
Abstract
Purpose:
To determine the occurrence of physiological significant coronary artery disease (CAD) by coronary CT angiography (CTA) derived fractional flow reserve (FFRCT) in asymptomatic patients with a new diagnosis (<1 year) of type-2 diabetes mellitus (T2DM).
Methods:
FFRCT-analysis was performed from standard acquired coronary CTA data sets. The per-patient minimum distal FFRCT-value (d-FFRCT) in coronary vessels (diameter ⩾1.8 mm) was registered. The threshold for categorizing FFRCT-analysis as abnormal was a d-FFRCT ⩽0.75. Total plaque volume and volumes of calcified plaque, non-calcified plaque, and low-density non-calcified plaque (LD-NCP) were assessed by quantitative plaque analysis.
Results:
Overall, 76 patients; age, mean (SD): 56 (11) years; males, n (%): 49(65), were studied. A total of 57% of patients had plaques. The d-FFRCT was ⩽0.75 in 12 (16%) patients. The d-FFRCT, median (IQR), was 0.84 (0.79–0.87). Median (range) d-FFRCT in patients with d-FFRCT ⩽0.75 was 0.70 (0.6–0.74). Patients with d-FFRCT⩽0.75 versus d-FFRCT >0.75 had numerically higher plaque volumes for all plaques components, although only significant for the LD-NCP component.
Conclusion:
Every sixth asymptomatic patient with a new diagnosis of T2DM has hemodynamic significant CAD as evaluated by FFRCT. Flow impairment by FFRCT was associated with coronary plaque characteristics.
Keywords
Introduction
Coronary computed tomography angiography (CTA) is recommended as a first line non-invasive test in patients suspected of coronary artery disease (CAD).1,2 Beyond assessment of diameter stenosis, coronary CTA enables detailed analysis of the burden, and characteristics of coronary plaques. 3 Specific plaque properties such as low-density and positive remodeling are associated with an unfavorable clinical outcome, 4 and it has been demonstrated that adverse plaque features independently of stenosis severity are associated to impaired coronary flow.5–8 Recently, coronary CTA derived fractional flow reserve (FFRCT) has emerged for non-invasive physiological evaluation of CAD 9 before referral to invasive assessment in patients with stable angina pectoris. When validated against invasive FFR,10–12 the reference standard for decision-making on coronary revascularization,1,13 FFRCT demonstrated high diagnostic performance. Moreover, FFRCT has revealed an enhanced diagnostic sensitivity compared to stress perfusion imaging by single photon emission computerized tomography 14 and cardiac magnetic resonance. 15 FFRCT testing may change the downstream management of patients,16,17 and recently, it was demonstrated that the numerical value of FFRCT is an independent predictor of outcomes.18–20
The prevalence of CAD is high both at early 21 and advanced phases of type-2 diabetes mellitus (T2DM). 22 A strategy of identifying asymptomatic persons who may benefit from preventive medication has been debated for years. 23 In one prospective randomized study however, screening with traditional coronary CTA failed to demonstrate any incremental prognostic gain in T2DM. 24 To the best of our knowledge, no previous study has assessed the hemodynamic significance of CAD in patients with newly diagnosed T2DM.
Consequently, this exploratory study sought to determine the occurrence of physiological significant coronary stenosis by FFRCT and to relate these estimates with coronary plaque characteristics in asymptomatic patients with newly diagnosed T2DM.
Materials and methods
From March 2014 to August 2016, a total of 213 adult individuals diagnosed with T2DM (hemoglobinA1c >47 mmol/mol and plasma glucose >7 mmol/L) within the last year were identified via general practitioners or outpatient clinics in Region South of Denmark, and invited by letter to participate in this study. A detailed description of patient cohort exclusions criteria and demographic data have been published previously. 21
This post-hoc study was approved by the Regional Scientific Ethical Committee for Southern Denmark (S- 20140137) and by the Danish data Protection Agency (2008-58-0035), and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all the participants. The study was registered at ClinicalTrials.gov ID: NCT03022344 and protocol ID: 44110.
