
Abstract
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is characterized by airflow obstruction and the main symptoms are dyspnea and fatigue. Furthermore, individuals with COPD present systemic manifestations such as body composition abnormalities, systemic inflammation and skeletal muscle dysfunction. 1 This scenario of symptoms and dysfunctions leads patients to be less active in daily life compared to healthy elderly and, in general, to be physically deconditioned. 2 Solid scientific evidence based on objective monitoring of physical activity (PA) have shown that individuals with COPD spend a very large part of the time during the day in sedentary positions (e.g., sitting)3,4 and/or in activities of very low energy expenditure. 5
Widely accepted recommendations by the American College of Sports Medicine (ACSM) indicate that, in order to maintain or improve health, adults are required to perform at least 30 min/day of moderate intensity PA for 5 days/week (150 min/week) or 20 min/day of vigorous intensity PA for 3 days/week (60 min/week) .6,7 According to the ACSM, individuals are classified as physically active if they fulfill these recommendations; otherwise, they are classified as physically inactive.
In individuals with COPD, the level of physical activity in daily life (PADL) is related to a higher risk of exacerbations and mortality.8,9 It is recommended that PADL assessment is performed objectively by using valid and portable PA monitors since they are able to quantify time spent in activities such as walking and in body positions (i.e., standing, sitting, and reclined) during a given period. 10 Moreover, the use of these PA monitors also allows to estimate energy expenditure (EE), a reflection of PA intensity. Therefore, by using these monitors it is possible to classify whether the individual is active or inactive in daily life according to the abovementioned ACSM recommendations.6,7 However, while time spent in PA has been widely investigated in COPD, to the best of our knowledge there is no previous description yet in the literature about EE/minute, that is, EE classified on a minute-by-minute basis in real life during walking and different body positions (i.e., standing, sitting, and reclined). Perhaps even more importantly, it is yet unknown if EE/minute walking predicts the classification of an individual as physically active or inactive, or if this is essentially determined by the time spent walking. This analysis is novel in the literature and provides a detailed “minute-by-minute” picture of the individual’s PA characteristics, therefore fine-tuning data that could otherwise be more superficially reported as “averaged.” Therefore, this study aimed to describe and compare EE/minute walking and in different body postures in individuals with COPD; and to investigate if EE/minute walking is a predictor of these individuals’ classification as physically active or inactive according to the ACSM classification.
Methods
Ethics, design, and sample
The study was developed at the Laboratory of Research in Respiratory Physiotherapy (LFIP) of the State University of Londrina (Brazil) from August 2016 to May 2020. The project was approved by the institutional Research Ethics Committee (no.1.730.247/2016). All subjects were carefully informed about the procedures and provided written informed consent to take part in the study.
This study concerns a retrospective analysis of baseline assessment data from patients recruited for admission in an outpatient-based physical training program from an ongoing study in the same centre (Clinical Trials: NCT01537627). These patients underwent routine medical consultation with a pulmonologist in the public health service and through this consultation and registry, they were indicated to the research team and invited to take part in the study. All individuals were cross-sectionally assessed concerning PADL (primary outcome), lung function, exercise capacity, anthropometric data, body composition, limitation by dyspnea in daily life and functional status, as described in detail below.
The study comprised a convenience sample of individuals with COPD who sought treatment due to symptoms or were referred to pulmonary rehabilitation. Inclusion criteria were: subjects diagnosed with COPD according to the Global Initiative for Obstructive Lung Disease (GOLD) 1 ; no acute exacerbation in the previous month; absence of severe comorbidities; and non-participation in any regular physical training in the last year. Exclusion criteria were the non-availability of minimum PADL valid assessment (see below).
Assessments
Physical activity in daily life
PADL was objectively evaluated using two PA monitors previously validated in individuals with COPD11,12: the Sensewear® Armband (SAB)(BodyMedia, USA) and the Dynaport® Activity Monitor (DAM) (McRoberts BV, The Hague, the Netherlands). All patients were carefully instructed on how to wear the devices, which were worn simultaneously for 7 days, during awake time. 13 A valid day comprised a minimum wearing time of at least 10 h/day, and a minimum of four valid days (out of the 7) was required.
The DAM is a PA monitor which provides the exact time that the patient spends per day in each position (i.e., average time spent/day walking, standing, sitting, and reclined), as well as estimates the respective energy expenditure. The SAB PA monitor uses algorithms based on the wearer’s sex, age, weight, height, and dominant arm to estimate EE minute-by-minute.13, 14 Meticulous minute-by-minute analysis was performed, and the predominant minute (when the patient stayed for more than 30 s in the same position) was checked and noted in four activities and postures by using the DAM: walking, standing, sitting, and reclined. The predominant minutes were then synchronized with the SAB minutes and the EE was evaluated per minute for each of the same four activities and postures. Both devices were used simultaneously since they are complementary, that is, the DAM is limited in evaluating movements of the upper limbs (a feature of the SAB), whereas the SAB cannot identify body positions (a feature of the DAM).
