
Abstract
Diabetes-induced atherosclerotic cardiovascular disease is the leading cause of death of diabetic patients. Neuronal regulation plays a critical role in glucose metabolism and cardiovascular function under physiological and pathological conditions, among which, neurotransmitter neuropeptide Y has been shown to be closely involved in these two processes. Elevated central neuropeptide Y level promotes food intake and reduces energy expenditure, thereby increasing adiposity. Neuropeptide Y is co-localized with noradrenaline in central and sympathetic nervous systems. As a major peripheral vascular contractive neurotransmitter, through interactions with its receptors, neuropeptide Y has been implicated in the pathology and progression of diabetes, by promoting the proliferation of endothelial cells and vascular fibrosis, which may contribute to diabetes-induced cardiovascular disease. Neuropeptide Y also participates in the pathogenesis of atherosclerosis, the major form of cardiovascular disease, via aggravating endothelial dysfunction, growth of vascular smooth muscle cells, formation of foam cells and platelets aggregation. This review highlights the causal role of neuropeptide Y and its receptor system in the development of diabetes mellitus and one of its complications: atherosclerotic cardiovascular disease. The information from this review provides both critical insights onto the mechanisms underlying the pathogenesis of atherosclerosis and evidence for the development of therapeutic strategies.
Introduction
Treatment of diabetes-induced atherosclerotic cardiovascular disease (CVD) represents a big challenge for clinicians. So far, the mechanisms by which diabetes causes atherosclerosis and subsequent CVD remain to be fully understood and great effects have been put into this aspect. Many factors have been indicated to contribute to the aetiology of this process, and recent studies have found that neuropeptide Y (NPY), a neurotransmitter co-stored and co-released with sympathetic nerve in the peripheral nervous system, plays an important role in the regulation of glucose metabolism and the development of atherosclerosis via modulating peripheral vascular function. 1 Being overweight or obese is the major risk factor accounting for 80%–90% of patients with diabetes. 2 Recent research has uncovered the critical functions of the NPY system in obesity. Hypothalamic NPY has been implicated in control of appetite and energy balance. 1 Meanwhile, the level of NPY in central and peripheral altered in some pathological conditions. For example, increased level of peripheral NPY not only causes dysregulation in glucose metabolism, insulin resistance (IR) and abnormal lipolysis but also promotes abnormal proliferation of vascular smooth muscle cells (VSMCs) in heart and enhances function of macrophage and platelets.3–6 As all these factors are involved in developing diabetic complications including atherosclerosis, this review will summarize the latest researches on the role of NPY in the development of diabetes mellitus (DM)-induced atherosclerotic CVD.
NPY and receptors
Distribution and biological actions of NPY
NPY, a 36-amino acid peptide, was first isolated from porcine brain by Tatemoto and colleagues in 1982, and it belongs to the NPY family, which also comprises the structurally similar peptide YY and pancreatic polypeptide. 7 NPY is synthesized within the endoplasmic reticulum of NPY neurons and mostly stored in the dense core of large vesicles through axonal transport. NPY is widely distributed in central and peripheral nervous system and is one of the most abundantly expressed neuropeptides in the brain. 8 In central, NPY is expressed in the hypothalamus, cerebral cortex and brainstem, with highest concentration found in the hypothalamic arcuate nucleus (ARC), where it has direct access to circulating hormones, such as insulin, leptin and ghrelin, due to a semi-permeable blood brain barrier. In fact, there are two main neuronal populations regulating energy homeostasis in the ARC: one is orexigenic NPY/agouti-related peptide (AgRP) neurons and the otheris anorexigenic proopiomelanocortin/cocaine- and amphetamine-related transcript (POMC/CART) neurons.1,9,10 NPY neurons in the hypothalamic ARC then project to second-order neurons within the hypothalamus including the paraventricular nucleus, the ventromedial nucleus and the lateral hypothalamus9,11,12 to modulate food intake and energy balance. 13 It has been therefore well recognized that the NPY system plays a critical role in the regulation of energy homeostasis and the pathophysiology of obesity. In the periphery, NPY is primarily co-stored and co-released with noradrenaline in the sympathetic postganglionic neurons and adrenal medulla-chromaffin cells. 14 In addition, NPY is also found in platelets and adipose tissue.15–18 Since sympathetic nervous system has a significant role in the aetiology of cardiac disease, there is emerging evidence implicating central and peripheral NPY in the development of cardiac disease and atherosclerosis.19,20
NPY receptor and its signing pathways
NPY exerts its biological effects via at least five G-protein-coupled receptors: Y1, Y2, Y4, Y5 and Y6,11,21 with various distribution in central and peripheral nervous system. In general, NPY inhibits adenylate cyclase through NPY receptors coupled to the Gi/oG proteins, leading to reduced cyclic adenosine monophosphate (cAMP) levels in target cells. 22 Inaddition, Y receptors such as the Y1 receptor are reported to bind to different G protein subunits and activate various mitogen-activated protein kinase cascades. 23 These NPY downstream signing pathways are correlated with the occurrence and development of metabolic and CVDs.
