
Abstract
Background
First-degree relatives (FDRs) of individuals with type 2 diabetes mellitus (T2DM) are at increased cardiometabolic risk due to genetic predisposition, even in the absence of overt disease. To evaluate subclinical myocardial dysfunction using speckle-tracking echocardiography (STE) and to assess serum levels of endothelial dysfunction related biomarkers, Endothelin-1 (ET-1), E-selectin, and Endocan, in normoglycemic FDRs of patients with T2DM, compared with healthy controls.
Methods
This study included 151 normoglycemic participants, comprising 75 individuals in the study group and 76 in the control group. Global longitudinal and circumferential strain values were assessed using STE. Serum levels of ET-1, E-selectin, and Endocan were measured using ELISA.
Results
ET-1 levels were significantly higher in the study group (p = 0.047). STE revealed lower strain values in the study group in both SAX Basal/Mid/Apical (p = 0.027) and A4C/A2C/A3C mean views (p = 0.013). E-selectin showed a negative correlation with myocardial strain values, although no significant between-group difference was observed.
Conclusions
Normoglycemic FDRs of T2DM patients exhibited subclinical myocardial strain abnormalities and elevated ET-1 levels, suggesting early cardiovascular alterations associated with genetic predisposition. ET-1 and E-selectin may serve as potential biomarkers for preclinical myocardial dysfunction in at-risk individuals.
Keywords
Introduction
Type 2 diabetes mellitus (T2DM) is a well-established and independent risk factor for the development of cardiovascular diseases (CVD). 1 A growing body of epidemiological evidence indicates that individuals with T2DM have a markedly elevated risk of CVD morbidity and mortality compared to the general population. Large cohort studies, especially those conducted in high-income countries, have shown that individuals with T2DM have approximately twice the risk of developing CVD compared to individuals without diabetes. 2 Even in the absence of overt disease, first-degree relatives (FDRs) of people with T2DM often exhibit early metabolic disturbances such as insulin resistance, increased adiposity, and an elevated cardiovascular risk profile. 3
Endothelial dysfunction is not only an early indicator of atherosclerosis but also plays a pivotal role in its progression and the development of vascular complications. T2DM is closely associated with endothelial impairment, and several circulating biomarkers serve both as indicators and mediators of this pathological process.4,5
E-selectin is an adhesion molecule expressed only on activated endothelial cells. It plays a key role in mediating leukocyte adhesion and transendothelial migration. Elevated serum E-selectin levels have been linked to endothelial dysfunction and are considered a marker of increased cardiovascular risk. 6 Endothelin-1 is a potent endogenous vasoconstrictor that contributes to endothelial dysfunction. Elevated ET-1 levels impair endothelial integrity through increased oxidative stress, inflammation, and altered vasomotor tone. 7 Endocan or Endothelial Cell-specific Molecule-1 (ESM-1) is a proteoglycan secreted by endothelial cells, with its expression markedly upregulated in response to inflammatory stimuli. Elevated Endocan levels have been identified as a specific marker of endothelial dysfunction in conditions such as sepsis, atherosclerosis, and other vascular inflammatory diseases.8,9 These three biomarkers remain clinically relevant as early and specific indicators of pathological processes involving endothelial dysfunction. They may also hold potential value in the assessment of cardiometabolic risk.
Left ventricular dysfunction can be assessed not only by conventional methods but also through two-dimensional STE, which offers high sensitivity and accuracy in detecting subclinical ventricular impairment. This technique enables quantitative evaluation of both regional and global left ventricular function using two-dimensional imaging.10,11 Previous studies have demonstrated subclinical left ventricular dysfunction, as assessed by STE, in patients with newly diagnosed T2DM. 12 Previous studies have demonstrated that FDRs of individuals with T2DM exhibit significant changes in subclinical atherosclerosis markers, such as increased carotid intima-media thickness and aortic stiffness, even without overt T2DM or dysglycemia. These findings suggest a potential genetic or familial predisposition to increased cardiometabolic risk..13,14 However, studies investigating whether FDRs of individuals with T2DM exhibit subclinical myocardial dysfunction remain limited, despite growing evidence of early vascular alterations in this population.
This study aimed to investigate the presence of subclinical myocardial dysfunction using STE in FDRs of individuals with T2DM who did not have diabetes themselves, and to compare them with healthy individuals without a family history of T2DM. Additionally, the study sought to explore the potential association between circulating levels of endothelial dysfunction-related biomarkers—including E-selectin, ET-1, and Endocan—and subclinical myocardial impairment in this at-risk population.
