
Abstract
Oxygen therapy is a common intervention in health care worldwide; yet, despite universal use, it is evident through poor practice that oxygen is often prescribed and administered injudiciously. It is proposed that possibly an influencing culture presides, whereby oxygen is often poorly understood and uncertainty regarding its use exists. It is unclear where the origins of this culture lie but exploring perceptions may enlighten the problem. A review of the literature was undertaken to establish what is already known about this elusive phenomenon. The paucity of any direct evidence regarding perceptions of oxygen directed the review to utilize a critical interpretative synthesis (CIS). The aim of this study was to explore how respiratory patients perceive oxygen therapy. A systematic search in Medline, Cinahl, Embase, British Nursing Index and PsychInfo yielded 1514 studies of which 42 were selected to consider the review question. The CIS allowed evidence from across studies to synthesize existing and new interpretations of data related to patients’ perceptions of oxygen therapy. Synthetic constructs then informed the synthesizing arguments, namely positive – feeling safe, enabler and comforter; negative – fear, oxygen versus self, restriction and embarrassment; and impartiality – mixed blessings. The findings are divergent, and at times contradictory. There appears uncertainty among patients regarding the purpose and benefits of oxygen therapy, though an underlying faith in health-care professionals is apparent. This faith seems to foster acceptance of a life-changing therapy, despite the impact, burden and incomplete understanding. There is a clear need for further research regarding these elusive perceptions in order to improve clinical practice in respect of oxygen.
Keywords
Introduction
Oxygen is one of the commonest therapeutic interventions in health care worldwide. Yet, despite the widespread use, problems regarding prescription and administration exist, 1 –7 resulting in a significant burden for patients, carers and health care resources.
Poor practice regarding oxygen therapy, such as inadequate assessment and poor follow-up, has been uncovered in the United Kingdom. 7 This led to major changes in prescription and provision of domiciliary oxygen therapy, principally the provision of clinical standards for initial assessment and subsequent patient management. 8 Despite implementation of these changes, problems continue. 9,10 It is unclear what factors contribute to persisting poor practice; the problem may stem from a belief that oxygen alleviates breathlessness, 11 but there is no evidence supporting this claim.
Oxygen in both acute and chronic settings has been recognized as a major area for improvement in the United Kingdom, 12 but in order to address these recommendations there is a need to identify reasons for enduring poor practices.
The review question, ‘how do respiratory patients perceive oxygen therapy?’, is orientated towards respiratory patients’ perceptions rather than efficacy of the intervention. The literature is therefore dominated by qualitative research as these voices are brought to the fore. Relevant quantitative data were also evident and so directed the review to one of an integrative approach. Integration and synthesis of both qualitative and quantitative research, although complex and challenging, have the potential to enhance holistic understanding of the topic being investigated and therefore increases relevance. 13
The specific review question appears elusive in published literature, and it became apparent that extrapolation from studies with a wider focus was necessary. This directed the decision to utilize an interpretative, rather than aggregative, approach and informed the selection of a critical interpretive synthesis method.
The aim of this review was to explore respiratory patients’ beliefs and perceptions of oxygen therapy in order to highlight and provide a platform for further investigation.
Method
Meta-ethnography 14 is an interpretative approach that aims to make sense of what a collection of qualitative studies are saying rather than just narrating the various findings. A variant of meta-ethnography, critical interpretative synthesis (CIS), has been developed as a method to review large, diverse and complex bodies of literature, 15 allowing explicit integration of qualitative and quantitative evidence through an interpretative process. One of the distinguishing features of CIS is that whilst it draws upon conventional systematic review methodology, it differs by allowing discretion in study selection to include papers that may not necessarily answer the review question directly but may contribute to findings. The authorial voice is also permitted, indeed essential, in the interpretation. 15
Search strategy
A systematic approach to searching, locating and retrieving relevant literature was adopted (Centre for Reviews and Dissemination (CRD), 2009). Medline (1950–2014), Cinahl (1981–2014), Embase (1980–2014), British Nursing Index (1985–2014) and PsychInfo (1806–2014) and searched via Evidence Search (www.evidence.nhs.uk) using key words oxygen therapy, chronic respiratory disease, COPD, interstitial lung disease. No date or publication type restrictions were applied.
Synonyms and term variants were searched and combined using the Boolean ‘OR’ (e.g. oxygen therapy OR O2 therapy). Different facets were combined with the Boolean ‘AND’. Truncation (*) was utilized to capture plurals and spelling variants (e.g. Oxygen therap*). Advanced search operators for phrase searching (“”) were used to improve the focus. The search was limited to English language, human and adult studies as per inclusion criteria (Table 1).
