
Abstract
Aortic stenosis and diabetes mellitus are both progressive diseases which, if left untreated, result in significant morbidity and mortality. There is evidence that the prevalence of diabetes is substantially increased in patients with aortic stenosis and those with diabetes have increased rates of progression from mild to severe aortic stenosis. There are good data supporting the hypothesis that aortic stenosis and diabetes mellitus are associated with diabetes mellitus being detrimental towards the quality of life and survival of patients. Thus, a thorough understanding of the pathogenesis of both of these disease processes and the relationship between them aids in designing appropriate preventive and therapeutic approaches. This review aims to give a comprehensive and up-to-date insight into the influence of diabetes mellitus on patients with degenerative aortic stenosis, as well as the prognosis and therapeutic approach to these patients.
Introduction
Aortic stenosis (AS) and diabetes mellitus (DM) are both progressive diseases which, if left untreated, result in significant morbidity and mortality. There are data that DM influences the natural course of AS, and those with diabetes might have an increased rate of progression from mild to severe AS.1–3 In addition, the prevalence of AS and DM is high and expected to rise further in years to come. This is mainly due to the expected increase in number of elderly and obese people, 2 with both conditions related to the prevalence and progression of AS and DM.
Histopathological data suggest that degenerative AS is an active process that shares many similarities with atherosclerosis, including lipid deposition, inflammation and calcification. 4 Furthermore, risk factors for AS have been shown to be similar to those for coronary artery disease (CAD). 5
Diabetes plays an important role in enhancing the pathophysiological mechanism of atherosclerosis 6 and is a marker of poor prognosis in both the Society of Thoracic Surgeons (STS) and the European system for cardiac operative risk evaluation (EuroSCORE) II risk scores7,8 for the evaluation of procedural risk in cardiac surgery. There are data supporting the hypothesis that AS and DM are associated, with DM being detrimental towards the quality of life and survival of patients.3,9 Thus, a thorough understanding of the pathogenesis of both these disease processes and the relationship between them aids in designing appropriate preventive and therapeutic approaches.
This review aims to give a comprehensive and up-to-date insight into the influence of DM on patients with degenerative AS, as well as the prognosis and therapeutic approach to these patients.
Degenerative AS and atherosclerosis
AS is the most common valve disease that requires intervention in developed countries, and degenerative AS is the most prevalent form of AS.10,11
There is compelling histopathologic and clinical data suggesting that degenerative AS is, in fact, an active disease involving lipoprotein deposition, chronic inflammation, osteoblastic transition of valve interstitial cells and active leaflet calcification.12,13 The initial stages of degenerative AS show more similarities with atherosclerosis than the progressive phase, in which fibrosis and calcification are more pronounced.
Macrophages, mast cells, CD4+ T cells and CD8+ T cells have been identified from the surgically removed calcific aortic valves. 14 Moreover, inflammation, assessed through leukocytes and tumour necrosis factor (TNF)-α transcripts, within degenerative AS is associated with an active remodelling process, severity of AS and haemodynamic progression rate. 15 The interplay between low-density lipoprotein (LDL) cholesterol levels and degenerative AS has already been described. 16 This connection between lipids and the development of degenerative AS has been supported by the observation of diffuse atherosclerotic lesions in the aortic leaflets of patients with familial hypercholesterolemia and no other atherosclerotic risk factors. 17 In addition, a causative role of elevated LDLs and the risk of both vascular atherosclerosis and AS has been presented in the Cardiovascular Health Study. 18 Finally, valvular endothelial cells and interstitial cells (VECs and VICs) play an important role in the progression of degenerative AS. Various VIC phenotypes have been identified in diseased human heart valves including quiescent fibroblast-like VICs, which can differentiate into osteoblast-like VICs, which are responsible for the active deposition of calcium in aortic leaflets.19,20
Furthermore, the Multi-ethnic study of atherosclerosis (MESA) investigators have investigated the link between metabolic syndrome, DM and vascular (coronary artery) calcification. 21 Their results have shown that for patients with no coronary artery calcification at baseline [as assessed by computed tomography (CT) scanning], the relative risk of incident coronary artery calcification at follow-up scanning (mean of 2.4 years) was 1.7- to 1.9-fold higher in patients with the metabolic syndrome, DM or both conditions, than in patients without DM or metabolic syndrome. 21 The interplay between DM and vascular calcification is important, as arterial wall stiffening further increases the global afterload on an already high left ventricular (LV) burden in patients with AS.
DM and atherosclerosis
Although development of diabetes-related atherosclerosis follows the same histopathological course as atherosclerosis in non-diabetic patients, atherosclerosis is accelerated in both type 1 and type 2 DM. 22 Hyperglycaemia itself induces a large number of alterations in vascular tissue that potentially promotes accelerated atherosclerosis; including non-enzymatic glycosylation of proteins and lipids; oxidative stress and protein kinase C activation. 23 However, the development of atherosclerosis might not only be a result of hyperglycaemia but also caused by the secondary insulin resistance, dyslipidemia, hypercoagulability and altered secretion of local regulatory substances. Collectively, these abnormalities of endothelial, platelet, smooth muscles, lipoproteins (mainly LDL) and coagulation are the main contributors to accelerated atherosclerosis in diabetic patients.