Coronary CT angiography
A detailed description of the applied CT acquisition protocol and plaque analysis strategy has been published previously. 21 In brief, all participants underwent coronary CTA by using a dual-source scanner (SOMATOM Definition Flash; Siemens Healthcare, Forcheim, Germany). Pre-scan oral beta-blockers were administered targeting a heart rate of ⩽60 beats/min. Sublingual nitroglycerin, dose of 0.5 mg, was administered 2 to 4 min before the scan. An initial non-contrast enhanced scan for calcium scoring was performed. One experienced CT cardiologist (more than 10 years of experience in coronary CTA interpretation), blinded to all clinical data, analyzed the CT datasets. Vessels >2 mm in diameter were evaluated and graded visually as follows: normal (0%), non-obstructive stenosis (1–29%), intermediate stenosis (30–69%), obstructive stenosis (⩾70%). Location of stenosis was reported using a 17-segment model. 12
One trained reader performed plaque analysis using a validated semi-automated software program (AutoPlaque, version 2.0, Cedars-Sinai Medical Center, Los Angeles, CA, USA).3,25 Total plaque volume and the volumes of calcified plaque (CP), non-calcified plaque (NCP) and low-density NCP (LD-NCP) were assessed. Coronary plaque volumes and characteristics were assessed on a per-patient and a per-vessel basis. All plaque analyses were performed by staff blinded to FFRCT-results and other patient data. 21
Medical treatment was not affected by the results of coronary CTA or FFRCT as these were not available for the treating physicians.
FFRCT
Standard acquired coronary CTA data sets were transmitted for central FFRCT analysis (HeartFlow Inc., Redwood City, California). 12 The principles behind FFRCT computation have previously been described in detail. 9 FFRCT was displayed for each point in the coronary tree. Any FFRCT-value in the major coronary arteries ⩾1.8 mm in diameter, including side branches, was registered.
The per-patient minimum distal FFRCT-value (d-FFRCT) was registered. A d-FFRCT-value ⩽0.75 was indicative of impaired flow.26,27
Follow-up
Electronic patient journals were used to register major adverse outcomes (all-cause mortality, myocardial infarction and stroke) at follow-up, 4 to 6 years after the initial coronary CTA.
Statistical analysis
Continuous variables are presented as mean values and 95% confidence intervals if normally distributed or median and interquartile range (IQR) if non-normally distributed. Categorical variables are presented as frequencies (n) and percentages. Q-plot was used for testing whether the data were normal distributed. Differences in plaques composition between d-FFRCT ⩽0.75 versus d-FFRCT >0.75 were tested using the Wilcoxon rank-sum test. A p-value <0.05 was considered statistically significant. All statistical analyses were performed using Stata software, version 14.0 (StataCorp LLC, College Station, TX, USA).
Results
In total, 115 (54%) patients agreed to participate in this study of whom FFRCT-analysis was available in 76 patients, Figure 1. Clinical characteristics are presented in Table 1. Stenosis severity according to vessel location (n,%) was as follows: normal (n = 150): left anterior descending artery (LAD), 44 (29%); left circumflex artery (CX), 55 (37%); right coronary artery (RCA), 51 (34%); non-obstructive stenosis (n = 69): LAD, 29 (42%); CX, 17 (25%); RCA, 23 (33%); intermediate stenosis (n = 4): LAD, 1 (25%); CX, 2 (50%); RCA, 1 (25%) and obstructive stenosis (n = 5): LAD, 2 (40%); CX, 2 (40%); RCA, 1 (20%). Mean (SD) heart rate was 59 (7) beats/min and median (IQR) radiation dose was 6.0 (4.7–6.9) mSv.
