
Abstract
Objective
We aimed to investigate whether patients with polycystic ovary syndrome (PCOS) and a family history (FH) of type 2 diabetes mellitus (T2DM) are at increased risk of endocrinological and metabolic abnormalities, and whether this risk differs between first-degree and second-degree relatives, and between maternal and paternal transmission.
Methods
A total of 680 patients with PCOS were enrolled in this retrospective, single-center study. Endocrine and glycolipid metabolism parameters were compared.
Results
The free androgen index (FAI), and levels of fasting blood glucose (FBG), fasting insulin (FINS), homeostatic model assessment-insulin resistance (HOMA-IR), total cholesterol (TC), and low-density lipoprotein cholesterol were significantly higher, whereas sex hormone binding globulin (SHBG) levels were significantly lower in patients with PCOS and a FH of T2DM. In patients with PCOS with a FH of T2DM in first-degree relatives, age and levels of FBG, FINS, and HOMA-IR were significantly higher than those who had a FH of T2DM in second-degree relatives. A maternal history of T2DM was associated with a higher body mass index, FAI, and TG levels, and lower SHBG levels.
Conclusions
Patients with PCOS and a FH of T2DM have more severe hyperandrogenism and metabolic disorders, especially in those with maternal transmission.
Keywords
Introduction
Polycystic ovary syndrome (PCOS) is a common endocrine disorder affecting up to 5% to 20% of reproductive-age women. 1 In addition to the poor reproductive consequences, women with PCOS are at great risk of developing a number of metabolic abnormalities.2,3 Insulin resistance is present in 50% to 70% of patients with PCOS,4–6 whereas type 2 diabetes mellitus (T2DM) is found in 4% to 10%. 7 Moreover, lipid abnormalities, including elevated triglyceride (TG) and low-density lipoprotein cholesterol (LDL-c) levels, and decreased high-density lipoprotein cholesterol (HDL-c) levels, are often found in PCOS. 8
Family studies have indicated a genetic susceptibility to PCOS.9,10 A positive family history (FH) of T2DM is associated with development of PCOS.11,12 A FH of T2DM appears to be an important factor in predicting the risks of metabolic abnormalities in women with PCOS.13–15 Vrbikova et al. 16 found that defective early beta cell function was characteristic of only patients with PCOS and a positive FH of T2DM. Most studies on the FH of diabetes in patients with PCOS focused on the patients’ first-degree relatives,13,14 but few studies have examined the health status of their second-degree relatives. 15 Whether there is any difference in the clinical phenotype between patients with PCOS whose first-degree relatives have a FH of T2DM and those whose second-degree relatives have a FH of T2DM is unclear. Additionally, whether there is a difference between maternal or paternal transmission of T2DM in patients with PCOS is unclear. Furthermore, no previous studies have analyzed the effect of T2DM FH on patients who are non-obese and have PCOS. This is important because of the higher prevalence of obesity, which is an important factor of abnormal glucose and lipid metabolism,17,18 in patients with PCOS and a FH of T2DM. 15
In the current study, we aimed to investigate whether patients with PCOS and a positive FH of T2DM are at increased risk of endocrinological and metabolic abnormalities. We also investigated whether this risk differs between patients with a FH of T2DM in first-degree relatives and patients with a FH of T2DM in second-degree relatives, and between maternal and paternal transmission of T2DM. Our study may contribute to intervention and customization of treatment of PCOS depending on patients’ FH of T2DM.
Materials and methods
Subjects
Chinese female patients with PCOS, aged from 20 to 40 years, who were non-obese (body mass index [BMI] < 28 kg/m2 19,20), and who visited the Department of Gynecological Endocrinology in Ren Ji Hospital, School of Medicine, Shanghai JiaoTong University from 2015 to 2019 were enrolled. The study was based on routine clinical practice and conducted under a protocol approved by the Ethics Committee of Ren Ji Hospital (2015-087K) with informed written consent of the patients.
