
Abstract
To investigate predictors of accelerated decline in forced expiratory volume in 1 s (FEV1) in individuals with preexisting airflow limitation (AL). Participants in the Health2006 baseline study aged ≥ 35 with FEV1/ forced vital capacity (FVC) < lower limit of normal (LLN) were invited for a 10-year follow-up. At both examinations, data were obtained on demographics, spirometry, fitness level, allergy, and exhaled nitric oxide. We used multiple regression modeling to predict the annual decline in FEV1, reported as regression coefficients (R) and 95% confidence intervals (CIs). A total of 123 (43% of those invited) participated in the follow-up examination, where more had exercise-induced dyspnea but fewer had asthma symptoms. Being female (R = −29.8 ml, CI: −39.7 to −19.8), diagnosed with asthma (R = −13.7, CI: −20.4 to −7.0) or atopic dermatitis (R = −29.0, CI: −39.7 to −18.4), and having current asthma symptoms or nightly respiratory symptoms (R = −22.1, CI: −31.9 to −12.4 and R = −14.3, CI: −19.9 to −8.7, respectively) were significantly associated with a steeper decline in FEV1. Although to a smaller extent, a steeper decline was also predicted by age, baseline FEV1, waist/hip-ratio, and number of pack-years smoked. In individuals with preexisting AL, being female and having ever or current respiratory symptoms were associated with an accelerated annual decline in FEV1.
Keywords
Introduction
Since the study published in 1977 by Fletcher and Peto, 1 it has been widely accepted that forced expiratory volume in 1 s (FEV1) gradually declines throughout adulthood. Studies addressing annual decline of FEV1 in both chronic obstructive pulmonary disease (COPD) 2,3 and asthma 4,5 have shown a greater decline than in individuals with no history of obstructive airway disease. However, a very high degree of variability in decline within both COPD and asthma has been reported, 2 –4 making it hard to risk-stratify individuals based solely on their level of lung function, especially in early stages of airflow limitation (AL).
Most studies on the course of FEV1 over the life span have been conducted in either large population cohorts 5,6 or in individuals with known asthma or COPD. 2 –4 However, increasing focus on the heterogeneity of both asthma, not least in adults, and COPD, as well as recognition of the overlap between the two, 7 –11 warrants studies where these airway diseases are deconstructed into traits that can be measured, with the overall aim of potentially identifying traits or factors that can be modified and lead to an improvement in outcome. AL is seen not only in patients labeled as having either asthma or COPD but also in asymptomatic individuals. Studying predictors of long-term outcome in individuals with AL in general, irrespective of a diagnostic label or not, may thus add knowledge useful for predicting future risk in individuals with this trait. Another potential gap in the available studies of FEV1 decline is that most are solely based on spirometry data, smoking history, and self-reported symptoms. A more multifaceted approach, including more detailed information on symptoms and objective assessments, may therefore be of importance, as a wide variety of characteristics are likely to influence the rate of decline in lung function.
Therapeutic trials have so far been the most promising regarding asthma, 12 –15 not showing desired results in COPD. 16,17 Prevention, mainly in the form of smoking cessation, 18,19 is preferable by far, and early initiation is crucial. 20 AL can be detected easily through spirometry. Although underdiagnosing of COPD is a known problem, 21,22 screening is not recommended in asymptomatic smokers. 23 In a large cohort study of individuals at high risk of COPD, Colak et al. found 78% of those meeting the spirometric criteria for COPD (pre-bronchodilator (BD) AL, plus a FEV1 < 80% predicted) not to have been previously diagnosed, although only 29% of these individuals were asymptomatic. 24 Thus, waiting for individuals to recognize, and respond to, symptoms of a low lung function can result in an already extensive damage before receiving a diagnosis.
With this 10-year follow-up study, we aimed to identify predictors of decline in FEV1 in individuals with AL at baseline, in hope of providing knowledge to assist in early detection of individuals at high risk of progressive AL.
Methods
Material
For this study, we focused on a subgroup (n = 313) from the Danish Health2006 cohort. 25 We selected participants who, at the baseline examination, were 35 years or older and had a FEV1/FVC ratio < lower limit of normal (LLN, 5% percentile). 26 Invitations were issued via post, with reminder letters sent after 3 and 9 months. A final reminder was sent after 12 months, including a copy of the questionnaires and a prepaid return envelope. Participants were deemed unresponsive if not having responded 3 months after the final letter.
