
Abstract
Our aims were to study left ventricular (LV) function and myocardial blood flow reserve (MBFR) in long-term type 1 diabetes and associations with advanced glycation end products (AGEs). A total of 20 type 1 diabetes patients from the Oslo Study without significant stenosis on coronary angiography were compared with 26 controls. LV systolic and diastolic functions were assessed by two-dimensional strain and the ratio between pulsed Doppler transmitral early (E) velocity and tissue Doppler velocity (E′), respectively. MBFR was evaluated by contrast echocardiography. The AGE methylglyoxal-derived hydroimidazolone was analysed in serum. Glyoxal hydroimidazolone in skin collagen was determined by liquid chromatography-mass spectrometry. Strain was significantly reduced (−19.5% ± 1.9% vs −21.4% ± 3.5%, p < 0.05), and E/E′ increased in the diabetes patients compared to controls, 7.3 ± 2 versus 6.0 ± 1.5, p < 0.05. Significant lower MBFR was present in the diabetes patients, 3.4 (2.1, 5.3) versus 5.9 (3.9, 9.6), p < 0.01. Both AGEs correlated significantly with E/E′. The impaired LV function with correlation to AGEs in concert with reduced MBFR in diabetics without coronary artery disease may indicate possible mechanisms for diabetic cardiomyopathy.
Keywords
Introduction
Diabetes is a major risk factor for macrovascular coronary heart disease. Previous studies1,2 have reported a high prevalence of preclinical diastolic impairment in type 1 diabetes and demonstrated that impaired left ventricular (LV) diastolic function is one of the main features of diabetic heart disease. HbA1c has been found to correlate with impaired diastolic function. 1 Advanced glycation end products (AGEs), the glucose-derived compounds formed non-enzymatically and accumulated in long-lived tissue proteins, have been associated with the development of diabetic vascular complications, and have also been suggested as a pathophysiologic mechanism for a diastolic heart failure in these patients.3,4 None of these studies, however, have excluded coronary artery disease by angiography.1,2,4
LV dysfunction in the absence of hypertension, coronary artery and valvular heart disease has been defined as diabetic cardiomyopathy. 5 However, there are still uncertainties about the diagnosis of diabetic cardiomyopathy and how it develops. LV systolic and diastolic functions in diabetes patients have mainly been examined by standard echocardiography, and recently also by tissue velocity imaging (TVI). 6 Few studies have used novel echo methods as contrast and two-dimensional (2D) strain in long-standing type 1 diabetes.
Some studies have indicated a disturbance in coronary flow in the absence of coronary macrovascular disease in diabetes.7,8 Similar results have been demonstrated in type 1 and type 2 diabetes. 9 It is, however, not known whether similar findings are present in long-term type 1 diabetes patients by use of the novel method transthoracal myocardial contrast echocardiography (MCE) by dipyridamole stress.
Our main aim was to study LV systolic and diastolic functions in a cohort with long-term type 1 diabetes by standard and novel echo modalities. Our hypotheses were that these patients, even without coronary artery disease, would have impaired LV systolic and diastolic function and have reduced myocardial blood flow reserve (MBFR) by quantitative stress MCE. Another hypothesis was that reduced LV systolic and diastolic functions would be associated with glycaemic control and AGEs.
Methods
Study design
In the Oslo Study from 1982, 45 patients with type I diabetes were randomized to either continuous subcutaneous insulin infusion with portable pumps, multiple (>5) daily insulin injections or continued conventional treatment with two daily injections. After 4 years, intensified treatment retarded the progression of microvascular complications, and all patients were consequently offered intensified treatment, and followed prospectively. Criteria for inclusion were as follows: age 18–45 years, diagnosis of type 1 diabetes at <30 years of age, disease duration more than 7 years but less than 30 years, C-peptide <0.1 nmol/L and no or minimal microvascular complications. 10 After 27 years follow-up, 33 participants were still being followed. Two had died of causes not related to diabetes, one ‘dead in bed’ possibly associated with diabetes, eight were lost to follow-up and one had to withdraw from the examinations because of newly diagnosed cancer. Of these patients, 27 of them, not significantly different from the total group regarding age and glycaemic control, were included in this study.