Finally, patients were classified as “physically active” or “physically inactive” in daily life according to the recommendations of the ACSM, as follows: individuals who perform at least 30 min/day in activities of moderate-to-vigorous intensity for 5 days/week (i.e., >150 min/week) or 20 min/day in vigorous intensity PA for 3 days/week (i.e., >60 min/week) were classified as physically active, whereas those who did not achieve this threshold were classified as physically inactive.6, 7
Lung function
Pulmonary function was assessed with a plethysmograph (Vmax, Carefusion, Hoechberg, Germany) according to ATS/ERS standards.15, 16 Reference values from the Brazilian population were used. 17
Exercise capacity
Exercise capacity was evaluated by the 6 min walking test (6MWT) according to international guidelines. 18 Once again, reference values from the Brazilian population were used. 19
Anthropometric data
Body composition was assessed by bioelectrical impedance (Biodynamics 310 TM [Biodynamics Corp, USA]) according to international standards 20 and the manufacturer’s recommendations. Fat-free mass (FFM) was calculated using a specific formula for individuals with COPD. 21
Dyspnea in daily life
The Portuguese-validated version of the Medical Research Council (MRC) scale was used to evaluate the limitation by dyspnea in daily life. 22 This scale ranges from 1 to 5, and higher values mean worse limitation.
Functional status
The Portuguese-validated version of the London Chest Activity of Daily Living (LCADL) scale was used to assess functional status (i.e. performance in activities of daily living). 23 The scale comprises four domains (self-care, domestic, physical, and leisure), and higher values mean worse functional status.
Statistical analysis
Data analysis of the predominant minute in each activity and body position (by the DAM) was synchronized with the EE of the same minute (by the SAB) using Microsoft® Excel. Statistical analysis was performed using the SPSS 22.0 (IBM, Armonk, NY, USA) and GraphPad Prism 6.0 (GraphPad Software, San Diego, CA, USA). The Shapiro–Wilk test was used to verify normality in data distribution and data were accordingly described as mean ± standard deviation or median [257–5%interquartile range]. Spearman’s coefficient was used to verify the correlation of EE/minute with other outcomes.
The comparison of EE/minute between patients classified as active and inactive was performed using the Mann–Whitney test, whereas the comparison of EE/minute among the four different activities and body positions was performed using the Kruskal–Walis test. Multiple binary logistic regression analysis was performed to investigate if EE/minute and time walking/day are determinants of the classification as physically active (with adjustment for BMI, sex, and FEV1). For all analyses, the level of statistical significance was set as p < 0.05.
Results
Characteristics of the sample.

Data were expressed as mean ± standard deviation and median [25–75% interquartile range], according to normality in data distribution. M: Male; F: Female; BMI: body mass index; FFM: Fat-free mass; FEV1: forced expiratory volume in the first second; FVC: forced vital capacity; 6MWT: Six-minute walk test; m: meter; MRC: Medical Research Council scale; LCADL: London Chest Activities of Daily Living scale; MVPA: moderate-to-vigorous physical activity; min: minutes.
Comparison between groups “physically active” and “physically inactive.”