Examinations
All examinations were performed in all participants at both baseline (2006–2008) and follow-up (2016–2017) if not otherwise stated. A detailed description of the examinations has been published elsewhere. 25
Questionnaires
All participants answered questionnaires on perceived health, known diseases (including, e.g. eczema, rhinitis, and asthma), physical activity level, dietary habits, alcohol, smoking habits, hormone replacement therapy, family and social relations, education, and work.
Anthropometric measures and obesity
Height, weight, and hip- and waist-circumference were measured. Body fat percentage was determined using impedance.
Fitness level
Fitness level was measured through the Danish Step Test: 27 a test with fixed step height but increasing pace up to a maximum of 6 min.
Sensitization to specific aeroallergens
At baseline, skin prick testing was only performed in a subgroup of participants, at follow-up in all participants. Skin prick testing for 10 aeroallergens (birch, grass, mug wort, horse dander, dog hair, cat hair, Dermatophagoides pteronyssinus, Dermatophagoides farinae, Alternaria alternate, and Cladosporium herbarum) was performed using the Soluprick (ALK-Abelló A/S, Hørsholm, Denmark). Participants were considered sensitized to allergens if developing a wheal with a diameter larger than 3 mm. Specific immunoglubline E (IgE) to the most common aeroallergens, that is, birch, grass, cat, and D. pteronyssinus, was measured and considered positive if >0.35 kU/l.
Lung function
Lung function was measured according to the American Thoracic Society/European Respiratory Society (ATS/ERS) standards, 28 at baseline with a SpiroUSB (Micro-Medical Ltd, Rochester, UK), and at follow-up with a Vitalograph 6800 pneumotrac (Hamburg, Germany), primarily because the SpiroUSB was not available at the time of the follow-up examination. Predicted FEV1 was calculated based on height, age, and sex. 29
Fractional exhaled nitric oxide
Fractional exhaled nitric oxide (FeNO) was measured with Niox-Mino (Aerocrine AB, Solna, Sweden) according to ATS standards. 30
Definitions
Participants were defined as never-smokers or ever-smokers (former or current) by answering the questionnaire item Do you smoke? with the options Yes, No, but I have previously, or No, never. Pack-years were calculated by multiplying the duration (years) with intensity (grams tobacco per day, with 1 cigarette equating to 1 g, a pipe or cheroot to 3 g, and a cigar to 5 g of tobacco). Regarding alcohol consumption, participants were defined as nondrinkers if they had a weekly consumption <1 international unit. Body mass index (BMI) was divided into the following groups: underweight (<18.5), normal weight (18.5–24.99), overweight (25–29.99), and obese (>30). 31
Statistical analysis
All analyses were done in IBM SPSS Statistics, V.24. For differences between baseline and follow-up, we ran Paired T-test for continuous, McNemars test for dichotomous, and Wilcoxon signed rank test for ordinal variables. Missing data, primarily unanswered items from the questionnaires with different items in different cases and fitness tests not undertaken due to musculoskeletal problems were considered missing at random and were dealt with by multiple imputation in SPSS. Results are reported as either percentage of group or mean (SD).
A multiple linear regression analysis with backward stepwise deletion of nonsignificant variables was run to predict decline in FEV1 from clinical and self-reported variables. All variables included in the final model added statistically significance (p < 0.05). Results from the regression analysis are reported as unstandardized regression coefficient (R), unstandardized standard error (SE), and 95% confidence interval (CI).
Results
Follow-up cohort
Of the 313 eligible for invitation 19 were deceased since baseline, and we were unable to obtain valid contact information on six. Invitations were sent to the remaining 288 participants.
A total of 123 (42.7%) participants were examined, another 21 filled in and returned the questionnaires by mail (Figure 1).

Flowchart over inclusion process of participants from the Health2006 cohort.
The analyses in the present study are based on data from the 123 individuals who participated physically in both examinations. Compared to the 165 eligible, but not participating individuals, participants in the follow-up examination were at baseline more likely to be current smokers (p < 0.05), have a positive skin prick test (p < 0.02) and positive specific IgE (p < 0.01), but less likely to have chronic bronchitis (p < 0.01) and diabetes (p < 0.05). The mean fitness level (NS) and weekly alcohol consumption (NS) were slightly higher in the 123 who participated at follow-up, otherwise the follow-up group was representative of the entire group eligible for invitation to participate in the present study.
