
Abstract
Background:
Advanced protein glycation is an important mechanism for the development of late diabetic complications including atherosclerosis. Methylglyoxal-derived hydroimidazolone-1 is the most abundant advanced glycation end product in human plasma.
Aim:
To investigate the relationship between methylglyoxal-derived hydroimidazolone-1 and early signs of atherosclerosis in children and adolescents with type 1 diabetes and healthy controls.
Methods:
A total of 314 diabetes patients aged 8–18 years were compared with 120 healthy controls. Serum methylglyoxal-derived hydroimidazolone-1 was measured by immunoassay. Atherosclerosis was evaluated by assessing carotid intima-media thickness by ultrasound, arterial stiffness by Young’s modulus and inflammation by C-reactive protein.
Results:
Methylglyoxal-derived hydroimidazolone-1 was significantly increased in the diabetes group compared with controls, 155.3 (standard deviation (SD) = 41.0) versus 143.0 (SD = 35.1) U/mL, p = 0.003, as was C-reactive protein, median 0.51 (0.27, 1.83) versus 0.31 (0.19, 0.67) mg/L, p < 0.001. There was no significant difference between the groups regarding carotid intima-media thickness or Young’s modulus. Multiple regression analysis showed a significant positive association between methylglyoxal-derived hydroimidazolone-1 and C-reactive protein in the diabetes group.
Conclusion:
Serum levels of methylglyoxal-derived hydroimidazolone-1 in diabetes patients are increased and associated with low-grade inflammation, but not yet arterial stiffness or wall thickness. This indicates that methylglyoxal-derived hydroimidazolone-1 may be important in the early phase of the accelerated atherosclerotic process in diabetes.
Introduction
Atherosclerosis is a slowly progressing process that begins in childhood. Macrophage foam cells in the intima layer of human arteries have been detected in infants. 1 Patients with type 1 diabetes mellitus (T1D) have an increased risk of developing atherosclerosis and cardiovascular disease.2,3 Increased production of advanced glycation end products (AGEs) is one of several pathways that may connect T1D and atherosclerosis, and increased oxidative stress has been proposed as the common initiating factor. 4 The laboratory evidence for the involvement of AGEs in atherosclerosis is accumulating, especially as anti-AGE treatment in rodent models has shown reduced progression of atherosclerotic lesions. 5 However, there is still a need for clinical studies to determine whether this is also the case in humans.
Methylglyoxal is a highly reactive α-oxoaldehyde. It is formed in part by non-enzymatic fragmentation of the triosephosphates created in glycolysis, and the rate is increased in hyperglycaemia. 6 One of the earliest vascular changes in diabetes is impairment of endothelial vasorelaxation, and this may be mediated by intracellular methylglyoxal. 7
When methylglyoxal reacts with an arginine residue of a protein, the resulting compound is known as methylglyoxal-derived hydroimidazolone, and the protein has become an AGE. Hydroimidazolones are the dominant AGEs in both serum and tissue, and methylglyoxal-derived hydroimidazolone-1 (MG-H1) is the most common product. 8 MG-H1 modifications have recently been described in endothelial cells of normal and atherosclerotic vessel walls in human carotid arteries. 9
It is a challenging task to objectively, and preferably non-invasively, evaluate the extent of early atherosclerosis in children and adolescents. Measurement of intima-media thickness in arteria carotis communis [carotid intima-media thickness (cIMT)] is widely used and predicts cardiovascular events in subjects without clinically evident disease. 10 C-reactive protein (CRP) is commonly used as a marker of inflammation in clinical practice and has proven to be a good predictor of cardiovascular disease. 11 Young’s modulus, which is a measure of stiffness in elastic materials, can be assessed by ultrasound. 12 There is an established link between hyperglycaemia and reduced elasticity, 13 and arterial stiffness precedes plaque formation in the development of atherosclerosis. 14
Current concepts claim an important role for AGEs in the development of late diabetic complications including atherosclerosis. Since atherosclerosis is a disease that starts in childhood and MG-H1 is the most common AGE in serum, we wanted to investigate whether there is a meaningful relationship between levels of MG-H1 and signs of early atherosclerosis in children and adolescents with or without diabetes. To our knowledge, this has not previously been reported.
