
Abstract
Background:
The prevalence of diabetes mellitus and its associated complications such as peripheral artery disease is increasing worldwide. We aimed to explore the distinct impact of type 1 diabetes mellitus and type 2 diabetes mellitus on treatment and on short- and long-term outcome in patients with peripheral artery disease.
Methods:
Retrospective analysis of anonymized data of hospitalized patients covered by a large German health insurance. Assessment of patient’s characteristics (comorbidities, complications, etc.) and outcome using multivariable Cox regression and Kaplan–Meier curves.
Results:
Among 41,702 patients with peripheral artery disease, 339 (0.8%) had type 1 diabetes mellitus and 13,151 (31.5%) had type 2 diabetes mellitus. Patients with diabetes mellitus had more comorbidities and complications than patients without diabetes mellitus (p < 0.001). Type 1 diabetes mellitus patients exhibited the highest risk for limb amputation at 4-year follow-up (44.6% vs 35.1%, p < 0.001), while type 2 diabetes mellitus patients had higher mortality than type 1 diabetes mellitus (43.6% vs 31.0%, p < 0.001).
Conclusion:
Although the fraction of type 1 diabetes mellitus among patients with peripheral artery disease and diabetes mellitus is low, it represents a subset of patients being at particular high risk for limb amputation. Research focused on elaborating the determinants of limb amputation and mortality in peripheral artery disease patients with diabetes mellitus is warranted to improve the poor prognosis of these patients.
Keywords
Introduction
Peripheral artery disease (PAD) is one of the most frequent vascular diseases. It is estimated that over 200 million people worldwide suffer from PAD. 1 Diabetes mellitus (DM) is one of the main risk factors of developing PAD 2 and an independent predictor of increased limb amputation and mortality in patients with PAD.3–5
Beyond its pro-atherosclerotic effect in different vascular beds, DM is a promoter of diverse organ failure, such as in chronic kidney disease (CKD), chronic heart failure (CHF), diabetic retinopathy and so on, which additionally adversely impact the already poor prognosis of patients with DM. Moreover, PAD patients with DM have frequently infrainguinal and crural Trans-Atlantic Inter-Society Consensus (TASC) II C/D lesions 6 which are often complex and highly calcified with unsatisfactory acute and poor long-term results. 7
Type 1 and type 2 diabetes mellitus (DM I and II) have different pathologies and epidemiological characteristics. DM I is caused by an immune-associated destruction of pancreatic beta cells leading to a lifelong dependency on insulin injections, usually manifested at childhood or adolescence.8,9 In contrast, DM II is defined by insulin resistance of the peripheral cells and by a relative insulin deficiency. Moreover, DM II is associated with genetic factors 9 and usually is manifested in older adults. 10
While sufficient data are available from population studies and randomized trials regarding the incremental risk of cardiovascular diseases associated with DM II, data in patients with DM I, particularly with respect to PAD and the impact of the co-prevalence of PAD and DM I on the long-term limb and overall outcome, are scarce. We aimed to explore the frequency, the current vascular treatment and the subsequent outcomes in terms of limb salvage and survival in a large-scale, non-selective cohort of hospitalized PAD patients with concomitant DM in relation to DM type.
Material and methods
In 2004, a diagnosis and procedure-related flat-rate remuneration system, the German diagnosis-related groups (G-DRG-system) was introduced leading to a uniform definition of all somatic in-patient care. The G-DRG system requires one main diagnosis for the in-hospital admission. Additional secondary diagnoses can be coded reflecting the complexity of the disease which can have additive impact on the reimbursement. The diagnoses are coded according to the German Modification of the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10).
Our data source consisted of anonymized patient’s data from the largest health insurance in Germany, the BARMER GEK. Approximately, 8.5 million people are insured by the BARMER GEK, which is around 10% of the entire German population.
Patients hospitalized between 1 January 2009 and 31 December 2011 with a primary or secondary diagnoses of PAD (ICD codes I70.20-I70.24) were included in the analysis. For PAD, patients were classified in relation to the clinical stage as indicated by the Rutherford category (RF) into four different sub-groups allocated by the ICD codes: I70.20-21 was categorized as RF 1–3, I70.22 as RF 4, I70.23 as RF 5 and I70.24 as RF 6. The diagnosis of DM (ICD codes: E10.50, E10.51, E10.74, E10.75, E11.50, E11.51, E11.72–E11.75), of other comorbidities such as coronary artery disease (CAD, ICD-10 I25*), CKD (ICD-10 N18*), CHF (ICD-10 I50*), malignancies (ICD-10 C*), hypertension (ICD-10 I10*-I15*), obesity (ICD-10 E66) and dyslipidaemia (ICD-10 E78) were also obtained from the ICD codes. Likewise, all vascular procedures (Operationen- und Prozedurenschlüssel, OPS codes: endovascular: OPS 8-836, 8-83ba, 8-83bb, 8-84*; surgical: OPS 5-380, 5-381, 5-382, 5-383, 5-388, 5-38a, c–f, 5-392, 5-393, 5-394, 5-395) and in-hospital complications such as acute renal failure (ICD-10 N17*), acute myocardial infarction (MI, ICD-10 I21*), ischaemic stroke (ICD-10 I63*), infection (ICD-10 B95-99*) and sepsis (ICD-10 A30-49*) as well as the in-hospital amputations (OPS 5-864*, 5-865*, 5-866*) were assessed by the ICD codes from the database.