NPY and DM
NPY in the development of obesity
Obesity is a major risk factor for diabetes, which is closely related to atherosclerosis. Numerous studies have shown that NPY regulates the development of obesity through the central and peripheral nervous system.24,25 In the hypothalamic ARC, increased NPY neurons directly inhibited POMC neurons either by direct activation of Y receptors or via tonic release of gamma-aminobutyric acid (GABA), leading to increased food intake. 1 In addition, activating NPY neurons in the ARC resulted in decreased energy expenditure. 26 Previous study showed that dorsomedial hypothalamus (DMH) NPY knockdown in rats led to development of brown adipocytes in inguinal white adipose tissue (WAT) via the sympathetic nervous system, which increased brown adipose tissue (BAT) activity. 27 Our previous study 26 demonstrated that ARC-derived NPY played a key role in the control of sympathetic outflow and BAT function. ARC NPY signalling inhibited sympathetically innervated BAT thermogenesis, involving the downregulation of uncoupling protein 1 (UCP1) expression in BAT. In addition, NPY also acts through the autonomic nervous system to control insulin secretion and activity, thus contributing to the pathophysiology of obesity and diabetes.28,29 Moreover, it is worth noting that noradrenergic NPY, co-localized with noradrenaline in the same neurons of the brainstem or sympathetic nervous system,30,31 takes part in energy metabolism in response to long-term stress.32–34 Recent studies of OE-NPYDβH mouse models overexpressing noradrenergic NPY showed that NPY in noradrenergic neurons indeed contributed to the development of stress-induced obesity accompanied with impaired glucose metabolism and IR.35,36 Taken together, both central and peripheral NPY are crucial for the development of obesity and adiposity.
The role of NPY in control of insulin secretion
There is evidence demonstrating that NPY plays an important role in modulating insulin secretion. Earlier studies showed that NPY treatment markedly inhibited glucose-stimulated insulin secretion in isolated isletsof mouse and promoted beta-cell replication via theactivation of extracellular signal–regulated kinasecascades,37,38 and deletion of NPY gene specifically in islet cells caused the increase of insulin secretion. 39 In contrast, in vivo experiments, the intracerebroventricular (ICV) microinjection of NPY in wild-type mice significantly increased circulating insulin level 30 min post-treatment. As for indirect effect of NPY on insulin secretion, overexpression of NPY in mice leads to hyperinsulinemia and impaired glucose tolerance in addition to hyperphagia and marked body weight gain.40,41 Besides, previous studies reported that reduced blood glucose level in peripheral blood was able to activate partial NPY neurons to increase feeding behaviours.42,43 Furthermore, fat-produced leptin is also involved in the regulation of serum insulin level and glucose metabolism via hypothalamic NPY. 44 Therefore, the data strongly suggest that the direct action of NPY on pancreatic islets ex vivo insulin release is inhibitory, while the central action of NPY indirectly leads to an increase in plasma insulin. In view of the effects of NPY on central stimulating feeding and drinking behaviour in the rat,45,46 it is reasonable that NPY induced delayed and transient increase of circulating insulin. The inhibitory action of NPY on insulin secretion is thought to be mediated by the Y1 receptor on islet β cells. 38 Disruption of NPY system leads to dysregulated energy balance and a cluster of metabolic syndrome including hyperinsulinemia, hyperglycaemia and fat accrual. 47
NPY neurons are involved in DM
Since obesity, insulin level and diabetes are interrelated, NPY has been suggested to be directly or indirectly involved in the regulation of the occurrence and development of diabetes. A recent study has shown that increased NPY expression in the arcuate and dorsomedial nuclei induces hepatic IR which is believed to be mediated by Y1 receptor in the hypothalamus. NPY had also an effect on glucose metabolism by downregulating cell phosphatidylinositol 3-kinase (PI3K) and glycogen synthase kinase-3 phosphorylation of adipose cells. 48 It has been confirmed by Torekov et al. 49 and Campbell et al. 50 that the Y2 receptor mutation of human was one of the predisposing factors in type 2 diabetes mellitus (T2DM). Furthermore, by comparing coronary artery bypass surgery patients with diabetic and non-diabetic, Ejaz et al. 51 reported that the genes and protein expression of Y2 and Y5 receptor significantly decreased in diabetic patients, and it could result in neuropeptide systems anomaly, which may lead to diabetes autonomic neuropathy and cardiovascular complication. Therefore, it is no doubt that NPY may significantly promote the occurrence and development of diabetes and atherosclerosis.