Methods
A letter of invitation was sent to all patients with T1D aged 8–18 years registered in the national Norwegian Childhood Diabetes Registry and living in the southeast health region of Norway. A total of 800 letters were sent, 314 patients responded and these were included in the study. The healthy control subjects were primarily classmates of the participating diabetic children, and 120 were included. The study was conducted in accordance with the Declaration of Helsinki, the protocol was approved by the Norwegian Regional Committee for Research Ethics and all participants gave their written informed consent. The data were collected between 2006 and 2009, and the details have previously been described by Margeirsdottir et al. 15
Before a clinical examination, fasting blood samples were taken in the morning between 7:30 and 10:00 a.m. Serum was separated within 1 h by centrifugation at 2500 × g for 10 min and kept frozen at −80 °C until analysed. Routine laboratory analyses were performed by conventional methods.
After blood sampling, the subjects were examined by high-resolution carotid ultrasonography in the supine position using a Siemens Acuson Sequoia 512 (Siemens Acuson, Mountain View, CA, USA) ultrasound scanner equipped with a linear array 14 MHz transducer. All images were recorded from the far wall of the common carotid artery in end-diastole. An experienced radiologist, blinded to the subjects’ diagnosis and clinical details, later performed all the measurements of thickness and elastic properties offline. Blood pressure was measured in the radial artery using a standard oscillometric device.
Glycated haemoglobin (HbA1c) was measured at a Diabetes Control and Complications Trial (DCCT)–standardized laboratory using high-performance liquid chromatography (Variant; Bio-Rad, Richmond, CA, USA).
CRP was determined using an enzyme-linked immunosorbent assay (DRG Instruments GmbH, Marburg, Germany) with a detection limit of 0.1 mg/L and an inter assay coefficient of variation of <5%.
MG-H1 was measured by dissociation-enhanced lanthanide fluorescent immunoassay (DELFIA). The anti-hydroimidazolone antibodies showed little cross-reactivity and high sensitivity. The development of the assay has previously been described in detail.16,17 The assay has shown a significant positive correlation with a stable isotopic dilution analysis liquid chromatography-mass spectrometry (LC-MS/MS) technique (Dr V Monnier, Cleveland, OH, USA) (unpublished observation).
Young’s modulus, E, is a measure of stiffness in elastic materials. It is the ratio of the stress applied to the arterial wall and its change in shape in the same direction, known as strain. 12 It can be expressed as
where d is the arterial diastolic diameter and IMT is the intima-media thickness. DC is the distensibility coefficient, which is the relative change in lumen area during systole for a given change in pulse pressure;
Statistical analysis
Demographic and clinical data are presented as proportions, means with their standard deviations (SDs) or medians with the 25th and 75th percentile. Differences in continuous variables between diabetes patients and controls were tested with the Student t-test for normally distributed data and the Mann–Whitney U-test for non-normally distributed data. Correlation analyses between continuous variables were performed using Pearson’s correlation coefficient (r) for normally distributed data or Spearman’s rho (ρ) for non-normally distributed data. The χ2-test for contingency tables with different degrees of freedom was used to detect associations between categorical independent variables. Univariate linear regression analysis was performed to study the association between MG-H1 as the exposure variable and either cIMT, Young’s modulus or CRP as outcome variables. CRP was loge-transformed to achieve normally distributed residuals. To identify possible confounders, we studied all variables that could theoretically influence MG-H1, cIMT, Young’s modulus or CRP. Only variables with significant relationships with both the exposure and the outcome variables were considered as possible confounders and included in the multivariate analysis. Adjustment for multiple confounding factors was done using multivariate linear regression analysis with a manual backward elimination procedure. A significance level of 5% was used. All statistical analyses were performed using the SPSS software package for Mac, version 18.0 (SPSS, Chicago, IL, USA).