Comorbidities, cardiovascular risk factors and diagnostic/interventional procedures were assessed 24 months before the index hospitalization and followed until 31 December 2012 (up to 4 years from the index hospitalization). The resource utilization data (in-hospital length of stay and the per-case reimbursement costs) were restricted only to in-hospital treatments. The detailed methodology and patients’ selection criteria have previously been described.3,7,11
Statistics
The entire patients’ cohort was divided into three different groups: patients without DM, patients with DM I and patients with DM II.
Categorical variables are presented as absolute numbers (n) and as the percentage (%) of all patients in the respective group. Continuous variables are presented as the median and the interquartile range. Categorical variables were compared using the χ²-test. Continuous variables were compared using the Kruskal–Wallis test. Multivariable Cox regression models were made for the major adverse events death and amputation using the likelihood ratio test (LR) backward method which eliminates covariates which do not have influence in the analysed model. The following covariates were used in our model: DM I, DM II, age, sex, hypertension, obesity, dyslipidaemia, smoking, CKD, CAD, CHF and the Rutherford stages 1–6 (1–3, 4, 5, and 6). Tables 3 and 4 show the results after the elimination process of the LR backward method. Kaplan–Meier models were used to assess the cumulative survival and amputation-free time during follow-up for each group. Comparison was made by the log rank test. A p-value < 0.05 was considered significant. All statistics were made by SPSS version 23 (IBM, Chicago, IL, USA). Figures were made by version 25.
Results
Baseline characteristics and comorbidities
Among the entire study cohort of 41,702 patients with PAD, 339 (0.8%) patients had DM I, 13,151 (31.5%) patients had DM II and 28,212 (67.7%) patients did not have concomitant DM. Baseline characteristics of the entire cohort are presented in Table 1.
Baseline characteristics and comorbidities with regard to diabetes type I and type II.
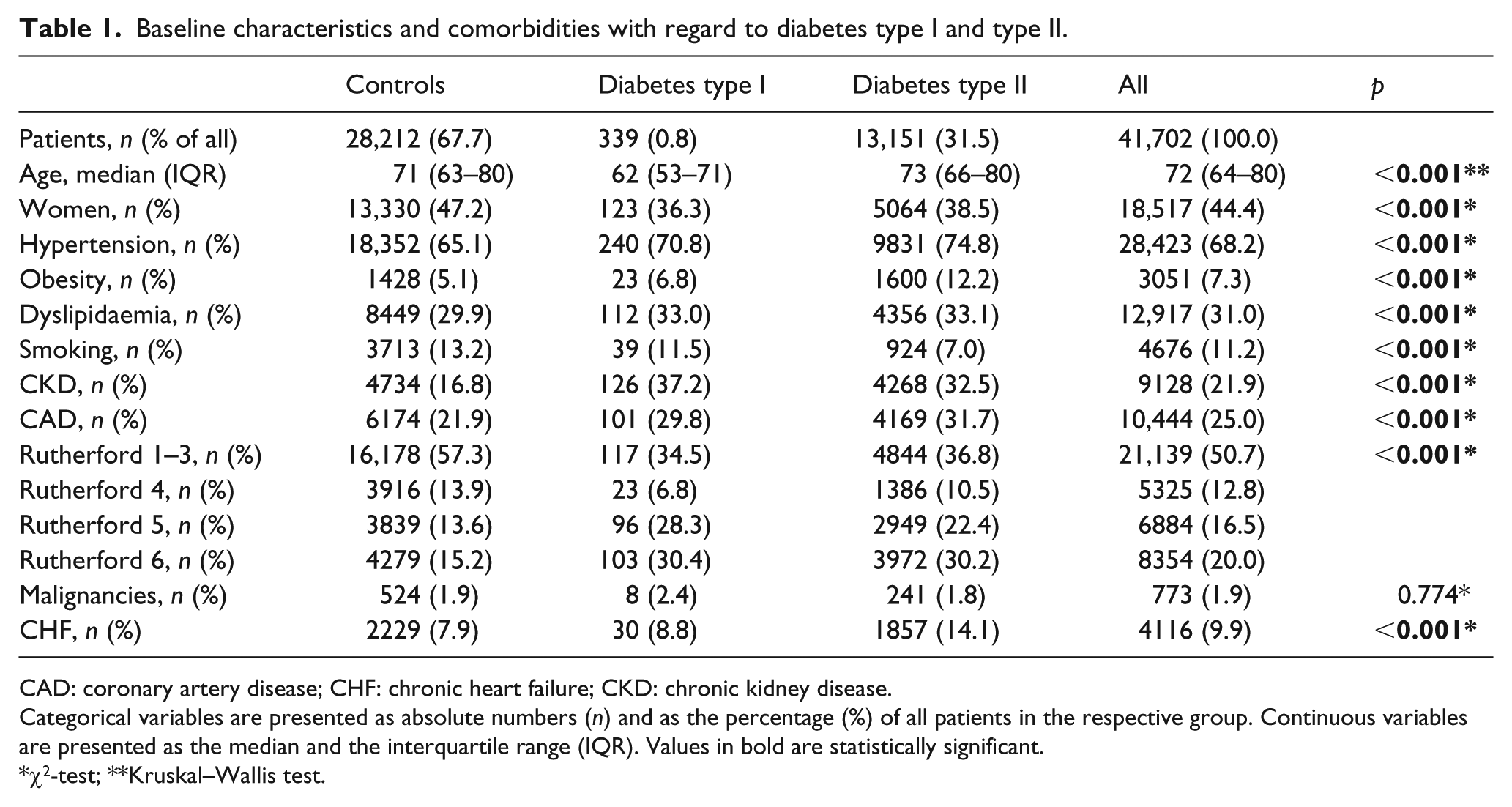
CAD: coronary artery disease; CHF: chronic heart failure; CKD: chronic kidney disease.