It has been proposed that enhanced inflammation is a process that is common to both degenerative AS and DM.24,25 However, it should be kept in mind that despite having similarities with atherosclerosis, the aortic valve has some inherent properties that differ from the vascular wall. 26 The tissue and cellular organization as well as the effect of haemodynamic stress imposed upon the aortic valve are quite different from the vessels. For example, statins, although very efficient to reduce clinical events in patients with atherosclerosis, are ineffective in preventing progression in degenerative AS or reducing valve-related adverse events. 27
The link between DM and degenerative AS
Epidemiology
Recent large studies have shown that the prevalence of diabetes is higher in cohorts with AS than in the general population. In the CURRENT AS population cohort of 3815 patients with severe AS, 11.4% patients had DM, 21% of whom were on insulin therapy, while in the PRIMID AS study 14.4% of the 174 patients had diabetes.28,29 In addition, from 2009 to 2015 in the United States, among Medicare beneficiaries with severe AS undergoing surgical aortic valve replacement (SAVR), the prevalence of diabetes increased from 19.7% to 31.6%. 30 A similar trend is observed in Spain in the last 15 years. 31 The connection is also distinct in the converse. In a large population-based prospective study from Larsson and co, the incidence of AS in patients with type II DM during long-term follow-up was 3.42% versus 1.68% in non-diabetic patients (p < 0.05). 3
The link hypothesis
Cote et al. 15 analysed excised aortic valves from 285 patients with degenerative AS undergoing aortic valve replacement (AVR). They revealed that in 81 (28.4 %) patients, the presence of chronic inflammatory infiltrates was documented within valve tissue, which was characterized by the existence of a cluster of cells as well as the presence of neovascularisation and osseous metaplasia. To summarize, their findings suggest that chronic inflammation, although not present in most of the explanted tissues, is nonetheless an important contributor to the pathophysiology of degenerative AS. Among 2.683 participants in the Framingham Heart Study’s offspring cohort, inflammatory biomarkers (C-reactive protein (CRP), intercellular adhesion molecule-1, interleukin-6 and monocyte chemoattractant protein-1) were associated with calcified aortic valve on echocardiography. 32 However, the association is non-significant once adjusted for cardiovascular risk factors, suggesting that the observed association between inflammatory markers and valvular calcification may be mediated by common risk factors, such as diabetes. As shown by Natorska et al., 33 DM augments the expression of proinflammatory CRP and tissue factor in patients with severe AS. CRP activates macrophages and T lymphocytes, complement fixation and modulates platelet activation, 34 while tissue factor affects coagulation and leads to thrombin formation which, in turn, increase valve calcification. 35 Elevated plasma CRP level is associated with the development of DM, complementing the previous data which demonstrated independent association between CRP and AS progression. 36 Furthermore, it has been shown that in VIC, transient hyperglycaemia leads to excessive synthesis of proinflammatory phospholipids and an activation of coagulation, which might facilitate AS in patients with poorly controlled diabetes. This is another hypothesis in the link between degenerative AS and DM. In other words, DM both induced and accentuated inflammatory response and enhanced lipid accumulation that also affects the aortic valve. An important causative role of diabetes in pathogenesis and development of degenerative AS and the potential impact of intensive risk-factor modification in mitigating the burden of this disease have been demonstrated in the Cardiovascular Health in Ambulatory Care Research Team (CANHEART) study. 37 In this study, diabetes [hazard ratio (HR): 1.49; 95% confidence interval (CI): 1.44–1.54], among other risk factors, was significantly associated with increased risk of developing severe AS (p < 0.001).
Although required, it is unlikely that adequately powered trials with sufficient long-term follow-up will be conducted to evaluate impact of DM and other atherosclerotic risk factors on AS. And this is only one among several issues that needs to be addressed in order to understand the complex interplay between diabetes and AS (Table 1). Nevertheless, optimal management of these risk factors is warranted, given the other established cardiovascular benefits. 38 However, large registries, such as UK Biobank registry, which encompasses hundreds of thousands of middle-aged persons, might, to some extent, replace the lack of randomized trials and help in determining whether DM influences the incidence and progression of AS.
Key issues to address in severe AS patients with diabetes.
AS: aortic stenosis.
Influence of diabetes on AS progression
Diabetes not only predisposes to degenerative AS but may also contribute to faster progression of AS(1). Several authors have demonstrated the interaction between DM and the progression and severity of AS, especially in patients with less significant (moderate) AS.1,33,39 However, the data supporting this hypothesis are inconsistent, and, in general, there is lack of data on the longitudinal effect of diabetes on the progression of AS severity. The studies evaluating the influence of DM on AS progression have been presented in Table 2.
Studies investigating influence of DM on AS incidence and progression.
