
Abstract
Chronic obstructive pulmonary disease (COPD) is the most prevalent form of chronic respiratory diseases worldwide. Pulmonary rehabilitation, including self-management education, highlights the importance of good patient–provider communication in establishing optimal care. There is a growing awareness of the potential impact of health literacy (HL) on the patients’ access to and understanding of medical information. This study was designed to explore the patients’ and health care professionals’ (HCPs) perceptions of the role of HL in health communication.
Semi-structured interviews and focus groups were conducted with 12 patients and 20 HCPs at a Pulmonary Rehabilitation Center in Metropolitan Toronto.
Although the term health literacy was not familiar to many patients, the contribution of knowledge to patient well-being was consistently identified by patients and HCPs. Barriers to communication included provider time constraints and the use of medical jargon. For providers they also included patient characteristics, language, culture and awareness of health resources. Approaches that might improve communication incorporated family support, peer support, better print and visual teaching material and a trusting empathic patient–provider relationship.
The findings provide an increased understanding of patients’ and providers’ perceptions of HL as a barrier to effective communication of medical information to patients with COPD as well as approaches that might improve this communication.
Introduction
The World Health Organization (WHO) defines health literacy (HL) as “cognitive and social skills that determine the motivation and ability of individuals to gain access to understand and use information in ways which promote and maintain good health.” 1 Globally, HL is emerging as an important factor in predicting population health outcomes, health education and health promotion.2–6 This emphasis is likely to increase, given the rising health care costs as well as the growing immigrant population across the globe. 7 HL literacy is also a public health issue. Based on the results of the Adult Literacy and Life Skills Survey, over 60% of adult Canadians lack basic skills to read, understand and utilize fundamental health-related information. 8 Moreover, Canadians with the lowest HL levels were 2.5 times more likely to be in poor health than those in whom it was considered to be satisfactory.
HL is important in the management of chronic respiratory conditions such chronic obstructive pulmonary disease (COPD) 9 which is estimated to affect over 510 million people worldwide. 10 The prevailing standard of care for patients with COPD, endorsed by many professional societies, 11 includes pulmonary rehabilitation, which emphasizes supervised exercise training, self-management education 12 and psychological support. Each of these components requires effective communication of health information between health care professionals (HCPs) and patients. Education self-management is especially important as it addresses the correct administration of medications and the timely response to acute exacerbations of COPD in order to reduce hospitalizations. 13 Patients with respiratory disease unable to understand complex verbal information or use written information effectively have less knowledge of their underlying disease, poorer symptom management and reduced health status compared with those who have adequate HL. 14
Although an improved understanding of the impact of HL in individuals with COPD will enable practitioners to optimize communication, thereby improving health care among their patients,15,16 many (HCPs) are uninformed as to its relevance for patient care 17 or regarding the availability of standardized measures of HL. Moreover, lack of awareness of HL by patients is often associated with a poor understanding of health information.18,19 Patients may not understand what the problem is, what can be done about it or how management recommendations might help and they may also be too embarrassed to acknowledge this deficit.
This study was undertaken to explore patients’ and HCPs’ perceptions of the role of HL on patient–provider communication, within the context of an urban pulmonary rehabilitation center in order to better understand the meanings attributed to HL and to identify barriers to effective communication. The specific research questions were the following: (1) How do patients with COPD and their HCPs perceive the role of HL in the communication of health-related information? (2) What are the barriers to clear communication of health-related information? (3) Which resources could facilitate communication of medical information? This information will assist clinicians to better understand the importance of HL in COPD and to recommend ways in which it may be integrated into clinical practice to enhance the patients’ understanding of their disease and their adherence to health care recommendations.
Methods
A qualitative approach was used to gain insight into the perspectives and experiences of key stakeholders. It utilized data gathered during individual interview sessions and focus groups with the participants. Ethics approval was obtained from the local hospital research ethics board and written consent was obtained from all participants.
Participants
Participants included 12 patients referred to an urban pulmonary rehabilitation center, with a diagnosis of COPD and 20 HCPs working at the same location. The HCPs were university graduates (physicians, nurses, therapists, pharmacists and health educators) with at least 1 year of clinical experience in this setting. All participants spoke English as their primary language of communication.
Data collection strategies
Data was collected over a period of 8 months (January to August 2011). Individual interviews and focus groups were the primary sources of study data. At the beginning of each session, participants completed a profile questionnaire to record their personal and demographic information.