Diabetes and atherosclerosis
Coronary atherosclerotic heart disease, also called as coronary heart disease (CHD), is a lipid-driven inflammation disease characterized by endothelial dysfunction and plaque deposition in vessel wall. 52 Diabetes has long been recognized to be an independent risk factor for CHD in addition to obesity, smoking, hypertension and gout. Studies have shown that the incidence of CHD in patients with diabetes is two to four times higher than in patients without diabetes.53,54 Atherosclerosis is the cause of a majority of CHD events and accelerated by diabetes and metabolic syndrome. Diabetes-induced atherosclerosis is closely related to high blood sugar as well as IR.
Hyperglycaemia and atherosclerosis
Hyperglycaemia is a major risk factor for microvascular complications and could lead to metabolic disorders, IR, pancreatic β cell damage, impaired glucose tolerance and ultimately induce diabetes. Keeping glycemic under control can effectively reduce the risk of DM atherosclerotic CVDs.6,55,56 Furthermore, United Kingdom Prospective Diabetes Study showed that patients with T2DM choosing sulfonylurea or insulin to control blood sugar level could significantly reduce the risk of myocardial diseases compared with other therapies such as conventional therapy and intensive therapy with metformin. 57 Chronic hyperglycaemia also causes the proliferation of VSMCs, chronic inflammation and the advanced glycation end products (AGEs) increasing, which accelerate atherosclerosis development.58–60
Studies show that hyperglycaemia could cause dysregulated nitric oxide (NO) bioavailability and unbalanced accumulation of reactive oxygen species (ROS), leading to endothelial dysfunction,61,62 which elucidated that hyperglycaemia was implicated in abnormal vascular contraction in CVD conditions.
Insulin resistance and atherosclerosis
IR is a prominent feature of T2DM, 63 and it is an important risk factor for inducing atherosclerosis in patients with diabetes even in the absence of hyperglycaemia. 64 In addition to muscle, the liver, adipose tissue and pancreas, 65 interestingly, insulin receptors are also found in vascular endothelial cells, suggesting a role of insulin in the regulation of proliferation and function of vascular endothelial cells. When under physiological conditions, insulin inhibits thrombosis by reducing the levels of tissue thromboplastin and plasminogen activator inhibitor 1, which subsequently prevents occurrence of arteriosclerotic lesions and plaque.66,67 It is also evidenced that IR in patients with obesity can cause platelet activation and thromboxane increased. Interestingly, it has been demonstrated that T2DM patients with obesity have significantly elevated inflammatory factors and free fatty acids (FFA) in circulation which could activate inflammatory pathways by binding to Toll-like receptors (TLRs).68,69 Activation of TLRs inhibits phosphorylation of insulin receptor substrate (IRS), leading to the suppression of PI3K/Akt signalling and decreases glucose transporter 4 (GLUT4) expression, ultimately causing IR.70,71 Together, these studies suggest that abnormal insulin signalling which is exacerbated by obesity due to enhanced inflammation promotes the occurrence and development of atherosclerosis.
NPY and diabetes-induced atherosclerotic CVD
DM-associated CVD is a major healthcare issue. Diabetes increases the risk of CVD and associated mortality, and patients with diabetes often display a faster progressionof atherosclerosis.72–74 Hyperglycaemia and hyperinsulinemia are important clinical indicators of diabetes, which are also implicated in the development of atherosclerosis. Abnormally, elevated NPY, centrally or peripherally, is closely associated with the pathophysiology of metabolic syndrome including hyperglycaemia and hyperlipidemia.75,76 Therefore, NPY may also be involved in the development of diabetes-induced atherosclerotic heart disease.