Inclusion and exclusion criteria.

To minimize publication bias, a wider Internet and grey literature search was conducted; database searches were supplemented with hand-searching key journals and ‘citation snowballing’. 16 Discussion with experts in the field, together with searching key respiratory conference proceedings ensured inclusion of contemporary literature not yet indexed in databases.
Inclusion criteria and study selection
Two reviewers independently screened the title and abstracts for eligibility against inclusion and exclusion criteria (Table 1) and relevance to the research question. In the event of disagreement, the full text was requested. Value judgements regarding the credibility and potential contribution were then deferred to the quality appraisal phase.
Quality assessment
A leading contention related to quality appraisal and integrative reviews is whether studies should be excluded on the grounds of poor quality. 17,18 It is further argued 19 that assessment of qualitative research is an interpretative act that requires informed reflective thought rather than just a simple scoring system. Content and relevance of findings therefore was a key consideration and articles were quality appraised on their own merit and within the context of the review question.
The diversity of studies warranted development of a hybrid quality appraisal/data extraction sheet based on criteria for disparate data as suggested by Hawker et al. 20 This identified various methodological strengths and weaknesses without excluding studies of poorer quality. 21 Using Hawker et al.’s protocol for assessment, a score of 1–4 is assigned to each of 10 criterion resulting in an accumulative score that indicated the overall assessed methodological rigour of each empirical study (ranging from 10 (very poor) to 40 (good)). A cross-section of articles was cross-checked by an independent reviewer and differences resolved by discussion and consensus. The process of quality appraisal, including relevance, reduced the number of studies from 59 to 51. Reasons for exclusion, together with references, are outlined in Table 2.
Reasons for exclusion of studies and references.

HCP: health-care professionals; COPD: chronic obstructive pulmonary disease.
Data extraction strategy
A data extraction proforma was constructed that detailed characteristics and quality appraisal of included studies, including relevance to the research question, together with examples of verbatim extracts from qualitative studies representing the ‘voice’ within the literature (Table 3). Data extraction was undertaken by the lead researcher and a sample independently reviewed.
Grid of themes and representation from the literature – patients.
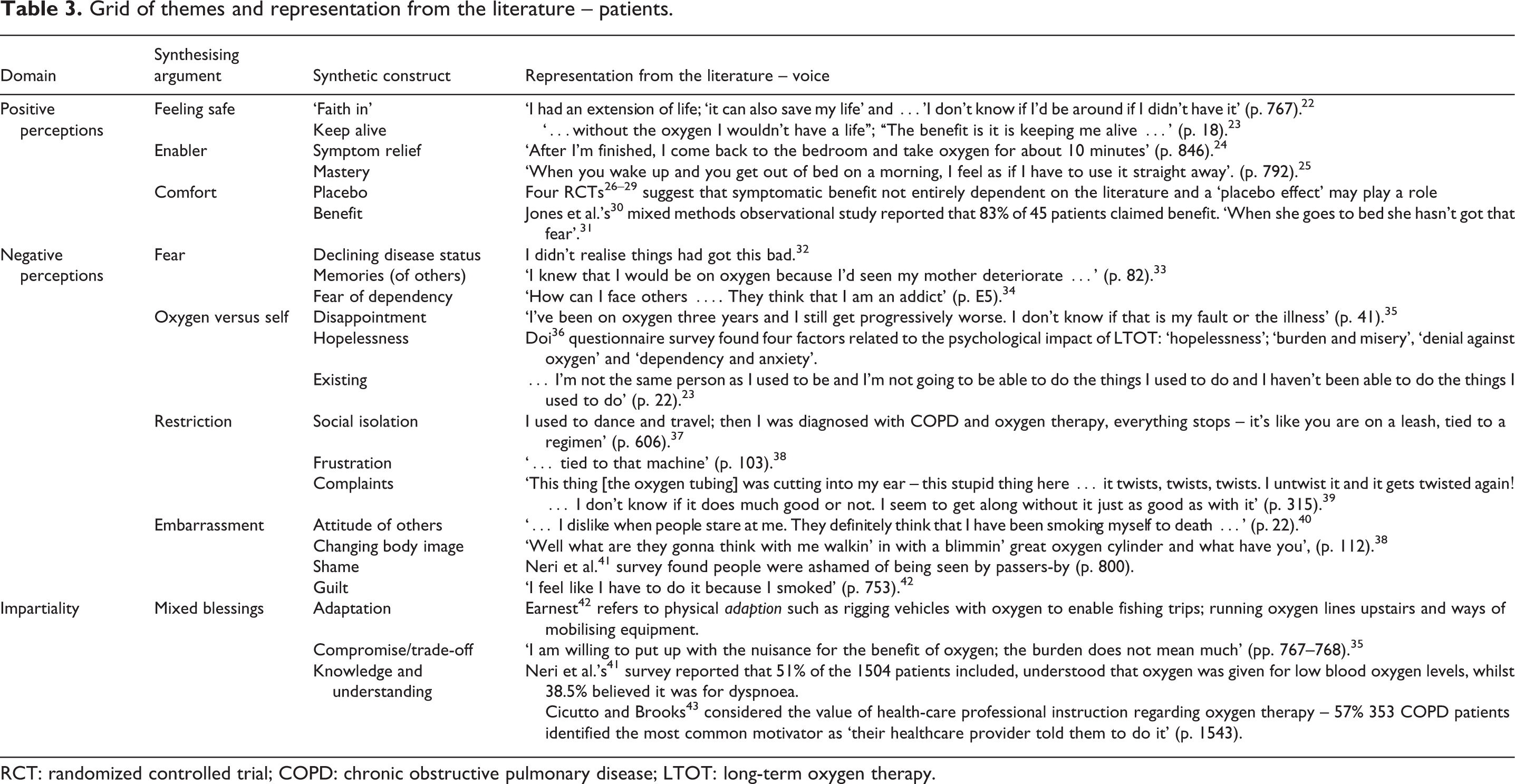
RCT: randomized controlled trial; COPD: chronic obstructive pulmonary disease; LTOT: long-term oxygen therapy.