Results
The diabetes patients had a mean duration of disease of 5.5 years (SD = 3.4) and a mean HbA1c of 8.4% (SD = 1.2) (68 mmol/mol, SD = 13.1). Almost all (97%) were using intensive insulin treatment, defined as using insulin pumps or basal-bolus regimens with more than four daily insulin injections, and 60% used insulin pumps.
The patients were representative of the young T1D population in Norway regarding HbA1c, blood pressure, lipid status, age, gender and pubertal stage. 15 They were, however, slightly older, with marginally longer diabetes duration, higher body mass index (BMI) and more were pump users. This is because only patients above the age of 8 years were included in the study.
The clinical and metabolic characteristics of the diabetes patients and controls are shown in Table 1. Compared to the control subjects, the diabetes patients were taller, heavier and had higher BMI and waist circumference. They also had increased systolic and diastolic blood pressure, total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, apolipoprotein B and apolipoprotein A1.
Clinical and metabolic characteristics.
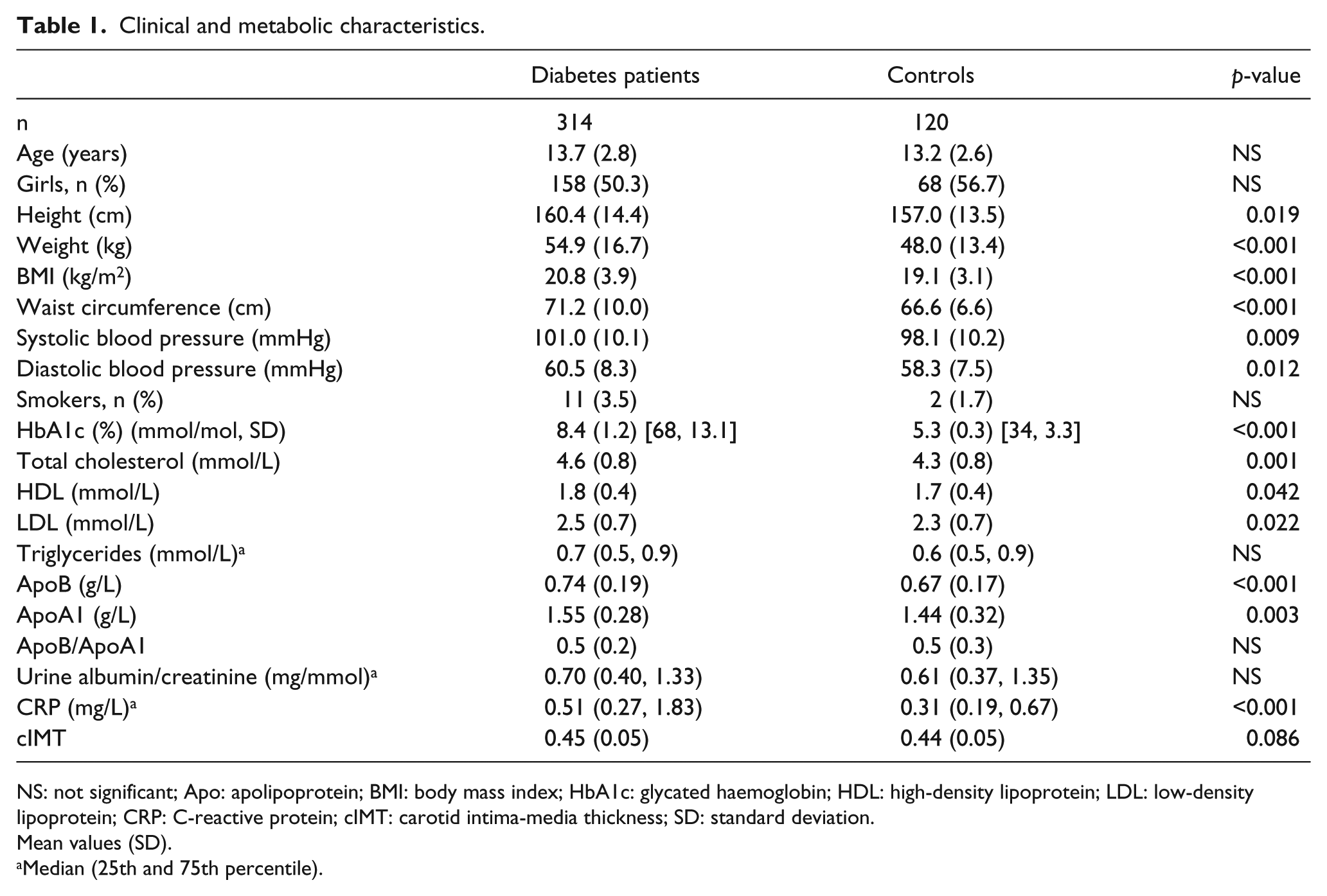
NS: not significant; Apo: apolipoprotein; BMI: body mass index; HbA1c: glycated haemoglobin; HDL: high-density lipoprotein; LDL: low-density lipoprotein; CRP: C-reactive protein; cIMT: carotid intima-media thickness; SD: standard deviation.
Mean values (SD).
Median (25th and 75th percentile).
The levels of MG-H1 were significantly increased in the diabetes group compared to controls (Table 2). The girls had higher levels of MG-H1 than the boys, significantly so in the diabetes group. We found no relationship with puberty to explain this difference (data not shown). The smokers had significantly higher levels than the non-smokers. No comparisons of smoking and MG-H1 between the groups of diabetic patients and controls were performed, due to few smokers and low statistical power. Furthermore, MG-H1 correlated positively with HbA1c in the diabetes group, Pearson’s r = 0.12, p = 0.037.
Levels of methylglyoxal-derived hydroimidazolone-1 (U/mL).
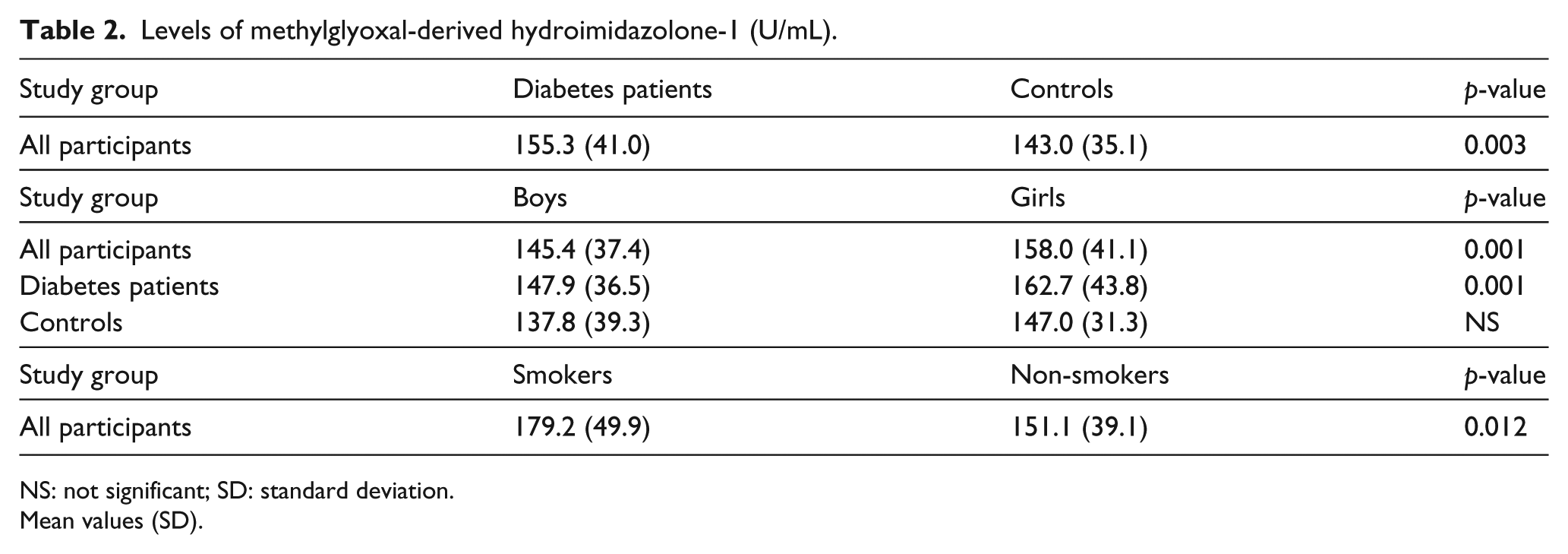
NS: not significant; SD: standard deviation.