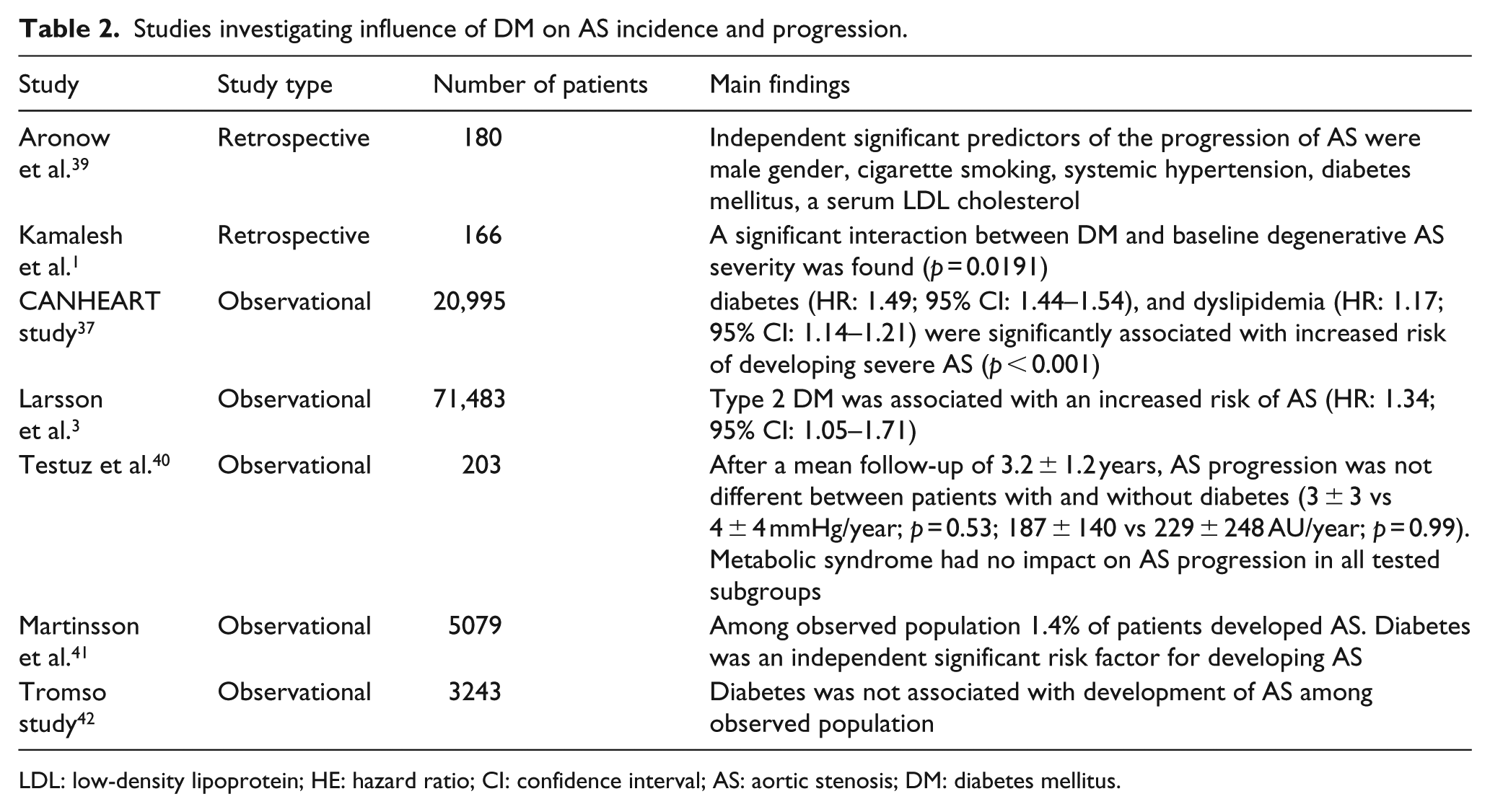
LDL: low-density lipoprotein; HE: hazard ratio; CI: confidence interval; AS: aortic stenosis; DM: diabetes mellitus.
Aronow et al. 39 first reported that in 48 of 180 patients with mild AS, mean annual progression in peak systolic gradient was higher in diabetic compared to non-diabetic patients (5.7 vs 4 mmHg, p < 0.05). However, this was a retrospective study involving only patients ⩾60 years and with multiple confounding factors. Kamalesh et al. 1 showed that DM has accelerated progression of AS only in patients with moderate stenosis at baseline. However, all other analysed parameters did not show a significant difference between diabetic and non-diabetic patients, nor did the influence on the progression of the AS. For instance, in patients with mild AS, despite a long period of follow-up and less-calcified valves, diabetes did not affect the progression of the disease. The difference in gradients and the annual rate of progression were not significant even in patients with moderate AS. Therefore, the results of this study should be interpreted with caution. Among the 1.12 million Canadians aged ⩾65 who were followed for more than a decade, the CANHEART study investigators 37 found an independent and dose-response relationship between hypertension, diabetes and dyslipidemia and the risk of developing severe AS. The combination of these risk factors accounted for approximately one-third of the attributable risk for AS on a population level. Hypertension had the highest attributable risk at 23.4%, followed by diabetes [5.6%; (HR: 1.49; 95% CI: 1.44–1.54)] and dyslipidemia (4.4%). In the recently published study by Larsson et al., 3 DM type II was associated with increased risk of developing AS (HR: 1.34; 95% CI: 1.05–1.71).
On the other hand, data from a study by Testuz et al., 40 a prospective study of 203 patients with at least mild AS, showed no impact on AS progression in patients with diabetes and metabolic syndrome after a 2-year follow-up. A possible theory is that cardiovascular risk factors may play a role at the early phase of AS disease, while they have no or limited influence on AS progression in latter stages of the disease. This hypothesis is in line with observation from Simvastatin and Ezetimibe in Aortic Stenosis (SEAS) trial, 27 in which lipid-lowering therapy did not reduce the composite outcome of combined aortic valve events and ischaemic events in patients with AS. Still, high-risk AS patients, with known atherosclerotic disease or DM, were not included in the SEAS trial, which limits the interpretation of the obtained results. Contradictory results regarding the association between DM and AS were also obtained in two Scandinavian studies. In a study by Martinsson et al., 41 DM was associated with an approximately three-fold increased risk of AS in a cohort of 5079 Swedish adults but was not associated with the risk of AS in a cohort of 3243 adults in Tromso study. 42 The Tromso study was probably underpowered for concluding association between DM and AS as only six subjects among DM patients developed AS.