Synthesis of the extracted data
Mirroring criteria set out by Flemming, 18 the current review adopted the following stages of synthesis; the article was read and understood in relation to itself; relevant data were extracted and translated into one another through identification of concepts, themes and metaphors; synthesis of the translations into emergent synthetic constructs; finally exploring relationships between the constructs which allowed explanatory accounts to be suggested in the form of synthesizing arguments. This integration of evidence from across studies allowed, in the absence of evidence directly addressing the research question, new interpretations of data which is demonstrably grounded in existing evidence. 21
Findings
The flow chart (Figure 1), adapted from PRISMA, 44 provides a summary of the search outcome. At this stage, articles were separated into two categories, namely patients (42 studies) and health-care professionals (HCPs; 12 studies), with a total of 51 articles (three articles being eligible for both). Results from patients’ perceptions are reported here, results from HCPs perceptions are reported in a companion paper.

Flowchart of study selection.
The final selection of articles related to patient perception is summarized in Table 4.
Grid of literature – study characteristics – patients.

RCT: randomized controlled trial; COPD: chronic obstructive pulmonary disease; LTOT: long-term oxygen therapy;O2: oxygen; FEV1: forced expiratory volume in 1 second; SGRQ: Saint George Respiratory Questionnaire, BMI: Body Mass Index; HCP: health-care professional; PRN: when needed; NIV: non-invasive ventilation; SBOT: short burst oxygen therapy.
aStudies included in Cullen and Stiffler’s meta-synthesis.
bStudies also included in the review of HCP’s perception.
Few studies directly addressing the research question were evident therefore studies were selected on the basis that some aspect of, or reference to, the study’s findings included patients’ perceptions of oxygen therapy.
The final selection of 42 articles consisted of varying methodological approaches, quality, countries of origin, and patient groups, reflecting the heterogeneity of studies. The number of patients in each study ranged from 5 to 1504. Quality appraisal scores ranged from 21 (poor) to 38 (good) out of a maximum score of 40; no papers were excluded on the basis of quality as discussed previously.
The synthetic constructs and their subsequent synthetic arguments can be classed into three distinct domains: negative perceptions; positive perceptions and impartiality. These constructs, together with the number of articles that contributed to each, are outlined in Tables 5 and 6.
Synthetic constructs and synthesising argument.

Grid of themes and sub-themes and occurrences – patients.