None of the participants had clinical symptoms of heart disease, but to exclude subclinical coronary artery disease, a coronary angiography was performed in the 27 participants. Seven patients were detected with significant coronary artery stenosis (two had single vessel disease, two had two and three had three vessel disease) and excluded from the final analysis. A total of 20 diabetes patients without cardiovascular disease were then included and compared with 26 age- and sex-matched healthy controls. The participants of the control group had no cardiovascular disease or did not report using any anti-hypertensive medication or statins. HbA1c was measured in the diabetic patients prospectively every year for 27 years. Informed consent was obtained from each patient, and the investigations conform to the principles outlined in the ethical guidelines of the Declaration of Helsinki 1975, revised Hong Kong 1989. The study protocol was approved by the Regional Committee for Ethics in Medical and Health Research of South-Eastern Norway.
Echocardiography
All echocardiography recordings were performed as recommended by the American Society of Echocardiography 11 without knowledge of the clinical status of the participants. EchoPac program (GE Vingmed Ultrasound AS, Norway) was used for offline analysis. LV mass was determined by Devereux’s formula and indexed to body mass index. 12 More sensitive echocardiographic methods to detect mild and early diastolic and systolic dysfunction than standard echocardiography measurements are TVI and 2D speckle tracking imaging. TVI images were obtained from an apical four-chamber apical view, and systolic peak velocities during LV contraction (S′) were measured and averaged. 13 Automated function imaging (AFI) reflecting systolic LV function, based on 2D speckle tracking imaging, was assessed as a measure of global LV longitudinal strain. 14 Longitudinal strain is presented as negative values; a larger negative value indicates a larger extent of deformation or shortening.
Mitral inflow velocities included peak early filling (E) and late diastolic filling (A) velocities and the E/A ratio. 13 Early diastolic TVI (E′) velocities were measured at similar locations as S′ and averaged. E/E′ and E/E′/end-diastolic volume (EDV) were calculated as indices for LV filling pressure 13 and stiffness, respectively.
Quantification of LV perfusion by MCE
A standardized vasodilator stress protocol with dipyridamole 0.56 mg/kg was used as recommended by the European Association of Echocardiography. 15 The ultrasound contrast agent SonoVue® (Bracco, Italy) was administered by a continuous intravenous (IV) infusion rate of 0.8 mL/min for 2 min at rest and then for 2 min after completion of the dipyridamole infusion. The quantitative perfusion analyses were performed as described previously by Malm et al. 16 by one examiner (K.A.S.), blinded for the clinical status of the participants. Myocardial blood volume (A), myocardial blood velocity (β) and their product myocardial blood flow (MBF) 17 were estimated, and MBFR (stress/rest ratio) was calculated. Due to low quality of the basal images of almost all views, we decided to perform analyses only in the mid segments of apical four-chamber, apical two-chamber and apical long-axis views. The basal and apical segments, where others 16 previously have reported artefacts (basal) and low values (apical) due to spatial problems, were therefore excluded. The MBF and MBFR reported in this article are the median values of all three views combined.
Coronary angiography
The quantitative analyses of the coronary angiograms were performed using an automated stenosis analysis program (Centricity Cardas Xi2, GE Healthcare, Norway). An independent experienced examiner blinded for the MCE data did the coronary angiography examinations and their analyses (M.B.). A significant coronary artery stenosis was defined as ≥50% diameter stenosis.
AGEs and HbA1c
All blood samples were taken after overnight fast. Serum levels of methylglyoxal-derived hydroimidazolone (MG-H1) were measured with a competitive immunoassay developed in our laboratory. 18 During the clinical examinations, a 3-mm punch skin biopsy was obtained from the upper inner quadrant of either buttock (area without sun exposure), and immediately stored on ice and under N2 at −80°C. The skin samples were enzymatically proteolysed, and the collagen-linked AGE glyoxal hydroimidazolone (G-H1) was determined by liquid chromatography-mass spectrometry as previously described. 19 The mean value for annual measurements over 27 years is used in this article (HbA1c27). The different methods used in the first years of the cohort have previously been described. 20 DCA 2000 (Bayer Diagnostics, NY) has been used the last 10 years. The accuracy of the method has been secured by use of the same internal Diabetes Control and Complications Trial (DCCT)-adjusted standard. The interassay coefficient of variation was <3%.
Statistical methods
Continuous variables are represented as mean ± standard deviation (SD) if normally distributed and as median (interquartile range) if not. Comparisons within the group were performed using the paired t-test. Comparisons between groups were performed using the student t-test, if appropriate after log transformation. Correlations between two continuous variables were performed using Spearman’s rank order coefficient. To explore the predicative ability of MG-H1 on the dependent variable E/E′, a multiple linear regression model was applied. Variables for linear analysis were selected based on univariate correlation analyses and variables known or likely to be associated with E/E′. No variables in the included model correlated strongly (r < 0.6). Because of the relative small sample size, only variables from the univariate analysis with p < 0.1 were included in the multiple model. We adjusted for gender, diabetes duration, creatinine and blood pressure in the final multiple linear regression analysis. The assumption of linearity and normal distribution of residuals were achieved in the presented model.