During the 10 years from baseline to follow-up, 24 participants had quit smoking (and none started). At follow-up, a greater proportion of participants experienced exercise-induced dyspnea, while fewer had symptoms of rhinitis or asthma (Tables 1 and 2; Figure 2). Mean decline in FEV1 was 28.2 ml/year (SD: 31.6 ml), with a broad range of annual change from a 128 ml decline to a 64 ml increase.
Self-reported characteristics of participants in the Health2006 follow-up study at baseline and follow-up (n = 123).a

aNumbers reported as mean (SD).
bCalculated for participants with a current or former history of smoking.
cCalculated for participants who reported a current alcohol consumption only.
dCalculated for participants reporting a diagnosis of asthma only.
eCough with sputum for at least 3 months/year for at least 2 consecutive years.
fMeasured on a scale from 1 to 5, where 1 is best.
Clinical characteristics of participants in the Health2006 follow-up study at baseline and follow-up (n = 123).a
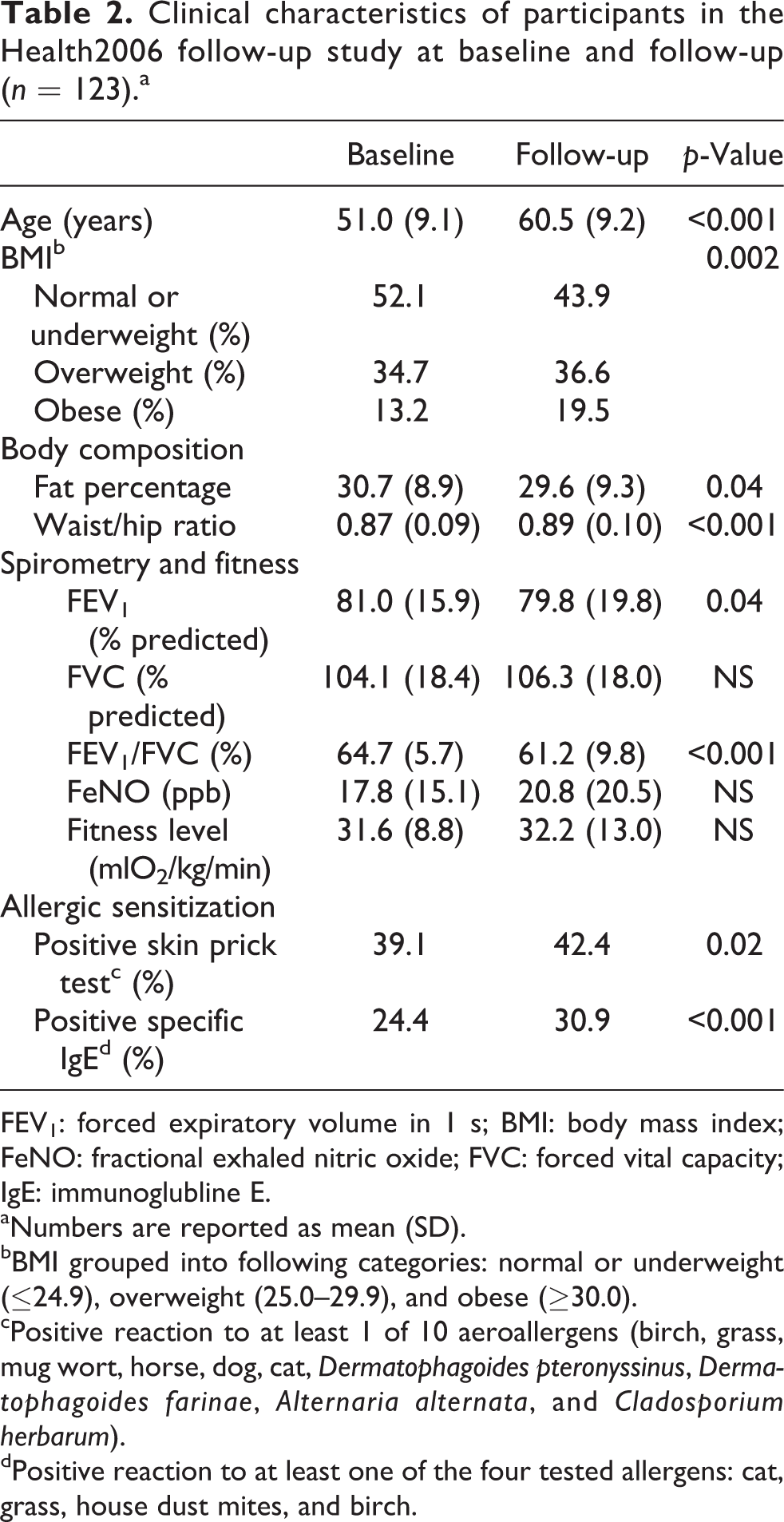
FEV1: forced expiratory volume in 1 s; BMI: body mass index; FeNO: fractional exhaled nitric oxide; FVC: forced vital capacity; IgE: immunoglubline E.