Interviews
In order to protect privacy and ensure confidentiality, patients took part in a single one-on-one interview session with the principal investigator and interview questions were read to the participants (Appendix A). Individual interviews were conducted with physicians, in order to accommodate incompatible schedules and also to minimize any unequal power relations that might influence answers within a focus group. All interview sessions were open ended and topic based.
Provider focus groups
The 20 HCPs were divided into three groups for 1-hour focus group discussions to elicit information regarding their individual and collective experiences. After obtaining written informed consent, all interviews and focus groups were audio-recorded and transcribed.
Data analysis
A framework approach was used with a detailed interview schedule and set research questions determined by the authors. The analysis aimed to describe the experiences and perspectives of participants within specific contexts. This approach allows researchers to identify themes that accurately reflect textual data and are integral to describing the phenomenon under investigation. 20 Themes coded by the principle investigator were confirmed by one of the other investigators (DB) reading selected transcripts, with agreement by consensus.
Results
The participants were 12 patients (six females) aged 53–83 years (mean = 69.6 ± 9.9) and 20 HCPs (16 females) aged 30–63 years (mean = 47.4 ± 10.7). The patients’ educational level ranged from high school to university (Table 1). All patients were fluent in English. Two patients (AB 3 and AB 9) were subsequently noted to have predominantly morbid obesity (AB 3) and predominantly localized bronchiectasis (AB 9). Mean pulmonary function results are shown for the remaining COPD patients (Table 1).
Description information on the 12 patients interviewed.
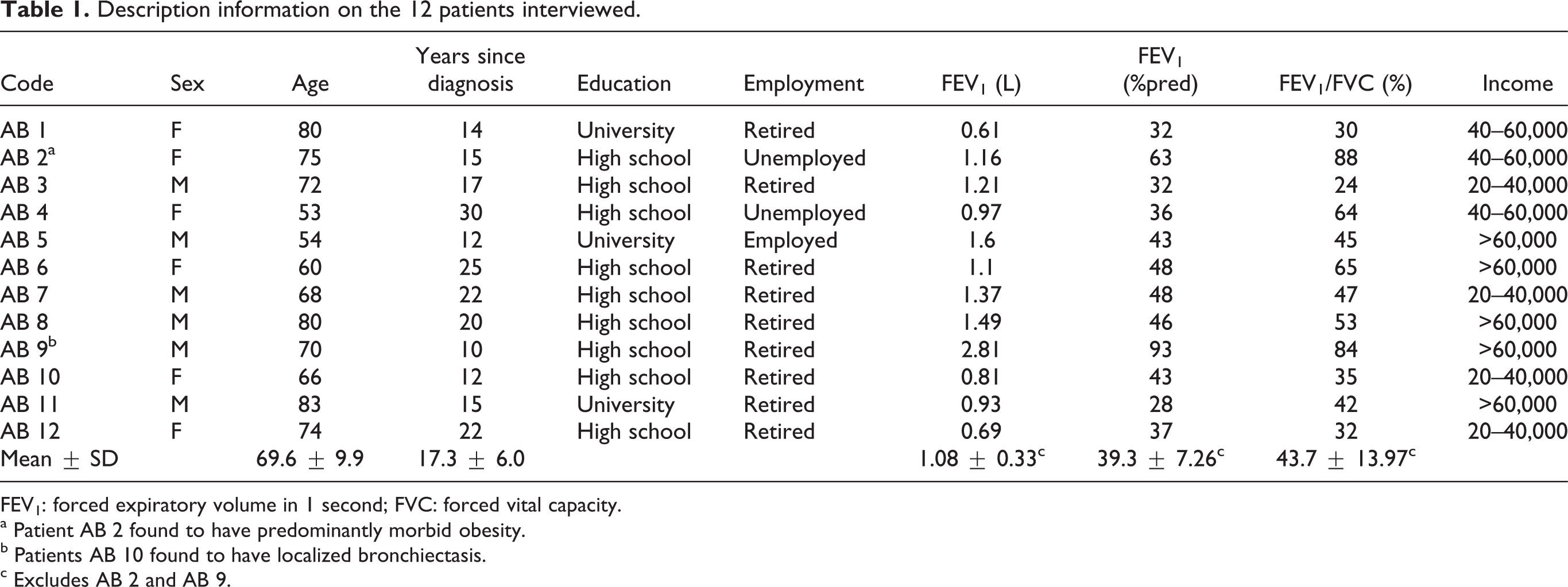
FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity.
a Patient AB 2 found to have predominantly morbid obesity.
b Patients AB 10 found to have localized bronchiectasis.
c Excludes AB 2 and AB 9.