Bearing in mind the opposing results of the published studies, definite evidence that DM does indeed cause/worsen AS is lacking. Nevertheless, to date, there has been no randomized controlled trial to specifically examine whether antihyperglycemic/antidiabetic therapy can prevent the development or slow the progression of AS.
Myocardial changes in diabetic patients with AS
The symptoms in AS are due to an imbalance between the increase in LV haemodynamic load caused by valvular obstruction and the capacity of the LV to overcome this increase in load both at rest and during exercise. The mechanical signal generated by increased LV systolic pressure initiates a cascade of biological events, including re-expression of immature foetal genes, which lead to cardiac growth in patients with AS. 43 In patients with degenerative AS, LV concentric remodelling or hypertrophy has been connected to worse myocardial function and increased risk of cardiac events and mortality compared to patients with normal LV geometry or with eccentric LV hypertrophy.44,45
Interstitial and perivascular fibrosis is present in diabetic patients. 46 In addition to the increase in collagen deposition, cross-linking of collagen fibres may be increased by diabetes, contributing to the reduction in ventricular compliance. 47 Although clinical evidence to support this notion is not in agreement, some studies48,49 indicate that glycation of collagen fibres is indeed increased in hearts of diabetic patients.
There are several potential mechanistic explanations how DM affects the myocardium of patients with concomitant AS. The characteristics of DM, namely hyperinsulinemia, insulin resistance, hyperglycaemia and increased level of non-esterified fatty acids, contribute to oxidative stress, advanced glycation end products,50,51 altered calcium handling (diminished Ca 2 sensitivity of contractile elements in cardiomyocytes, prolongation of action potential duration and slower decay of Ca 2 transient52,53) and metabolic derangements (diabetes reduces the efficiency of energy production by increase in fatty acid uptake and suppression of glucose oxidation 53 ).
A study using cardiac magnetic resonance imaging (cMRI) demonstrated significant association of insulin resistance and hyperglycaemia with an increase in LV mass and LV mass-to-LV end-diastolic volume ratio regardless of age and gender. 54 Metabolic syndrome and/or diabetes compound the development of more concentric hypertrophy in the presence of AS. 55 Lindman et al. 10 showed that diabetic patients with AS had an increased LV mass, LV end-systolic dimension, LV end-diastolic dimension and decreased left ventricular ejection fraction (LVEF) and longitudinal systolic strain (p < 0.01 for all) compared to non-diabetic patients. In multivariable analyses after adjusting for confounding factors, DM was an independent predictor of increased LV mass (β = 26 g, p = 0.01), LV end-systolic dimension (β = 0.5 cm, p = 0.008) and LV end-diastolic dimension (β = 0.3 cm, p = 0.025). After additionally adjusting for LV mass, DM was associated with reduced longitudinal systolic strain (β = 1.9%, p = 0.023) and a trend towards reduced LVEF (β = −5%, p = 0.09). Their results support the hypothesis that DM has an adverse effect on LV remodelling and function in patients with severe degenerative AS. It has also been suggested that diabetes [standardized partial regression coefficient (SPRC) = –0.187, p = 0.018], is associated with poor postoperative LV mass regression unrelated whether the treatment was transcatheter aortic valve implantation (TAVI) or SAVR. 56 Diabetes is also associated with higher prevalence of persistent LV hypertrophy (47% vs 39%, p < 0.05) and independently predicts less LV mass reduction in hypertensive patients who are taking antihypertensive treatment. 57
Imaging approach to diabetic AS patients
LV hypertrophy is initially an adaptive process to restore wall stress and cardiac performance, which characterizes both AS and DM. Ultimately, there is progressive deterioration in LV function which increases the risk of death and heart failure. This transition from adaptation to decompensation is driven by progressive myocyte death and myocardial fibrosis.3,58 Therefore, we emphasize that it is important to consider AS as a condition that affects both the valve and the myocardium. Indeed, current guidelines recommend AVR in patients with severe AS and evidence of LV decompensation, defined by either the presence of symptoms or an impaired LVEF <50%. 59
Assessment of myocardial structure and function
In patients with AS, apart from the standard echocardiographic parameters that define AS severity, namely transvalvular gradients, valve area and maximal velocity across the valve, the parameters that define the LV structure and function are also of significant importance. It is now widely recognized that LVEF is not a sensitive marker of myocardial dysfunction, 60 and impairment in LVEF is often a late manifestation that, once noted, may not be reversible. 61
The most frequent echocardiographic finding in both, asymptomatic diabetic and AS patients is LV diastolic dysfunction with normal LVEF. LV diastolic dysfunction evaluated by transmitral LV filling pattern (i.e. abnormal relaxation and/or pseudonormal filling) is observed in 47%–75% of asymptomatic normotensive patients with well-controlled type II DM.62,63 In patients with DM, high diastolic LV stiffness hinders LV remodelling and raises LV filling pressures at similar LV filling volumes as in patients with heart failure. 64 Mechanisms responsible for raising myocardial stiffness in DM patients consist of excessive fibrosis, 65 deposition of advanced glycation end products 66 and high cardiomyocyte stiffness. 64 Falcão-Pires et al. 49 have through histomorphometry and immunohistochemistry quantified myocardial collagen volume fraction and myocardial advanced glycation end-product deposition in patients with and without DM who were referred for AVR due to the severe AS. They have demonstrated worse diastolic LV dysfunction in diabetic AS patients versus non-diabetic AS patients. Impaired LV diastolic function and increased myocardial fibrosis in diabetic AS patients is also shown through reduced LV end-diastolic distensibility, higher LV end-diastolic pressure (21.1 mm Hg for AS vs 28.4 mm Hg for AS-DM; p = 0.04), higher myocardial collagen volume fraction (non-diabetic AS 12.9% vs AS-DM 18.2%; p < 0.001), more advanced glycation end-product deposition in arterioles, venules and capillaries (non-diabetic AS 14.4 score per 1 mm2 vs AS-DM, 31.4 score per 1 mm2; p = 0.03).