Reproducibility data were tested by intraclass correlation coefficient (ICC) for EDV, and peak early filling (E) and E/E′ were tested in eight random participants. Measurements were performed by one of the authors (K.A.S.) and a colleague from our echocardiography laboratory. The level of significance was set at p < 0.05. All calculations were performed using SPSS version 18.0 (SPSS, Chicago, USA).
Results
Clinical and demographic characteristics of the study population are summarized in Table 1.
Clinical and demographic characteristics in patients with type 1 diabetes and controls.
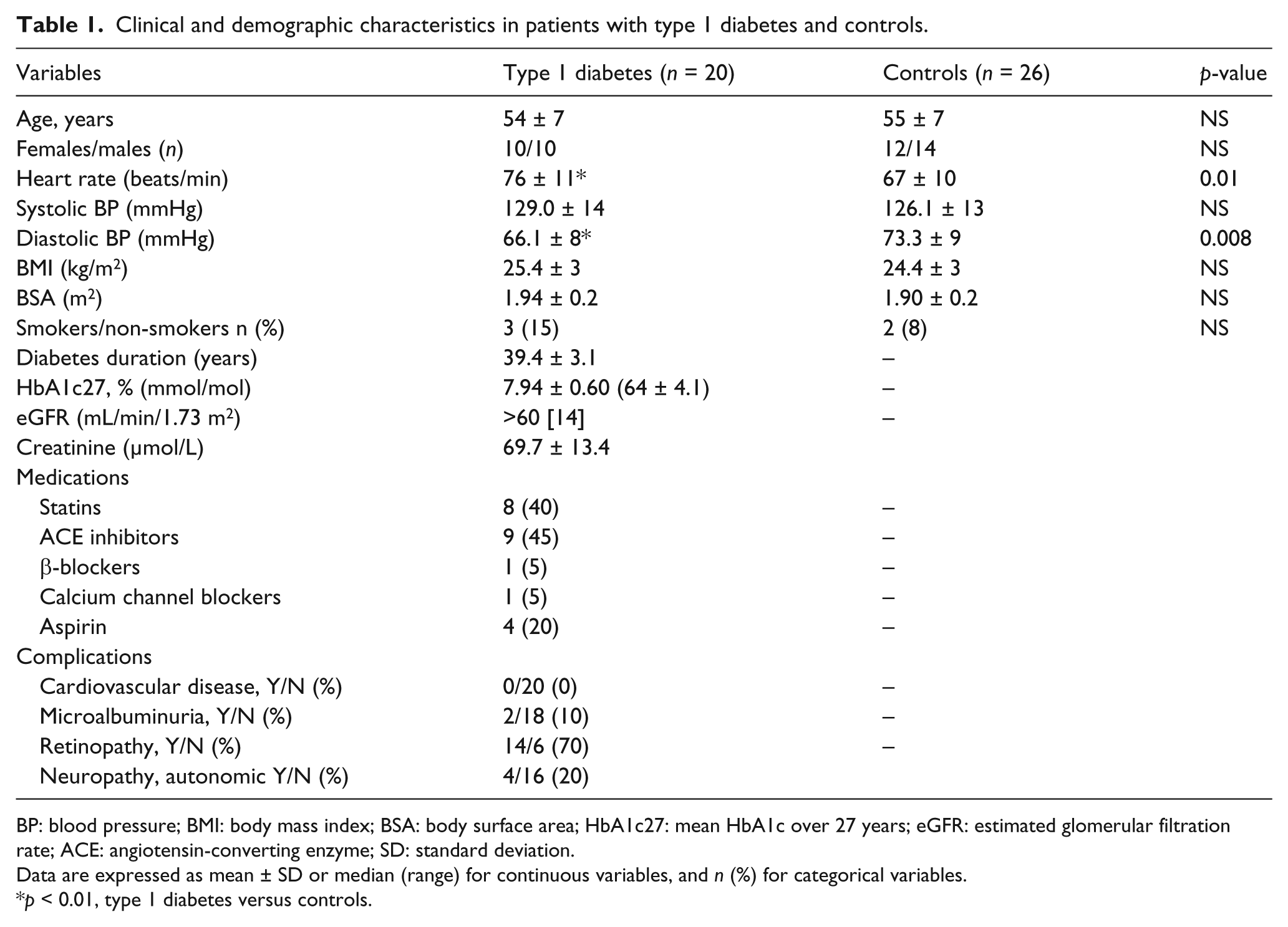
BP: blood pressure; BMI: body mass index; BSA: body surface area; HbA1c27: mean HbA1c over 27 years; eGFR: estimated glomerular filtration rate; ACE: angiotensin-converting enzyme; SD: standard deviation.