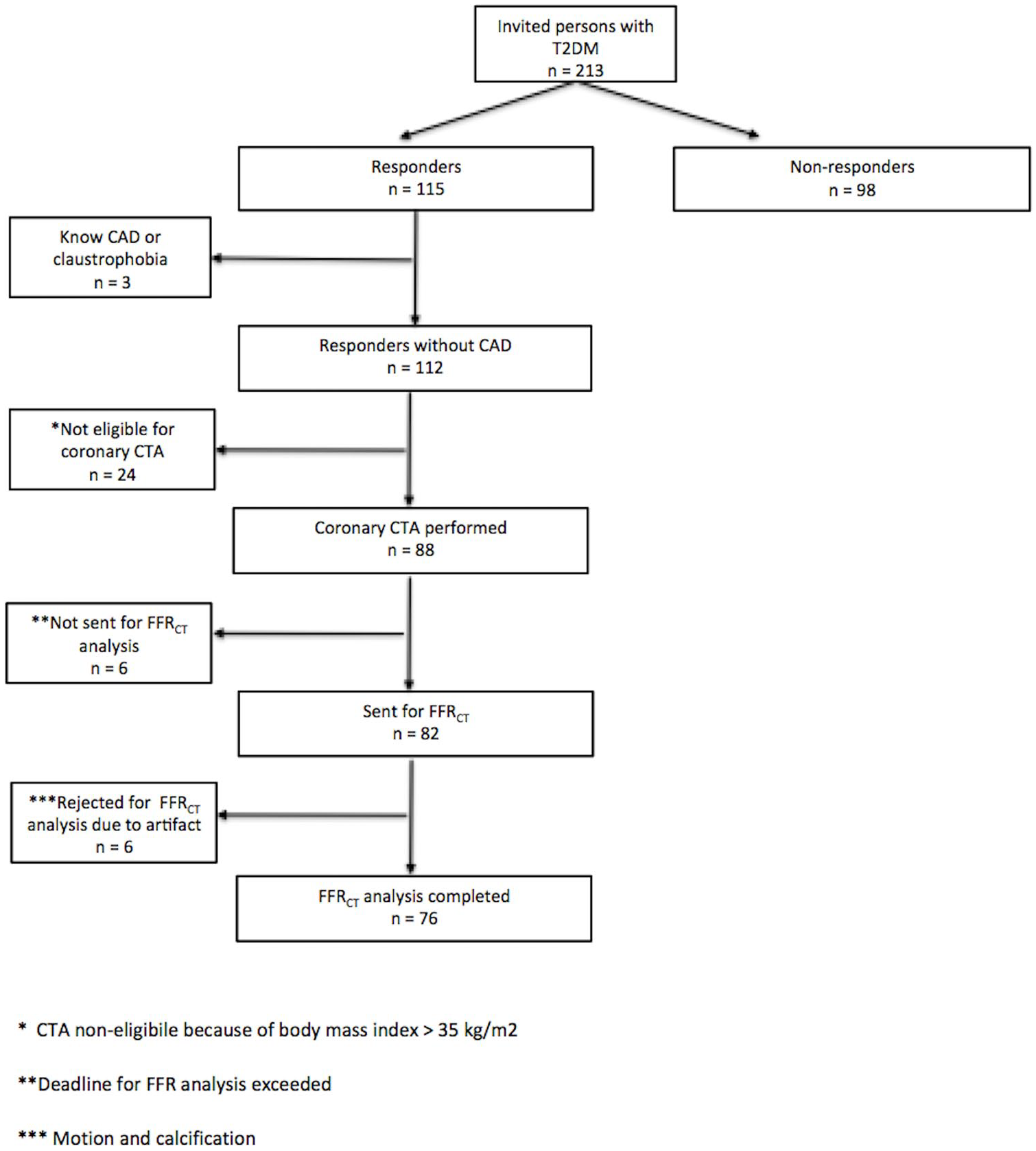
Flow diagram.
Clinical characteristics.