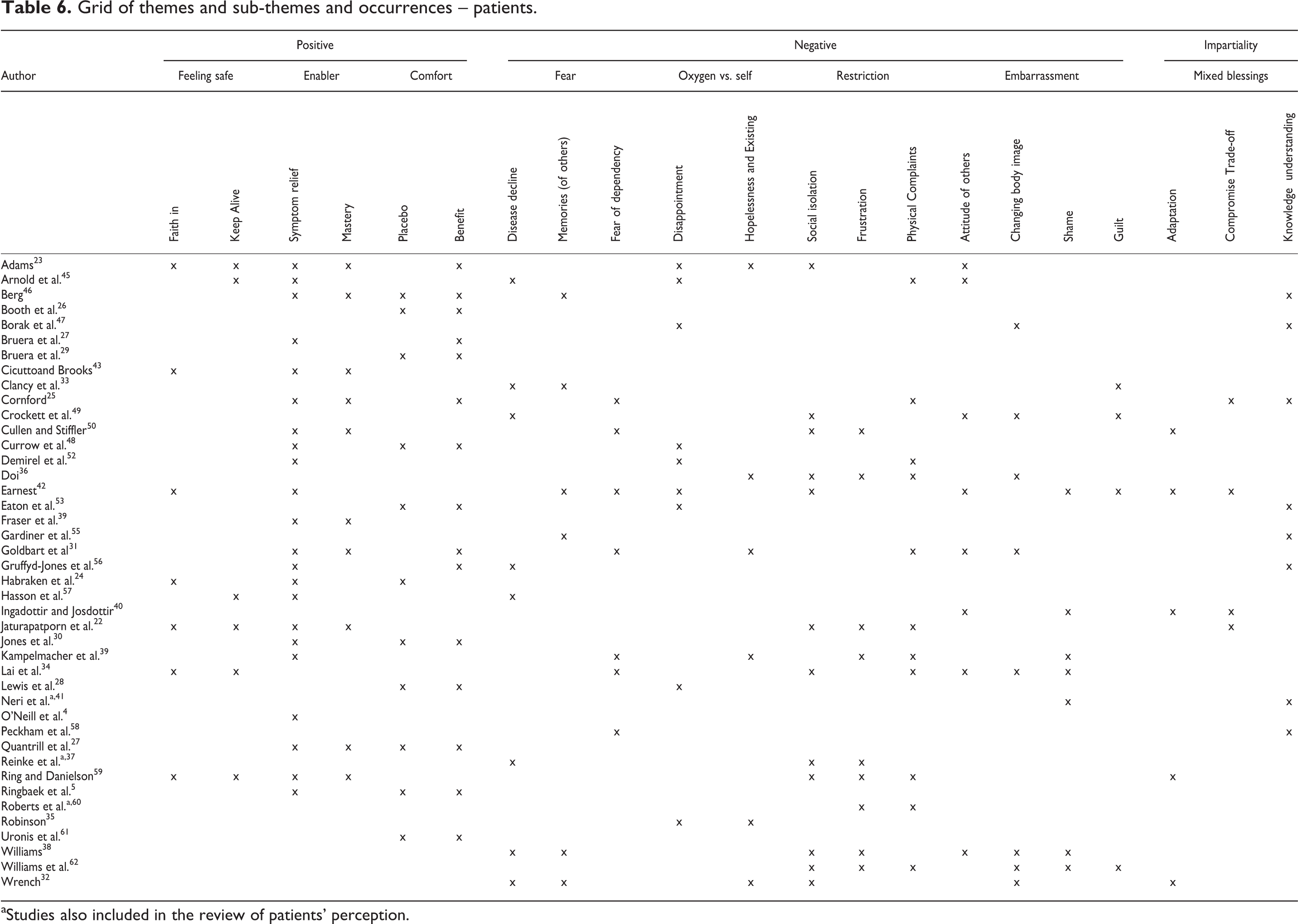
aStudies also included in the review of patients’ perception.
Positive perceptions
Three main synthesizing arguments were constructed that reflected patients’ positive perceptions of oxygen therapy: feeling safe, oxygen as an enabler and oxygen as comfort.
Feeling safe: keeping alive and faith in HCPs
It is apparent within several reviewed studies that patients often regard oxygen as tantamount to keeping them alive. 22,23,34,57,59 A key finding in Ring and Danielson’s 59 phenomenological study of chronic obstructive pulmonary disease (COPD) patients with long-term oxygen therapy (LTOT) was ‘an advantage to the body’. How this correlated to patients’ knowledge and understanding was unclear. Similarly, perceptions regarding oxygen as being ‘essential’ 34 fail to illuminate what manifested this belief. Patients identify oxygen as a life-saving intervention: ‘I don’t know if I’d be around if I didn’t have it’. 22 Likewise Adams 23 discusses oxygen as ‘enabling patients to live’, whilst other studies reported patients feeling safe through increased confidence 45 or relief of dyspnoea. 31
Earnest 42 highlights patients stated trust in the prescribing physician. This notion of faith and trust in HCPs is further legitimized in the literature 22 –24,34,43,59 and was often associated with compliance and identified as a motivator for self-care.
