
Abstract
Purpose:
The purposes of this study were to compare the presence, extent and composition of coronary plaques in asymptomatic patients with newly diagnosed type 2 diabetes to age- and sex-matched controls.
Methods:
Patients with newly diagnosed (<1 year) type 2 diabetes (n = 44) and controls (n = 44) underwent contrast-enhanced coronary computed tomography angiography. Advanced plaque analysis including total plaque volume and volumes of plaque components (calcified plaque and non-calcified plaque, including low-attenuation [low-density non-calcified plaque]) was performed using validated semi-automated software.
Results:
Coronary artery calcification was more often seen in patients with type 2 diabetes (66%) versus controls (48%), p < 0.05. Both the absolute volume (median; interquartile range) of low-density non-calcified plaque (7.9 mm3; 0–50.5 mm3 vs 0; 0–34.3 mm3, p < 0.05) and the increase in low-density non-calcified plaque ratio in relation to total plaque volume (τ = 0.5, p < 0.001) were significantly higher in patients with type 2 diabetes. More patients with type 2 diabetes had spotty calcification (31% vs 0%, p < 0.05). By multivariate analysis, the presence of any low-density non-calcified plaque was higher in males (odds ratio: 4.06, p < 0.05), who also demonstrated a larger low-density non-calcified plaque volume (p < 0.001). The presence and extent of low-density non-calcified plaque increased with age, smoking, hypertension and hyperglycaemia, all p < 0.05.
Conclusion:
Asymptomatic patients with newly diagnosed type 2 diabetes had plaque features associated with increased vulnerability as compared with age- and sex-matched controls.
Introduction
Coronary artery disease is a major cause of morbidity and mortality in the industrial world.1,2 Several studies have shown a relationship between type 2 diabetes (T2D), an increased risk of coronary artery disease and a poor long-term prognosis,3,4 findings that have been strengthened by studies demonstrating advanced cardiovascular involvement even in asymptomatic patients with T2D.5,6 However, the available information on coronary artery disease in patients with T2D relies on studies of diabetes populations with either long diabetes duration5,7 or known cardiovascular disease.8,9 The literature regarding coronary artery disease and coronary plaque morphology in patients with newly diagnosed T2D is sparse.10,11
Contrast-enhanced coronary computed tomography angiography (CCTA) has evolved as a robust imaging modality for ruling out significant coronary artery disease.12,13 Moreover, CCTA permits detailed non-invasive coronary plaque assessment.14,15
The purposes of this study were to evaluate the presence, extent and composition of coronary plaques in asymptomatic patients with newly diagnosed (<1 year) T2D and to compare these findings with age- and sex-matched controls.
Methods
Patients with T2D
From March 2014 to August 2016, a total of 213 adult patients diagnosed with T2D (haemoglobin A1c > 47 mmol/mol and plasma glucose > 7 mmol/L) within the last year were identified via general practitioners or outpatient clinics in the Region of Southern Denmark and invited by letter to participate in the study. A total of 115 (54%) patients agreed to participate. Patients were systematically evaluated by questionnaires and examination for symptoms of or known cardiovascular disease (defined as previous myocardial infarction, angina pectoris, stroke/transient ischaemic attack and/or peripheral atherosclerosis), in which case they were excluded from the study. Two patients with cardiovascular disease were excluded. Patients with pregnancy or inability to provide informed consent were also excluded. Patients with the following characteristics were excluded from the study: renal insufficiency (estimated glomerular filtration rate < 45 mL/min or serum creatinine > 140 micromole/L), body mass index (BMI) > 35 kg/m2, absence of sinus rhythm, contraindications to iodinated contrast agents and inability to perform a 10-s breath hold. 16
Control group
In total, 72 controls were recruited from the general population by advertisement in the local press. Controls were systematically evaluated by questionnaires and examination for cardiovascular disease (criteria consistent with those described for patients with T2D) and T2D (undiagnosed T2D in this group was excluded by fasting plasma glucose and by an oral glucose tolerance test) were excluded. Seven controls with cardiovascular disease were excluded. In addition, exclusion criteria were consistent with those described for patients with T2D. Only 52 of controls met the inclusion criteria and underwent CCTA.
Matching
Patients with T2D were matched 1:1 by age (±<1 year) and sex, giving a total of 44 persons in each group. Figure 1 summarizes the selection of study populations.