Materials and methods
Data collection and analysis
The study was carried out among individuals admitted to the Internal Medicine outpatient clinic at Izmir Katip Celebi University Atatürk Education and Research Hospital. In accordance with the protocol approved by the institutional ethics committee, all participants were verbally informed about the study at the time of enrollment, and written informed consent was subsequently obtained. This study was approved by the Ethics Committee of Izmir Katip Celebi University (Approval No: 0057; Date: May 24, 2021). Medical records and laboratory results of individuals who had previously presented to our hospital for various reasons were reviewed. Those meeting the eligibility criteria were included in the study. Waist circumference and body mass index (BMI) were measured; previously obtained blood test results, including HbA1c and routine biochemical parameters, were also evaluated. At the second visit, blood samples were collected from eligible participants for the measurement of E-selectin, ET-1, and Endocan levels. During the second visit, STE was performed by a single cardiologist to ensure consistency in image acquisition and interpretation.
Image acquisition and analysis of STE parameters
STE analyses were performed using images acquired with the EPIQ/iE33 ultrasound system (Philips Healthcare, Andover, MA, USA). Images were acquired at a frame rate of 50–90 frames per second while participants were instructed to hold their breath. Apical four-chamber, three-chamber, and two-chamber views, as well as short-axis images at the basal, mid, and apical levels, were evaluated. For each participant, the analysis of images obtained from an average of three cardiac cycles was considered sufficient. Circumferential strain measurements of the left ventricle were obtained from short-axis views acquired at end-diastole by manually tracing the endocardial borders. Longitudinal strain measurements were derived from apical four-chamber, three-chamber, and two-chamber views, with the endocardial borders initially marked at the lateral, basal, and apical segments at end-diastole. The software automatically delineated the myocardial contours based on these reference points, and manual adjustments were performed when necessary. Global longitudinal strain (GLS) and global circumferential strain (GCS) values were calculated by averaging the strain measurements obtained from all myocardial segments.
Assessment of endothelial biomarkers and laboratory parameters
Blood samples collected from participants were centrifuged at 3000 rpm for 10 min, and the separated serum samples were stored at −20°C in Eppendorf tubes until analysis. Hemolyzed and lipemic samples were excluded from the study. After thawing at room temperature, serum levels of ET-1, Endocan, and E-selectin were measured using commercially available ELISA kits (Elabscience, USA) on a semi-automated microplate reader (BioTek ELx800, USA). Routine biochemical parameters were analyzed using the Architect c16000 analyzer (Abbott Laboratories, IL, USA).
Inclusion and exclusion criteria
A total of 151 normoglycemic participants were included in the study. The study group consisted of 75 individuals who had at least one FDRs diagnosed with T2DM, while the control group comprised 76 individuals without a family history of T2DM. Normoglycemia was defined according to the following criteria: HbA1c < 5.7%, fasting plasma glucose <100 mg/dL, and a 2-h plasma glucose level <140 mg/dL following a 75 g oral glucose tolerance test (OGTT). Exclusion criteria included a history of coronary or valvular heart disease, heart failure, vascular diseases (i.e., high blood pressure), hepatic or renal insufficiency, alcohol or drug abuse, pregnancy, lactation, use of medications affecting glucose metabolism, a diagnosis of diabetes mellitus, impaired glucose tolerance, and lipid metabolism disorders. Arterial blood pressure was measured in all participants during clinical evaluation. Individuals with a resting blood pressure exceeding 140/90 mmHg were excluded from the study to eliminate the potential confounding effect of hypertension. To avoid potential confounding, all individuals using any form of medication at the time of recruitment were excluded from the study. Individuals who did not consent to the required tests, missed scheduled visits, or withdrew from the study were also excluded.
Statistical analysis
Data were analyzed using IBM SPSS Statistics version 23.0 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as mean ± standard deviation, median (minimum–maximum), while categorical variables were expressed as frequencies and percentages. The distribution of continuous data was assessed using the Kolmogorov–Smirnov test. For comparisons between two independent groups, the Mann–Whitney U test was applied, and the Kruskal–Wallis test was used for comparisons involving more than two groups. Categorical variables were analyzed using the Pearson chi-square test or Fisher’s exact test, as appropriate. Correlations between continuous variables were assessed using Spearman’s rank correlation coefficient. A p-value of <0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of the study and control groups.