All participants thought that HL had an important impact on an individual’s overall well-being and disease management. The results are presented in three sections: (1) individual understandings of HL and its significance for communicating health information; (2) barriers to communication and (3) resources and strategies that could improve patient–provider communication. In each section, the results provide the patient and then the provider perspectives.
HL in the communication of health information?
Patients’ perspectives
Defining HL
Most patients (75%) had not heard of HL. Five (41%) had learned about it primarily through the media and secondarily through their providers. Most patients (75%) provided a definition that placed HL within the boundaries of knowledge of their disease and patient–provider communication.
HL as knowledge. In defining HL in terms of disease knowledge, symptoms and treatment options, one patient stated that HL is the “the language to do with health, explaining what the disease is… how to control it” (AB 4). Other descriptions included “knowledge about your condition” (AB 8) and “how knowledgeable you are about health” (AB 8).
HL as communication. Some patients mentioned both the written and oral aspects of HL and defined it as a way of understanding and communicating health information. From this perspective, HL is a key factor in effective patient–provider communication. For example, one patient defined it as “to know … to find whether we understand what is written or told to us” (AB 2).
Significance of HL
Patients acknowledged the importance of HL in promoting awareness of symptoms and treatment options, self-management, accessing and utilizing the health care system. One patient commented, “if I didn’t know about the problem, like, about the disease, I wouldn’t know what’s going on. And, for quite a few years, people said it was in my head. And I found out it’s not, so, … once I started coming in here, and learning about it, and how to live with it, it does play a lot” (AB 4). Another patient explained, “well, I have a rare disease, and the more I can understand about the rare disease and, … um… , what functionalities within the health world, or health departments of the province and of this country that can help me… the better off I’ll be with that help” (AB 5). The impact of HL on improving communication and developing a better rapport between patients and providers was acknowledged. For example, “I definitely believe that health literacy plays a role in your health because before I started at [this center], I was very naive about my disease and the symptoms. The only thing I got was through the Internet. Now I can more or less understand what, uh, what I’m going through and if I have any concerns, I can relate to the professionals what they are actually telling me” (AB 6).
Providers’ perspectives
Defining HL
Most HCPs had learned about HL primarily through their workplace and secondarily through the media. Providers defined HL in terms of a patients’ ability to seek and understand health-related information, provision of information to patients, knowledge of the disease, its symptoms and treatment options.
HL as the ability to seek and understand health information. One provider explained that “health literacy refers to a person’s familiarity and understanding of matters related to health. Factors related to maintenance of good health as well as factors related to deteriorating health and illness, and…somewhere in there some basics of the anatomy and the physiology of the normally functioning body.” and another as “the way a patient seeks and uses and understands how the health information applies to him.”
HL as the provision of health information. Some providers defined HL as the provision (communication) of health-related information to their patients and underlined the necessity to use clear, simple language to convey meaning. One provider stated that “[health literacy] means the provision of information to patients about their health, whether it’s verbal or written, in a way that is understandable to them” Another said, “[health literacy is] appropriate communication between health care professionals and patients, and between the patients and healthcare professionals.”
HL as knowledge. The HCPs defined HL as the knowledge of and about the disease. One stated that “[health literacy is] the health issues that [patients] are aware of, you know, health conditions. They know all about diagnosis, medication, the care that goes into them, you know, they are aware, and they are knowledgeable.” Another provider said that “I always presumed [that] it’s the knowledge about a certain topic, in this case a health care topic, like either personal health issues or the diagnosis of the disease, or general health, I don’t know how detailed it has to be.”