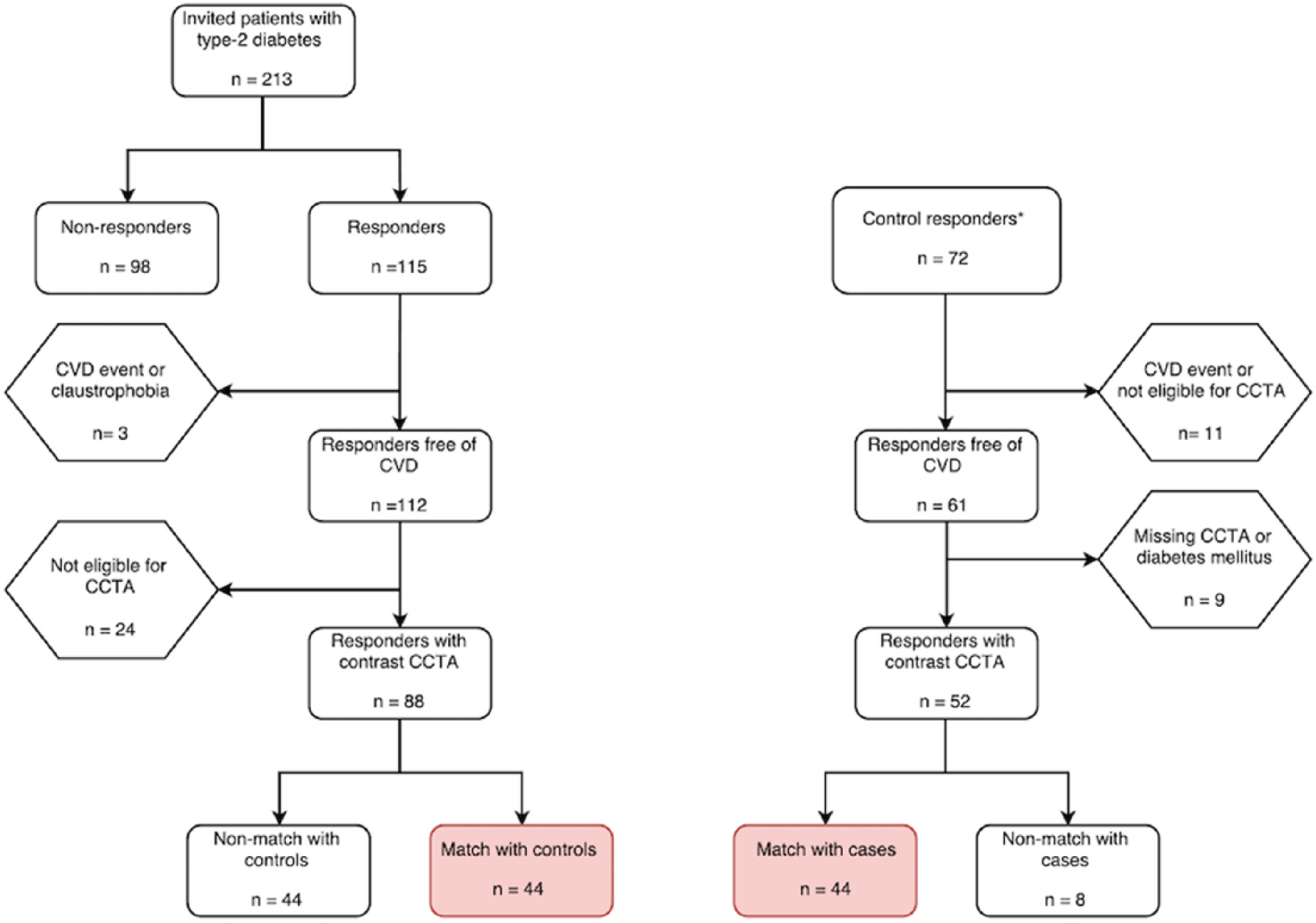
Flow diagram of the study populations (for further information, see text).
Ethical considerations
The scientific protocols were approved by the Regional Scientific Ethical Committee for Southern Denmark (S-20140137 and S-1-10-72-349-13) and by the Danish Data Protection Agency (2008-58-0035 and 1-16-02-505-13) and were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all individual participants included in the study. The study is registered at ClinicalTrials.gov ID: NCT03022344 and protocol ID: 44110.
Demographic data
Medical history, current medications and smoking habits were obtained from questionnaires. Height, weight and waist–hip ratio were measured. Venous blood samples were taken under fasting conditions and were analysed for low-density lipoprotein, high-density lipoprotein, triglycerides, total cholesterol, haemoglobin A1c, fasting glucose, C-reactive protein and creatinine. Glomerular filtration rate was estimated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula. 17
Morning midstream urine samples were examined for urine albumin/creatinine ratio. Brachial blood pressures were measured by oscillometric techniques over 24 h, using TM-2430 (A&D Co., Ltd, Saitama, Japan). 18 Blood pressures were defined as mean values of the 24-h recordings. Hypertension was defined as blood pressures ≥140/90 mm Hg or treatment with at least one antihypertensive agent. Hypercholesterolaemia was defined as total cholesterol ≥5 mmol/L or low-density lipoprotein ≥3 mmol/L or treatment with at least one lipid-lowering agent. Abdominal obesity was defined as a waist–hip ratio above 0.90 for males and above 0.85 for females, or a BMI above 30.0 kg/m2.