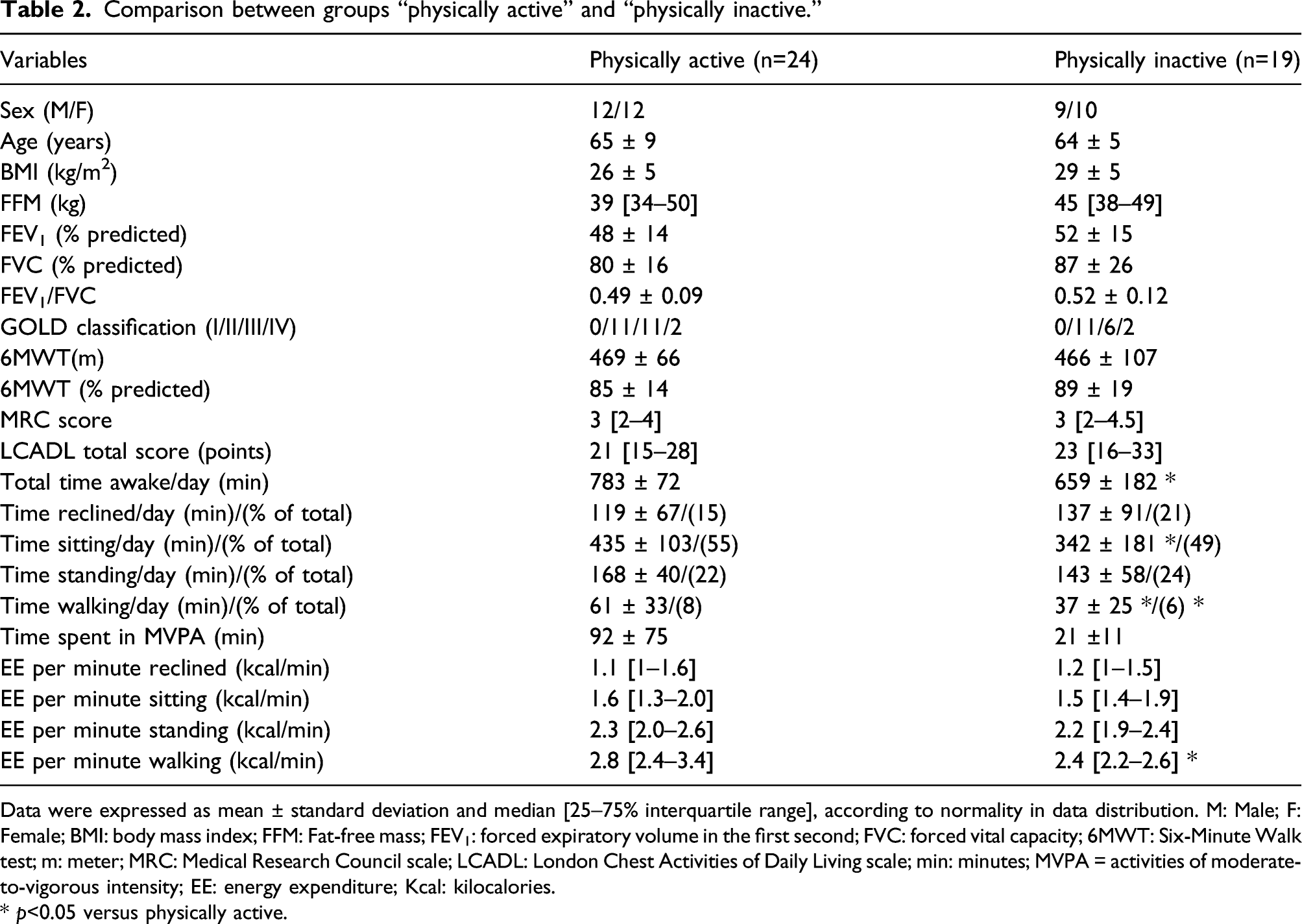
Data were expressed as mean ± standard deviation and median [25–75% interquartile range], according to normality in data distribution. M: Male; F: Female; BMI: body mass index; FFM: Fat-free mass; FEV1: forced expiratory volume in the first second; FVC: forced vital capacity; 6MWT: Six-Minute Walk test; m: meter; MRC: Medical Research Council scale; LCADL: London Chest Activities of Daily Living scale; min: minutes; MVPA = activities of moderate-to-vigorous intensity; EE: energy expenditure; Kcal: kilocalories.
* p<0.05 versus physically active.
The binary logistic regression model analysis yielded that, regardless of the time walking/day, EE/minute walking was a significant predictor of the classification as physically active (OR=18.2 [2–165]; p=0.01), together with BMI (OR=0.68 [0.5 – 0.9]; p=0.008) (model: Chi-square = 22.431, p< 0.05; R2 [Nagelkerke] = 0.556).Time walking/day was not statistically significant (OR=1.0 [0.9–1.0]; p=0.14).
Correlation of EE per minute in different activities and body postures (walking, standing, sitting, and reclined) with different variables and characteristics in individuals with COPD.

Sex: one for male; 0 for female; FFM: Fat-free mass; FEV1: forced expiratory volume in the first second; FVC: forced vital capacity; 6MWT: Six-Minute Walk test; MRC: Medical Research Council score; LCADL: London Chest Activity of Daily Living scale.
* p<0.05.