Mean values (SD).
As we have previously reported, the diabetes patients had more frequently elevated cIMT than healthy control subjects: 19.5% were above the 90th percentile of healthy control subjects, and 13.1% were above the 95th percentile (p < 0.001). Mean cIMT was significantly higher in diabetic boys compared to controls 0.46 (SD = 0.06) versus. 0.44 (SD = 0.06) mm, p = 0.04, but not in girls or in the entire study population. 15 We did not find any significant difference in Young’s modulus between the diabetes group, 367.5 (SD = 137.4) kPa, and the control group, 354.8 (SD = 116.7) kPa. CRP, however, was significantly increased in the diabetes group compared to controls, median 0.51 (0.27, 1.83) versus 0.31 (0.19, 0.67) mg/L, p < 0.001. When excluding values above 10 mg/L, as these might be caused by infections rather than vascular inflammation, the results were essentially the same, median 0.47 (0.26, 1.47) versus. 0.31 (0.19, 0.62) mg/L, p < 0.001.
Investigating the influence of MG-H1 on the parameters for atherosclerosis, univariate analysis revealed statistically significant relationships between MG-H1 and cIMT [βunadj = −3.2 × 10−4, standard error (SE) = 7.4 × 10−5, p < 0.001] and natural logarithm of C-reactive protein (LnCRP) (βunadj = 0.008, SE = 0.002, p < 0.001) in the diabetes group. No associations were found in the control group.
The results from the multivariate linear regression analyses with a manual backward elimination procedure in the diabetes group are presented in Table 3.
Multiple regression analyses in the diabetes group with MG-H1 as the exposure variable.
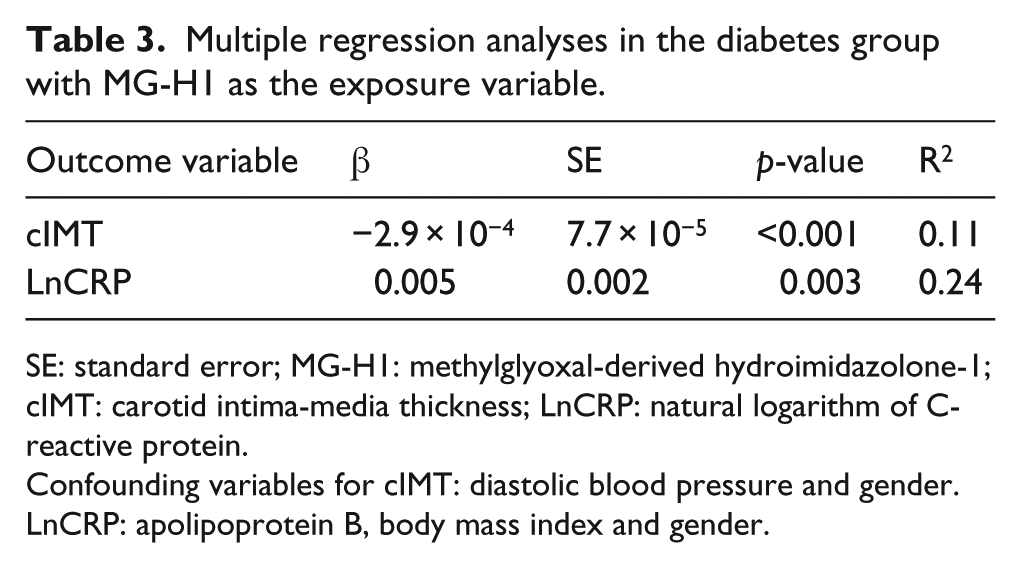
SE: standard error; MG-H1: methylglyoxal-derived hydroimidazolone-1; cIMT: carotid intima-media thickness; LnCRP: natural logarithm of C-reactive protein.