Cardiac computed tomography
Acquisition
Image acquisition was performed in accordance with guidelines defined by the Society of Cardiovascular Computed Tomography. 19 Both patients with T2D and controls underwent CCTA (Siemens SOMATOM Definition Flash, Forcheim, Germany). Pre-scan oral and/or intravenous beta-receptor blockers were administrated, targeting a heart rate ≤60 beats/min. Sublingual nitroglycerine, dose of 0.5 mg, was administrated immediately before the scanning. Contrast-enhanced CCTA (Optiray™ 350 mgI/mL [Mallinckrodt]) was undertaken using the following settings: gantry rotation time 280 ms, 2 mm × 64 mm × 0.6 mm collimation, 100 or 120-kV tube voltage (depending on body geometry). A reference mAs of 320 with automatic tube current modulation was employed. Scans were prospective step and shoot, gated 65%–75% of the R-R interval. Images were reconstructed at 65%, 70% and 75% of the R-R interval, using iterative reconstruction (SAFIRE level 3) and kernel B31 (medium–smooth). Slice thickness was 0.6 mm with 0.3-mm interval. Both patients with T2D and controls underwent a standard non-contrast scan, with a reference mAs of 50 for assessment of coronary artery calcifications (CACs) by the Agatston score. 16
Data analyses
Reconstructed CCTA images were transferred to a workstation, syngo.via (Siemens Healthcare) for post processing. One experienced computed tomography (CT)-cardiologist, blinded to the clinical data, analysed all CCTA data.
Images were deemed non-evaluable if artefacts affected ≥3 coronary segments. A modified 17-segment model was used for allocation of plaques to a distinct vessel territory. 20 All coronary plaques were evaluated by visual assessment according to the following indicative criteria for coronary artery disease: non-obstructive (1%–29% stenosis), borderline (30%–69% stenosis), obstructive (70%–99% stenosis) and occlusive (100%) plaque. Images of the best phase of the cardiac cycle for visualization of coronary arteries were transferred to a research workstation for plaque assessment. CAC were quantified by non-contrast CCTA and were assessed by summing up the scores from all foci in the coronary arteries, expressed in Agatston units (U), using dedicated software (syngo Calcium Scoring, Siemens Healthcare).
Plaque quantification
Coronary segments >2 mm with plaques (tissue structures >1 mm2)21,22 were analysed by one trained reader using a validated semi-automated software (AutoPlaque, version 2.0, Cedars-Sinai Medical Center, Los Angeles, CA, USA).14,15,21 CCTA images were examined in multiplanar reformats, and a circular region of interest (normal reference blood pool) was placed in the aorta. Scan-specific thresholds for non-calcified plaque (NCP) and calcified plaque (CP) volumes were automatically generated. 15 Adjustments were made if necessary. Coronary plaque burden was defined as (plaque volume/vessel volume) × 100%. Remodelling index was calculated as maximum lesion vessel area/area of a proximal normal reference point. 23 Low-density non-calcified plaque (LD-NCP) was defined as a plaque with components attenuation <30 Hounsfield units. 23 The part of the NCP that was not classified as LD-NCP was defined as the non-low-density non-calcified plaque (non-LD-NCP). All coronary plaques were categorized as belonging to one of the three vessel territories. The left main was considered part of either left anterior descending artery or left circumflex artery. 22 The analyses were performed by one experienced reader, who was blinded to all other patient data.
Intra-observer variability
The intra-observer variation for the assessment of plaque components were evaluated in 16 patients (8 patients with T2D and 8 controls) with an Agatston score > 0. Studies were re-analysed 3–4 weeks after the initial evaluation by the same reader.
Statistical analysis
The design of the study was a matched case-control study in which each patient with T2D was matched to a control by age (±<1 year) and sex. Sample size estimations were performed for comparison of LD-NCP between patients with T2D and controls. From previous studies, the standard deviation (SD) on LD-NCP was known to be approximately 25 mm3. 22 With a beta = 0.2 and an alpha = 0.05, it was calculated that 44 patients in each group were needed to obtain the required strength of the study.
Shapiro–Wilk test was used for testing the normal distribution of data. Continuous variables were presented as mean values and 95% confidence interval if normally distributed or median and interquartile ranges (IQRs) if non-normally distributed. Differences in baseline demographics between patients with T2D and controls (group-wise differences) were determined using paired t-test for normally distributed variables and Wilcoxon signed-rank test for non-normally distributed variables. Categorical variables were presented by frequencies and corresponding percentages.
LD-NCP data were characterized by a point mass at zero followed by a highly skewed continuous distribution, that’s why a two-part model was chosen for the regression analyses to evaluate the association with the independent variables. First, a logistic regression model was used to determine the association between covariates and the presence or absence of LD-NCP. Second, the association between covariates and the extent of LD-NCP volumes among participants with LD-NCP was determined by a generalized linear model with the gamma distribution using link-name identity. In the model, the following covariates were included: age, sex, BMI, hypertension, hypercholesterolaemia, smoking (ever smoker vs non-smokers) and haemoglobin A1c.
Differences in proportions between matched pairs were analysed by McNemar’s test. Kruskal–Wallis test and Kendall’s rank correlation were used to evaluate associations between plaque components and total plaque volume tertiles. Intra-observer variability of plaque characteristics was analysed using the paired t-test.