Significance of HL
Providers mentioned increased awareness of disease symptoms and treatment options, self-management and effective communication as the impact of HL’s on individual health and well-being. One provider said, “I think [health literacy] plays a big role, because quite often the patient is unable to understand the information provided. The physician and the patient may leave the room with different impressions of the circumstance, and the patient is not sufficiently confident, because of their poor understanding, to actually ask the more important questions for their well-being.” Other providers considered limited HL as a barrier to good patient–provider communication which may ultimately have adverse effects on a patient’s self-management. One provider commented, “[low health literacy] can serve as a barrier that [patients] don’t understand and comprehend what’s going on … there could be adverse reactions. Our whole program is focused around teaching patients to manage their chronic condition. If they do not understand, then they won’t be able to care for themselves.” Providers also mentioned that good HL may lead to a better quality of life. One physician said, “I think a patient who is well informed might not live longer, but they will live better.”
Barriers to communication of health information
The participants were asked about barriers to effective patient–provider communication, and the strategies they employed to overcome or repair communication breakdowns. Patients and providers differed on their respective perceptions of barriers to communication.
Patients’ perspectives
According to the patients, the barriers to effective patient–provider communication are the use of medical jargon, the patient–provider relationship, the lack of trust between patients and providers, the absence of visual cues in the educational materials and the time constraints.
Medical jargon
Many patients stated that providers frequently used medical jargon in their communication and that this impeded their understanding of their disease and treatment options. Difficulty in understanding medical terms was associated with insufficient literacy skills or unfamiliarity with the specific medical condition they are suffering from. One patient said, “[what makes it difficult for me to understand is] medical terminology. Then there are long words I have no idea. As I said, I have got, like a grade 5, maybe grade 4 now understanding of words and … you just … if I can’t make out the word, I skip over it and I lose the whole concept” (AB 4).
Another patient referred to the difficulty in understanding “Latin words” and elaborated “Well … I mean, initially when I got diagnosed they kept calling it … in my case they kept calling it tracheobronchomegaly and I didn't know what that was, and there was very little information on that particular name on the Internet at the time” (AB 5).
Patient–provider relationship
The HCPs’ personality and approach to building relationships with patients was also mentioned as a barrier to communication. While most patients expressed satisfaction in the quality of care they were provided with at the center, many talked about the “unapproachability” of some of their providers. Patients underlined the importance of building a “trusting” relationship with their providers that would enable them to freely approach them and ask questions and seek information. The absence of such relationship, patients said, may lead to a lack of trust and therefore, reluctance to inquire about their disease. One patient talked about the positive characteristics of her providers that had helped her adjust. She said “I feel that they have … here they have all been extremely helpful; kind, considerate and pleasant to deal with. They will tell me any thing about myself that I need to know” (AB 1). Another patient had a similar experience. She elaborated, “You have the OTs [occupational therapists]. You have the nurses. You have the doctors. And if you have any questions, I usually go up and ask the doctor and she'll look it all up and get the information for me. And I’ve seen a couple other doctors here, and they took their time explaining about the situation and it really helped” (AB 3).
The providers’ dialect or lack of language proficiency were also mentioned as sources of difficulties in communicating information.
Time constraints
Although patients acknowledged that the providers’ busy schedule and number of patients did not allow them to spend more time with each patient, they believed that the “little time” they spent with their providers was insufficient for them to ask questions and clarify misunderstandings. One patient said, “[one barrier is the providers’] availability … they're very fast here. I also go to [another hospital’s name] for respiratory care there and the doctor there allows more time, and he's the one who actually sits down and explains things to me. 'Cause he knows the cardiologist and they talk and I would like them all to be [more attentive]” (AB 4) and, another patient said that “[one of the providers] … he's … he's very pleasant, and easy to deal with, but … he does give the impression that his time is valuable ([faint] mm-hmm) that you shouldn't waste it. But when there's something that … that needs to be discussed, he will discuss it” (AB 2).
Another patient commented, “You know, I go to a see … I go to an appointment with Dr. [name withheld], for example and, you know, the wait might be five minutes whereas I've gone to other respirologists and I'm in the waiting room for an hour, which is … I mean, time … time is important to a lot of people and we all have, um, a schedule that we try to follow, and when you go to another doctor's office, especially in downtown Toronto for example, and you're waiting for an hour before he sees you … well, granted I understand they're busy, but … that's … you know, sometimes it's unfair” (AB 5).
Providers’ perspectives
In discussing their perceptions of barriers to effective patient–provider communication, the providers mentioned the following factors: the patients’ culture and language, the patients’ characteristics, the lack of awareness of available resources, organizational factors and the stigma of low-literacy patients.