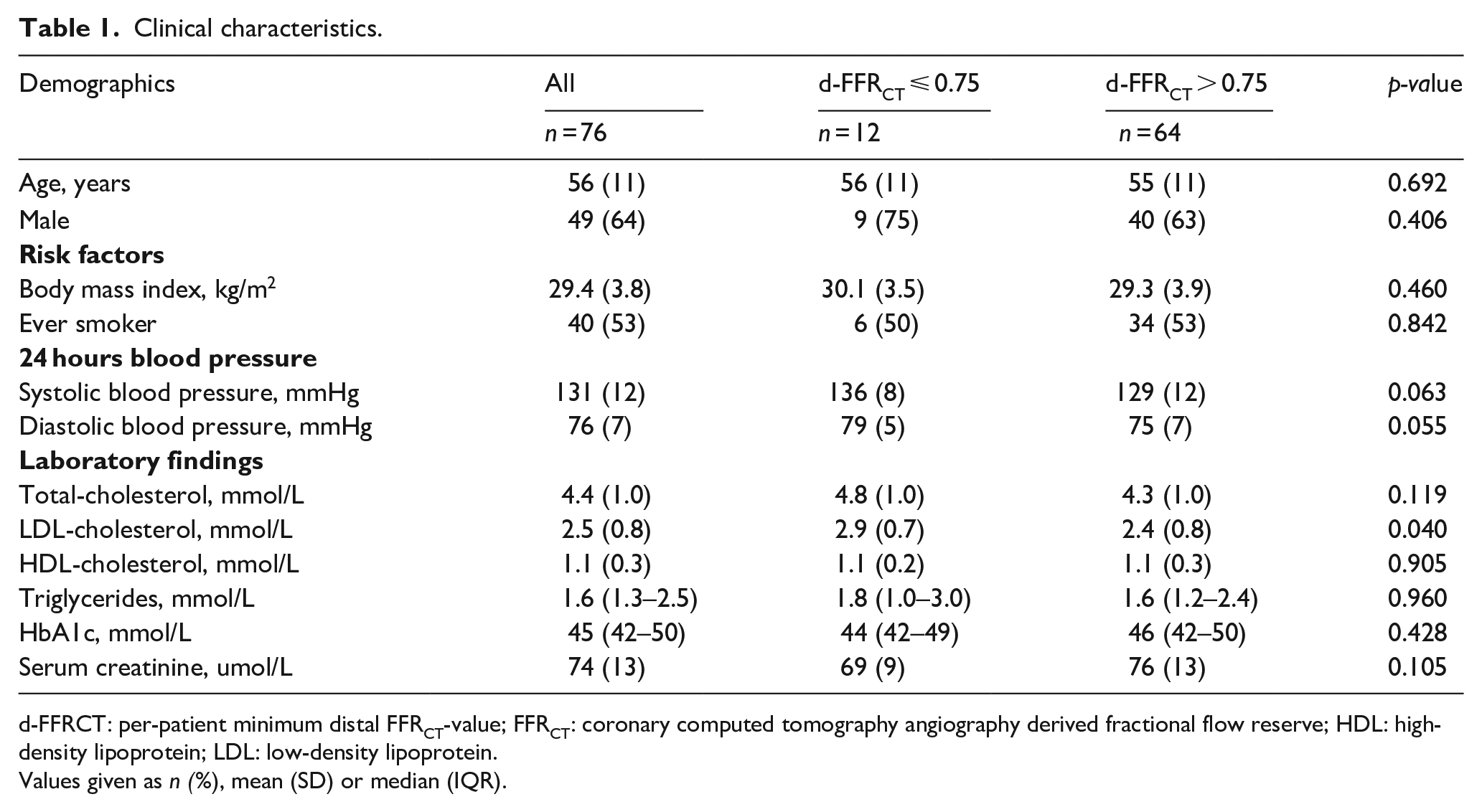
d-FFRCT: per-patient minimum distal FFRCT-value; FFRCT: coronary computed tomography angiography derived fractional flow reserve; HDL: high-density lipoprotein; LDL: low-density lipoprotein.
Values given as n (%), mean (SD) or median (IQR).
FFRCT: Plaque relationship
A total of 43 (57%) patients had plaques. Median (IQR) Agatston score was 1 (0–110) U. Thirty-five (46%) patients had an Agatston score of zero. The d-FFRCT, median (IQR), was 0.84 (0.79–0.87). d-FFRCT was ⩽0.75 in 12 (16%) patients. Median (range) d-FFRCT in patients with d-FFRCT ⩽ 0.75 was 0.70 (0.6–0.74). Patients with d-FFRCT ⩽ 0.75 versus d-FFRCT > 0.75 had higher LDL-cholesterol, while no differences between groups regarding BMI, gender, age, smoking habits, blood pressures or HbA1c were observed, Table 1. Patients with d-FFRCT ⩽ 0.75 versus d-FFRCT > 0.75 had numerically higher plaque volumes for all plaque components, however the difference was statistical significance only for the LD-NCP component, Table 2.
Patient-specific coronary plaque volumes according to the per-patient minimum distal FFRCT-value in asymptomatic patients with early stage T2DM.