A p-value <0.05 was considered statistically significant. All statistical analyses were performed using Stata software, version 14.0 (StataCorp LLC, College Station, TX, USA).
Results
Clinical characteristics
Clinical characteristics are presented in Table 1. Patients with newly diagnosed T2D were more often treated with 2 or more antihypertensive (30% vs 16%, p < 0.05) or cholesterol-lowering (52% vs 18%, p < 0.05) drugs compared to controls. Among patients with T2D, 6% received both oral medication and insulin therapy, 76% were treated with oral medication only and 18% had diet-controlled diabetes. Additionally, patients with newly diagnosed T2D had lower low-density lipoprotein, high-density lipoprotein and total cholesterol. Mean haemoglobin A1c was 45 mmol/mol, which is within the normal range (<47 mmol/mol).
Clinical characteristics of the study populations.
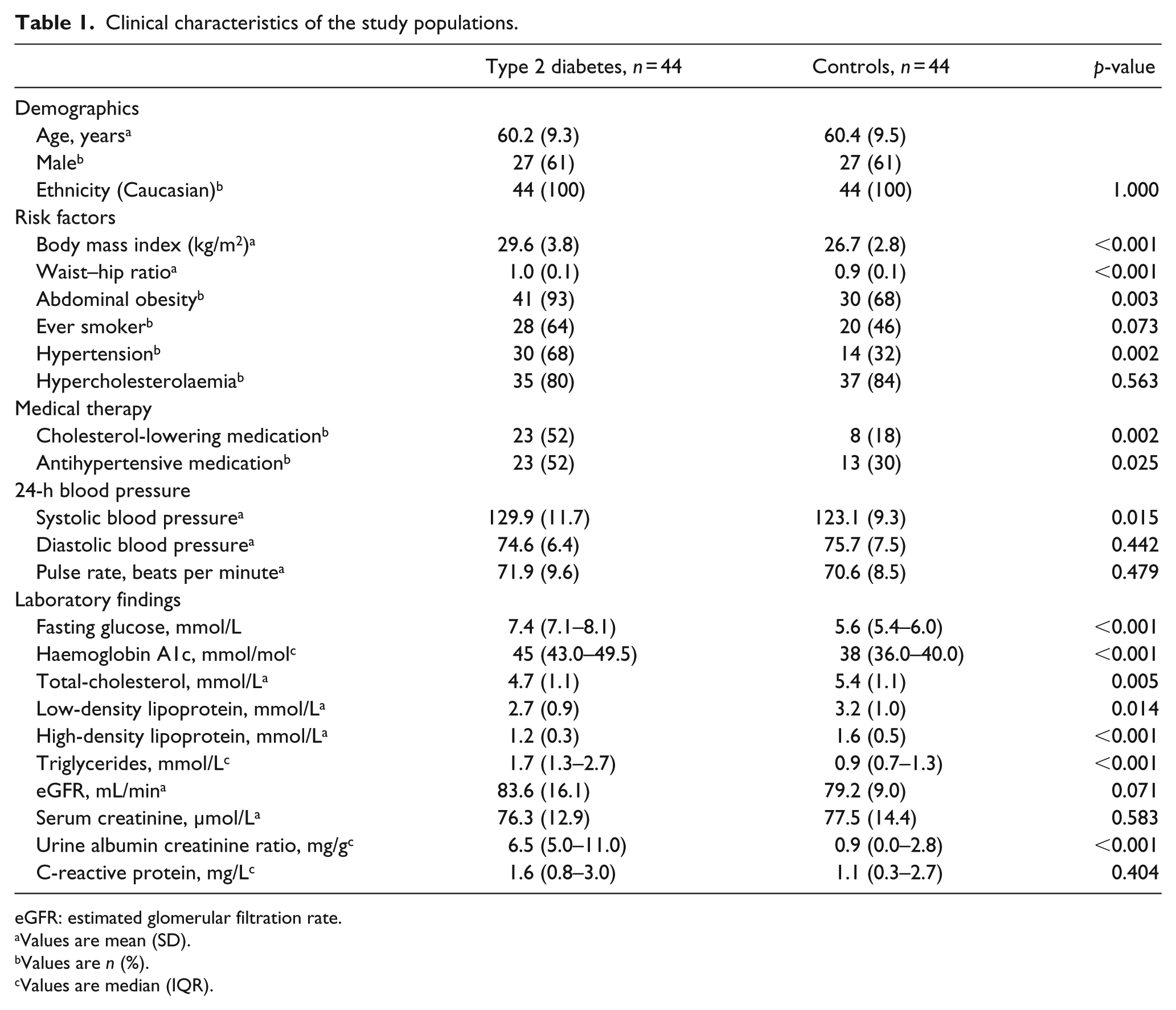
eGFR: estimated glomerular filtration rate.
Values are mean (SD).
Values are n (%).
Values are median (IQR).