PCOS was diagnosed according to the revised Rotterdam criteria. 21 Two of the following three characteristics were required to confirm the diagnosis of PCOS: clinical and/or biochemical signs of hyperandrogenism, oligo- and/or anovulation, and polycystic ovaries (by ultrasound). Exclusion criteria were as follows: 1) a history of Cushing’s syndrome, androgen-secreting tumors, or adrenal hyperplasia; 2) presence of thyroid dysfunction and hyperprolactinemia; 3) use of oral contraceptives or any medication known to affect metabolic function within the previous 3 months; and 4) presence of diabetes mellitus.
A FH of T2DM was assessed by using questionnaires asking whether T2DM is prevalent in the patients’first-degree and second-degree relatives. To ensure the accuracy of the results, after the patients completed the questionnaire, we reminded them to confirm their condition with their family members suffering from diabetes. We regularly followed up the enrolled patients over the phone, reconfirmed the FH that they provided at the clinic, and corrected inaccurate family history information. Patients with more than one relative suffering from T2DM were excluded. First-degree relatives included a parent (father or mother) and full sibling (brother or sister). Second-degree relatives included a grandparent, aunt, and uncle.
Anthropometric measurements
The height and weight of each subject wearing light clothing were measured to the nearest 0.1 cm and 0.1 kg, respectively, using a digital scale and stadiometer. Weight was measured by an RGZ-120 electronic scale (Suhong Corp., Changzhou, China). The BMI was calculated as the weight in kilograms divided by the square of height in meters. Waist circumference was determined by measuring the circumference at the narrowest point between the lower border of the rib cage and the iliac crest. Hip circumference was determined by measuring the circumference at the level of the symphysis pubis and the greatest gluteal protuberance. The waist-to-hip ratio was then calculated by dividing the waist circumference by the hip circumference.
Laboratory analysis
Blood sampling for hormonal and metabolic examinations between days 2 and 5 of the menstrual cycle or, in the case of secondary amenorrhea >3 months, at any time. After basal blood samples were taken, an oral glucose tolerance test (OGTT) with sampling for blood glucose and insulin levels at 0 and 120 minutes was carried out with 75 g of an oral glucose load. Luteinizing hormone (LH), follicle-stimulating hormone (FSH), estradiol, prolactin (PRL), thyroid-stimulating hormone (TSH), total testosterone, sex hormone-binding globulin (SHBG), and androstenedione (AD) levels were detected by chemiluminescence (Elecsys Auto analyzer; Roche Diagnostics, Basel, Switzerland). Anti-Müllerian hormone (AMH) levels were measured by an enzyme-linked immunosorbent assay kit (Kangrun, Guangzhou, China). The free androgen index (FAI) was calculated as total testosterone (nmol/L)×100/SHBG (nmol/L). 22 Blood glucose and insulin samples were stored at 4°C and analyzed on the day of sampling. Plasma glucose levels were determined using glucose oxidase methodology. All measurements were performed with Roche reagents (D 2400 and E 170 Modular Analytics modules with Roche/Hitachi analyzers; Roche Diagnostics). Insulin levels were measured by radioimmunoassay. The intra-assay coefficient of variation of insulin assays was 5.5% and <10%, respectively. Insulin resistance was estimated using the homeostatic model assessment-insulin resistance (HOMA-IR), which was calculated as fasting insulin (µIU/mL)×fasting glucose (mmol/L)/22.5. 23 Total cholesterol (TC), TG, and LDL-c levels were measured with Roche reagents (D 2400 and E 170 Modular Analytics modules with Roche/Hitachi analyzers; Roche Diagnostics).
Statistical analysis
Statistical analyses were performed by using the IBM Statistical Package for the Social Sciences version 20 (IBM Corp., Armonk, NY, USA). The data were initially subjected to the Kolmogorov–Smirnov test to assess deviation from Gaussian distribution. The unpaired t test was used to assess the differences in normally distributed variables. Multiple stepwise regression analysis was further conducted to identify independent risk factors. All data are shown as mean ± standard deviation. A p value <0.05 was considered statistically significant.