Data are expressed as mean ± SD or median (range) for continuous variables, and n (%) for categorical variables.
p < 0.01, type 1 diabetes versus controls.
Baseline echocardiography results are presented in Table 2. Longitudinal strain was significantly lower in the diabetes patients compared to the controls −19.5% ± 1.9% versus −21.4% ± 3.5% (p < 0.05), while E/E′ was significantly higher in the diabetes patients, 7.3 ± 2 versus 6.0 ± 1.5 (p < 0.05). Inter-observer variability was tested in eight subjects, with intraclass coefficients (confidence intervals) of 0.95 (0.82, 0.99), 0.98 (0.95, 0.99) and 0.99 (0.96, 0.99), for EDV four-chamber, E velocity and E/E′, respectively.
Two-dimensional, M-mode, pulsed Doppler and tissue velocity imaging data in patients with type 1 diabetes and control individuals.
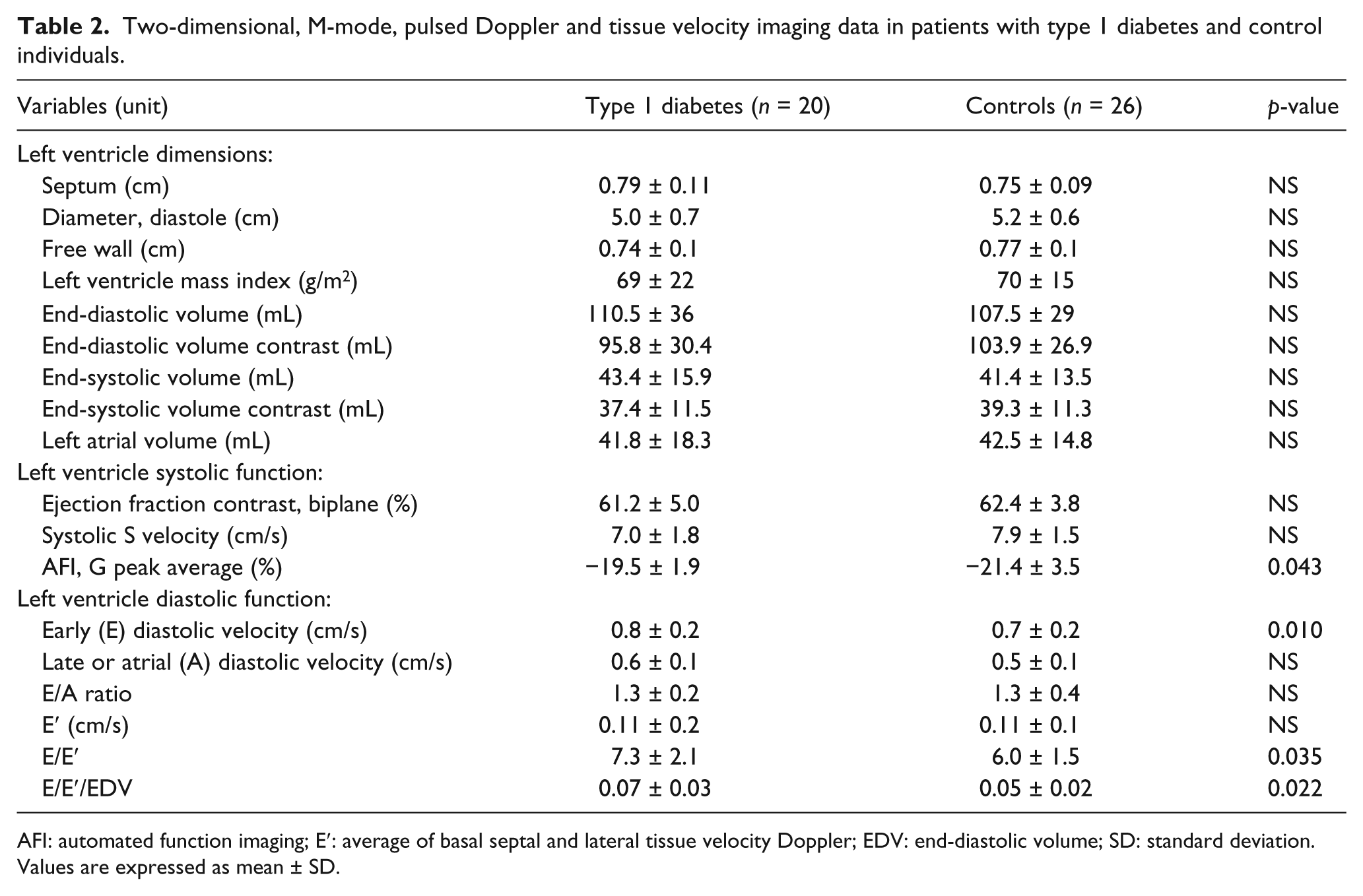
AFI: automated function imaging; E′: average of basal septal and lateral tissue velocity Doppler; EDV: end-diastolic volume; SD: standard deviation.