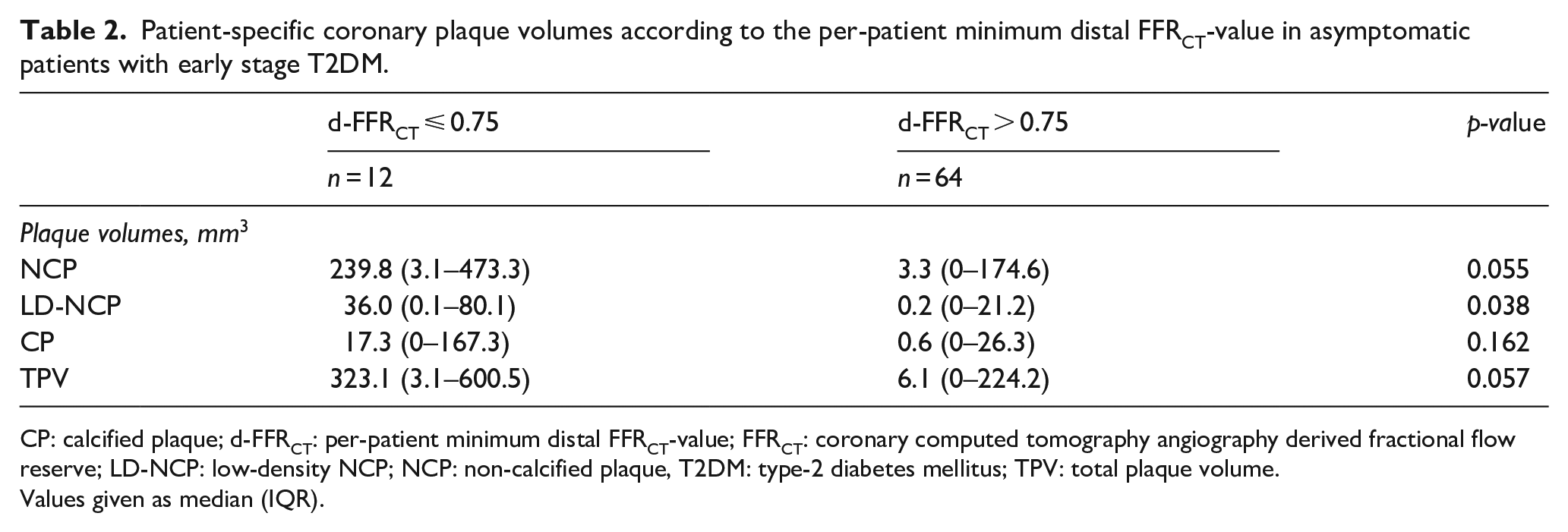
CP: calcified plaque; d-FFRCT: per-patient minimum distal FFRCT-value; FFRCT: coronary computed tomography angiography derived fractional flow reserve; LD-NCP: low-density NCP; NCP: non-calcified plaque, T2DM: type-2 diabetes mellitus; TPV: total plaque volume.
Values given as median (IQR).
Follow-up
Follow-up, mean (SD), was performed 4.8 (0.5) years after the index coronary CTA. One patient died due to alcoholic liver cirrhosis (index coronary CTA: Agatston Score, 36 U; non-obstructive CAD; d-FFRCT, 0.91) one had a stroke (index coronary CTA: Agatston Score, 109 U; non-obstructive CAD; d-FFRCT, 0.88) and one patient suffered a myocardial infarction (index coronary CTA: Agatston Score, 1150 U; double-vessel CAD; d-FFRCT, 0.51), Figure 2. For details on stenosis location and – severity and coronary plaque volumes, see supplemental material.