The effect of central NPY on atherosclerosis
Elevated NPY level in the hypothalamic Arc leads to defects characteristic of obesity, including hyperphagia and significant body weight gain, hyperinsulinemia and hyperleptinemia via Y1/Y2/Y5 receptors.12,77 It has also been proven that NPY promoted and aggravated hyperglycaemia in a DMH NPY knockdown rat models. 78 Hyperglycaemia not only damages the structure of blood vessels but also causes the changes in the protein function and increase in inflammatory factor, which accelerate the process atherosclerosis. Increased AGEs induced by hyperglycaemia spread out of the cell, modified circulating proteins and then bound to AGE cell receptors. This binding prompted the production of inflammatory cytokines, causing vascular injury. 79 It is worth noting that dysregulated NO bioavailability and unbalanced accumulation of ROS induced by hyperglycaemia have been reported to cause endothelial dysfunction. For one thing, Maritim et al. 61 reported that reduced NO bioavailability is a key change for endothelial damage, and ROS is an important link between blood sugar and diabetic vascular complications. 62 It is known that increased plasma fatty acid concentration is responsible for impaired insulin signalling in skeletal muscle, and this is associated with reduced NO synthesis in muscle due to downregulated endothelial NO enzyme. Therefore, NO endothelial dysfunction could accelerate atherosclerotic lesion formation. In addition, hyperglycaemia-induced excessive ROS can stimulate the release of a variety of vascular inflammation–related factors such as glycosylation end products (AGEs), protein kinase C (PKC) and nuclear factor-kB (NF-kB).80,81 It has demonstrated thatPKC is the upstream signal molecule in the regulation of vascular homeostasis. For instance, activation of PKC in DM enhanced vascular contractility. 82 Notably, there was increased PKC expression and activity in vascular disease and in certain forms of hypertension. Targeting of vascular PKC using PKC inhibitors may reduce vascular smooth muscle (VSM) hyperactivity. 83 For another, endothelial cell dysfunction involving the selective recruitment of cytokines and circulating monocytes from the blood into the intima resulted in an atherosclerotic lesion, which led to multiple factors acting on neighbouring VSMCs to induce the formation of plaque. 84 Additionally, central NPY systems are also very important in the regulation of vascular function. For instance, NPY binding with Y1 receptor can mediate vasoconstriction and stimulate the proliferation of smooth muscle cells by enhancing the norepinephrine (NE).7,85 Thus, central NPY is deeply interrelated to hyperglycaemia-induced atherosclerotic plaque and the NPY receptor subtypes are involved in the occurrence and development of atherosclerosis in different stages.
The effect of periphery NPY on atherosclerosis
In recent years, the researches of the effect of NPY and its receptors in adipose tissue have achieved great success by gene knock-out technology. 86 Stress-induced exacerbation of diet-induced obesity mice resulted in gross abdominal obesity, liver and skeletal muscle steatosis, whereas germline NPY2R−/−mice was resistant to these symptoms. 76 Moreover, Baker et al. 87 have confirmed that the NPY-Y2 receptor in adipose tissue and endothelial cells can promote the growth of adipose tissue. The activated Y2 receptors in the endothelial cell and adipose cells also facilitate the growth of pre-adipocytes. 