Categorical variables are presented as absolute numbers (n) and as the percentage (%) of all patients in the respective group. Continuous variables are presented as the median and the interquartile range (IQR). Values in bold are statistically significant.
χ2-test; **Kruskal–Wallis test.
With an average age of 62.6 years, PAD patients with DM I were the youngest cohort compared with patients with DM II (72.5 years) and without DM (71.3 years). Compared to PAD patients without DM, patients with DM (both type I and type II) were more male, fewer smokers and had a higher frequency of comorbidities such as hypertension, obesity, dyslipidaemia, CKD, CAD and CHF. Patients with PAD and DM also had higher rates of critical limb ischaemia (CLI), that is, at Rutherford categories 5 and 6 (p < 0.001) compared to PAD patients without DM. With respect to diabetes type, comorbidities such as hypertension, obesity, CAD and CHF were more frequent in DM II, while smoking, CKD and CLI at RF 5 were more frequent in DM I (p < 0.001).
In-hospital vascular treatment, outcome and complications
The rates of invasive angiography, of endovascular and surgical revascularization procedures, in-hospital complications and the associated costs are presented in Table 2.
Treatment, complications and outcomes during index hospitalization.
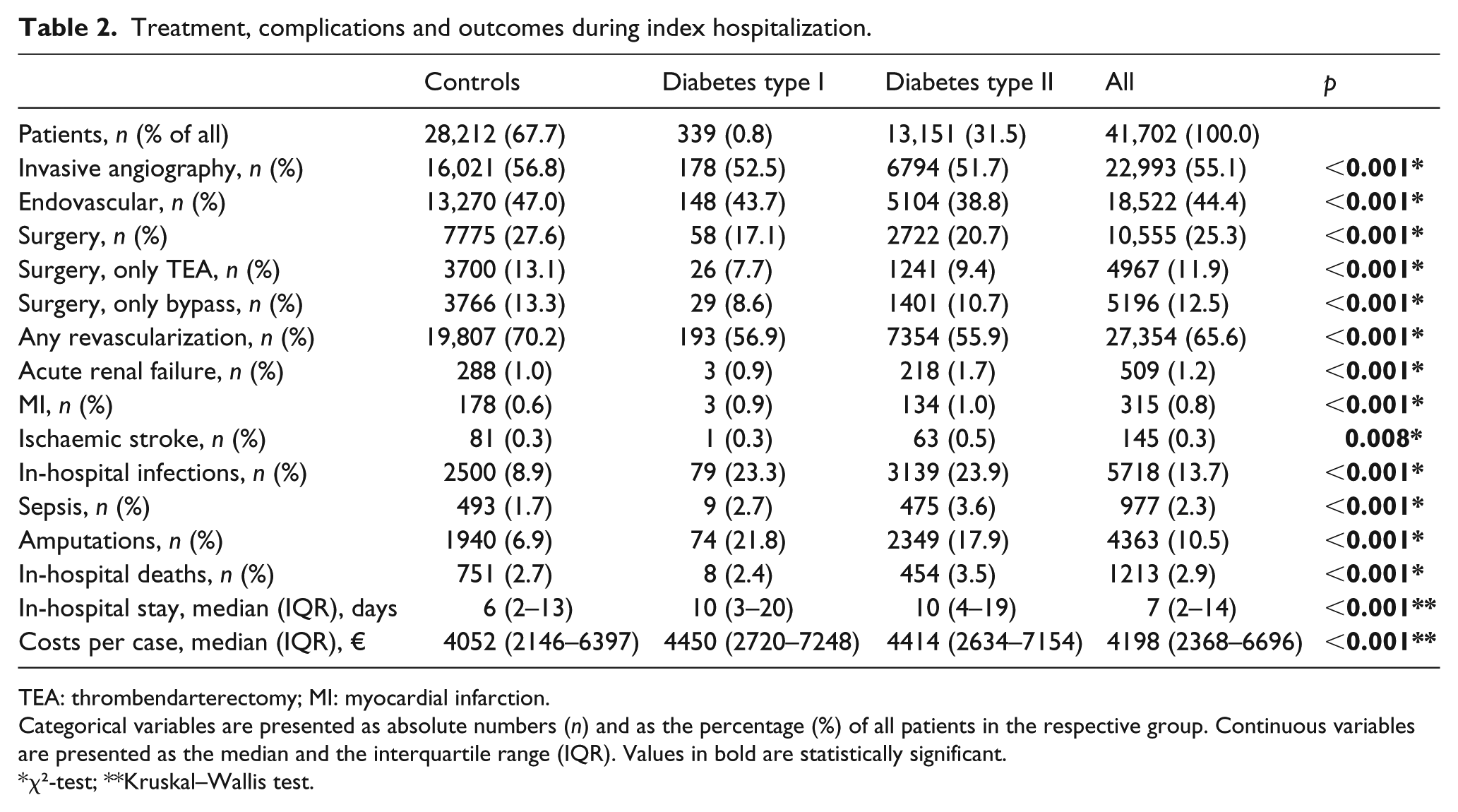
TEA: thrombendarterectomy; MI: myocardial infarction.