Systolic LV function in AS patients might be additionally impaired by diabetes, mainly through the lower midwall shortening compared to subjects without diabetes. 67 In fact, more sensitive indices of systolic function such as echo tissue Doppler and strain rate imaging (SRI) indicate additional subclinical reduction in LV systolic function in patients with diabetes.68,69 Taking into consideration the high global afterload that the LV myocardium is subject to in AS patients who often have concomitant hypertension, the valvuloarterial impedance (Zva), a combined measure of arterial systolic pressure and mean transvalvular gradient, might be a parameter of interest. In patients with additional diabetes or/and systemic hypertension, an increase in blood pressure superimposed on an increased valvular resistance leads to a significant increase in LV systolic wall stress. The contribution of vascular load is an essential factor to be noted in all patients with AS, as it further increases LV global afterload, which is associated with decreased stroke volume, impaired myocardial function and reduced survival.70,71
Cross-sectional imaging techniques in AS assessment
While echocardiography is currently the gold standard of valvular imaging and assessment of severity in AS patients with or without diabetes, modern noninvasive imaging, such as positron emission tomography (PET), CT and cMRI, provides important information on LV remodelling and cardiac function. Measures from these investigations are now proven to be good outcome measures and have the potential to inform how we manage these complex patients.
CT and PET/CT
CT imaging has an important role in assessing calcium burden in the aortic valve and correlates closely with echocardiographic measures of haemodynamic severity. 72 Recent data have demonstrated that the aortic valve CT calcium score provides powerful prediction of disease progression and prognosis.73,74 In the TAVI era, CT angiography is increasingly used for valve sizing prior to TAVI procedures. 75 PET tracer, 18 F-Sodium fluoride, has been used to image developing microcalcification in stenotic aortic valve. 76 As such, it might provide complementary information to CT measured aortic valve calcification.
CT imaging is able to detect macroscopic calcium deposits in the aortic valve; however, it is unable to identify fibrosis or lipid deposition, which are the hallmark of the myocardium changes in diabetic patients with AS. Fibrosis occurs later as the AS advances, and it is characterized by three main patterns: endocardial fibrosis, microscars (mainly in the subendocardium) and diffuse interstitial fibrosis. 77 Furthermore, reduced capillary density, in absolute terms as well as in relation to the number of cardiomyocytes, accompanies myocardial fibrosis in patients with severe AS. 78 All types of fibrosis represent potential imaging targets that might be helpful in determining the timing for AVR in asymptomatic patients. As fibrotic changes are also commonly observed in the myocardium of diabetic patients, measuring fibrosis might be of special importance in asymptomatic diabetic patients with severe AS. However, to this point, no study has specifically compared the amount of fibrosis and its significance in diabetic AS patients versus non-diabetic AS patients.
Cardiac MRI is the imaging modality that offers a direct, whole-heart assessment of myocardial fibrosis. Early studies suggested that transthoracic two-dimensional echocardiography could also assess the extent of fibrosis in DM;79,80 however, these techniques have not been translated into clinical practice. At present, myocardial fibrosis is better measured by cMRI. Late gadolinium enhancement can assess focal scarring and extracellular volume expansion (ECV), a surrogate of interstitial fibrosis. This can be quantified by pre and post contrast T1 mapping.81,82
Focal midwall myocardial fibrosis has been demonstrated in up to 60% of patients with AS, 83 and it is associated with impaired cardiac function and adverse cardiovascular events in AS patients.84,85 Of note, focal midwall fibrosis was shown to be an independent predictor of cardiovascular and all-cause mortality in patients with haemodynamically significant AS.83,85 Recent data from the British Society of Cardiovascular Magnetic Resonance (BSCMR) Valve Consortium on myocardial scar and mortality in severe AS showed that focal myocardial fibrosis quantified by Late Gadolinum Enhancement (LGE) was present in over 50% of patients, and this was associated with a two-fold higher mortality rate and associated with higher all-cause and cardiovascular mortality both in the context of surgical and transcatheter AVR. Musa et al. 86 demonstrated that indexed ECV increase across patients with mild, moderate and severe AS (of which 15% had diabetes), and that increase across the indexed ECV tertiles was observed for each of the markers of disease severity and LV decompensation: indexed LV mass, peak aortic valve velocity, plasma high-sensitivity cTnI concentrations, serum brain natriuretic peptide (BNP) concentrations, diastolic dysfunction and longitudinal systolic dysfunction (p < 0.05 for all).
Clinical implications of DM in patients with AS
In clinical practice, most asymptomatic patients with diabetes and isolated severe AS have preserved LVEF and require a careful risk stratification in order to decide between elective intervention and a watchful waiting strategy. Moreover, impaired LV global myocardial deformation is associated with an increased risk for earlier symptom onset and the need for AVR. 87 Thus, beyond the conventional assessment of LV hypertrophy and LVEF, early assessment of LV deformation parameters (in particular global longitudinal strain) and myocardial fibrosis (estimated by cMRI) could be helpful in the decision-making process, especially in diabetics, in whom the presence of symptoms could be masked. However, in view of the fact that no single parameter of LV function predicts the optimal timing for AVR in asymptomatic diabetic patients, all available imaging information must be considered for optimal decision-making in clinical practice.