Enabler: symptom relief and mastery
Patients clearly utilize oxygen as a tool for symptom management, 4,22,23,31,41,43,45,54 appearing to enable patients to perform activities and to self-manage. 25,46 A meta-synthesis exploring patient’s perspectives of oxygen 50 also identified self-management as a key theme. Patients are often started on oxygen for shortness of breath, despite no documented hypoxia. 22 This rationale for prescribing oxygen for dyspnoea rather than hypoxia is common 4,26,54,56 and may have a bearing on patients’ expectation.
Enablement through improvement in both subjective dyspnoea and objective post activity recovery times demonstrated benefits with oxygen (vs. air) but the effect was small. 27 Those patients who distinguished oxygen from air perceived that it was ‘better than nothing’ (p. 703), suggesting an effect from the sensation of air flow as a means of reducing dyspnoea 63,64 and thus enabling increased activity. Interestingly, some authors 4,24 report that perceived relief of breathlessness post exercise could correspond with cessation of exercise itself rather than oxygen. Other accounts of enablement refer to oxygen increasing stamina and giving strength, 59 giving energy, 23 managing anxiety 56 and improving quality of life. 5
The use of oxygen to relieve breathlessness is the most commonly recurring topic and clearly relates to enabling patients. Whatever contributes to this symptom relief, it is apparent that oxygen enables patients to achieve some degree of mastery over both their symptoms and, consequently, their disease.
Comfort: benefits and the placebo effect
Literature often discusses patients’ perceived benefit from oxygen therapy; it is important to distinguish whether this benefit is physiological or the result of a placebo effect, but either way it is apparent that oxygen can be comforting. This placebo effect in itself could be attributed to either facial cooling/stimulation 63,64 or as a result of a psychological phenomenon.
Quantitative studies aiming to assess the benefits of oxygen in relation to dyspnoea were included in this review because they contained some data or insight into patient perceptions. Subjective benefits of oxygen were found to be comparative with air in experimental studies 26,28,29 and unrelated to the extent of hypoxia. 26,28 A possible placebo effect is identified. 26,28,30 The nature of participants enduring terminal illness however needs to be considered when interpreting these results.
The cessation of breathlessness by oxygen, as perceived by patients, doesn’t always meet expectations. A systematic review and meta-analysis 61 determining the efficacy of palliative oxygen for relief of refractory dyspnoea showed that oxygen doesn’t always provide symptomatic benefit. This may reflect the subjective nature of dyspnoea and difficulty measuring this complex phenomenon.
Oxygen appears as a positive addition to therapeutic treatment for respiratory disease, it fosters a feeling of safety and is synonymous with life. There appears a faith in oxygen to keep patients alive and relieve symptoms which appears to contribute to the notion of mastery and self-management with indubitable benefits to patients.
Negative perceptions
Within the considered literature four major synthesizing arguments were constructed featuring negative perceptions of oxygen therapy for patients: fear, oxygen versus self, restriction and embarrassment.
Fear: declining disease status; memories (of others); and fear of dependency
Articles reported oxygen was symbolic of declining disease status or patients getting worse.—33,32,37,49 The initiation of oxygen therapy is seen as a key milestone in the disease trajectory and symbolizes declining health, one patient reported that initially they thought they would ‘get off’ it but then accepting that ‘this is the way it’s going to be’ and analogy with a ‘death sentence’. 49 This issue is quite clearly linked with memories (of others), with one patient reporting, ‘I knew that I would be on oxygen because I’d seen my mother deteriorate’. 49 This association with death appears as a direct contradiction to previous constructs of faith in and keep alive. 22,23,34
Reflection on previous experiences is seen further. Exploration of oxygen in respect of living with COPD revealed recalled memories of others using oxygen, ‘…the fact that it could get to the stage where my father was…’. 55 Earnest 42 reported similar reflections, but on patient’s own experiences rather than others’, stating that fear of past events such as an exacerbation, panic and fear of running out of oxygen all led to increased reliance on oxygen.
Fear of dependency was a recurring theme. Authors make reference to patients not using prescribed oxygen due to their fear of addiction 52 and the perception that others have of them whilst wearing the oxygen in public, ‘Wearing an oxygen cannula just looks like someone addicted to drugs…’. 34 This can be related to non-compliance, with reports of 20% of patients using oxygen for fewer hours than prescribed as a result of fear of addiction. 39
Oxygen versus self: disappointment, hopelessness and existing
These constructs seems to capture some form of internal struggle patients experience with oxygen. Contra to their expectations, patients often report feeling disappointed with oxygen, for some this was related to dyspnoea. 23,35 Futility was identified, ‘I’ve been on oxygen three years and I still get progressively worse’; 35 ‘I’m still out of breath’. 45 This lack of benefit is perhaps suggestive of belief that oxygen is curative.