Patients’ culture and language
HCPs unanimously referred to patients’ culture and language as the main barriers to effective communication. In describing cultural barriers, one of the providers commented, “I realize there are sometimes cultural barriers as important as language barriers because when I go to Persian patients, the way I greet them has an impact on how they open up to me, giving me the information. And sometimes I hear from other people that they couldn’t get this information from the patient simply because they felt they were dealing with a stranger. But you go in from their own culture, those doors that are closed, they open up to you.” HCPs identified that a patient’s lack of language proficiency was a signal that they should expect some level of communication difficulty, as evident in this quote, “There are probably a few factors that go into that. First thing would be language. I'm mostly … comfortable in English and in French. I have had a couple of patient interactions in Hebrew but not to any great extent. And in hand gestures Italian, but if my patient cannot speak fluent English or French, or even workable English or French – workable enough to have a reasonable conversation, I mean, not necessarily even in a medical sense, but for a casual man in the street conversation, then right away that's the first flag that communication is going to be difficult and that person will have a hard time understanding … or I will have a hard time getting the message across.”
Medical jargon
HCPs also considered the use of medical jargon as a barrier to understanding. One stated, “my perception is that when we do patient education we have classes here but after, we use medical language which is not understandable to many patients.” One of the physicians acknowledged the disadvantages of using of medical jargon when speaking with patients but also referred to the providers’ intuitional use of their professional language. She said, “A lot of our terminology in medicine is almost a separate language really, it's not part of day-to-day language and we try to put it in a lay person's language, but the further you go on in medicine, probably the worse you get at doing that as that language to you becomes more day to day.”
Patients’ characteristics
Characteristics such as age and personality also play a role in patient–provider communication. One of the providers stated, “For some people (providers) it's easy and they do a good job. Maybe it comes naturally to them or maybe they have spent a little bit more time looking at how adults learn or how to deal with an older population, because [reduced] health literacy sometimes goes with an ageing population. So [for example] when you're 85, and you can't see very well, and you can't hear very well and your sensation isn't very good and you're asked to fill out a consent form with tiny print, right? So that's the kettle of fish just dealing with an ageing population meaning you can go into the 80s and even to the 90s.” Another barrier to communication might be the patient’s cognitive ability. As one of the providers mentioned, “sometimes, it’s just that they don’t have the competency or maybe the cognitive level to understand and so, right away from the diagnosis, you can tell that maybe they don’t have the competency or the cognitive ability to comprehend.”
Organizational factors
Organizational factors refer to barriers within the organization that impede communication, such as time constraints, funding and lack of available resources for the providers to improve communication. HCPs acknowledged time constraints as one of the main barriers to spending sufficient time with their patients to ensure their understanding of their disease and medical instructions. A provider explained, “The other thing is whether we have the time to sit down and explore and find out how much they understand. We’re rushed, from one patient to another, from one classroom to another, and we don’t have the time to sit down and really explain, to ask questions, to see how much they do understand, because not just the verbal communication, but also through nonverbal communication, you can pick up stuff. But sometimes you are busy and you don’t have the time to finish.”
Stigma of low-literacy patients
Shame and embarrassment of being labeled as low literate was mentioned as one of the causes of patients’ reluctance to ask questions. One of the providers said, “What I have noticed in particular is that sometimes people have language skills that are not too bad, but they just think, they are ashamed, maybe they are afraid to speak. When they are for a while in a program, all of a sudden you find out that they are not so bad in language and that they can actually communicate.” HCPs also mentioned that many patients, regardless of their education and language proficiency, do not speak up in patient education classes for the fear of “appearing dumb,” or are too “shy to admit lack of understanding.”
Resources that facilitate communication of medical information
Participants were asked about the types of resources (personal and organizational) and strategies that might have a positive impact on patient–provider communication. In defining communication strategies, we used the definition proposed by the WHO which defined communication strategies as “Ways to inform the public about health concerns and to maintain important health issues on the public agenda. The use of the mass and multi media and other technological innovations to disseminate useful health information to the public, increases awareness of specific aspects of individual and collective health as well as the importance of health in development.”1 Similarly, resources refer to all materials (print and multimedia), programs, personnel, funds and all other services that can be utilized to provide health information and care for patients.