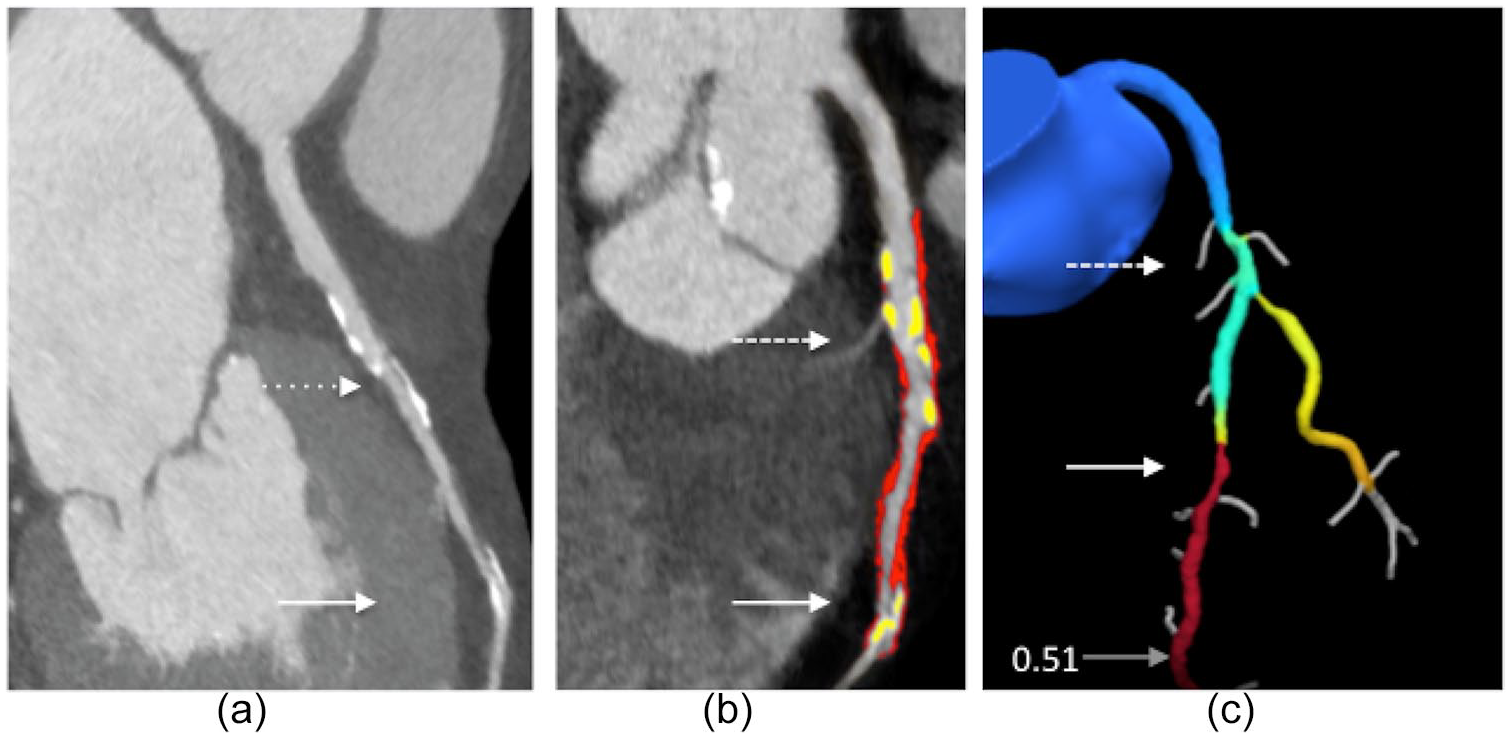
Illustration of corresponding coronary CTA, quantitative plaque analysis and FFRCT.
Discussion
The present study confirms that patients with T2DM have a high burden of CAD already at an early stage of the disease process and demonstrates that every sixth asymptomatic patient with a new diagnosis of T2DM has hemodynamic significant CAD as evaluated by FFRCT.
This study provides new knowledge by showing that high-risk coronary features such as coronary flow impairment by FFRCT and adverse plaque characteristics by coronary CTA are frequent in asymptomatic patients with a new diagnosis of T2DM.