Categorical variables are presented as absolute numbers (n) and as the percentage (%) of all patients in the respective group. Continuous variables are presented as the median and the interquartile range (IQR). Values in bold are statistically significant.
χ²-test; **Kruskal–Wallis test.
Patients with DM I and DM II underwent fewer revascularization procedures than patients without DM (p < 0.001). Any revascularization procedures (endovascular and/or surgical) were performed more frequently in PAD patients without DM than in patients with DM. However, the rates of revascularizations were similar between both DM types. Endovascular procedures were performed more frequently in patients with DM I (43.7%) than in those with DM II (38.8%). However, the proportion of surgical procedures was higher in patients with DM II (20.7%) than in patients with DM I (17.1%).
Generally, the rate of in-hospital complications was higher in patients with DM than in patients without DM. Although major adverse events such as MI and stroke were rare, they occurred more often in PAD patients with than without DM. Patients with DM I (23.3%) and patients with DM II (23.9%) had a 2.5-fold higher frequency of in-hospital infections than patients without DM (8.9%). In addition, sepsis occurred more often in patients with DM I (2.7%) and with DM II (3.6%) than in patients without DM (1.7%).
The rate of lower limb amputation during the index hospitalization was 6.9%, 21.8% and 17.9% in patients without DM, with DM I and DM II, respectively (p < 0.001). The percentage of in-hospital deaths was highest in patients with DM II (3.5%), followed by those without DM (2.7%) and with DM I (2.4%). Patients with DM had a longer in-hospital stay (median of 10 days) than patients without DM (median of 6 days) with no difference between type I and type II DM. The mean per-case reimbursement costs were highest for DM I, followed by DM II and lowest in patients without DM (p < 0.001, Table 2)
Long-term outcome
The cumulative survivals and amputation-free times are shown in Figures 1 and 2.
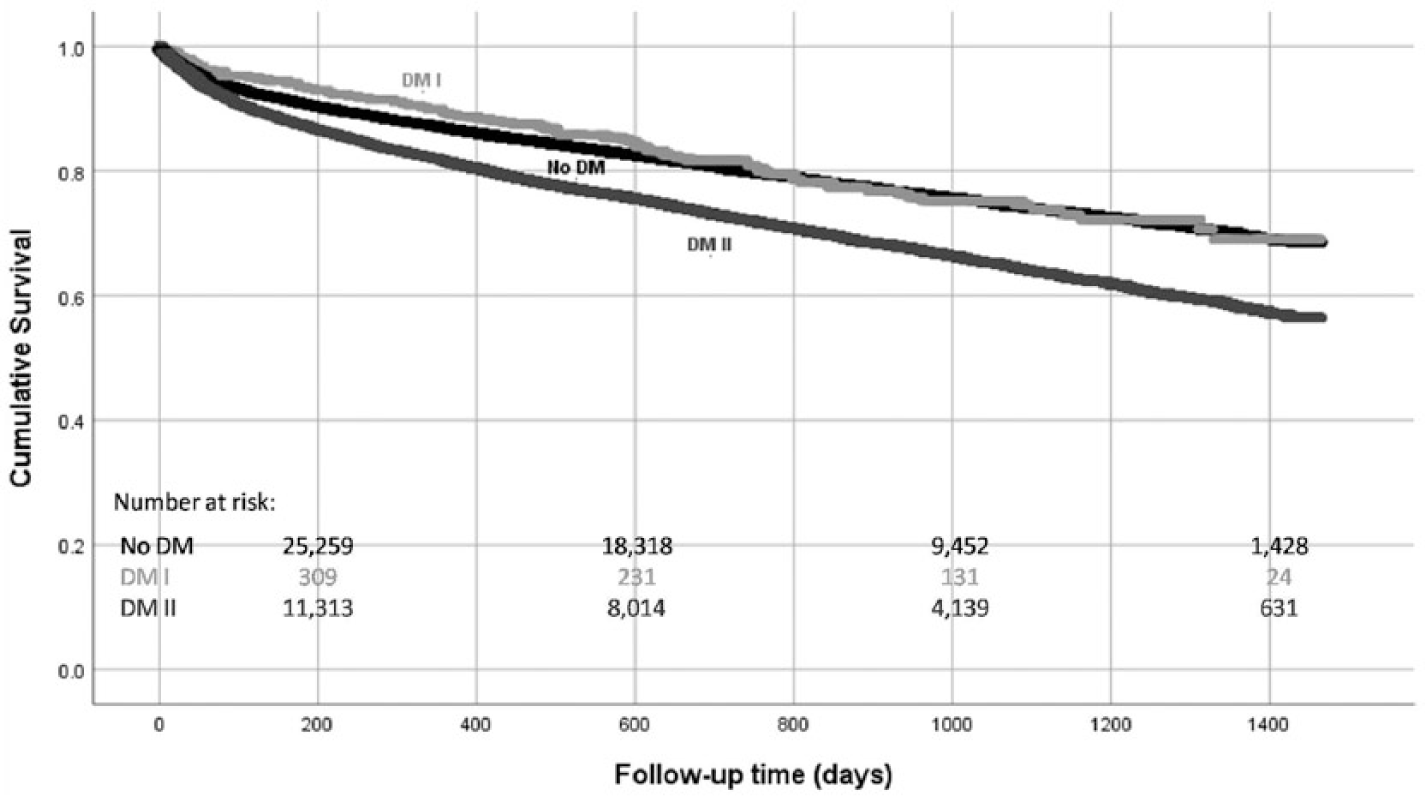
Cumulative overall survival at 4-year follow-up among patients with PAD, PAD + DM type I and PAD + DM type II.