7 Additionally, NPY systems are very important in the regulation of vascular function. For instance, NPY binding with Y1 receptor can mediate vasoconstriction and stimulate the proliferation of smooth muscle cells by enhancing the NE.7,85 Importantly, obesity was observed in OE-NPYDβH mouse models that overexpressed noradrenergic NPY. On one hand, the obesity was not caused by hyperphagia, but lipogenic effects of noradrenergic NPY directly induce fat accumulation in WAT and liver. On the other hand, in OE-NPYDβH mouse models, the inhibition of sympathoadrenal activity took place in the brainstem as well with decreased thermogenesis, lipolysis and light-time locomotor activity. It is well known that atherosclerosis is a process of interaction between vascular regeneration and thrombosis. 7 Disruption of NPY systems would induce hyperinsulinemia and ultimately leads to compensative IR. Rask-Madsen et al. 88 found that the mice with knocked-out defective insulin signalling pathway in endothelial cell displayed apparent endothelial dysfunction and induced expression of adhesion molecules as well as atherosclerotic lesions. Moreover, IR has been suggested to be correlated with dysregulation of vascular cell adhesion molecule-1 and NO in arterial ECs, leading to defective vasodilation and increased entry of inflammatory cells into the plaque. In advanced plaques, IR promoted apoptosis of VSMCs and macrophages, which resulted in plaque necrosis. Then, these perturbations precipitated plaque rupture and acute thrombotic vascular occlusion. 89 Likewise, if NPY was administered to the injured carotid artery, macrophages and foam cells were markedly increased, leading to significantly enlarged plaque lesions. Besides, the increase of NPY expression was observed in unstable human endarterectomy plaques during atherogenesis. For example, synergistic effects of Y2 and Y5 receptors on the endothelial cells stimulate their proliferation, migration and the formation of capillary which ultimately increase the atherosclerotic plaque formation.15,87,90 Furthermore, plaque development and murine mast cell activation were promoted by perivascular overexpression of NPY. 91 NPY not only changes the vascular structures in pathological condition 92 but also plays a role in platelet–vascular interactions. In physiological state, NPY level is rather low in platelets; however, in the case ofvascular injury, the expression of NPY in platelets is significantly increased, suggesting a role of NPY in platelet activation, platelet adhesion, aggregation and thrombosis during vascular injuries.91,93
In summary, NPY plays a crucial role in regulating the energy homeostasis centrally and peripherally. In the brain, NPY directly controls feeding behaviour and energy balance via multiple hormonal and neuronal pathways; it affects WAT and BAT metabolism viasympathetic neuronal pathway, which may lead to obesity in T2DM patients. These disturbances elevate the FFA level in circulation. The increased FFA binds to the TLRs and activates the inflammatory pathway, which promotes FFA-induced IR and influences some vascular inflammation–related factors (AGEs, PKC and NF-kB). IR is a prominent feature of T2DM. Moreover, central NPY modulates insulin secretion and subsequent blood glucose level. The abnormal insulin signalling promotes the occurrence and development of atherosclerosis. In periphery, NPY is expressed in tissues such as the liver, adipose tissue and platelets, which participatesin inflammation, lipid metabolism, cell migration, platelet function and so on. These perturbationspathologically induce the atherosclerosis. In the noradrenergic neurons of the brainstem and sympatheticnervous system, overexpressing noradrenergic NPY contributed to the development of stress-inducedobesity accompanied with impaired glucose metabolism and IR, notably IR was associated with coronary plaque vulnerability which exacerbated the progress of atherosclerosis. 