Results
Clinical characteristics, and endocrinological and metabolic parameters in patients with PCOS with and without a FH of T2DM
A total of 680 patients who were non-obese (BMI < 28 kg/m2) and had PCOS were included in this study, of whom 203 had a family history of T2DM (PCOS FH+ group), while the remaining 477 did not (PCOS FH- group).
We compared clinical characteristics, and endocrinological and metabolic parameters between the PCOS FH+ and the PCOS FH- groups (Table 1). We found that SHBG levels were significantly lower, whereas the FAI and levels of fasting blood glucose (FBG), plasma glucose 2 hours after a 75-g oral glucose load (glucose 2h, fasting insulin (FINS), HOMA-IR, TC, and LDL-c were significantly higher in the PCOS FH+ group than in the PCOS FH- group (all p < 0.05). Age, BMI, waist circumference, hip circumference, waist-to-hip ratio, and levels of LH, FSH, LH/FSH, estradiol, PRL, testosterone, AD, AMH, TSH, insulin 2h, and TG were similar in the two groups.
Clinical characteristics, and endocrinological and metabolic parameters in patients with PCOS with and without a family history of type 2 diabetes mellitus.

Analyses were performed using the independent t test. Values are mean ± standard deviation.
PCOS, polycystic ovary syndrome; FH-, negative family history of type 2 diabetes mellitus; FH+, positive family history of type 2 diabetes mellitus; BMI, body mass index; WC, waist circumference; HC, hip circumference; WHR, waist-to-hip ratio; LH, luteinizing hormone; FSH, follicle-stimulating hormone; PRL, prolactin; SHBG, sex hormone-binding globulin; FAI, free androgen index; AD, androstenedione; AMH, anti-Müllerian hormone; TSH, thyroid-stimulating hormone; FBG, fasting blood glucose; glucose 2h, glucose 2 hours after a 75-g oral glucose load; FINS, fasting insulin; insulin 2h, insulin 2 hours after a 75-g oral glucose load; HOMA-IR, homeostatic model assessment for insulin resistance; TG, triglycerides; TC, total cholesterol; LDL-c, low-density lipoprotein cholesterol.
Clinical characteristics, and endocrinological and metabolic parameters in patients with PCOS and a FH of T2DM in first-degree or second-degree relatives
The 203 patients in the PCOS FH+ group were further divided into two subgroups, including the first-degree FH+ group (in which first-degree relatives were diagnosed with T2DM, n = 83) and the second-degree FH+ group (in which second-degree relatives were diagnosed with T2DM, n = 120). As shown in Table 2, age and levels of FBG, glucose 2h, FINS, and HOMA-IR in the first-degree FH+ group were significantly higher than those in the second-degree FH+ group (all p < 0.05). The remaining variables were similar in the two groups. To determine whether the effects of a FH in first-degree or second-degree relatives produced the observed differences, multiple stepwise regression models were used. In these models, a FH of T2DM in first-degree or second-degree relatives was as an independent factor only for FBG levels (p = 0.018) (Table 3).
Comparison of clinical characteristics, and endocrinological and metabolic parameters in patients with polycystic ovary syndrome and a family history of type 2 diabetes mellitus in first-degree or second-degree relatives.

Analyses were performed using the independent t test. Values are mean ± standard deviation.
FH+, positive family history of type 2 diabetes mellitus; BMI, body mass index; WC, waist circumference; HC, hip circumference; WHR, waist-to-hip ratio; LH, luteinizing hormone; FSH, follicle-stimulating hormone; PRL, prolactin; SHBG, sex hormone-binding globulin; FAI, free androgen index; AD, androstenedione; AMH, anti-Müllerian hormone; TSH, thyroid-stimulating hormone; FBG, fasting blood glucose; glucose 2h, glucose 2 hours after a 75-g oral glucose load; FINS, fasting insulin; insulin 2h, insulin 2 hours after a 75-g oral glucose load; HOMA-IR, homeostatic model assessment for insulin resistance; TG, triglycerides; TC, total cholesterol; LDL-c, low-density lipoprotein cholesterol.