aNumbers are reported as mean (SD).
bBMI grouped into following categories: normal or underweight (≤24.9), overweight (25.0–29.9), and obese (≥30.0).
cPositive reaction to at least 1 of 10 aeroallergens (birch, grass, mug wort, horse, dog, cat, Dermatophagoides pteronyssinus, Dermatophagoides farinae, Alternaria alternata, and Cladosporium herbarum).
dPositive reaction to at least one of the four tested allergens: cat, grass, house dust mites, and birch.

Characteristics of participants from Health2006 (n = 123) at baseline and follow-up. *Self-reported symptoms during the previous 12 months. #Doctor diagnosed at any point in life.
Predictors of decline in FEV1
In the multiple regression analysis, we ended with a final model which statistically significantly predicted loss of FEV1 (p < 0.001, adjusted R 2: 0.28). Independent variables did not show multicollinearity, assessed by both correlation coefficients and tolerance values. All variables included in the final model are given in Figure 3.

Regression coefficients for prediction of decline in FEV1 at follow-up for participants at the Health2006 cohort (n = 123), change in ml per year per 1 unit increase in each variable, unless otherwise stated. *Per 10 unit increase. €On a scale of 1-5, where 1 is best. #Per 0.1 unit increase. FEV1: forced expiratory volume in 1 s.
Variables predicting a greater decline in FEV1 were heterogeneous in character. Women lost nearly 30 ml more in FEV1 per year than men (R = −29.8, CI: −39.7 to −19.8, p < 0.001), same as participants ever diagnosed with atopic dermatitis compared to those without (R = −29.0, CI: −39.7 to −18.4, p < 0.001). Ever receiving a diagnosis of asthma also predicted a greater decline in FEV1, but to a smaller extend (R = −13.7, CI: −20.4 to −7.0, p < 0.001). Both symptoms of asthma (R = −22.1, CI: −31.9 to −12.4, p < 0.001) and nightly respiratory symptoms (R = −14.3, CI: −19.9 to −8.7, p < 0.001) in the 12 months prior to the baseline examination predicted a greater decline in FEV1. In contrast, a higher fitness level was the most prominent predictor of a smaller annual decline of FEV1 (R = 8.7 ml per 10 units increase, CI: 5.0 to 12.4, p < 0.001). All regression coefficients (R), SEs, and CIs are given in Table 3.
Multiple regression analysis for prediction of annual decline in FEV1 over time in participants from the Health2006 cohort (n = 123) with airflow limitation at baseline.a

FEV1: forced expiratory volume in 1 s; SE: standard error.
aRegression coefficients are reported as change in ml per year per 1 unit increase in each variable, unless otherwise stated.
bPer 10 unit increase.
cOn a scale of 1–5, where 1 is best.
dPer 0.1 unit increase.
Discussion
In this population-based, follow-up study of individuals with preexisting AL, we found that the decline in FEV1 ranged considerably between participants. The main predictors of accelerated decline in FEV1 were being female, having respiratory symptoms and ever being diagnosed with asthma or atopic dermatitis.
There is an ongoing debate over which definition of AL to use; FEV1/FVC < LLN, or the more straightforward FEV1/FVC < 0.70. Using the traditionally applied fixed ratio (FEV1/FVC < 0.70), there may be over diagnosing in the older population and underdiagnosing of the younger. 32 Underdiagnosing has also been a point of critique for using LLN, missing those with milder degrees of airflow obstruction. 33 In the tiotropium trial TIOSPIR, Calverley et al. 34 found that the participants who would have been excluded using LLN had the same risk of death and cardiovascular events as the remaining participants in the trial, although a lower risk of exacerbations. On the other hand, Colak et al. 35 found increased cardiovascular morbidity and early death in those underdiagnosed using fixed ratio, compared to LLN. Recently, Miller et al. found that using fixed ratio only, a large group of individuals were diagnosed with COPD, who might simply have an age-related lower lung function, and symptoms due to cardiovascular problems, and not necessarily COPD. 36 Finally, Akkermans et al. 37 found that the decline in FEV1 in those diagnosed with airflow obstruction based on a fixed ratio was close to those deemed non-obstructed, compared to those with obstruction based on LLN. Whichever definition of airflow obstruction is chosen, whether for interventional or explorative studies, researchers have to decide either to risk inclusion of individuals with age-related AL or exclusion of primarily younger individuals with negative normal FEV1/FVC ratio. For the present study, we decided, also based on the age distribution in our cohort, to define AL based on FEV1/FVC < LLN.