Impact of DM on patients with AS: treatment and prognostic implications
DM influences the event-free survival of patients with AS, both those who are treated conservatively and those who are subjected to percutaneous or surgical intervention. This was evidenced within the data available from the CURRENT AS registry where DM was associated with non-cardiac death in AS patients. 88 Furthermore, Rosenhek et al. 89 in a review of 116 patients with severe AS, quantified as a peak velocity of >5 m/s, showed that diabetes was an independent predictor of poor outcome, specified here as death and indication for AVR in AS in addition to elevated cholesterol levels and peak velocity of >5.5 m/s. In the recently published registry by Lancellotti et al., 90 DM was an independent determinant of cardiovascular mortality in patients with severe AS. Linke et al. 91 have recently published a large single-centre observational study of 1818 patients who underwent TAVI. All-cause 3-year mortality was the primary endpoint with patients stratified according to gender and presence of diabetes. Diabetes in males showed a significant increase in all-cause mortality, 39.8% versus 29.7% (p < 0.01) compared to non-diabetic males. There was no difference within the diabetic and non-diabetic female cohort, and the presence of diabetes did not increase 30-day mortality within the whole cohort or males alone. 91 It is therefore uncertain whether DM independently affects AS-related outcomes, and further studies in larger populations are needed.
Comorbidities, such as chronic kidney disease and CAD are common in DM patients and affect the risk–benefit analysis because they exert an independent influence on a patient’s life expectancy regardless of the valvular disease. Therefore, the effect of DM on AS patients can be compounded by commonly coexisting conditions. Microvascular complications are major contributors to morbidity and mortality in patients with diabetes. 56 One potential mechanism in the association of diabetes and AS is that diabetes additionally impairs coronary microvascular function in asymptomatic patients with severe AS and non-obstructed coronary arteries. 92 It has been shown that impaired microvascular function in asymptomatic patients with severe AS is a predictor of a worse outcome in severe AS patients.93–95 Within the PRIMID AS population, it was shown that patients with a lower myocardial perfusion reserve were associated with development of symptoms in the medium term, 29 and this may be worsened in patients with diabetes. The reduction in microvascular circulation in AS patients may also be responsible for myocardial ischaemia and potentially fatal arrhythmias that are observed in diabetic AS patients with normal or non-obstructive epicardial coronary circulation.29,92,96
Medical therapy
Medical treatment of diabetic patients with severe AS using antidiabetic medication in the form of both oral tablets and insulin may target the valve or the myocardium. In theory, specific medical therapy should halt AS progression, reduce its haemodynamic repercussions on LV function and remodelling and improve clinical outcomes. However, none of the current medications that are used in patients with AS for treating cardiac disease or comorbidities appear to affect the survival of patients with AS, nor has it been proven to slow down the course of the disease. As discussed, diabetes and metabolic syndrome has been identified as a potential contributor to the progression of AS and the occurrence of adverse events in the context of AS. 97 However, there is no consensus based on the evidence at present.
Due to the similarities that degenerative AS has with atherosclerotic process, statins have been the most extensively studied medications in AS. Unfortunately, none of these trials were able to demonstrate reduced haemodynamic progression or improved clinical outcomes.27,98,99 However, except for the SEAS trial, 27 none of these trials were powered adequately to detect significant clinical benefits. A meta-analysis comprising 2344 patients reported no significant improvement in haemodynamic parameters, AVR rates or cardiovascular death. 99 Lipoprotein(a) [Lp(a)] has been also proposed as a potential therapeutic target in AS. A post hoc subanalysis of the Aortic Stenosis Progression Observation: Measuring Effects of Rosuvastatin trial (ASTRONOMER) showed that in patients with mild to moderate AS, elevated levels of Lp(a) were associated not only with faster progression of AS but also with significantly worse clinical outcomes after multivariable adjustment. 100 Niacin, antisense-specific Lp(a) inhibitors and PCSK9 inhibitors may reduce Lp(a) levels 101 and potentially a new treatment target. The Early Aortic Valve Lipoprotein(a) Lowering trial (EAVaLL; NCT02109614) is currently randomizing patients with aortic sclerosis or mild AS to niacin versus placebo, evaluating the progression of aortic valve calcium score by cardiac CT as the primary endpoint.
Arterial hypertension and AS are frequently present as concomitant diseases. Hypertension increases afterload, thereby accelerating LV hypertrophy. Indeed, in the study by Rieck et al., 102 among 1616 patients with initially asymptomatic mild-to-moderate AS, hypertension was associated with a more abnormal LV structure and increased CV morbidity and mortality during a 4.3-year follow-up. However, there are no studies addressing specific antihypertensive medications in patients with AS. In clinical practice, diuretics are avoided if the LV chamber is small because even smaller LV volumes may reduce the cardiac output. Angiotensin-converting enzyme (ACE) inhibitors might be advantageous due to the potential beneficial effects on LV fibrosis in addition to hypertension control, 103 while beta-blockers should be a drug of choice in patients with concomitant CAD. 104 Angiotensin receptor blockers might even have superior effects on valve fibrosis and calcification, 105 but, again, prospective large well powered studies are lacking. Vasodilators are often avoided in hypertensive patients with severe AS because of concern that they may precipitate life-threatening hypotension although there is no trial data to support this assertion.