Results of multivariate linear regression models (first-/second-degree FH).

#Standardized coefficient beta.
FH, family history; WC, waist circumference; HC, hip circumference; BMI, body mass index; SHBG, sex hormone-binding globulin; FAI, free androgen index; FINS, fasting insulin; insulin 2h, insulin 2 hours after a 75-g oral glucose load; HOMA-IR, homeostatic model assessment for insulin resistance; TG, triglycerides; TC, total cholesterol; LDL-c, low-density lipoprotein cholesterol.
Clinical characteristics, and endocrinological and metabolic parameters in patients with PCOS and a paternal or maternal FH of T2DM
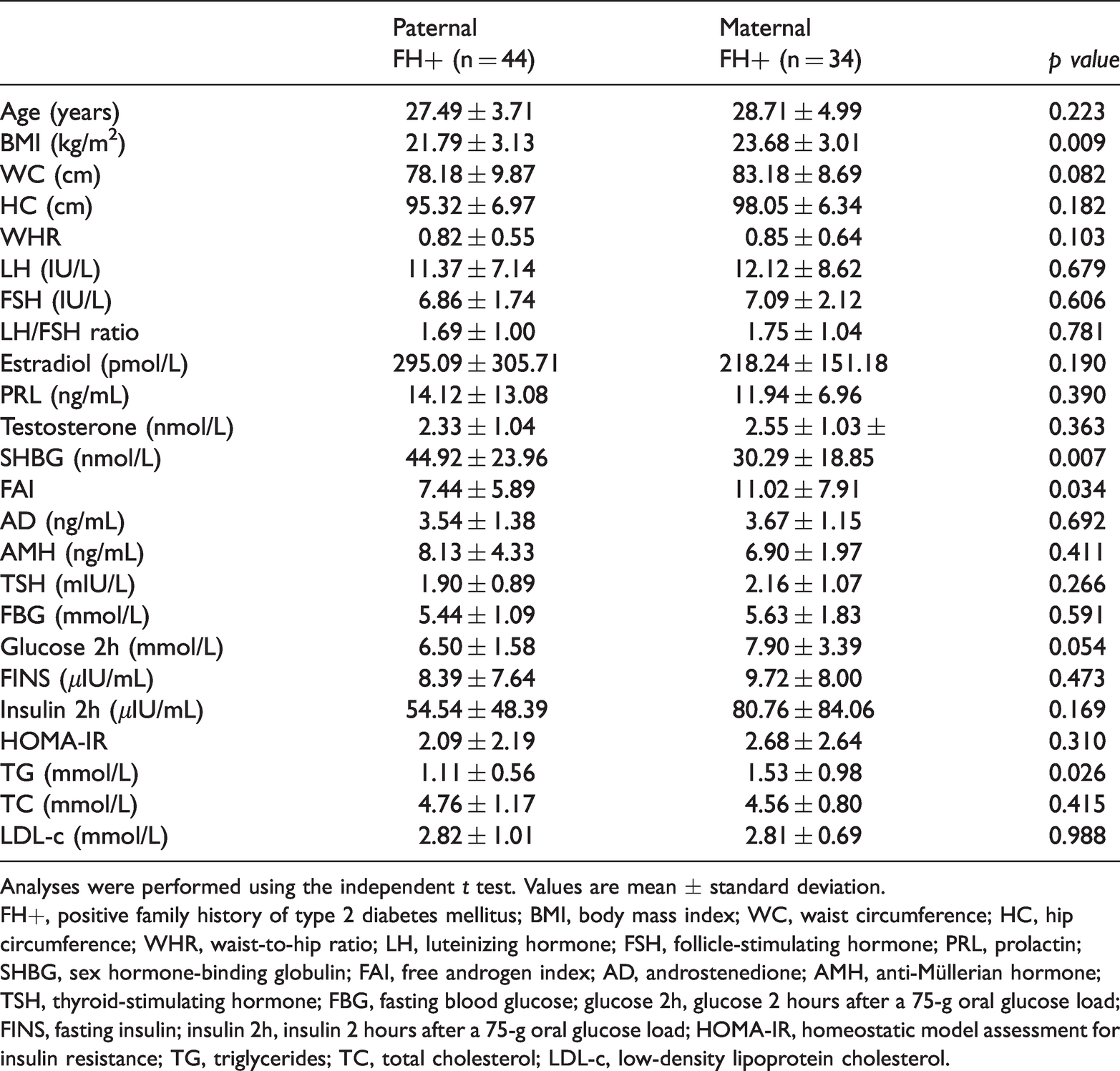
Among the 83 patients with PCOS and a first-degree relative diagnosed with T2DM, 34 had a maternal FH of T2DM (defined as a mother with T2DM) (maternal FH+ group) and 44 had a paternal FH of T2DM (defined as a father with T2DM) (paternal FH+ group). BMI, the FAI, and TG levels were significantly higher, and SHBG levels were significantly lower in the maternal FH+ group than in the paternal FH+ group (all p < 0.05). There were no differences in the remaining variables between the groups (Table 4). Multiple stepwise regression analysis showed that PCOS with a maternal FH of T2DM had higher levels of FBG, glucose 2h, FINS, and HOMA-IR (all p < 0.05, Table 5), which indicated a worse glycemic status.
Comparison of clinical characteristics, and endocrinological and metabolic parameters in patients with polycystic ovary syndrome and a paternal or maternal family history of type 2 diabetes mellitus.
Analyses were performed using the independent t test. Values are mean ± standard deviation.