Values are expressed as mean ± SD.
Multiple linear regression analyses
In a model of linear regression analysis applying E/E′ as dependent variable, and MG-H1, sex, systolic blood pressure, diabetes duration and creatinine as independent variables, univariate analysis showed that MG-H1 could explain 37% of the variation in E/E′, 33% in creatinine, 21% in systolic blood pressure, 9% in duration of diabetes and 20% in gender. When adjusting for creatinine, systolic blood pressure, duration of diabetes and gender, MG-H1 was still associated with E/E′ (p = 0.014) (Table 3).
Univariate and multiple linear regression models for associations with E/E′ in the diabetes patients (n = 20).
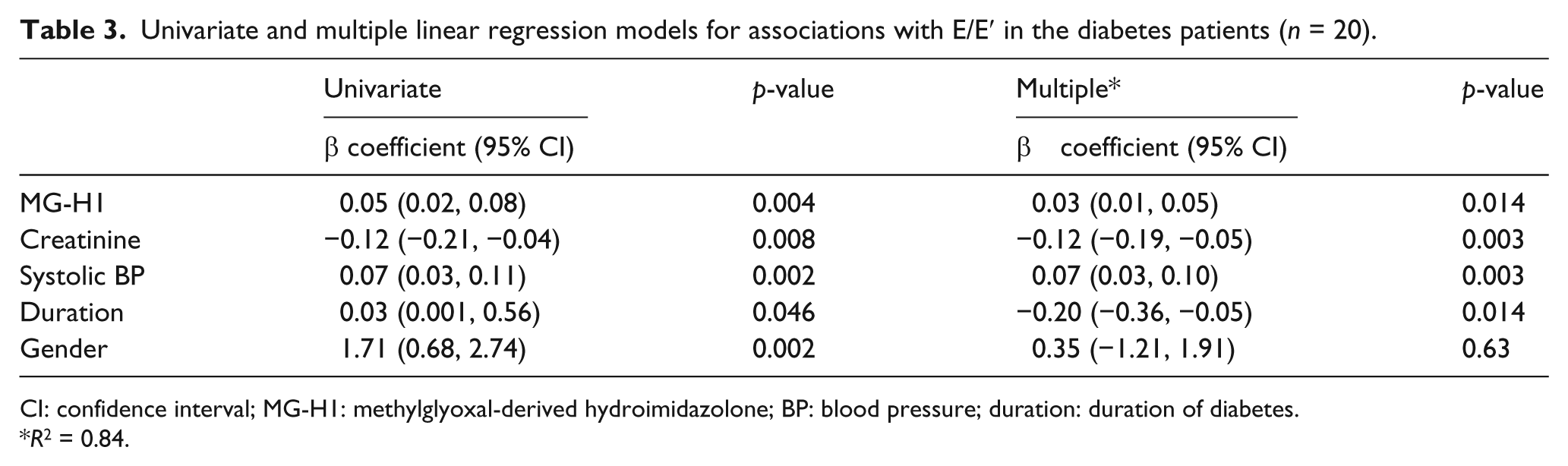
CI: confidence interval; MG-H1: methylglyoxal-derived hydroimidazolone; BP: blood pressure; duration: duration of diabetes.
R2 = 0.84.
MCE at rest and during dipyridamole stress
A significant lower MBF during stress was found in the diabetes patients compared to controls, 2.18 (1.29–2.84) versus 4.95 (2.50–5.46), p = 0.001. Similarly, MBFR was significantly lower in diabetes patients compared to controls (Figure 1). No differences were observed between the groups during rest, 1.88 (1.33–2.34) versus 1.90 (1.13–2.69), p = 0.83.