Decline in FEV1
The mean decline observed in our study in FEV1 is comparable to other observations—both in studies of individuals with asthma or COPD and in studies of the general population. van Oostrom et al. 6 found different trajectories of FEV1 in a general population, where the decline in those with a normal course (trajectory in line with reference values) was 31.1 and 25.9 ml/year for men and women, respectively. Lange et al. 4 analyzed the changes in FEV1 in a large cohort over 15 years and found that people who reported having asthma had both a lower FEV1 at inclusion and a steeper decline in FEV1 over time, compared to those without asthma (38 vs. 22 ml, respectively). In patients with known COPD, Vestbo et al. 2 found a mean decline in FEV1 of 33 ml/year, the most prominent predictors of decline in FEV1 being smoking, exacerbations, emphysema, and BD reversibility. The traditional view was that an accelerated decline in FEV1 over time, due to tobacco smoking, leads to COPD. 1 However, FEV1 at a given point of life is determined not only by rate of decline, but also by the peak level attained in early adulthood. 5,38,39
More than 10% (n = 15) of our cohort had an increase in FEV1 over the 10 years between baseline and follow-up. They were more likely to be men and had a baseline FEV1 nearly 12% lower than the remaining cohort. The large variation could be due to technical issues with spirometry, natural, spontaneous variation in participants with asthma or a result of regression toward the mean. Some participants might also have been unaware of their low lung function when entering the cohort, subsequently being examined and possibly started on treatment by their physician. This could have led to an initial increase in FEV1, resulting in the higher value at follow-up than at baseline. Vestbo et al. 2 also found a considerable between-subject variation, from over 200 ml decline to over 100 ml increase per year. In patients with COPD, Zafari et al. 3 found a change in FEV1 ranging from a 124 ml/year decline to a 15 ml/year increase.
Predictors of decline in FEV1
Smoking
Several studies have shown that smoking is a determinant of decline of FEV1. 2 –6 We didn’t find an effect of smoking status, and the effect of pack-years was not of a substantial size, with barely 3 ml greater decline per year per 10 additional pack-years. The divergence in results could be due to the type of study population, as both Vestbo et al. 2 and Zafari et al. 3 studied populations with known COPD, and thus a smoking history. Participants with asthma have been shown to be more susceptible to the detrimental effect of smoking than non-asthmatics. 4,5 However, when performing linear regression for those with a smoking history only, the decline was only found to be 5 ml greater per 10 pack-years. The differences in effect of smoking may also simply just be a problem regarding power due to the size of our cohort.
Sex
As FEV1 is affected by height, and men are usually taller than women, one would expect men to have a greater decline over time than women. Neither Lange et al. 4 nor Vestbo et al. 2 reported a marked between-sex difference, and Zafari et al. 3 only found a 8.9-ml greater decline in women than men. In contrast, we found women to have a much steeper decline in FEV1 than men, more than twice the yearly decline. Analyzing only individuals with a low baseline FEV1 weakened the effect of sex. Although women had a higher mean FEV1% predicted, their mean absolute FEV1 was, as expected, lower than in men (results not shown). Thus, it is not a case of a greater decline due to a greater volume at onset.
Fractional exhaled nitric oxide
We found a high FeNO to be associated with a slower decline in FEV1. In contrast to our findings, van Veen et al. 40 found that having a high FeNO (>20 ppb) predicted over 40 ml greater loss per year compared to having a low FeNO (<20 ppb). However, their study was on non-smoking, difficult-to-treat asthmatics. Smoking is known to lower FeNO. 41 With the number of smokers at baseline, FeNO was likely suppressed, and “high” FeNO might represent normal values, compared to the lower FeNO in smokers. FeNO is higher during rhinovirus infections, which may also result in a lower lung function. If having a common cold at baseline could result in both higher FeNO and lower FEV1, the resulting loss over time may be underestimated. Participants were asked to cancel their appointment in the case of illness, but some could have forgotten.