FH+, positive family history of type 2 diabetes mellitus; BMI, body mass index; WC, waist circumference; HC, hip circumference; WHR, waist-to-hip ratio; LH, luteinizing hormone; FSH, follicle-stimulating hormone; PRL, prolactin; SHBG, sex hormone-binding globulin; FAI, free androgen index; AD, androstenedione; AMH, anti-Müllerian hormone; TSH, thyroid-stimulating hormone; FBG, fasting blood glucose; glucose 2h, glucose 2 hours after a 75-g oral glucose load; FINS, fasting insulin; insulin 2h, insulin 2 hours after a 75-g oral glucose load; HOMA-IR, homeostatic model assessment for insulin resistance; TG, triglycerides; TC, total cholesterol; LDL-c, low-density lipoprotein cholesterol.
Results of multivariate linear regression models (maternal/paternal FH).

Analyses were performed using multiple stepwise regression analysis. #Standardized coefficient beta.
FH, family history; WC, waist circumference; HC, hip circumference; BMI, body mass index; SHBG, sex hormone-binding globulin; FAI, free androgen index; FBG, fasting blood glucose; glucose 2h, glucose 2 hours after a 75-g oral glucose load; FINS, fasting insulin; insulin 2h, insulin 2 hours after a 75-g oral glucose load; HOMA-IR, homeostatic model assessment for insulin resistance; TG, triglycerides; TC, total cholesterol; LDL-c, low-density lipoprotein cholesterol.
Discussion
In this study, we examined endocrinological and metabolic characteristics in Chinese patients who were non-obese and had PCOS and different types of a FH of T2DM. We compared the clinical features of patients with PCOS who had a FH of T2DM in first-degree relatives with those who had a FH of T2DM in second-degree relatives. Additionally, the differences in endocrinological and metabolic characteristics were identified between patients with PCOS and a maternal FH of T2DM and those with a paternal FH of T2DM.