Confounding variables for cIMT: diastolic blood pressure and gender. LnCRP: apolipoprotein B, body mass index and gender.
In the diabetes group, the association between MG-H1 and cIMT and LnCRP remained significant when controlling for confounding factors. When only including values of CRP < 10, the results were very similar, β = 0.004, SE = 0.002, p = 0.029 and R2 = 0.217.
We also investigated the relationship between traditional risk factors (blood pressure, lipids, smoking and BMI) and the parameters for atherosclerosis. As previously reported, we found no associations with IMT or Young’s modulus. 15 However, we found that triglycerides (β = 0.923, SE = 0.168, p < 0.001 and R2 = 0.32, controlling for current acute illness, gender and BMI) and BMI (β = 0.079, SE = 0.019, p < 0.001 and R2 = 0.36, controlling for current acute illness, triglycerides, MG-H1 and gender) were significantly associated with LnCRP in the diabetes group. In the control group, BMI was significantly associated with LnCRP, β = 0.108, SE = 0.039, p = 0.001 and R2 = 0.09, no confounding variables. The associations in both groups remained significant when only including values of CRP < 10 (data not shown).
Discussion
The main discovery in this study is that MG-H1 is positively associated with inflammation in children and adolescents with diabetes, but not arterial stiffness or wall thickness. Interestingly, this was not the case in the control group. This might be because production of AGEs is only damaging in diabetes, but we find this unlikely. As glycolysis is at the core of human metabolism, AGEs like MG-H1 become unavoidable by-products. This explains why cells have dedicated enzymes, like the glyoxalase system, to handle such reactive and dangerous compounds. 18 It is therefore more likely that the natural process of atherosclerosis is accelerated by diabetes and that 13.2 years of age is too early to detect the effects of AGEs in healthy control subjects. The diabetes patients had a mean disease duration of 5.5 years, and the fact that we find an association with MG-H1 this early in the atherosclerotic process suggests that AGEs are important in the pathogenesis.
The pathogenesis of atherosclerosis is not completely understood. Entities like arterial stiffness and inflammation become intertwined with many risk factors, and in the adult human, it is very difficult to ascertain which are the true propagators of the disease. 19 In childhood, however, the exposure to risk factors like increased blood pressure, obesity, smoking, decreased physical activity and hyperlipidaemia is less likely yet to have had an impact. This makes studies of atherosclerosis in this age group particularly interesting.