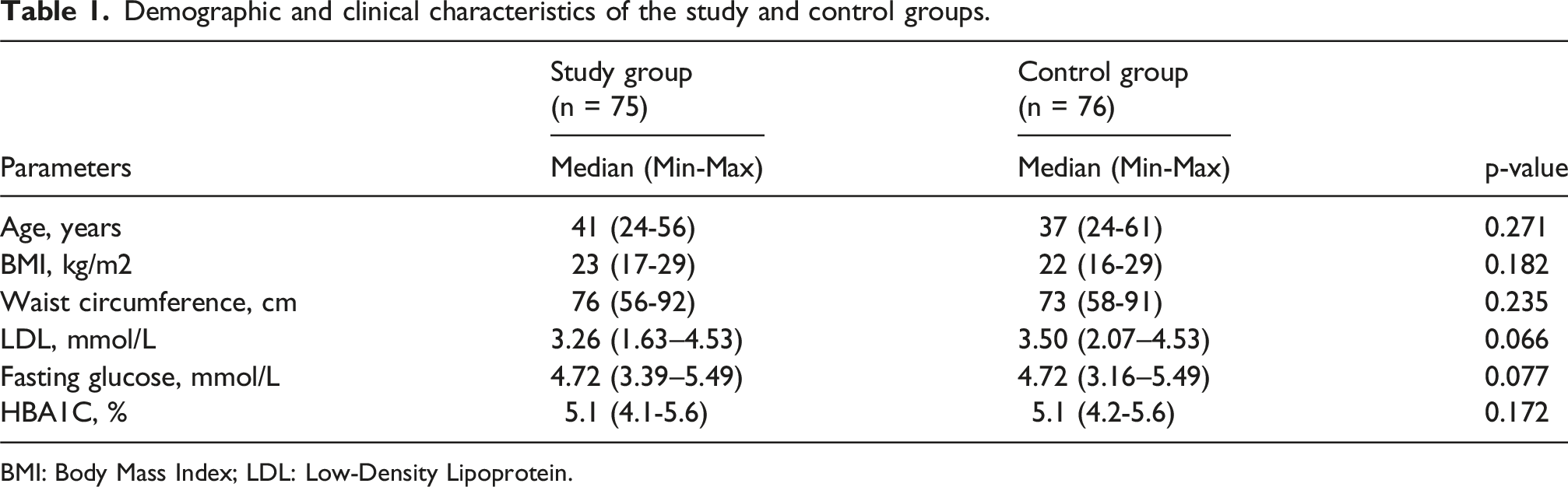
BMI: Body Mass Index; LDL: Low-Density Lipoprotein.
Comparison of biomarker levels and speckle-tracking echocardiography parameters between groups.

Note. Italicized values indicate statistically significant differences between groups.
Correlation between endothelial biomarkers and cardiac strain parameters.

Note. Italicized values indicate statistically significant differences between groups.
Discussion
This study aimed to investigate subclinical myocardial dysfunction and endothelial biomarker profiles in normoglycemic FDRs of individuals with T2DM, a population considered at elevated cardiometabolic risk due to genetic susceptibility. By comparing this at-risk group with age- and metabolically matched controls without a family history of T2DM, we were able to isolate early cardiovascular alterations potentially attributable to familial predisposition. The absence of significant differences in conventional metabolic parameters such as BMI, waist circumference, LDL, fasting glucose, and HbA1c enhances the internal validity of our findings. Notably, the detection of strain abnormalities and elevated ET-1 levels in the study group suggests that subclinical cardiac and vascular changes may precede overt metabolic dysfunction, underscoring the utility of STE and endothelial biomarkers in early risk stratification. To our knowledge, this is among the few studies to demonstrate such changes in asymptomatic individuals with a genetic background of T2DM, thereby contributing novel evidence to the literature.
In our study, participants in the study group showed a statistically significant reduction in left ventricular strain measurements, specifically in the SAX Basal/Mid/Apical and A4C/A2C/A3C mean values. Similarly, Ernande et al. demonstrated that subclinical myocardial injury in patients with T2DM can be detected using STE. 15 Taghreed et al. also reported significant differences in STE parameters between patients with T2DM and healthy controls. 16 These findings agree with the existing literature, supporting the presence of early myocardial changes in individuals at risk for T2DM.
Elevated ET-1 levels are widely recognized as a key biomarker of endothelial dysfunction. 7 ET-1 levels were found to be significantly higher in the study group compared to the control group. Consistent with our findings, Donatelli et al. reported increased ET-1 levels in patients with T2DM even in the absence of coronary artery disease. 17 The observed elevation in ET-1 levels in the study group may be interpreted as an early indicator of endothelial dysfunction, suggesting that the cardiovascular effects of T2DM may begin during the preclinical stage. Although STE findings in this group revealed signs of early myocardial impairment, correlation analysis did not demonstrate a statistically significant association between ET-1 levels and either the SAX Basal/Mid/Apical mean or the A4C/A2C/A3C mean values. Despite the absence of a direct correlation between ET-1 and STE parameters in our study, the elevated ET-1 levels may still reflect early intravascular alterations occurring at both systemic and local cardiac levels.