Interventional therapy
The only treatment shown to improve survival in severe AS patients is AVR. It has been shown that diabetic patients have elevated postoperative morbidity and mortality compared to non-diabetic patients after SAVR. 106 Tissue ischemia-reperfusion injury, often seen after SAVR, may cause the release of various inflammatory mediators and diabetic patients, as discussed above, are more sensitive to the oxidative stress and inflammation. 107 Open-heart surgery can initiate a systemic inflammatory response syndrome (SIRS) that is linked to an unfavourable outcome. 108 However, SIRS is also possible after TAVI with the influence on outcome. As TAVI is now an established therapeutic option for inoperable or high-risk AS patients, with tendency to shift towards lower-risk patients, analysis regarding the influence of DM on TAVI outcome has been done. In a careful review of the literature surrounding SAVR versus TAVI outcome in diabetic patients, an analysis from the PARTNER 1A trial have shown that diabetic patients have lower all-cause mortality after TAVI than after SAVR (18% vs 27.4%, p < 0.05). 109 These results were consistent whether the trans-femoral or trans-apical approach was used. In addition, DM impairs LV mass regression after SAVR, which indicates that people with diabetes have less benefit and a greater risk with SAVR compared to non-diabetic patients. 56 Contrary to this, López-de-Andrés et al. 31 have recently shown in a large retrospective study that type II DM patients have lower intrahospital mortality after SAVR than non-diabetic patients.
Continuous improvement in surgical approaches and technique, including minimally invasive SAVR and increased use of new tissue (stented or sutureless) valves, might to some extent explain conflicting results regarding the SAVR in diabetic patients. Furthermore, the increasing use of TAVI may have a beneficial influence on the mortality rate of AVR by subjecting more patients with high-risk (mainly type II) DM to TAVI instead of SAVR. Importantly, this was not reflected in higher mortality rate in DM patients undergoing TAVI. In study by Tokarek et al., 110 DM was not associated with a higher 30-day or 12-month all-cause mortality after TAVI nor was it associated with decreased post-procedural quality of life. A study by Mendez-Bailon et al. 111 as well as a meta-analysis by Sun et al. 112 did not find that diabetic patients have worse short-term outcome compared to non-diabetic patients when it comes to TAVI versus SAVR, or to TAVI only. In addition, in a study by Mendez-Bailon et al. diabetic patients undergoing SAVR had a higher mortality than diabetics undergoing TAVI. However, this study had significant limitations, including that diabetic patients undergoing TAVI were significantly younger than the non-diabetic patients and the degree of frailty and functional capacity of patients undergoing valve implantation was unknown. These factors could affect the study results. A randomized trial by Chorin et al. 113 showed no difference in 30-day mortality after TAVI between diabetic and non-diabetic patients. Similar results were obtained by Berkovitch et al. 114 who demonstrated no difference between insulin-dependent diabetic patients, non insulin-dependent diabetic patients and non-diabetic patients when looking at peri-procedural and mid-term outcome following TAVI, except for a higher incidence of acute kidney injury in insulin-dependent diabetic patients. On the other hand, a large registry from STS/American College of Cardiology (ACC) transcatheter valve therapy that encompassed 47,643 patients [of which 17,849 (37.5%) were patients with DM, and 6600 of the diabetic patients were on insulin] indicated that DM was associated with an increased 1-year mortality (HR: 1.30; 95% CI: 1.13–1.49; p < 0.001). 115 Subgroup multivariable analysis showed stronger mortality association in insulin-dependent diabetics (HR: 1.57; 95% CI: 1.28–1.91; p < 0.001) than in non-insulin dependent diabetics (HR: 1.17; 95% CI: 1.00–1.38; p = 0.052). In the study conducted by the investigators from the Mayo clinic DM (HR: 1.7, p < 001) was, along with older age, decreased LVEF and absence of AVR, an independent risk factor for mortality. 116 Danielsen et al. 117 recently reported that DM is the most frequent risk factor associated with hospital readmission within 30 days after TAVI (odds ratio (OR): 1.13–1.18). It also seems that males with DM are at higher risk for all-cause mortality after TAVI compared to males without DM, or compared to females, regardless of whether they are diabetics or non-diabetics. 91 In the same study, the interaction between male gender and DM was identified as an independent predictor of 3-year mortality after TAVI (HR: 1.88; p < 0.01). Larger studies (⩾100 patients) comparing SAVR versus TAVI in diabetic or non-diabetic patients are summarized in Table 3.
Larger studies comparing TAVI versus TAVI or SAVR versus TAVI in diabetic or diabetic versus non-diabetic patients.