94 Therefore, NPY can regulate or involve in diabetes-related atherosclerotic angiocardiopathy via different pathways. Here, in Figure 1, we summarize the mechanisms by which NPY participates in the diabetes-induced atherosclerotic angiocardiopathy.
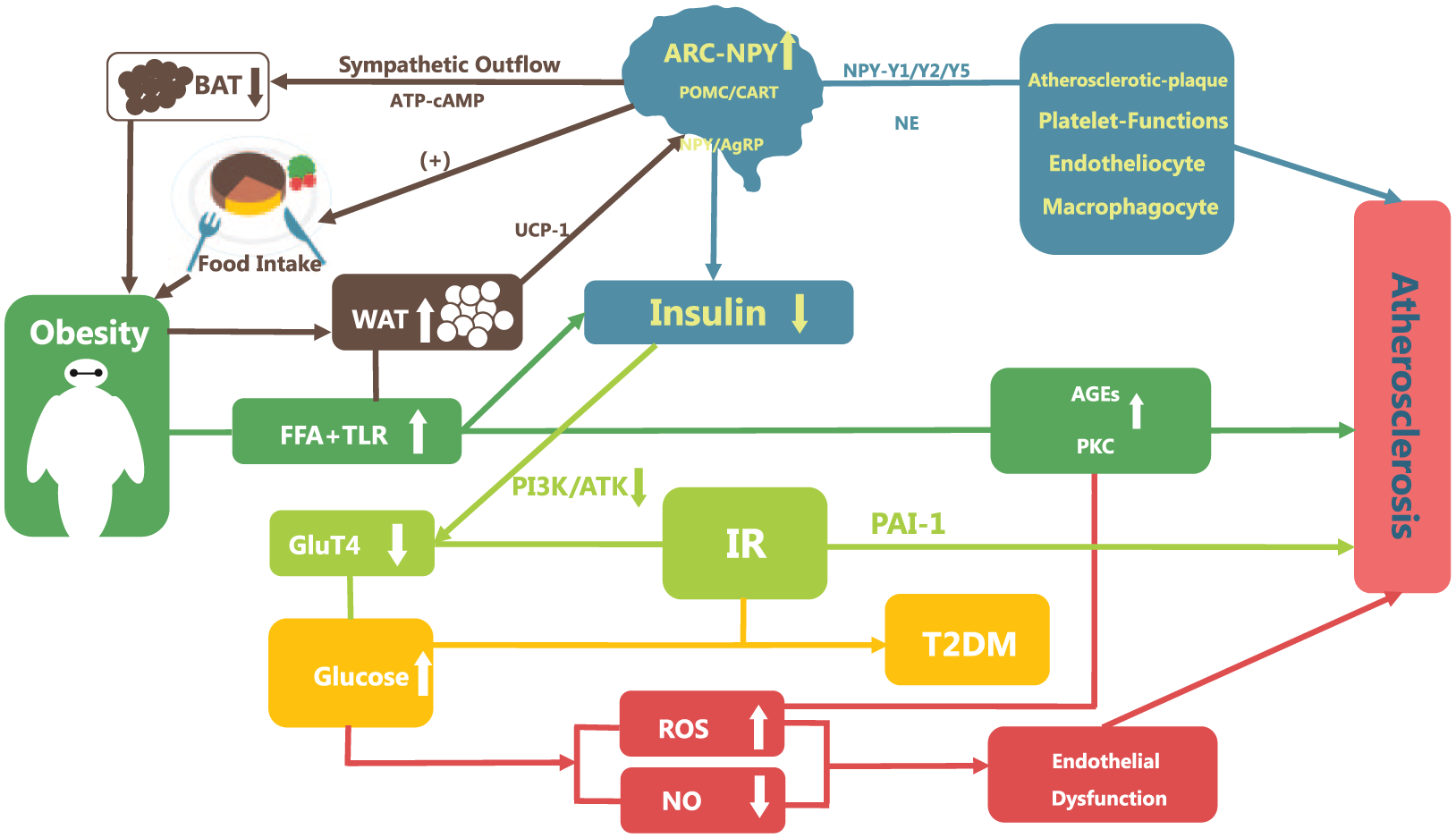
The mechanisms by which NPY participates in the diabetes-induced atherosclerotic angiocardiopathy. In the hypothalamic ARC, anorexigenic POMC/CART and orexigenic NPY/AgRP neurons are two main neuronal populations that regulate energy homeostasis. Increased NPY neurons directly inhibited POMC neurons either by direct activation of Y receptors or via tonic release of GABA, leading to increased food intake. In addition, activating ARC NPY signalling inhibited sympathetically innervated BAT thermogenesis and could promote WAT to store energy. Besides, NPY acts through the autonomic nervous system to control insulin secretion, and disruption of this hypothalamic signalling pathway contributes to the pathophysiology of obesity and diabetes. Diabetes has long been recognized to be an independent risk factor for atherosclerosis, and diabetes-induced atherosclerosis is closely related to high blood sugar as well as IR. Hyperglycaemia causes endothelial dysfunction via dysregulated NO bioavailability and unbalanced accumulation of ROS, ultimately leading atherosclerosis. Elevated NPY level in the hypothalamic is also involved in mechanisms underpinning the atherosclerosis, including abnormal proliferation of VSMCs, atherosclerotic plaque formation and endothelial dysfunction.
Concluding remarks and future perspectives
NPY is widely distributed centrally and peripherally and plays an important role in regulating glucose metabolism, energy metabolism and vascular function. In vivo and in vitro, studies have found that NPY is involved in the pathophysiology of T2DM and can affect the cardiovascular complications of diabetes, but its pathogenesis is still not clear. In contrast to great effort in investigating the role of NPY in obesity and diabetes, not many studies have explored the effects of NPY in the regulation of atherosclerosis and CVD. On one hand, the complex mechanism is still need more experimental research to verify, and, on the other hand, lack of human trials leads to limitation of its clinical application. There is no doubt that combining experimental and clinical research for NPY is imperative. Moreover, NPY also has become an increasingly attractive new therapeutic target, which opens up new avenues for the prevention and treatment of diabetes and CVD.
Key messages
Role of NPY system in the development of DMs and CVD;
Relationship between risk factors with NPY in central and peripheral nervous system;
Mechanisms that NPY involved in the glucose metabolism and energy expenditure.
Footnotes
Acknowledgements
Z.-y.S. and S.L. contributed equally to this work. All authors contributed substantially to study conception and design, drafting the article or revising it critically. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.