Patients’ perspectives
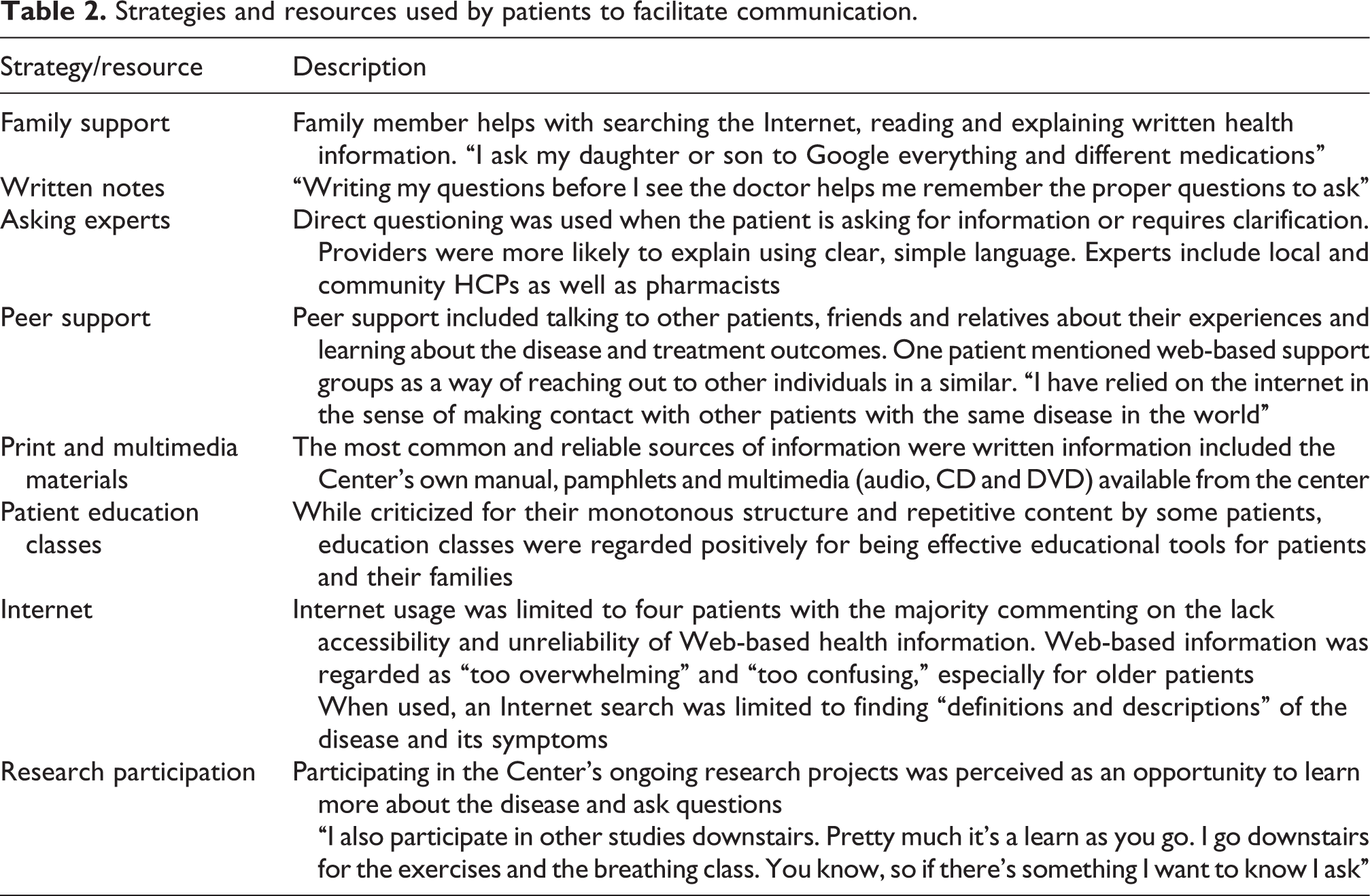
Patients were aware of problems that might arise in patient–provider communication and utilized diverse strategies to facilitate communication. These strategies and resources are summarized in Table 2.
Strategies and resources used by patients to facilitate communication.
Providers’ perspectives
HCPs discussed different strategies and resources that they commonly used in order to foster effective patient–provider communication. These strategies and resources are summarized in Table 3.
Strategies and resources used by providers to facilitate communication.
