
Abstract
There are many pathologies and/or surgical situations where understanding how cutaneous capillary blood flow is behaving would be of clinical benefit. Laser Doppler imaging (LDI) has long been considered an ideal candidate for this yet was never widely adopted. The technology was deemed too slow, needing minutes to record one image. Here, we present the use of a new, real-time LDI, which is sensitive enough to resolve pulsatile blood flow in the microcirculation and can record images and videos instantaneously. We show that when comparing the ratios of absolute perfusion images from different regions of the body, remarkably reproducible data can be obtained when looking at a control population of male volunteers. In the future, we plan to add more control and diseased groups, effectively giving the clinician a non-invasive, safe and easy-to-use diagnostic for assessing the extent of microcirculatory disorders and high-risk surgical situations.
Introduction
The quality of cutaneous microvascular perfusion is directly linked to the severity of pathologies such as diabetes, rheumatologic diseases and hypertension and is considered one of the most important parameters when assessing the healing potential of wounds 1 and reconstructive surgical procedures involving tissue transfer. 2 Early and reliable identification of at-risk patients can help the physician decide between more and less aggressive treatment approaches and streamline patient care by assessing the efficacy of a particular treatment earlier than its physical effects are obviously manifested.
Although there are many techniques suitable for measuring cutaneous microvascular perfusion, no single technology has been widely adopted and clinical assessment remains the method of choice for the vast majority of clinicians. 3 The reason for this is multifactorial; for a technology to be relevant, it should be more accurate than clinical assessment, should be easy to use, should be non-invasive, should offer information rapidly and should be user independent. 4 Recent reviews have suggested that Doppler probes offer the best compromise between these parameters. 5 The primary drawbacks are that these probes require direct contact with the skin, their measurements are not highly reproducible if the probe is removed/reattached and the region sampled is very small (1 mm2). This can cause them to be highly affected by local variations in microcirculation. Laser Doppler imaging (LDI) offers an interesting solution to many problems associated with probes; they require no contact and give information over a much larger region (up to 2500 cm2). Previous LDI studies have proven their efficacy in research, 6 while routine clinical applications have been limited primarily to burn depth assessment. 7 The drawback with traditional LDI technologies has been the length of time needed to scan and reconstruct an image. Requiring minutes, they have been deemed too slow for use in many clinical applications.
The device used in this study (EasyLDI; Aïmago SA, Lausanne, Switzerland) was designed to address the issues of speed associated with LDIs of the past. The EasyLDI is CE marked, provides real-time laser Doppler perfusion images, is compact and can be operated much like a traditional point-and-shoot digital camera. The device illuminates a 7 × 7-cm2 region, providing images with 140-µm pixel resolution at a rate of 12 per second. 8 There is no health risk associated with exposure to the EasyLDI.
The goal of the present investigation is to use real-time LDI to study regional variations in microcirculatory perfusion in a group of healthy individuals. It is known that levels of absolute perfusion vary greatly at different regions of the body and among individuals even when carefully stratifying patient groups by age, sex, body mass index (BMI) and the presence of microcirculatory disorders. Thus, our approach was not to evaluate absolute measures of perfusion but to compare the ratios of absolute perfusion between certain body regions among individuals and from this to develop a body mapping methodology that is based on intra-individual perfusion ratios.
Research design and methods
Ethical approval and patient selection
Our study included one group of eight healthy male volunteers between the ages of 22 and 42 years. All volunteers are current Aïmago employees and signed an informed consent before imaging was performed. No one in our group was a smoker, hypertensive, diabetic or suffering from a rheumatologic disease. Patients refrained from eating food or drinking coffee on the morning of the imaging. Measurements were taken between 9 and 11 a.m., in a quiet room of temperature ranging from 21°C to 23°C.
Imaging procedure
Patients were laid flat on their back and encouraged to get as comfortable as possible. Imaging began 5 min later. When imaging was finished, the patient was rolled on to their stomach and measurements were repeated. Seventeen sites were identified on each patient (Figure 1(d)), and 10-s perfusion videos were recorded at each.