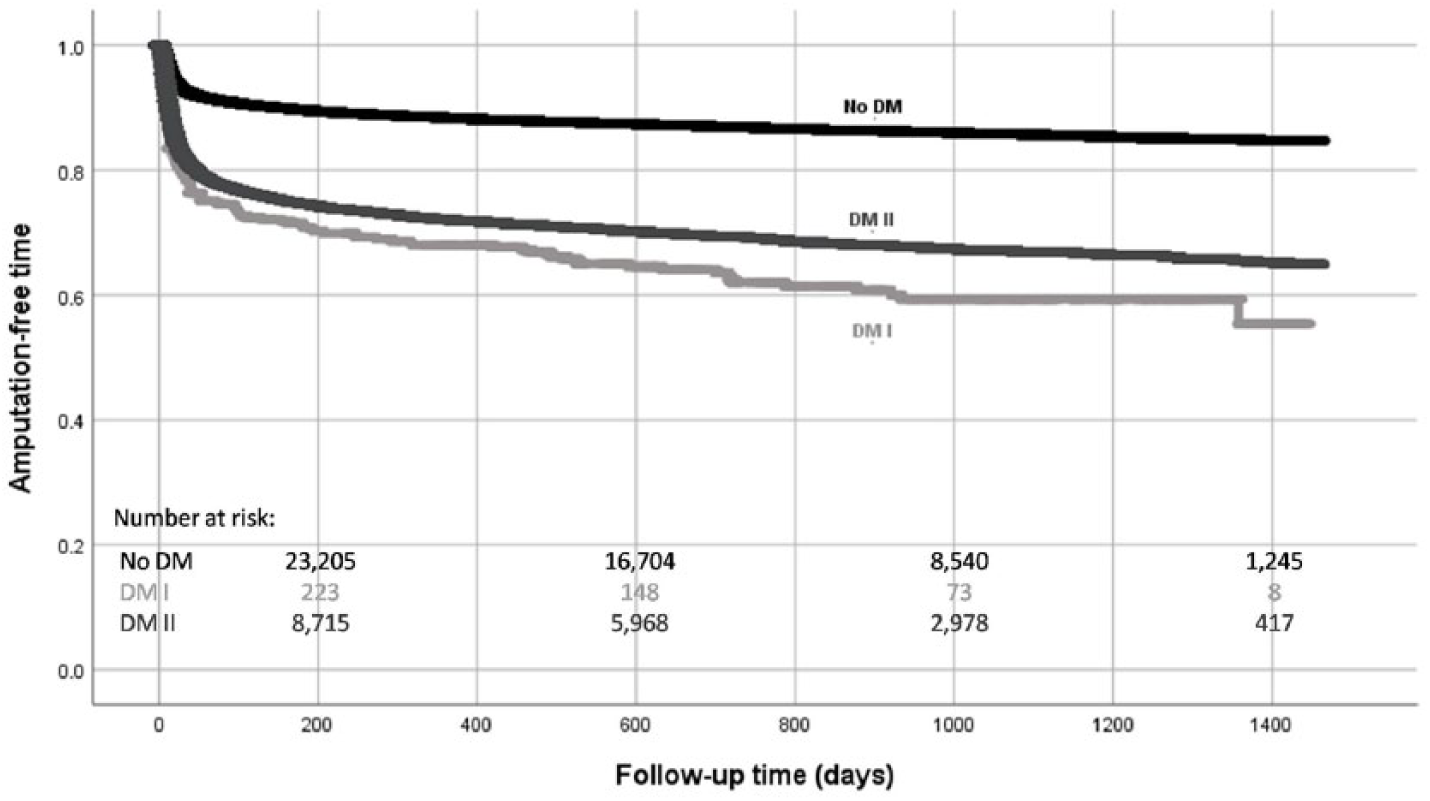
Amputation-free time at 4-year follow-up among patients with PAD, PAD + DM type I and PAD + DM type II.
As illustrated in Figure 1, the 1-, 2-, 3- and 4-year cumulative survival was 86.8%, 80.1%, 74.1% and 68.6% for PAD patients without DM; 89.3%, 81.6%, 73.8% and 69.0% for PAD patients with DM I; and 81.4%, 72.3%, 64.1% and 56.4% for PAD patients with DM II, respectively (p < 0.001).