This study confirms previous reports20,21 of increased levels of AGEs in children and adolescents with T1D, even in patients with young age, short duration of disease, intensified insulin treatment and blood glucose control that is representative for patients in a clinical setting. We also found a significant positive correlation with HbA1c in the diabetes group, where previous studies have been conflicting.20,21
There are several proposed mechanisms for AGEs to influence atherosclerosis development – one being that cross-linking of collagen and elastin in the arterial wall may lead to increased arterial stiffness. 22 Increased concentrations of methylglyoxal that lead to the formation of increased MG-H1 may also be associated with increased methylglyoxal-derived cross-links such as MODIC. 23 We were, however, unable to confirm an association between MG-H1 and arterial stiffness. Another mechanism is that AGEs can contribute to inflammation, at least in part, by binding to the receptor for AGE (RAGE) and subsequently increasing levels of the nuclear transcription factor nuclear factor (NF)-κB. 24 RAGE is expressed on the surface of several of the cell types in the arterial wall, 25 and binding leads to cellular activation and release of adhesion molecules and pro-inflammatory cytokines. 26 RAGE has several ligands, and the importance of the AGE/RAGE interaction in the pathogenesis of atherosclerosis is not quite certain. Furthermore, whether MG-H1 is among the AGEs that are able to activate RAGE is debatable and an issue that needs further study.7,27 It may be more likely that activation of RAGE by other ligands downregulates glyoxalase-1 and thereby increases methylglyoxal and MG-H1 concentrations. 28
Carotid IMT was slightly increased in the diabetes group and significantly so in boys, but we also expected to find a positive relationship with MG-H1. There was, however, a minor but significant inverse relationship between MG-H1 and cIMT. Thus, both increased wall thickness and arterial stiffness seem to develop later than inflammation.
Among others, hypertension and increased cholesterol levels are associated with the development of atherosclerosis and cardiovascular disease in adult humans. 19 In this study population of children and adolescents, however, we found no such relationship regarding cIMT and Young’s modulus – not even in the diabetes group, where many traditional risk factors were more pronounced. 15 We did, however, find that both triglycerides and BMI were significantly associated with CRP in the diabetes group, and BMI also in the control group. That the effects of traditional risk factors on atherosclerosis increase with time is not surprising and has been shown in the Pathobiological Determinants of Atherosclerosis in Youth (PDAY) study. 29 In our study, the mean age of all participants was 13.6 years, and this seems to be too early to detect the detrimental effects of most of the traditional risk factors.
Previously, increased levels of AGEs in cigarette smoking individuals have been described. 30 Interestingly, we also observe this, although our patients necessarily have a relatively short history of cigarette smoking. The possible combined effects of cigarette smoking and diabetes on AGEs and atherosclerosis are intriguing. However, as this study was not designed to explore these relationships, the number of smokers was too small to draw any reliable conclusions.
There are several limitations to this study. AGEs can have harmful effects both intracellularly and in the extracellular matrix. In this study, we only measured MG-H1 in serum, and we cannot be certain that the levels truly reflect the chemical reactions taking place in the arterial wall. The serum levels reflect both protein-bound and free MG-H1 adducts. The amounts and affinity for each are unknown. Although the immunoassay response was found to correlate with detection of MG-H1 by stable isotopic dilution analysis LC-MS/MS, it is currently unknown how changes of MG-H1 estimation by our immunoassay compare quantitatively with those by LC-MS/MS. Further work on this is required. The levels of MG-H1 were lower than expected, possibly because a part of the immunoassay was conducted at pH 9.8, where the stability of MG-H1 is uncertain. Young’s modulus is an accepted way of measuring arterial stiffness, but it is not the gold standard. 31 Furthermore, the method requires blood pressure to be measured at the same site as the elastic parameters. We measured blood pressure in the radial artery, which introduces a small approximation. It is unlikely that this influences the results, as the procedure was the same in all subjects. The cross-sectional design of the study makes it impossible to prove any direction of causality.
In conclusion, this study shows that the most abundant AGE in human plasma, MG-H1, is increased in children and adolescents with diabetes of short duration, despite intensive insulin treatment. It further shows that MG-H1 is associated with inflammation at an early point in time, where the effects of most of the traditional risk factors for cardiovascular disease are still undetectable.
Footnotes
Acknowledgements
We would like to thank Eva Bressendorf Lindseth of Oslo University Hospital for her many contributions to this study.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The study was funded by the University of Oslo, where M H is an employee, and ExtraStiftelsen Health and Rehabilitation.