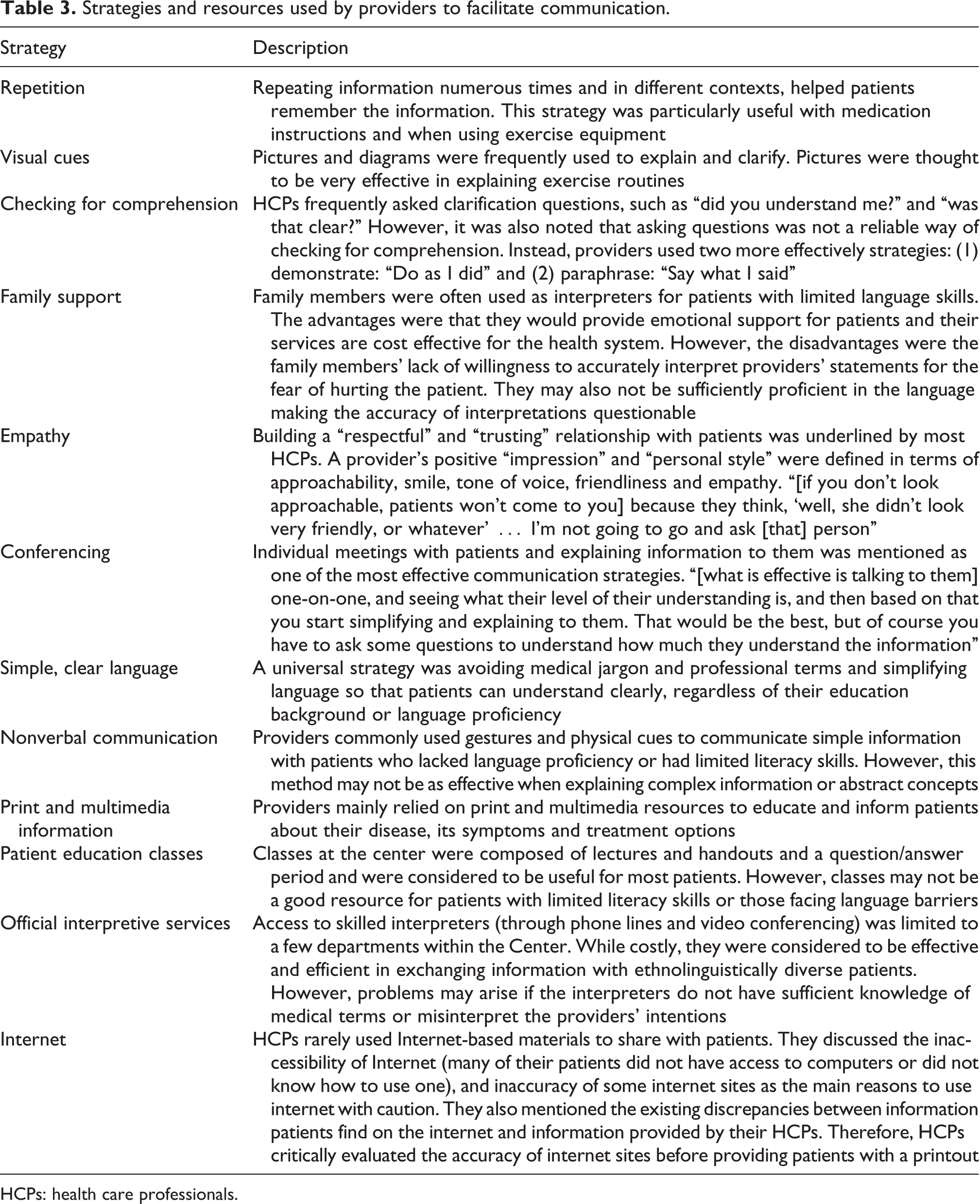
HCPs: health care professionals.
Discussion
This is the first qualitative study that has (1) investigated how COPD patients and providers perceive HL, (2) explored barriers to patient–provider communication and (3) identified strategies that might improve communication. It extends previous reports regarding the potential for reduced HL to affect physician communication and health status. 9. 19
With respect to definition and significance of HL, most patients had no previous knowledge of HL but were nevertheless able to define it in terms of knowledge of their disease and as a tool for effective patient–provider communication. They also underlined the role of HL on self-management, health promotion and access to health care services.21–24 Most HCPs were familiar with HL through the media or through the Center’s professional development programs. They associated it with the patients’ ability to seek and understand health-related information and recognized its impact on effective provision of health information to patients. HCPs noted that HL could impact on health through an understanding of symptoms, treatments options, self-management and effective communication.