Figure 1 compares the EE/minute of the four different activities and postures within the active and inactive groups, as well as in the total group (active + inactive). In the active group, significantly higher EE/minute was observed for walking and standing in comparison both to sitting and reclined (p >0.0001 for all), whereas there was no significant difference between walking and standing. Exactly the same results were found for the total group. In the inactive group, however, there were significant differences in EE/minute only when comparing walking versus reclined and standing versus reclined (p >0.0001 for all). Comparison of EE per minute of the four different activities and postures in the active and inactive groups and in the total group (active + inactive). EE: energy expenditure; Kcal: kilocalories; min: minutes. * P<0.05 compared to EE per minute reclined. † P< 0.05 compared to EE per minute sitting. EE/minute (kcal/min)
Discussion
The present study showed that individuals with COPD classified as physically active according to the ACSM criteria have higher time spent walking/day (as expected), but more importantly, also presented higher EE/minute walking, a variable reflecting intensity of PA in daily life. Moreover, EE/minute walking was a significant predictor of being active in daily life, and this happened independently of the time spent walking/day. Therefore, a high EE/minute walking was shown to be a stronger predictor of being classified as physically active than the time walking/day, since the former “outscored” the latter in the prediction model. Of notice, another contribution of the present study was to show that for each additional kilocalorie per minute walking, a patient has 18 times more chance to be classified as physically active in daily life and, by extension, to have reduced risk for cardiovascular disease and premature mortality, 24 among other additional health benefits (e.g., improve musculoskeletal health and help avoiding unhealthy weight gain).6,7 Furthermore, higher EE/minute in all four activities and body postures was mainly associated with lower age and male sex, but also with higher FFM and BMI, better lung function, exercise capacity, and functional status, as well as with less dyspnea in daily life. Finally, physically active individuals presented higher EE/minute in walking and standing in comparison to sitting and reclined, whereas physically inactive individuals presented significant differences in EE/minute only when comparing reclined with walking and standing.
It was certainly expected that time walking/day would be higher in physically active individuals in comparison to those physically inactive. However, this is the first time that physically active patients were shown to present higher EE/minute walking in comparison to those physically inactive. Another novelty of the present study was to show that EE/minute walking was a significant predictor of being active in daily life. Although this result seems to be intuitive (since the ACSM recommends that the 30 min/day of PA should be performed at least at moderate intensity), this was never confirmed by performing such a highly detailed minute-by-minute analysis. We are confident that, beyond any reasonable methodological doubt, it is confirmed that inactive individuals with COPD are characterized not only by lower time walking/day, but also by lower intensity (as reflected by lower EE during walking quantified in a rigorous minute-by-minute basis). Therefore, it should be highlighted that intensity of walking seems to be decisive when defining if an individual with COPD is physically active or inactive.
The strongest associations between EE/minute and clinical variables were found for age and gender. This can be explained by fact that the PA monitors’ algorithm uses these variables to estimate energy expenditure. 13 We can also highlight the strong correlation between EE/minute and fat-free mass, which is in line with similar results found in the study by Webb et al. 25 Weaker correlations were observed in the four activities/postures between EE and pulmonary function, dyspnea in daily life, exercise capacity, and functional status. Unlike the study by Pitta et al., 4 which found a strong correlation between 6MWT and physical activity represented as walking time in daily life, the present study showed a weak correlation between 6MWT and EE/minute in the four activities/postures assessed. This is likely due to the fact that walking time and EE reflect different aspects of PADL, which have their specific related factors.
Physically active patients showed a clear difference in EE/minute walking and standing in comparison to sitting and reclined. On the other hand, physically inactive patients showed no difference in EE/minute between sitting, standing, and walking, indicating that physically inactive individuals spend little energy in walking (probably very slowly) to the point of presenting similar EE/minute in comparison to a sedentary posture such as sitting. In other words, the intensity of walking in physically inactive individuals with COPD is not significantly different than that necessary during sitting. We hypothesize that this may be explained by a combination of low intensity while walking and high basal metabolic rate due to the increased ventilatory demand caused by the disease. This is well illustrated in the study by Vitorasso et al., 26 in which even patients with moderate-to-severe COPD who walked more than 30 min/day, did that at very low EE in the majority of the time. This should encourage us even further to pursue the goal of educating individuals with COPD to replace sedentary behavior by activities demanding higher EE.
Limitations of the present study include the non-availability of information concerning comorbidities of the individuals in the sample, not allowing to infer the role of these comorbidities in the findings. Further, the sample had relatively preserved exercise capacity, predominantly mild symptoms and moderate-to-severe airflow obstruction, somehow limiting the generalizability of the findings. Furthermore, the relatively small size of the subgroups should be considered before extrapolating from these findings. Further research in this field is warranted. The present study, however, brings some clinical implications: for individuals with COPD to be considered physically active, and consequently to achieve health benefits, higher walking intensities (i.e., spending more energy) are important, and not only to increase their walking time. This may motivate the development of strategies to help subjects with moderate-to-severe airflow obstruction and preserved exercise capacity to use their capacity and walk faster (i.e., with higher energy expenditure) in order to prevent/treat illnesses associated with physical inactivity.
In conclusion, despite the required caution regarding the generalizability of the findings, these results show that EE/minute walking is a significant predictor of being physically active in daily life in individuals with COPD, regardless of the time spent walking/day. Each 1 kilocalorie per minute walking improves in 18 times the chances to be physically active according to the ACSM. Finally, physically active individuals spend more EE/minute walking than those physically inactive.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.