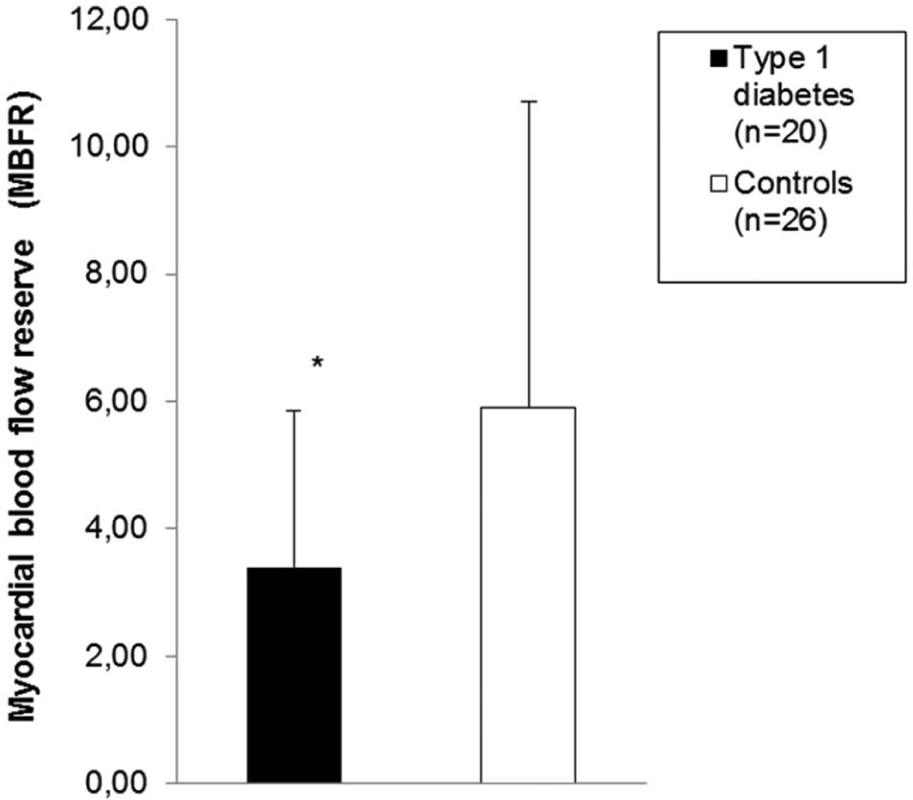
Global myocardial blood flow reserve in 20 type 1 diabetes patients (black) and 26 controls (white). The data are expressed as median (interquartile range). *p < 0.01 type 1 diabetes versus controls.
Correlations between LV function and myocardial perfusion with AGEs and glycaemic control
HbA1c over 27 years correlated significantly with 2D strain (Table 4). MG-H1 in serum correlated significantly with 2D strain, E/E′ and E/E′/EDV (Table 4). G-H1 was significantly associated with E/E′/EDV. Global MBFR did not correlate significantly with HbA1c27, MG-H1 or G-H1.
Spearman correlation coefficients for the association between LV function, myocardial blood flow reserve with AGEs and glycaemic control.
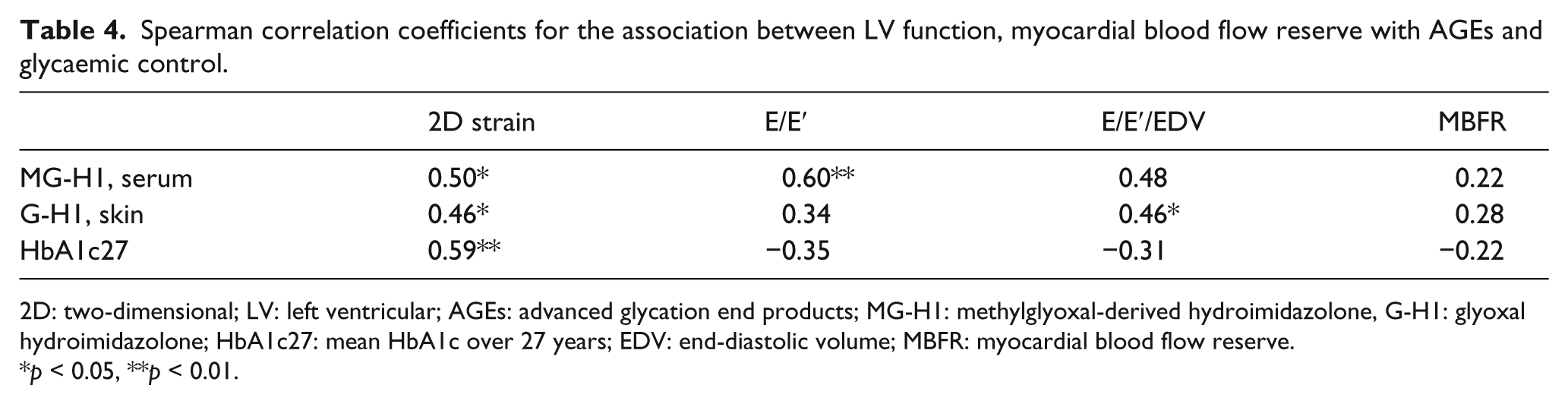
2D: two-dimensional; LV: left ventricular; AGEs: advanced glycation end products; MG-H1: methylglyoxal-derived hydroimidazolone, G-H1: glyoxal hydroimidazolone; HbA1c27: mean HbA1c over 27 years; EDV: end-diastolic volume; MBFR: myocardial blood flow reserve.