With respect to barriers to communication, all participants identified the overuse of medical jargon and HCPs time constraints as overarching barriers. Patients stressed the importance of the providers’ personality, approachability and empathy, when building a trusting relationship. HCPs identified the patients’ language, culture, age, cognitive ability, scarcity of resources and low literacy, as inhibiting their understanding of health information. Provider focus groups and interviews both acknowledged that the fear of being shamed hindered the resolution of communication breakdowns between patients and their caregivers.25–27 This increased patient vulnerability and reduced their willingness to request clarification regarding points of importance to their condition.
In identifying approaches to improve patient–provider communication, all participants noted that factors encouraging of improved communication included family support, Internet and other patient education programs. While the Internet was regarded as an effective tool for finding health information, it was sometimes inaccessible to people unaccustomed to using it as well as those with restricted financial resources. Patients mentioned peer support, multimedia resources and verbal inquiries as ways to improve their understanding of their disease. It has been recognized that speaking regularly to their providers improves a patient’s understanding of health information.28–30 Patients regarded participating in ongoing research projects as an opportunity to ask questions and learn about their disease. They identified peer support could include being connected to other patients as well as online communities and perceived that this sharing of information helped their gaining knowledge about the treatment options and possible outcomes of their condition. HCP providers commented that they repeat information, using simple language, as well as visual cues to improve communication with their patients. They also emphasized that spending “one-on-one time” with patients to explain detailed information as the most effective communication strategy. Using family members and friends as interpreters, although cost effective and accessible, may not always provide the most reliable information as the interpreters may not be able to accurately translate medical terms. Their reluctance to share negative news on health and prognosis also might result in their making subtle changes to content. In contrast, although professional interpretation services are likely more accurate, they are also costly and less readily available. Even professional interpreters may not be familiar with medical terms and the lack of interpersonal connection with the patient may inhibit the patient from freely asking question through the interpreter.
Although the study sample was from a single large pulmonary rehabilitation center with staff from all disciplines engaged in the communication of health care information, the information may not be generalized to the broader COPD population as disease severity, patient characteristics, social circumstances and HL might well differ in different jurisdictions. Interviews were restricted to patients who were fluent in English. A sample that included patients from more diverse cultural and linguistic backgrounds might have yielded a broader understanding of the patient’s perspectives and experiences of HL as a barrier to communication. There absence of formal HL testing of the patient population interviewed denied the opportunity of actually matching their comments to an objective measure. However, although there are some measures of HL that have been used in the population of patients with chronic disease, there is no standardized measure with documented validity, reliability and interpretability.31–34
The above findings provide an opportunity for physicians engaged in pulmonary rehabilitation to better understand and therefore respond to what patients and HCPs identify as the impact of HL on communication. Many of these barriers, such as time constraints, the use of medical jargon and patient–provider relationships can be addressed within the educational component of the pulmonary rehabilitation program. Other issues such as family support at home, sharing experiences with other patients and accessing information can be encouraged through peer support groups, chat lines and the development of easy to comprehend multimedia educational materials. Awareness of the impact of HL may be integrated into clinical practice by the rehabilitation team in order to enhance the patients’ knowledge of their disease, their ability to self-manage and their adherence to health care recommendations.
Conclusion
These findings provide insights into the COPD patients’ and providers’ perceptions of HL, their understanding of barriers to effective communication and ways in which these barriers may be reduced. Both patients and care providers identified HL and the use of clear simple language as determinants of health outcomes. They also noted the importance of a trusting empathic relationship in promoting good health. This study highlights the importance of an awareness of factors that might improve the exchange of health information between patients and providers. Such information should be included in health provider training programs.
Footnotes
Appendix A. Interview and focus group questions
Funding
This project was funded by West Park Hospital Foundation and by an unrestricted educational grant from GlaxoSmithKline Inc. Dr Roger Goldstein is supported by the National Sanitarium Association, University of Toronto, Chair in Respiratory Rehabilitation Research. Dr Dina Brooks is supported by a Canada Research Chair (Tier 2).