The construct hopelessness and existing further amplifies the struggle patients have accepting oxygen therapy as a beneficial adjunct to treatment. 23,32,35,36,39,47
Adams 23 evidenced patients’ loss of self and existing together with feelings of grief, ‘I just thought I’m not the same person as I used to be…’. Likewise Kampelmacher et al 39 reported the majority of patients complained of restricted autonomy. This loss of ability to govern one’s own life and actions can be regarded as an internal struggle as patients strive to accept oxygen despite the inevitably of restriction, loss of independence and reduced activity.
Restriction: social isolation, frustration and complaints
In contrast to oxygen as an enabler, many studies reported patients regarding oxygen as burdensome or restrictive. 22,25,31,34,36,37,45,59,62 Disadvantages such as decreased mobility, discomfort in relation to nasal prongs, barriers to accessing oxygen and noise of equipment suggest that oxygen therapy is not entirely benign. When referring to alterations in patients’ social life, recreation and pastimes quotes such as tied to that machine 38 further demonstrate resentment.
Adams 23 discussed the restrictive nature of oxygen as an enabling paradox reporting that although oxygen enabled participants to do more, it was often considered inconvenient. Apart from physical restrictions, patients make reference to restricted autonomy 39 and feelings of frustration, ‘This thing [the oxygen tubing] was cutting into my ear – this stupid thing here…it twists, twists, twists. I untwist it and it gets twisted again!’. 60 The patient’s frustration is clearly evident here as he weighs up the benefits versus the inconvenience.
Embarrassment: attitude of others; changing body image; shame and guilt
Attitude of others appears important. The use of therapy in public seems to threaten the image of a healthy person. 40 Additionally there is reference to ‘the negative body image’ associated with oxygen use 36 and patients feeling weak and sick. 42 This relationship between shame and guilt and caring about attitudes of others is recurrent 34,31,39,41,42 and often related to the stigma of smoking, with embarrassment recorded as a common theme . 49
This relationship between embarrassment, shame and guilt can be further typified when patients refer to changing body image. 38 Further reference to patients’ feeling of fraud and oxygen legitimizing their sick role 38 raises possibilities that using oxygen helps to dispel shame and guilt.
Earnest 42 discusses the conspicuous nature of oxygen therapy, one that advertises illness: a ‘public’ therapy. A finding endorsed by Williams et al. 62 who noted that oxygen made their illness ‘visible’. Interestingly, Adams 23 noted that most patients when interviewed did not wear oxygen.
The myriad of negative emotions captured in the synthesis seem to culminate in a profound sense of grief and loss for patients, including loss of identity and loss of power to change. 42 These feelings ultimately appear to lead to acceptance and a sense of patients having to put up with oxygen. Fear of dependency appears to subside as patients strive to come to terms with oxygen as part of their disease and, in some cases, seem to regard it as a means of penance.
Impartiality: Mixed blessings
Whether patients regard oxygen as a mixed blessing develops from a result of needing to adapt, conflicting views and beliefs, or a lack of knowledge, is unclear within the literature.
Mixed blessings: adaptation, compromise and knowledge and understanding
Cullen and Stifler’s meta-synthesis 50 identified the theme ‘adapting to life’s circumstances’, this finding was based on patients rationalizing oxygen whilst negotiating the interference with lifestyle. They refer to individual health beliefs driving the rationale for use and preferences for administration.
Robinson 35 considers adaptation as a need for compromise, claiming that patients in their study adopted a put-up-and-shut-up (p. 42) attitude in an attempt to adjust to this time-consuming and, for some, uncomfortable therapy. Jaturapatporn et al. 22 also refer to patients being willing to make compromise, one patient quoted, ‘I am willing to put up with the nuisance for the benefit of oxygen’.
Ingadóttir and Josdottir 40 use the term mixed blessings as a major theme. Patients make reference to purposefully developing an optimistic view of therapy, probably as a trade-off for the inconvenience. A similar compromise is seen in Cornford’s 25 study of lay beliefs regarding oxygen, one patient quoted his/her ‘respect’ for oxygen, reporting that he/she limits usage in order to preserve effect.
The final construct of knowledge and understanding appears as neither a positive nor a negative aspect. As already reported, the direct relationship between patients’ knowledge and understanding and perceptions is elusive. One study did try to uncover beliefs regarding patients’ understanding and knowledge of LTOT 41 and found that 51% of the 1504 patients surveyed, understood that oxygen was given for low blood oxygen levels, whilst 38.5% believed it was for dyspnoea. Whether this was a misunderstanding or misinformation given by HCPs is unclear.