In PAD patients without DM, the 1-, 2-, 3- and 4-year amputation-free time (Figure 2) was 88.4%, 86.9%, 85.7% and 84.7%, respectively. The corresponding figures in PAD patients with DM type I were 68.0%, 62.0%, 59.3% and 55.4% and in PAD patients with DM II 72.0%, 69.3%, 66.9% and 64.9%, respectively (p < 0.001).
Predictors of long-term outcome
The hazard ratios of potential risk factors for death and amputation are shown in Tables 3 and 4, respectively.
Multivariate Cox regression analysis of predictors of long-term death during the 4-year follow-up period.
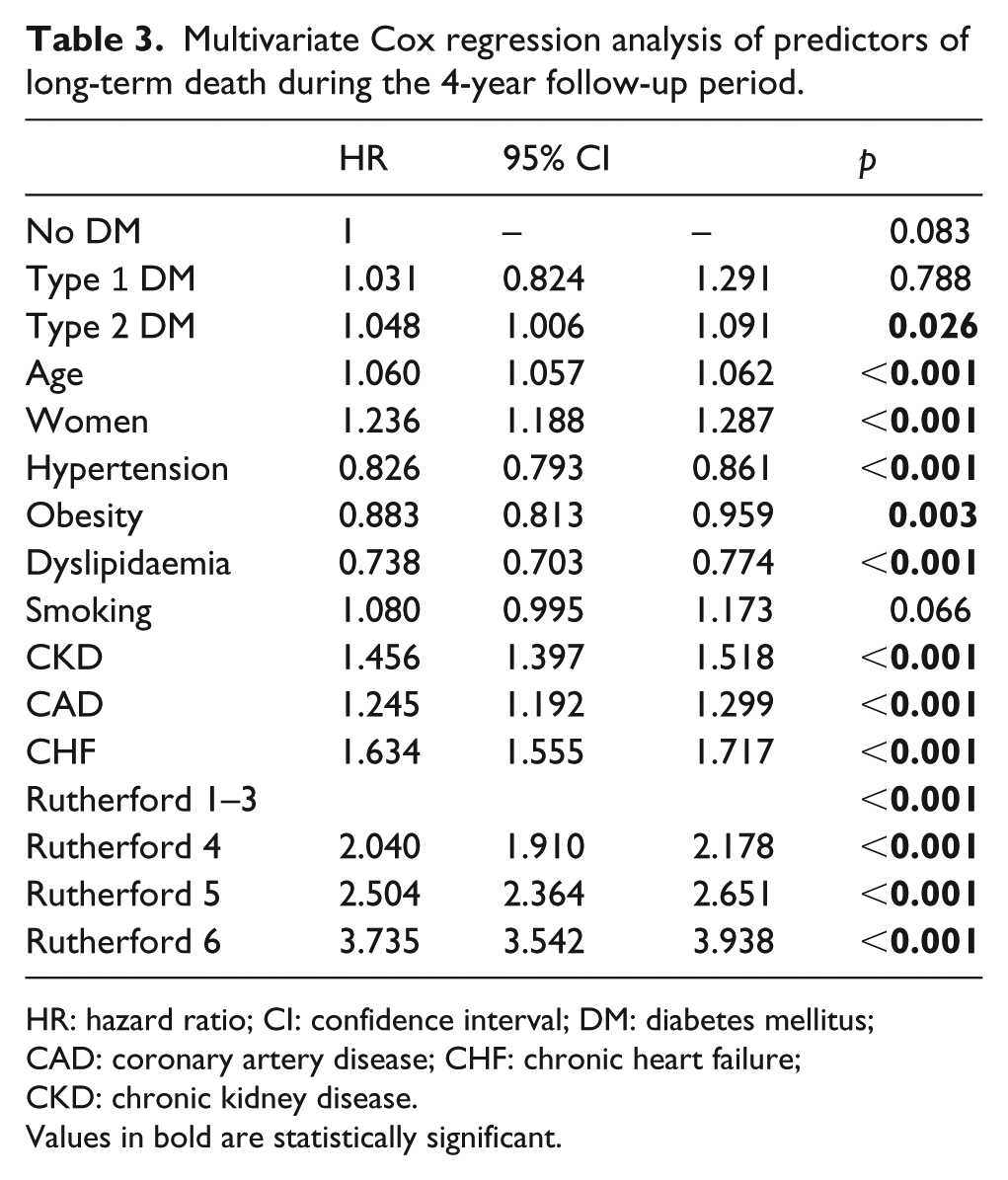
HR: hazard ratio; CI: confidence interval; DM: diabetes mellitus; CAD: coronary artery disease; CHF: chronic heart failure; CKD: chronic kidney disease.
Values in bold are statistically significant.
Multivariate Cox regression analysis of predictors of long-term limb amputation during the 4-year follow-up period.