p < 0.05, **p < 0.01.
Discussion
We have demonstrated that long-term type 1 diabetes patients without significant coronary artery disease, as documented by coronary angiograms, have impaired subclinical LV systolic and diastolic functions compared to controls. We also observed a consistent association between impaired LV diastolic function and AGEs, and a reduced MBFR indicating myocardial microangiopathy in these patients. Consistent with a previous study, type 1 diabetes seems to affect both diastolic function and MBFR adversely. 8
LV function and AGEs
We observed significant correlations between the AGEs MG-H1 in serum and G-H1 in skin with two different LV diastolic indices, E/E′ and E/E′/EDV, reflecting increased LV filling pressure and LV diastolic stiffness, respectively. These associations may suggest AGEs to be important in the development of diastolic dysfunction in these patients. MG-H1 and G-H1 are formed by different metabolic pathways, and both are produced in an accelerated rate when plasma glucose is elevated. AGEs modify proteins, increase vascular permeability and quench nitric oxide activity which results in an impairment in endothelium-dependent relaxation. 21 AGE deposition is observed within the atherosclerotic plaque present in vessels and cardiac myofibrils from diabetes patients, 22 and in the wall of small intramyocardial vessels. 23 Type I collagen is the most common connective tissue in skin and accounts for approximately 75% of total collagen in the adult myocardium, 24 and we measured G-H1 in collagen in skin. Moreover, the half-life of skin collagen is calculated to about 15 years, 25 making the accumulation of modified collagen important for long-term stiffness in many organs, including the heart.
The transmitral peak filling velocity E was significantly enhanced in our diabetes patients reflecting that the increased E/E′ ratio was driven by E and not by E′, which is in contrast to another study demonstrating impaired relaxation (E′) in diabetes patients. 6 Takeda et al., however, did not find E′ to be a significant determinant of heart failure in diabetes patients with preserved ejection fraction. They concluded that the progression from asymptomatic stage to diastolic heart failure may be induced by worsening of LV compliance rather than LV relaxation. 26 This is supported by our finding of increased E/E′/EDV, which also points to LV stiffness (reduced compliance) and remodelling as possible mechanisms for the diastolic impairment in our patients. The associations of both AGEs to E/E′/EDV without significant coronary artery disease add support to this notion. Moreover, the associations between our diastolic echo indices and AGEs remained significant after adjustment for known risk factors in a multivariable model.
A previous study of the same population some years earlier did not demonstrate the present impaired LV diastolic function, but a similar reduction of LV systolic function, and systolic strain tended to correlate with AGEs, but did not reach significance (r = 0.37, p = 0.07). 27 In the present study, a significant association between strain and AGEs was found. The explanation may be that serum AGEs in the previous study were measured 1 year before the echo examinations and represented total AGEs, whereas the AGEs measured in the present study were MG-H1 and G-H1. 27 We have also used AFI strain, which is less angle dependent than strain based on TVI in the previous study, and thus may be more sensitive for changes in the LV myocardium.
Myocardial blood perfusion
Our perfusion results indicate that patients with diabetes have impaired MBFR compared to controls. These findings are similar to a previous study in type 2 diabetes using MCE combined dipyridamole/stress protocol. 28 Moreover, MCE-derived MBF and its flow reserve have been validated against coronary angiography 29 and found to be a reliable method to reflect myocardial blood perfusion.