Although well-established, coronary CTA is restricted to describe morphological aspects of the atherosclerotic disease process, which has been the basis for evolvement of second-line non-invasive physiological assessment by FFRCT-based metrics. The d-FFRCT represents the sum of resistances related to both focal and diffuse atherosclerotic disease along the coronary vessel and thus may be positive even in the absence of focal stenosis and studies in symptomatic populations have demonstrated that adverse plaque characteristics are associated to the presence of coronary pressure loss.5–8 The present study adds to these findings by demonstrating similar associations in asymptomatic individuals with newly diagnosed T2DM. Of note, a d-FFRCT ⩽0.75 was associated with higher LD-NCP volumes and higher LDL-cholesterol levels. LD-NCP is considered a surrogate for lipid core plaques, 28 and has been associated to unfavorable outcomes. 4 Several imaging and histopathological studies have demonstrated more profound macrophage infiltration and larger necrotic core of coronary plaques in patients with T2DM compared to patients without diabetes.29–31 In addition, an abnormal glucose regulation is an important risk factor for coronary plaque progression and is associated with lipid-rich plaques in patients with T2DM compared to non-diabetic subjects.29,32 High levels of LDL-cholesterol is a well-known risk factor for cardiovascular events and is associated with the presence of high risk coronary plaques. 33 Otaki et al. 34 showed that a decrease in LDL-cholesterol is associated with plaque stabilization including a decrease in all components of NCP determined by coronary CTA. Whether LDL lowering can lead to recovery of abnormal flow is at the moment unresolved. However, the observed association between LDL-cholesterol levels and coronary flow impairment in this study and the long-term improvement of invasive fractional flow reserve following LDL lowering by rosuvastatin in a small series of patients with CAD in a small study Hashikata et al. 35 are supportive of this hypothesis.
It is well established that conventional clinical risk factors independently predict the development of CAD in T2DM,36,37 and that multifactorial prevention strategies for late complications are associated with lower rates of micro- and macro-vascular disease.38,39 The present study adds to these findings by demonstrating that a number of asymptomatic patients with T2DM, already at the time of diagnosis, have adverse coronary plaque characteristics with hemodynamic significance.
Information on the occurrence of morphological and physiological adverse plaque characteristics may be of value in identifying high risk patients with asymptomatic T2DM in whom intensive treatment with, for example, proprotein-konvertase-subtilisin/kexin-type 9 inhibitors, glucagon like peptide-1 receptor agonists or sodium-glucose cotransporter-2 inhibitors may be considered. These issues need delineation in future studies.
Limitations
The number of participants in the study was small. Both duration of cholesterol-lowering and antihypertensive medication and changes in cholesterol- and blood pressure levels may have had an impact on coronary flow impairment and plaque phenotype, which could not be accounted for in this study, as these data were not available.
Quantitative assessment of plaque volumes is dependent on several conditions. Recent studies indicated that changes in delineation of plaque boundaries and in discriminative Hounsfield levels improved the correlation between plaque volumes determined by intravascular ultrasound and CT angiography.40,41
Conclusion
In asymptomatic patients with a new diagnosis of T2DM, coronary flow impairment by FFRCT is frequently seen and is associated to quantitative estimates of coronary plaque components. Studies are needed to assess the value of performing coronary CTA and selective FFRCT for therapeutic management decisions in these patients.
Supplemental Material
Supplementary_File – Supplemental material for Coronary flow impairment in asymptomatic patients with early stage type-2 diabetes: Detection by FFRCT
Supplemental material, Supplementary_File for Coronary flow impairment in asymptomatic patients with early stage type-2 diabetes: Detection by FFRCT by Monija Mrgan, Bjarne Linde Nørgaard, Damini Dey, Jørgen Gram, Michael Hecht Olsen, Jeppe Gram and Niels Peter Rønnow Sand in Diabetes & Vascular Disease Research
Footnotes
Author contributions
MM: designed the study, collected, analyzed and interpreted the data and wrote the report. MM analyzed all CCTA using Autoplaque, did Agatston investigation and FFR analysis; DD: developed the analysis tool and reviewed the manuscript. BN: contributed to the discussion and reviewed the manuscript, JG and JG: designed the study, and edited the manuscript, MHO: conceived and designed the study and edited the manuscript, NPS: conceived and designed the study, collected, analyzed data and contributed to the discussion and reviewed the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Danish Diabetes Academy supported by the Novo Nordisk Foundation; The Faculty of Health Sciences-University of Southern Denmark; Department of Regional Health Research-Center Southwest, Denmark; Edith and Vagn Hedegaard Jensens Foundation, Karola Jørgensens Foundation and Sydvestjysk Cardiologisk Forskningsfund.
Bjarne Linde Nørgaard received unrestricted institutional research grants from
Siemens and HeartFlow. Damini Dey is a patent-holder of Autoplaque©
research software, and receives software royalties from Cedars-Sinai Medical
Center, Los Angeles, California, USA. The funders had
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.