Contrast-enhanced CCTA and plaque analysis
There was no difference in heart rate (median; IQR) during CCTA between patients with T2D and controls (60 beats/min; 54–63 beats/min vs 59 beats/min; 54–63 beats/min, p = 0.98). Significantly higher radiation doses (median; IQR) were applied in patients with T2D (435 mGy cm; 308–497 mGy cm) versus controls (238 mGy cm; 210–289 mGy cm), p < 0.001. The numbers of patients receiving 120 keV were equal in patients with T2D (n = 37) and controls (n = 36), p = 0.32.
CAC was identified in 29 (66%) patients with T2D versus 21 (48%) in controls, p < 0.05, Table 2. The Agatston score was significantly higher in patients with T2D, p < 0.05. Overall, we registered 174 segments with plaques in 50 participants, of which 96 (56%) were found in patients with T2D. The prevalence of coronary obstruction (≥70% stenosis) was 9.1% in patients with T2D versus 6.8% in controls, p = 0.50. No plaques were found in neither patients nor controls with an Agatston score of zero.
Assessment of coronary artery disease and plaque composition.
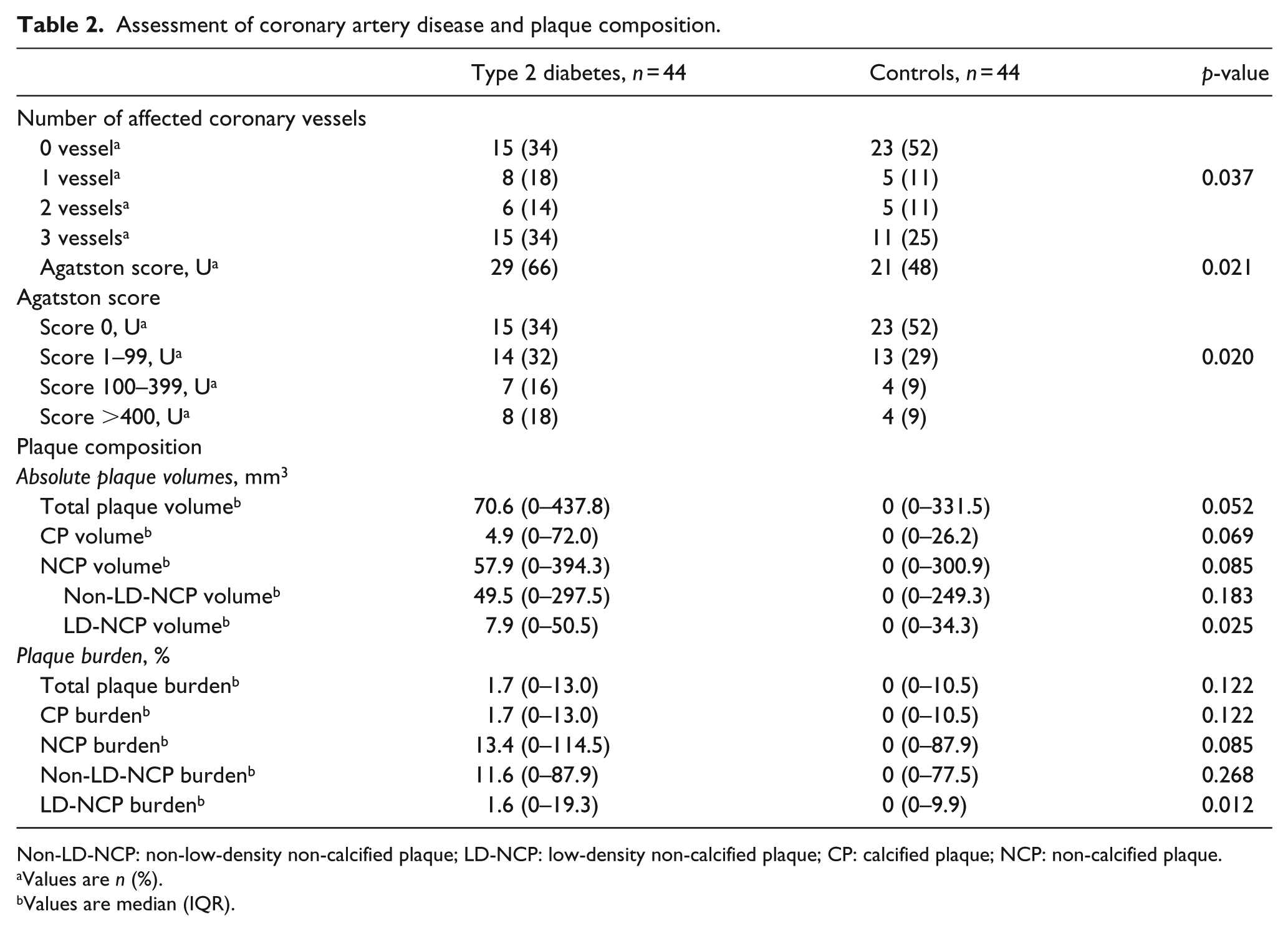
Non-LD-NCP: non-low-density non-calcified plaque; LD-NCP: low-density non-calcified plaque; CP: calcified plaque; NCP: non-calcified plaque.
Values are n (%).
Values are median (IQR).