The significance, or blind faith, that patients have for professionals caring for them has already been recognized as making patients feel safe. This probably also impacts on patients’ acceptance of the therapy. A further aspect to this is patients’ anxieties and fears associated with uncertainties regarding provision of oxygen therapy. Patients reported perceiving oxygen therapy was needed following hospitalization, but were uncertain why it hadn’t been provided or, if it had, when they should use it. 56 Further commentary regarding potential misinformation and unrealistic expectations is apparent with regard to patients not always being prepared for withdrawal of oxygen. 53
Peckham et al. 58 demonstrate a beneficial effect of education on compliance which could, in effect, increase potential efficacy for LTOT. In this UK based study, patients who received education following LTOT prescription had a better understanding of why they needed oxygen and showed better adherence to prescription regimes. Education therefore appears to impact on patients’ understanding, and, ultimately, perceptions of oxygen.
Discussion
Although few studies specifically addressed the review question, data extracted from existing literature allowed for illumination of patterns and construction of synthetic arguments concerning patients’ perceptions of oxygen.
For many patients oxygen is regarded as a positive therapy, a life-giving intervention, although it is not clear whether this arises from patients’ expected benefits, or faith in HCPs. Juxtapose to this, patients relate to removal or denial of oxygen as a sign of impending death. This finding may be relevant regarding why patients are often considered to demand oxygen or resist removal of established therapy.
It appears that patients’ understanding is often that oxygen is commonly given for relief of dyspnoea. Lack of rationale for oxygen prescription is apparent throughout the literature and makes it impossible to judge whether individuals require oxygen, or not. For some, oxygen helps to control dyspnoea but whether this is as a result of the sensation of air flow, 63,64 cessation of exercise or a placebo effect is unclear. Studies have shown that comparing to room air, there are no additional benefits of oxygen for the palliation of dyspnoea. 65 Likewise a Cochrane review 66 gives no firm conclusions regarding the efficacy of oxygen for symptom relief. But regardless of why oxygen relieves breathlessness it is clearly beneficial to patients.
Although physiological benefit for hypoxaemic patients cannot be disputed, for normoxic patients there appears to be a definite placebo effect. 65 Interestingly, Roberts et al. 60 observed that although several patients in their last year of life were taking morphine or an anxiolytic, none believed that these had been prescribed for relief of dyspnoea, highlighting patients’ preconceived ideas regarding the rationale for prescribed treatments and resultant expectation.
How patients build their expectations remains unclear. It would seem logical though that oxygen given to a breathless patient could lead to relief of breathlessness, a self-fulfilling prophecy perhaps. Conceivably this is further evidence of patients’ faith in HCPs or it could be that mastery itself reduces anxiety by allowing control over symptoms. Expectations do seem to contribute to the culture that exists regarding using oxygen for dyspnoea.
Fear as an overarching theme is a multifaceted concept with regards oxygen. Previous experiences of others are clearly significant and probably on occasion well founded. Fear of what oxygen symbolizes in respect of disease progression and the potential for addiction seems a powerful negative emotion and may ultimately impact on acceptance and compliance.
Oxygen for some is a marker of disease severity, often synonymous with palliative care and death. Oxygen is a visible therapy and for some it legitimizes the sick role 38 making visible an otherwise imperceptible illness. Harrison et al. 67 identify a similar concept in a meta-synthesis exploring patients’ response to acute exacerbations of COPD. They identified that by making breathlessness visible to others, patients could communicate the seriousness of their condition. Contrary to this finding, embarrassment regarding oxygen also appears significant, closely related to shame and guilt through aesthetics, and often related to issues such as smoking. In this respect, oxygen use in public is perceived as a stigma, a display of their sick bodies, maybe a penance for some.
Poor compliance with domiciliary oxygen therapy has been discussed elsewhere. 68,69 This current review has identified perceptions that may contribute to poor compliance and therefore may be an important target with regards education. Disillusionment with the lack of efficacy is one such aspect, this seems to relate to the belief that oxygen has curative qualities and that disappointment results from a lack of alleviation of symptoms. This could demonstrate an unrealistic expectation with regards to prognosis and perhaps highlights a fundamental lack of knowledge and understanding. Fear of addiction and dependency may also feed into these perceived negative associations.
