in Ethiopia provide pharmacy education in Degree and above only) and the quality of education in the private colleges is very concerning as majority of them were established for business purposes. 45 This showed that some of the diploma holders were not well competitive enough in intervening the asthma patient with their basic knowledge.
In this study, β-receptor agonists were reported as the most commonly utilized single-drug therapy anti-asthma drugs in community pharmacies followed by bronchodilators 27% and 10.7% respectively. A similar finding was reported by respondents in Saudi Arabia. 4 A higher prevalence of β-receptor agonists use could be partially explained by the fact that β-agonists have been mainstays of asthma therapy for many decades and are recommended treatment at all levels of asthma severity, as they provide prompt relief of asthma symptoms through smooth muscle relaxation and, thereby, bronchodilatation. 46 Salbutamol (albuterol) is also the first-line treatment for bronchial asthma based on the standard treatment guideline of Ethiopia. 47 Salbutamol is also available over the counter (OTC) in community pharmacies in Ethiopia.
When asked about anticipated barriers for counseling asthmatic patients, most of the pharmacists reported a lack of adequate time and knowledge about the disease and the medications as the possible reason. Previous studies have reported the same issue. 41,48,49 Emerging evidence has shown that having more technicians available to assist with dispensing duties would increase pharmacist time for asthma intervention and training was found to improve communication strategies and provide pharmacists with updated knowledge on asthma. 50,51 Consequently, training appears to be an important prerequisite for the effectiveness of pharmacy staff in disease management.
Limitation of the study
The current study being cross-sectional and as such because the results of the current study mainly relied on self-reported practices of the study participants, some of their responses may not reflect their actual practice as they may tend to diverge to the correct practices due to social desirability. The other major limitation of the study was, the total proportion of community pharmacists in the five cities were not known.
Recommendations
Pharmacy premises should be built with a separate room for counseling as counseling is one component of effective pharmaceutical care. An adequate number of pharmacy professionals should be employed in pharmacies which will decrease the workload, increase service efficiency, and improve the overall productivity of the pharmaceutical care service. It also appears evident that there is a need for continuing professional education and short-term training for pharmacists to update their knowledge and improve their engagement in the patient care service.
Conclusion
In summary, this study revealed that the majority of the pharmacists had a perception that they were able to identify and manage the triggering factors of asthma for their patients. The pharmacists also reported that they were able to provide basic facts about the disease and the medications, to their patients. However, they reported requiring more time and a suitable environment if they were to be able to counsel their patients regarding their disease management and medications they took even if the patients didn’t demand it.
Footnotes
Acknowledgments
The authors would like to thank all the data collectors and study participants for their effort and cooperation in conducting the study.
Author contributions
YKE: Performed the visualization, participated in the methodological selection, software processing, and supervision. WWH: Participated in conceptualization and writing of the original draft. ESA: Participated in the data curation and supervision. EAS: Participated in data curation, supervision, and visualization. GKB: Participated in data curation, supervision, and visualization. BAA: Participated in the writing of the original draft of the manuscript. DKY: investigation, writing, reviewing, and editing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest regarding the research, authorship, and/or publication of the article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.