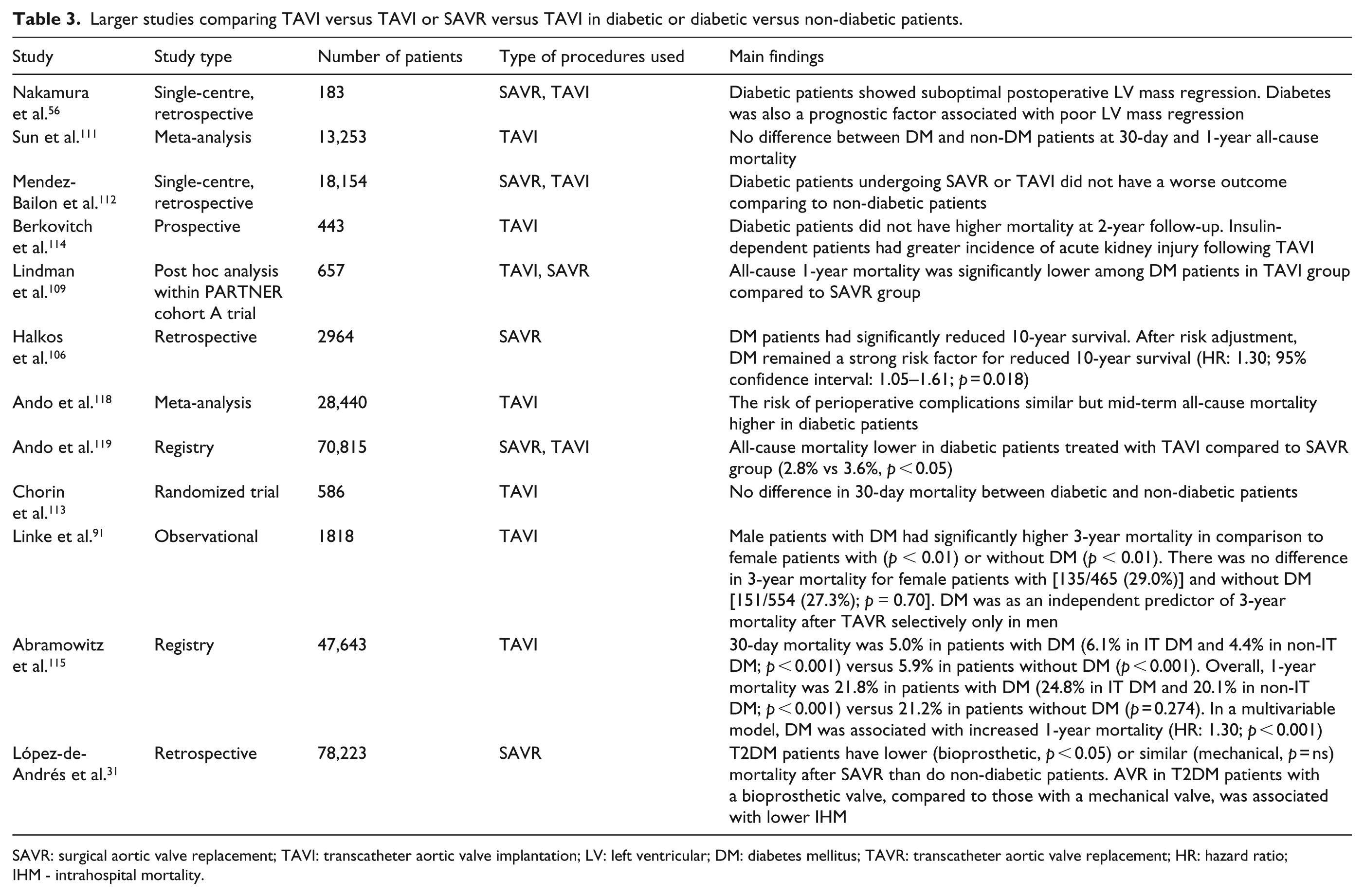
SAVR: surgical aortic valve replacement; TAVI: transcatheter aortic valve implantation; LV: left ventricular; DM: diabetes mellitus; TAVR: transcatheter aortic valve replacement; HR: hazard ratio; IHM - intrahospital mortality.
Despite the many studies quoted above, the optimal treatment for severe AS in both non-diabetic and diabetic patients is still contentious. Thus, several trials are currently investigating an early/elective interventional approach to asymptomatic severe AS patients [Early TAVR trial (NCT03042104), Evolved trial (NCT03094143), Estimate trial (NCT02627391), Avatar trial (NCT02436655)].120,121 The exceptions are patients with associated significant CAD for whom current guidelines recommend concomitant coronary artery bypass and SAVR even in cases of moderate AS. 59 This is even more pronounced now, as the latest European Society of Cardiology (ESC) guidelines on myocardial revascularization recommend coronary artery bypass grafting (CABG) over multivessel percutaneous coronary intervention (PCI) in diabetic patients. 122 However, current ESC and American College of Cardiology/American Heart Association (ACC/AHA) guidelines do not specifically state the best modality treatment of patients with isolated AS and concomitant diabetes but without significant CAD.59,123 In patients with isolated AS and concomitant DM, existing data appear to favour TAVI over SAVR as the optimal solution. However, the cited studies do not give us sufficient and reliable data on the severity and/or duration of diabetes, and majority of them were observational/retrospective in nature, with some significant differences among analysed groups of patients. Importantly, long-term follow-up data are lacking. At present, there is no large randomized trial looking at patients with AS and DM. Thus, until this happens, all of the studies above should be considered as hypothesis-generating.
Conclusion
Both AS and DM are long-term, progressive and often silent diseases that once symptomatic have a poor prognosis. DM appears to be associated with an increased prevalence of AS and contributes to increased AS progression although further data from larger epidemiological and well-controlled studies are required. Therefore, having both of the diseases carries a higher risk of an adverse event. In the absence of randomized controlled trials specifically in patients with AS and DM, individual risk assessment on a patient-by-patient basis, should be the cornerstone for treatment decisions. In patients being considered for intervention, discussion within a heart valve team and together with other specialist (diabetologist/anesthesiologist) is strongly recommended. This applies to both symptomatic and asymptomatic diabetic patients with severe AS. Prospective randomized trials are necessary for a more conclusive decision on what is the best treatment option for diabetic patients with severe AS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.