The reduced MBF and flow reserves were significant in the diabetes group without significant coronary artery disease on angiography, indicating that coronary artery disease cannot explain the impaired myocardial parameters. Moir et al. 28 have previously reported impaired MBFR in patients with type 2 diabetes without evidence of coronary heart disease using a semi-quantitative MCE-derived method, which supports our finding. Reduced MBFR has also been reported in type 1 diabetes by a different methodology. 9 A previous study by Rana et al. 30 observed a twofold increase in MBF in type 1 diabetes subjects which is in contrast to our only minor increase in MBF in the diabetic group, whereas others have found similar results with blunted increase in MBF and reduced MBFR suggesting a paradox coronary vasoconstriction in the absence of atheroma as a possible mechanism for this in type 1 diabetes. 8 However, none of these studies had excluded significant coronary stenosis by coronary angiography.7,8,9,30
Clinical implications
In a large cohort of type 1 diabetes patients, the incidence of heart failure increased progressively with HbA1c, with a range of 1.42–5.20 per 1000 patient-years between patients in the lowest (<6.5% (48 mmol/mol)) and highest (≥10.5% (91 mmol/mol)) categories of HbA1c, supporting hyperglycaemia in the development of heart failure. 31 We found significant correlations between LV functions with AGEs and HbA1c over 27 years. We therefore consider our data to indicate that both AGEs and HbA1c may predict the progression of cardiac myocardial damage in long-term type 1 diabetes not caused by epicardial coronary disease. Moreover, the association with both types of oxoaldehyde hydroimidazolones, that is, methylglyoxal and glyoxal, suggests possible oxidative processes as participants in the damage underlying systolic and diastolic functions.
Study limitations
Since we recruited healthy volunteers as controls, there were significant differences in the use of angiotensin-converting enzyme (ACE) inhibitor, beta-blockers and aspirin between the groups that also could influence the results. However, only one patient used beta-blockers, the medication expected to have any impact on LV function. It is likely that the medications used by our patients have minor influence on the results.
Hypoglycaemia has also been associated with disturbances in MBF and may therefore be a confounder of low MBFR. 30 However, none of our participants had symptoms of hypoglycaemia during the procedure.
Our study comprises a relatively small number of participants, which makes it difficult to allow for adjustment for all possible underlying confounders in multiple regression analysis. However, we consider that the long-term data on glycaemic control and the homogeneity of the group with minor variation in age and duration of disease to some extent compensate for the small sample size. The use of comprehensive methods as quantitative MCE, standard and novel echocardiography and coronary angiography also provide an objective evaluation of the myocardial status in this population.
In summary, we observed impaired subclinical LV systolic and diastolic function in a cohort of type I diabetes of 40 years duration without significant coronary heart disease, documented by coronary angiograms, compared to controls. The consistent relation between two different indices of AGEs, from skin and serum, and LV preclinical systolic and diastolic impairment may indicate AGEs to be an important mechanism for impaired heart function in type 1 diabetes. We have also demonstrated reduced MBFR in patients with normal coronary arteries, which may reflect myocardial microangiopathy in our patients. We therefore suggest these myocardial changes together with AGEs to be possible mechanisms in the development of diabetic cardiomyopathy.
Footnotes
Acknowledgements
K.A.S. designed the present follow-up study, performed echocardiography analysis, researched data and wrote the manuscript. T.N. designed the echocardiography follow-up, performed the echocardiography recordings and contributed to discussion and edition of the manuscript. V.M.M., C.M.S. and D.R.S. did the cross-sectional AGE analysis and edited the manuscript. P.A.T. performed the immunoassay analysis and edited the manuscript. M.B. did the coronary angiography examinations and their analyses and edited the manuscript. K.F.H. and K.D-J designed the study, followed the patients and contributed to discussions and writing of the manuscript. K.S. designed the echocardiography follow-up, supervised the echocardiography analysis, contributed to discussion and writing of the manuscript. K.A.S. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The authors thank Jonny Hisdal for help with graphics, Gard P Gjerdalen for help with echocardiography data reproducibility testing, Morten Wang Fagerland for statistical assistance and Ingebjørg Seljeflot for excellent laboratory facilities.
Declaration of conflicting interests
None declared.
Funding
This work was funded by the South-Eastern Norway Regional Health Authority (grant number 2009001), Oslo University Hospital and Oslo Diabetes Research Centre. The Vilma and Robert R. Kohn Advanced Glycation End product Analytical Facility at Case Western Reserve University provided comprehensive AGE analyses.