Alcohol
Our finding of a relationship between higher alcohol consumption and a slower decline in FEV1 seems peculiar. Lange et al. 42 found that the effect on FEV1 decline by a high alcohol consumption (350 g per week or more) was equivalent to 15 g of tobacco daily, while Schünemann et al. 43 found no correlation between total alcohol consumption and lung function decline, but on the other hand a positive relationship between wine drinking and change in FEV1, which is most likely due to confounding by a healthier lifestyle in wine drinkers. The mean weekly consumption in our cohort was around 130 g, and by that substantially lower than that in the cohort of Lange et al., 42 which may explain some of the differences in observations. However, the coefficient for alcohol consumption in our study was not very large, only 2.9 ml per 10 units of alcohol or more per week, which is not likely to be clinically relevant.
Body composition
We found no statistically significant association between BMI and decline in FEV1. However, a high waist/hip ratio predicted a steeper decline in FEV1, whereas a higher bodyfat percentage predicted a slower decline. Other studies on the effect of obesity on lung function have shown inconsistent results, from no effect 44 to a significant effect. 45 In mild to moderate COPD, Landbo et al. 46 observed a U-shaped curve for mortality risk with the lowest risk in normal to overweight participants. On the other hand, for severe COPD, the association was more linear with increasing risk of mortality for decreasing BMI. Our results may reflect a similar relationship, with a higher fat percentage being advantageous for FEV1 until a certain point.
Limitations and future perspectives
With our study being epidemiologically based, it has an inherent set of potential biases. First, participants in the original Health2006 cohort may not be representative for all invited individuals or for the background population. Thuesen et al. 25 found nonparticipants to be younger, more often male, with a shorter education and lower income than participants in Health2006, as well as having more hospital admissions. Thus, the external validity of the baseline examination might be suboptimal. Second, we found differences between those who accepted our invitation to the follow-up examination and those who either declined, did not respond, or were deceased. Attrition bias, with the most affected participants at baseline being more likely to not attend a follow-up examination, is very likely. Our participation rate was 43%, comparable to the rate in the baseline examination, 25 while some other Danish cohorts have had higher participation rates. 4,47 As participants in our cohort all had AL, it might explain our lower participation rate at follow-up, as nonparticipants might simply be too frail. Due to our closed cohort, we did not have the option of recruiting additional participants, as other long-term studies have done. We had originally calculated a sample size of 200 participants to be able to detect a 10 ml difference in annual decline of FEV1. With the 123 participants included, our minimal detectable difference was thus larger than 10 ml. Finally, recall bias is always a possibility in studies relying on self-reporting from participants, and with many of our data points being based on questionnaires, the internal validity might be affected.
As we found a diagnosis of asthma to be a predictor of decline in FEV1, and other studies have shown accelerated decline in participants with COPD, it seems legitimate to assume that we could have found similar results. Unfortunately, at baseline, the questionnaire did not include an item regarding previously diagnosed COPD. However, self-reported symptoms of chronic bronchitis were not associated with an accelerated decline in our analyses.
Another consideration is the lack of information between the baseline- and the follow-up examinations. Had we had more points of data over the years, it would have been a more accurate calculation of trajectories, as well as possibly explaining the few outlying cases, such as the participants experiencing an immense improvement in FEV1. Combined with more information, for example, on the use of inhaled medication over the years of follow-up and seasonal variations, more data points would probably have given us a better fitted model.
Our values of FEV1 were all without BDs, as the baseline examinations had not included reversibility testing. Most studies use post-BD values. Participants with more asthma-like traits could have a higher post-BD FEV1, compared with a more COPD-like participant with a more fixed FEV1, thus potentially skewing the effect of variables such as number of pack-years.
Medication has been shown in observational studies to slow the decline in FEV1 in patients with asthma, 12,15 and initially improve FEV1 in COPD. 48 In future studies, it would be interesting to link our cohort to the prescription databases, to look for treatment patterns in participants, at baseline as well as over time. It would also be of interest to see if the individuals declining participation in follow-up, as well as those deceased since baseline, had characteristics differing markedly from those participating in the follow-up.
In conclusion, in individuals with preexisting AL, we found the main predictors of a steeper decline in FEV1 to be female, have respiratory symptoms, and ever being diagnosed with asthma or atopic dermatitis. Our results lay the foundation for future analyses, and, adjusted for the shortcomings of the present study, may potentially help clinicians targeting the high-risk individuals for a more personalized intervention strategy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.