The assessment of coronary plaque composition is illustrated in Table 2. The LD-NCP volume was significantly higher in patients with T2D compared to controls, whereas total plaque volume, CP and NCP volumes were non-significantly higher in patients with T2D. Furthermore, the LD-NCP plaque burden was significantly higher in patients with T2D compared to controls, and more patients with T2D versus controls had spotty calcification (31% vs 0%, p < 0.05), while the remodelling index (median; IQR) was similar in the two groups (1.5; 1.5–2.0 vs 1.5; 1.4–1.6, p = 0.16). The association between the ratio of plaque components and total plaque volume tertiles in patients with T2D and controls is shown in Figure 2. The LD-NCP ratio increased with higher total plaque volume in patients with T2D (τ = 0.5, p < 0.005) but not in controls. There were no differences in BMI and radiation doses between tertiles of plaque volumes, neither in patients with T2D nor in controls.
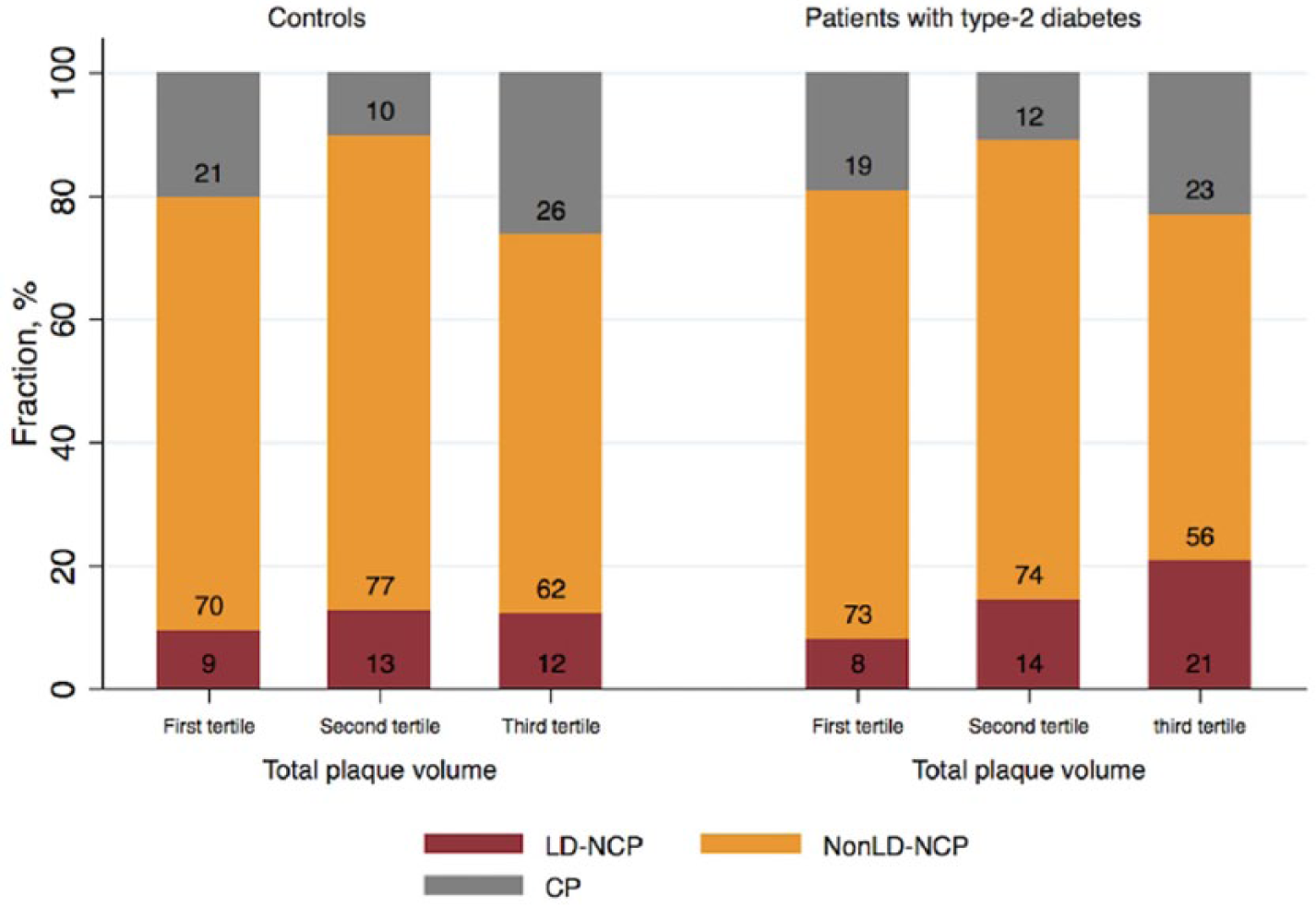
Ratio of coronary plaque components in relation to total plaque volume.