This study showed significant differences in glucose and lipid metabolism between patients with PCOS with and without a FH of T2DM, including FBG, glucose 2h, FINS, HOMA-IR, TC, and LDL-c levels. These findings are consistent with previous studies.13–15 These findings indicated that there were more severe abnormalities in glucose and lipid metabolism in patients who were non-obese and had PCOS with a FH of T2DM than those without a FH of T2DM. We also found that patients with PCOS and a FH of T2DM had lower SHBG levels than those without a FH of T2DM. Binding of testosterone by SHBG does not result in biological effects, and only approximately 1% to 2% of unbound free testosterone has biological activity. 24 Therefore, SHBG levels can be used to judge the severity of hyperandrogenism. A decrease in SHBG levels may lead to an increase in free testosterone levels in plasma. In this study, the FAI was higher in patients with PCOS and a FH of T2DM than in those without a FH of T2DM. Ehrmann et al. 13 found that the waist-to-hip ratio of patients with PCOS and a FH of T2DM was significantly increased, but this was not observed in our study. We speculate that the distinctive inclusion criteria of patients might have led to this difference between studies.
First-degree relatives of patients with diabetes are at increased risk of developing this disorder or having adverse metabolic outcomes compared with those with no FH of diabetes.25–28 This is also the case for second-degree relatives of patients with diabetes.29,30 First-degree relatives of patients with PCOS have a high risk of diabetes and glucose intolerance. 31 A FH of T2DM reflects a combination of genetic susceptibility, and shared environmental and behavioral factors. 32 Our study showed that levels of FBG, glucose 2h, FINS, and HOMA-IR in the first-degree FH+ group were significantly higher than those in the second-degree FH+ group. However, our study suggested that a FH of T2DM in first-degree or second-degree relatives might only independently affect FBG levels in patients with PCOS .
Whether maternal or paternal inheritance is more significant in diabetes is controversial. In several studies, a maternal history of diabetes was stronger than a paternal history of diabetes among diabetes populations. 33 Additionally, children with a parental history of diabetes, and especially a maternal history of diabetes, have an elevated risk for T2DM. 27 Animal models of gestational diabetes or maternal hyperglycemia have highlighted long-term changes in the offspring, including increased adiposity, insulin resistance, and β-cell dysfunction. 34 However, fathers, not mothers, might be disproportionately burdened with cardiovascular disease in families with PCOS. 35 In our study, patients with PCOS and a maternal history of T2DM had higher androgen levels and more severe lipid metabolic disorders than those with a paternal history of T2DM. Multivariable analysis further showed that levels of FBG, glucose 2h, FINS, and HOMA-IR were higher in patients with PCOS with a maternal history of T2DM than in those with a paternal history of T2DM. Proposed explanations for this finding include mitochondrial DNA mutations,36,37 the intrauterine environment, 38 and behavioral influence of the mother.39,40 Epigenetic changes play an important role in regulating gene expression during early development. Recent studies have identified a number of epigenetic modifications in the offspring associated with maternal hyperglycemia. 34 These biological mechanisms may lie behind our findings.
One limitation of our study is that we assessed a FH of T2DM by questionnaires, but we did not obtain information from the patients’ medical records. Use of patient recall rather than direct testing of family members is a common approach in studies assessing a FH and this is especially true for studies including a large sample size. However, use of questionnaires might have had a negative effect on the reliability of our findings. Additionally, the small sample size is a weakness of the study and may lead to false positives. Further clinical studies with a larger sample size are required to verify the findings.
In summary, we present evidence that patients who are non-obese and have PCOS and a FH of T2DM have an adverse metabolic profile. A history of T2DM with maternal transmission appears to be an important factor in predicting the risks of glucose metabolic abnormalities in women with PCOS.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Shanghai Municipal Key Clinical Specialty, the Chinese National Science Foundation (No. 81772770), the Key Discipline Project of Shanghai Municipal Commission of Health and Family Planning (15GWZK0701), the Shanghai Municipal Commission of Health and Family Planning (2017ZZ02016 and ZY[2018–2020]-FWTX-3006), and the Medical Engineering Research Fund of Shanghai Jiaotong University (YG2017MS54).