Education is undoubtedly important and has the potential to influence not only patients’ knowledge and understanding but also their perceptions. 70 Knowledge and understanding appear central but remain obscure; there seems an inability for patients to articulate the rationale or therapeutic benefit of oxygen. Whether the use of medical terms and jargon, the lay patient’s inability to understand physiology or whether they regard information as unimportant merits further investigation. Many patients may have stopped using oxygen through choice, rejection or removal; the views and opinions of this group are not evident in the published literature.
Oxygen can be seen as an irony to enablement with the main issues of physical side effects, restriction in terms of reduced mobility, and changes to daily activities, all leading to inevitable consequences of isolation. Oxygen in this context shows itself as a therapy that is not benign and often requires compromise, potentially propagating reduced physical activity and increased social isolation; a situation that so often self-perpetuates in the downward spiral so familiar for patients with chronic respiratory disease.
The synthesizing argument of mixed blessings seems to portray the necessity for patients to accept therapy in order to adapt and reap the benefits. Patients find tactics to adjust to oxygen in numerous ways that include physical, social and, sometimes, psychological compromise. The reasons why some patients adapt better than others remains ambiguous. Health beliefs appear to influence compromise and adaption but this facet clearly needs further exploration.
Patient perceptions of oxygen therapy demonstrate a paradoxical narrative with oxygen as an analogy with life and death, an enabler and restrictor and something to flaunt or hide. The ambivalence that often manifests then further develops to a stage of acceptance for some, but not all, patients. There appears uncertainty from patients regarding the purpose of oxygen, that is, whether it is to relieve symptoms or enable them to live. A faith in the health-care professional endorsing oxygen nevertheless is incontestable.
Overwhelmingly patients perceive oxygen as a positive therapy, but the findings from this review demonstrate that negative perspectives also exist and suggest that care should aim to counter these. The impact of oxygen on individuals and their carers is not insignificant 32 and the common belief that it is a benign therapy that needs to be dispelled. This in turn has the potential to influence expectations, culture and practice.
Summary and recommendations
The literature appears to render an insight, to some extent, into patients’ perceptions of oxygen therapy. The narrative is at times divergent, uncovering contradictory views. There appears to be an uncertainty among patients with regards the purpose and proposed benefits of oxygen therapy, though an underlying faith in health-care professionals is apparent. This faith seems to foster acceptance of a life-changing therapy, despite the impact, burden and incomplete understanding.
Although some enlightenment has emerged from the literature there is a clear need for further research regarding these elusive perceptions, from patients’, carers’ and health-care professionals’ viewpoints in order to improve clinical practice in respect of oxygen.
Strengths and limitations of the review
The high sensitivity of the initial search could be a considered strength of the review. The incorporation of participants’ voices is a further strength, allowing an idiographic approach and verification of the interpretative account. The authorial voice is key to the interpretations from the literature, and whilst drawing upon personal experience and preconceived ideas can be considered a threat to impartiality, alternatively it can be argued that the level of insight brought to the review through expertise was the fulcrum to the synthesizing constructs and true to CIS.
The quality of the reporting of included articles was an inherent weakness with many studies not being well described and methods of analysis not always explained. This issue of poor quality in write-up, as opposed to poor quality of methods, has been identified by other authors. 20 Ultimately most literature focuses on the impact of receiving oxygen as a therapy rather than actually what patients think or believe it does and this limits its ability to address the research question. A further limitation of the current review was the exclusion of lay carers’ perspectives. This may have added a further important dimension to the social construct of understanding of oxygen therapy.
The material selected displayed heterogeneity, being based on differing philosophical and scientific assumptions. This lack of similarity could be considered a weakness of the review, but alternatively it may be strength, allowing for an eclectic selection, necessary in the scarcity of directly relevant studies. Ultimately the purpose of this CIS was not to inform policy, nor even to inform practice (the paucity of data excluded this possibility) but to inform and give a foundation to this particular elusive phenomenon, through the identification of what is already known/evidenced and thus providing a platform for further investigation.
Dixon-Woods et al. 21 suggests that reflexivity in CIS is important. Conscientious reflection on the utilization of CIS included careful and repetitive consideration of the search strategy, study selection, data extraction and the process of synthesizing, both original data and the researchers’ interpretations of this data, to produce the synthetic constructs and subsequently the synthesizing arguments. The use of CIS itself opens the review up to criticisms of bias; however, when considering the dearth of evidence available, any alternative approach will have resulted in merely a thematic summary of accounts as offered in the original literature rather than in the context of the review question considered here.
Footnotes
Acknowledgement
I would like to thank Dr Dave Lynes, Edge Hill University, for his guidance with study selection and data extraction.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.