No statistically significant difference in E-selectin levels was observed between the study and control groups. Differing from our study design, Bannan et al. included individuals with type 2 diabetes mellitus (T2DM) as a third group in addition to FDRs of T2DM patients and healthy controls. Their analysis revealed a statistically significant difference in E-selectin levels between the T2DM group and the other two groups. However, no significant difference was observed between the FDRs of T2DM patients and the control group. 18 Roldan et al. have previously suggested that E-selectin may serve as a prognostic marker of vascular inflammation and atherosclerosis. 6 In our correlation analysis, E-selectin levels were negatively correlated with both the SAX Basal/Mid/Apical mean and the A4C/A2C/A3C mean strain values. In light of these findings, it may be hypothesized that elevated E-selectin levels are indirectly associated with subclinical cardiac dysfunction as detected by STE. However, studies investigating the relationship between E-selectin and STE parameters remain limited in the current literature.
Endocan is a proteoglycan secreted by endothelial cells in response to inflammatory stimuli. 19 In our study, no statistically significant difference in Endocan levels was observed between the study and control groups. A meta-analysis published by Khalaji et al. in 2023 reported that elevated Endocan levels are more pronounced in advanced stages of T2DM and in cases accompanied by vascular complications. The same meta-analysis revealed inconsistent findings in individuals with prediabetes. 20 These findings suggest that Endocan may be a more relevant marker in clinical scenarios involving overt inflammatory activity or advanced cardiac dysfunction. Its sensitivity in detecting subclinical myocardial dysfunction, however, may be limited.
This study has several limitations. The relatively small sample size and the single-time measurement of biomarkers may limit the generalizability of our findings. The use of a single cardiologist for STE assessments minimized interobserver variability, but it also precluded the assessment of interobserver reproducibility. Future studies with larger, more diverse populations and repeated biomarker measurements are warranted to validate these findings. In addition, multicenter trials and the inclusion of longitudinal follow-up may help clarify the prognostic significance of subclinical myocardial and endothelial changes in individuals at genetic risk for T2DM.
Conclusion
Our findings suggest that normoglycemic FDRs of individuals with T2DM may exhibit elevated ET-1 levels and signs of subclinical myocardial dysfunction as assessed by STE. Additionally, a negative correlation was observed between E-selectin levels and myocardial strain parameters, further supporting the role of endothelial dysfunction in early cardiac involvement. These results indicate that ET-1 and E-selectin may serve as potential biomarkers to aid clinicians in the early detection of subclinical myocardial injury in individuals with a genetic predisposition to T2DM.
Consent to publication
This study did not involve the publication of any individual patient data, images, or identifiable personal information. Therefore, specific consent for publication was not required according to the institutional ethics protocol approved by the Ethics Committee of Izmir Katip Celebi University.
Footnotes
Author note
Current affiliation: Dr. İsmet Çulcuoğlu is currently affiliated with Department of Oncology, Kütahya City Hospital, Kütahya, Türkiye. The research was conducted while the author was affiliated with Department of Internal Medicine, Atatürk Training and Research Hospital, Faculty of Medicine, İzmir Katip Çelebi University, İzmir, Türkiye.
Acknowledgments
The authors would like to express their sincere gratitude to the healthcare professionals and staff who contributed to the coordination, data collection, and technical support of this study.
Ethical considerations
This study was approved by the Ethics Committee of Izmir Katip Celebi University (Approval No: 0057; Date: May 24, 2021).
Consent to participate
In accordance with the protocol approved by the institutional ethics committee, all participants were verbally informed about the study at the time of enrollment, and written informed consent was subsequently obtained. All participants provided written informed consent for participation in the study.
Author contributions
Conceptualization, İ.Ç. and B.Ö.P.; methodology, İ.Ç.,M.Ü.and Ş.E.; software, İ.Ç and G.E.; validation, İ.Ç., Y.Ü., and V.E.; formal analysis, Y.Ü.; investigation, İ.Ç.; resources, İ.Ç.; data curation, İ.Ç. and H.E.Y.; writing-original draft preparation, İ.Ç.,M.Ü. and Y.Ü.; writing-review and editing, İ.Ç., G.E. and M.Ü.; visualization, İ.Ç.; supervision,Y.Ü.; project administration, B.Ö.P.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
According to the approval granted by the Ethics Committee of Izmir Katip Celebi University, data sharing is not permitted in order to protect participant confidentiality and comply with institutional data governance policies.