Multivariate analyses for the entire population are presented in Table 3. Men had a higher risk for the presence of any LD-NCP (odds ratio [OR]: 4.06, p < 0.05) and demonstrated a larger LD-NCP volume than women (p < 0.001). BMI was positively associated with the occurrence of any LD-NCP, while the inverse correlation was found between BMI and LD-NCP volumes. The presence and extent of LD-NCP increased with age, smoking, hypertension and the degree of hyperglycaemia.
Association between LD-NCP and cardiac risk factors – multivariate analysis.
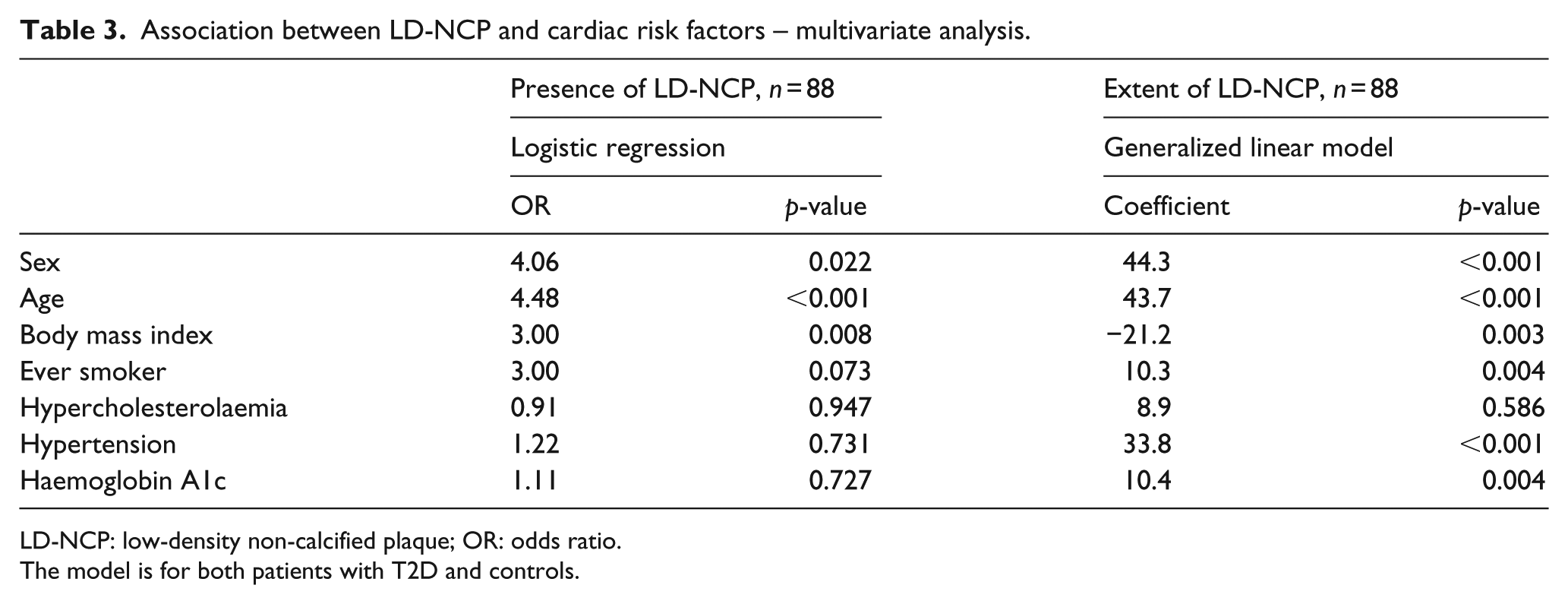
LD-NCP: low-density non-calcified plaque; OR: odds ratio.
The model is for both patients with T2D and controls.
A good intra-observer agreement on all of the applied plaque analysis components was found. No significant differences in mean NCP (mean difference: 7.4 mm3, p = 0.88), CP (mean difference: 0.76 mm3, p = 0.91) or LD-NCP volumes (mean difference: 0.22 mm3, p = 0.85) were observed.
Discussion
In this study, we evaluated the differences in the presence, extent and composition of coronary plaques between asymptomatic patients with newly diagnosed T2D and sex- and age-matched controls. The major finding of this study is related to the differences in the LD-NCP component between patients with T2D and controls both in absolute and relative terms. Our findings are consistent with previous reports that patients with T2DM have a higher atherosclerotic burden3,24,25 compared to populations without T2D,9,26,27 but this study extends previous observations by demonstrating that patients with T2D have a greater proportion of LD-NCP and more often spotty calcifications, indicating a vulnerable coronary plaque composition in patients with T2D already at the time of diagnosis. However, due to the limited number of patients in this observational study, it could not be proved which of the known cardiovascular risk factors contributed the most to the observed adverse coronary plaque structure in patients with newly diagnosed T2D.
In this study, we found that asymptomatic patients with a new diagnosis of T2D have a higher extent of CAC compared to controls. These findings are in accordance with the results of a study comparing CAC in healthy individuals and asymptomatic patients with T2D. 28 However, in the latter study, patients had longer diabetes duration than in the current.