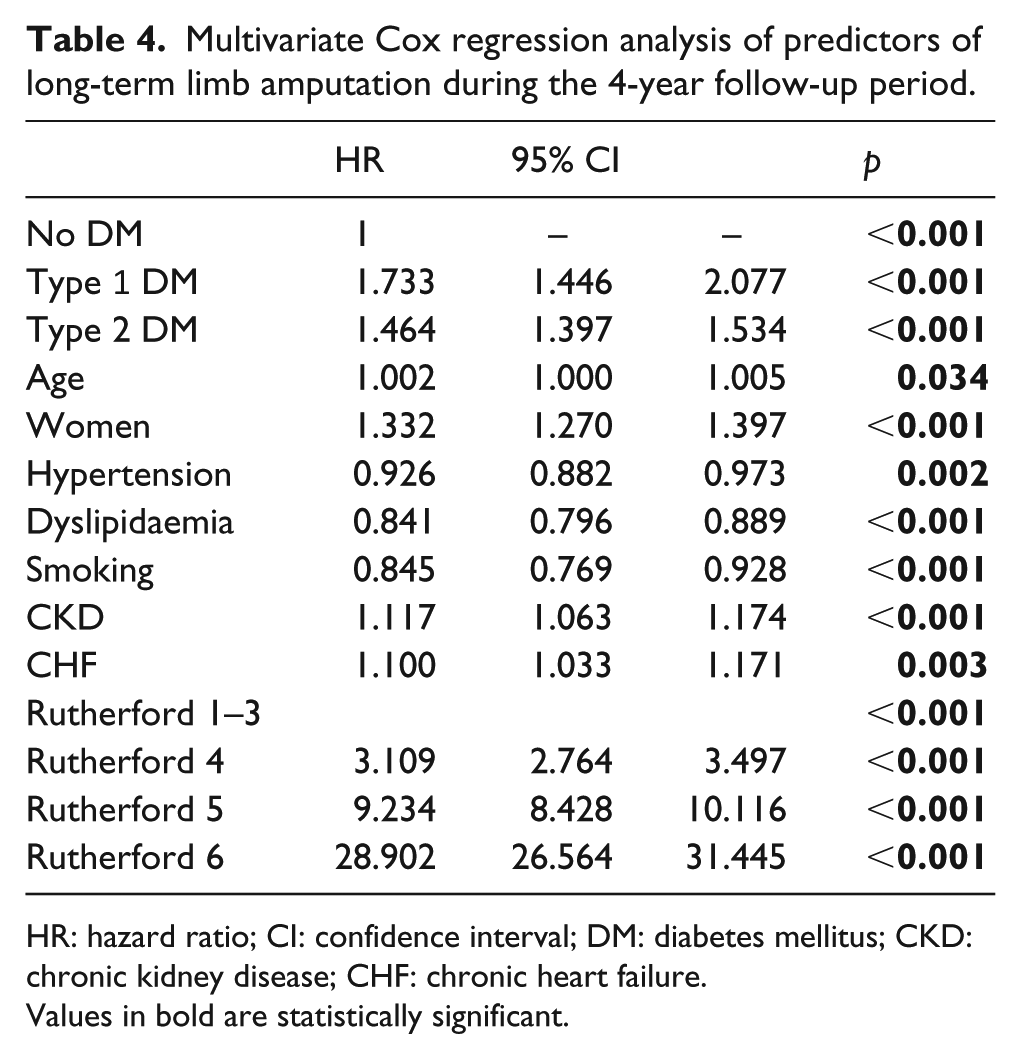
HR: hazard ratio; CI: confidence interval; DM: diabetes mellitus; CKD: chronic kidney disease; CHF: chronic heart failure.
Values in bold are statistically significant.
Male gender, CKD, CAD, CHF and Rutherford stages 4–6 increased significantly the risk of death. DM II had only marginal influence on the risk of death (hazard ratio (HR): 1.048, p = 0.026). In contrast to type II DM, DM I was not an independent risk factor for death.
As illustrated in Table 4, all evaluated risk factors for death except for CAD and obesity were also independent risk factors for amputation. DM I increased the risk of amputation by a HR of 1.733 (p < 0.001) and is therefore a stronger predictor for amputation than DM II which increased the risk of amputation by a HR of 1.464 (p < 0.001). Rutherford categories, however, were the strongest predictors of long-term amputation as well as of long-term mortality.
Discussion
As demonstrated in this large-scale, population-based analysis, DM is common in patients with PAD. Every third PAD patient suffers from concomitant DM. Since the assessment of DM was based on a coding system, it can be assumed that the real number of concomitant DM among PAD patients is higher than in our analysis due to unreported or unknown cases of DM. Nonetheless, our findings are in line with several studies depicting DM as an important risk factor for PAD.2,12,13
Expectedly, PAD patients with DM had more comorbidities than those without DM. With respect to diabetes type, comorbidities such as hypertension, obesity, CAD and CHF were more frequent in DM II, while smoking, CKD and CLI at RF 5 were more frequent in DM I. The higher frequency of hypertension and obesity in PAD patients with DM II could be explained by the fact that patients with DM II often suffer from the metabolic syndrome and stands in line with a recent study which pointed out these two conditions as two of the most frequent comorbidities in DM II patients. 14
The short- and long-term risk of ischaemic limb amputation was higher in patients with DM compared to patients without DM with the highest amputation rates among DM I. We previously have demonstrated that DM has an incremental impact on short- and long-term limb salvage in patients with PAD. 3 The highest amputation risk was observed in patients with diabetic foot syndrome with an amputation-free survival of 45.4% at 4 years. The risk of non-traumatic lower-extremity amputations in patients with DM I was explored in a Swedish population-based study including 31,354 patients. 15 During a mean follow-up of 12.5 years, the authors found a risk of lower-extremity amputation of 11% for women and 20.7% for men with DM I. The higher risk of amputation in our cohort may be due to the higher median age of the studied population, which was 62 years (range of 53–71) in our study compared to a mean age of 45.4 years (range of 25.2–69.7 years) at amputation in the study by Jonasson et al. The higher median age indicates a longer duration of DM in our study population and duration of DM has been shown to be an important determinant of diabetes-associated complications such as limb amputation. This assumption is substantiated by the higher prevalence of comorbidities and organ damage such as CKD in our study. Also, while Jonasson et al. determined the long-term amputation risk just in a population with DM I (without any information about the status of PAD), our analysis is performed in a specific PAD population additionally suffering from DM. Hence, it is conceivable that the risk of amputation is higher in older patients with concomitant PAD.