Although well validated, it should be acknowledged that the Agatston score is a semi-quantitative metric and only represents the CP component. The ability of contrast-enhanced CCTA to discriminate between different plaque components has been validated by comparison to intravascular ultrasound. 29 An intravascular ultrasound-based study by Amano et al. 30 reported a more lipid-rich coronary plaque content in patients with acute coronary syndromes and abnormal glucose tolerance. These lipid-rich plaque contents might correspond to the findings of previous autopsy studies, in which the prevalence of necrotic cores and inflammatory cells in coronary plaques among patients with T2D was high.31,32 Such plaques may be more vulnerable to rupture and as a consequence may be related to a higher cardiovascular event rate. Moreover, these lipid-rich portions of coronary plaques might be identical to parts of the NCP described by CCTA, especially the low-density NCP. Indeed, recent studies report that the LD-NCP component is an important determinator of acute coronary syndromes33,34 and that coronary lesions with high LD-NCP content more frequently are associated with lesion-specific ischaemia compared to lesions without these adverse characteristics. 22 A CCTA-based study by Nakanishi et al. 35 supplements these results, demonstrating that symptomatic patients with diabetes have progressively increasing NCP components compared to patients without diabetes. Importantly, they showed that larger NCP volumes at baseline are associated with progression in the LD-NCP volumes. In line with the study by Nakanishi et al., 35 we found that the degree of hyperglycaemia was independently associated with LD-NCP volumes.
As the structure of plaques are complex, the accurate mechanism of coronary plaque progression have not yet been proved but may be dependent on plaque composition, cardiovascular risk profile and level of inflammatory activation.10,36–38 Lehman et al. 38 found that the differences in the rate of progression are dependent on plaque composition and that this progression may be greater for NCP compared with CP.
Coronary plaque composition has primarily been evaluated in T2D populations with long duration of T2D5,7 or in patients with T2D with symptoms of suspected or known coronary artery disease.8,9 This study adds knowledge by indicating a more fragile coronary atherosclerotic plaque structure even in the early stages of T2D. This study is too small for evaluating any independent effects of the parameters in the metabolic syndrome on plaque vulnerability, but at the time of diagnosis, asymptomatic patients with T2D are likely to have more advanced stages of coronary plaques due to the often long and silent pre-diagnostic stages of this disease.
The findings in this exploratory study have to be confirmed in larger trials that might promote further insight into plaque morphology and thereby help designing more effective treatment strategies in patients with T2D. Asymptomatic patients with newly diagnosed T2D often have atypical or no symptoms at all, even in the presence of disease. Knowing that asymptomatic patients with T2D may have more vulnerable plaque already at diagnosis, a more aggressive treatment algorithm or screening for coronary artery disease might be considered at an early stage.
Limitations
The number of patients in this study was small. As only 54% of the invited patients with T2D agreed to participate, we cannot exclude some degree of bias. In patients with T2D, a significantly higher radiation dose was applied. It is well known39,40 that the interaction of different tissue structures with X-ray beams at different energies can create artefacts such as blooming, which might disturb exact volume-measurements of the distinct plaque components. However, in the lower plaque volume tertile, we found no differences in plaque composition between patients with T2D and controls despite differences in radiation doses. In addition, significant differences in plaque composition between tertiles of plaque volumes were found in patients with T2D despite identical radiation doses. Therefore, the findings in this study unlikely were affected by artefacts relating to the applied radiation dose.39,40 In addition, it should be emphasized that plaque analyses were performed using a scan-adaptive plaque threshold algorithm.
In conclusion, this study indicates that asymptomatic patients with newly diagnosed T2D have a high burden of coronary atherosclerosis and that coronary plaque composition in these patients displays features associated with an increased vulnerability. Several of the traditional risk factors for coronary artery disease were present already at the time of diagnosis of T2D, but the contribution of each of these factors for the observed adverse plaque composition in asymptomatic patients newly diagnosed T2D could not be further elucidated.
Footnotes
Acknowledgements
M.M. designed the study, collected, analysed and interpreted the data and wrote the report. M.M. analysed all coronary computed tomography angiography (CCTA) using AutoPlaque and did Agatston investigation; K.L.F. collected the control group and edited the manuscript; S.G. and K.A.Ø. trained M.M. in AutoPlaque and edited the manuscript. D.D. developed the analysis tool and reviewed the manuscript. M.W.K. performed CCTA data and edited the manuscript; B.L.N. contributed to the discussion and reviewed the manuscript; J.B.G. and J.G. designed the study and edited the manuscript; M.H.O. conceived and designed the study and edited the manuscript; N.P.R.S. conceived and designed the study, collected, analysed data and contributed to the discussion and reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The Danish Diabetes Academy supported by the Novo Nordisk Foundation; The Faculty of Health Sciences, University of Southern Denmark; Department of Regional Health Research, Center Southwest, Denmark; Edith and Vagn Hedegaard Jensens Foundation, Karola Jørgensens Foundation and Sydvestjysk Cardiologisk Forskningsfund. The funders had no role in the study design, data collection, data analysis and interpretation, writing of the report or the decision to submit the article for publication.