Despite the known preventive value of revascularization on limb amputation, particularly in patients with CLI and DM,16,17 patients with both, DM I and DM II, underwent fewer revascularization procedures than patients without DM (56% vs 70%, p < 0.001). Endovascular procedures were performed more frequently in patients with DM I (43.7%) than in those with DM II (38.8%). However, the proportion of surgical procedures was higher in patients with DM II (20.7%) than in patients with DM I (17.1%). Although speculative, a stricter adherence to evidence-based therapies such as revascularization in cases of relevant ischaemia might mitigate the outcome – at least in terms of limb salvage – in patients with PAD and concomitant DM. Such gaps between knowledge and the real-world practice (i.e. non-adherence to guidelines-recommended therapies) in patients with PAD is common and suggested to be one of the main reasons for the persistent poor overall prognosis of PAD patients.3,11,18 Another possible reason for the low rate of revascularization among PAD patients with DM might be the absence of typical symptoms such as claudication due to diabetic polyneuropathy. Lack of complaints might result in lower rates of diagnostic work-up and hence insufficient therapy. Last but not least, physicians involved in vascular care might still have the perception that distal (crural and pedal) arterial lesions, which more often occur in PAD patients with coexisting DM, may not be amenable for successful revascularization. Unfortunately, this misperception still exists. However, the specific causes of insufficient adherence to evidence-based and guidelines-recommended therapies are not known and have to be investigated in prospective studies.
In contrast to the impact on the amputation-free time, no significant influence of DM I on long-term mortality (HR: 1.031, p = 0.788) could be measured within 4 years of follow-up. DM II had only marginal adverse impact on long-term mortality (HR: 1.048, p = 0.026). This is contrary to a study which recently outlined a 1.85-fold higher risk of death in multivariate analysis for PAD patients with DM compared to those without DM. 19 Of note, the above-mentioned study included 331 patients, whereas our analysis included 41,702 PAD patients. Our findings of the adverse impact of both DM I and DM II on PAD patient’s comorbidities and complications but no further effect on mortality is in line with recently published data exploring the impact of DM in patients with CLI in an age-adjusted and propensity-score-matched analysis. 7
Strength and limitations
Our study has several limitations that have to be considered. This is a retrospective analysis. As a consequence, we can only develop hypotheses about the underlying causalities of our observations and potential selection and information bias cannot be excluded. Since our analyses were exploratory, we have not made an adjustment. As in any studies based on coding data, errors by miscoding or under-coding are possible. However, we focused our analysis on outcome endpoints (amputation and death), which are less prone to miscoding. Our study included only in-hospital treated patients. Usually, the in-hospital treated patients have more advanced stages of PAD and higher rates of comorbidities than patients who are managed in an out-patient setting. Therefore, the herein observed patients’ characteristics and the subsequent outcomes may differ in an out-patient setting. We do not have any data about the duration of DM, neither any data about the quality of antidiabetic therapy (e.g. HbA1c-levels), both having essential impact on the rate of complications and the subsequent outcome.
However, our analysis should be considered as highly relevant as its data source is contemporary, large-scale and nationwide. It shows the treatment and outcome of PAD patients additionally suffering from DM I and II in a real-world setting as the data come from unspecialized hospitals and not from vascular care centres.
Conclusion
In summary, our study depicts on a large, comprehensive database the numerous effects DM I and II have on patients suffering from PAD. Both DM I and II leads to more comorbidities and in-hospital complications, to higher PAD stages and in-hospital costs and to longer in-hospital stays. Indeed, the frequency of comorbidities varies between the two DM types. DM I has no significant impact on long-term mortality, and the impact of DM II is only marginal. In contrast to that, both conditions lead to a higher risk of amputation during up to 4 years of follow-up. DM I leads to a higher risk than DM II. Another conspicuous feature of our results is the fact that PAD patients with DM, both type I and type II, underwent fewer revascularization procedures than PAD patients without DM. This leads us to the assumption that there is a lack of adherence to the existing guidelines for treatment of PAD patients (also shown in Reinecke et al. 11 ), especially for those patients additionally suffering from DM I and DM II.
Footnotes
Acknowledgements
The authors thank the personnel of the BARMER GEK for their technical support and assistance during data retrieval.
Availability of data and materials
The data sets used and analysed during this study is available from the corresponding author in consideration of potentially applying restrictions on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The study is based entirely on anonymized data of a large German health insurance. According to local legal requirements, it does not require approval from ethics committees.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.