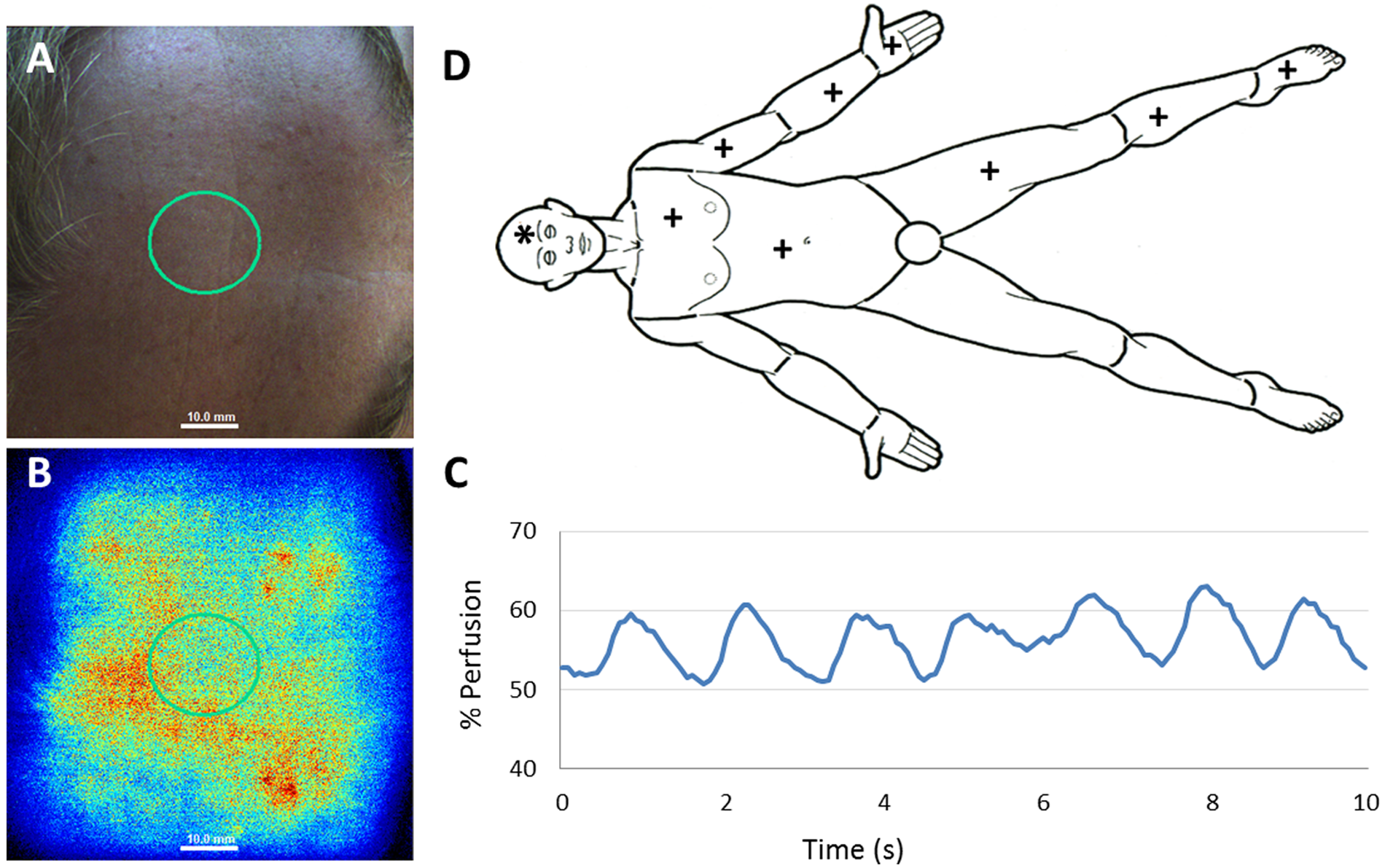
(a) Colour photo of the forehead region taken with real-time LDI camera; (b) sample LDI of forehead region; (c) graph of perfusion unit versus time from 10-s LDI sequence of forehead and (d) body map. The symbol ‘*’ indicates zone imaged and ‘+’ indicates both ventral and dorsal zones imaged.
Image analysis
Videos were grouped by body location for all patients. A region of interest (ROI) was defined manually for each 10-s video, delineating the largest possible area that was not affected by curvature. The average perfusion per unit per area of this ROI was then plotted and averaged over 10 s, giving an ‘average perfusion value’ for the particular body region of that patient. Average perfusion values can vary from a minimum of 0 to a maximum of 255 Aïmago Perfusion Units (APUs), and these values were normalized to a scale of 0%–100% to avoid confusion.
Statistical analysis
All multivariate analysis was carried out using analysis of variance (ANOVA), and interactions between pairs were assessed using the Tukey’s test. Values of p less than 0.05 were considered significant.
Results
Raw data analysis of ventral and dorsal data pairs from the same body region
Eight employees from the Aïmago team were imaged on 17 body locations as indicated in Figure 1(d). At each of these locations, a 10-s video of perfusion (Figure 1(b)) was saved along with the corresponding colour photograph for future location identification (Figure 1(a)). For each video sequence, a ROI was manually defined and applied to the same location for all images in the video sequence. Next, the average perfusion unit per unit area of the ROI was plotted versus time (Figure 1(c)). Here, microcirculatory pulsations can be visualized and average perfusion can be calculated for the defined sequence. Any large variations due to patient movement from the normal pulsation profile, for example, can be easily seen, indicating that the perfusion video is not valid and a new sequence should be recorded.
For each of the eight patients, an average perfusion value per unit area was calculated for the 17 body zones imaged. Data were grouped according to the body zone, and ANOVA statistical analysis followed by Tukey’s test was performed to look at data sets with significant interactions (data not shown). Ventral and dorsal interactions of all body parts imaged (excluding the hand) were shown to have non-significant interactions.
Data regrouping for non-significant ventral and dorsal interactions of the same body region
Data were regrouped into 10 groups, pairing ventral and dorsal data sets for all body regions except for the hand. The means and standard deviations of these data are shown in Figure 2.
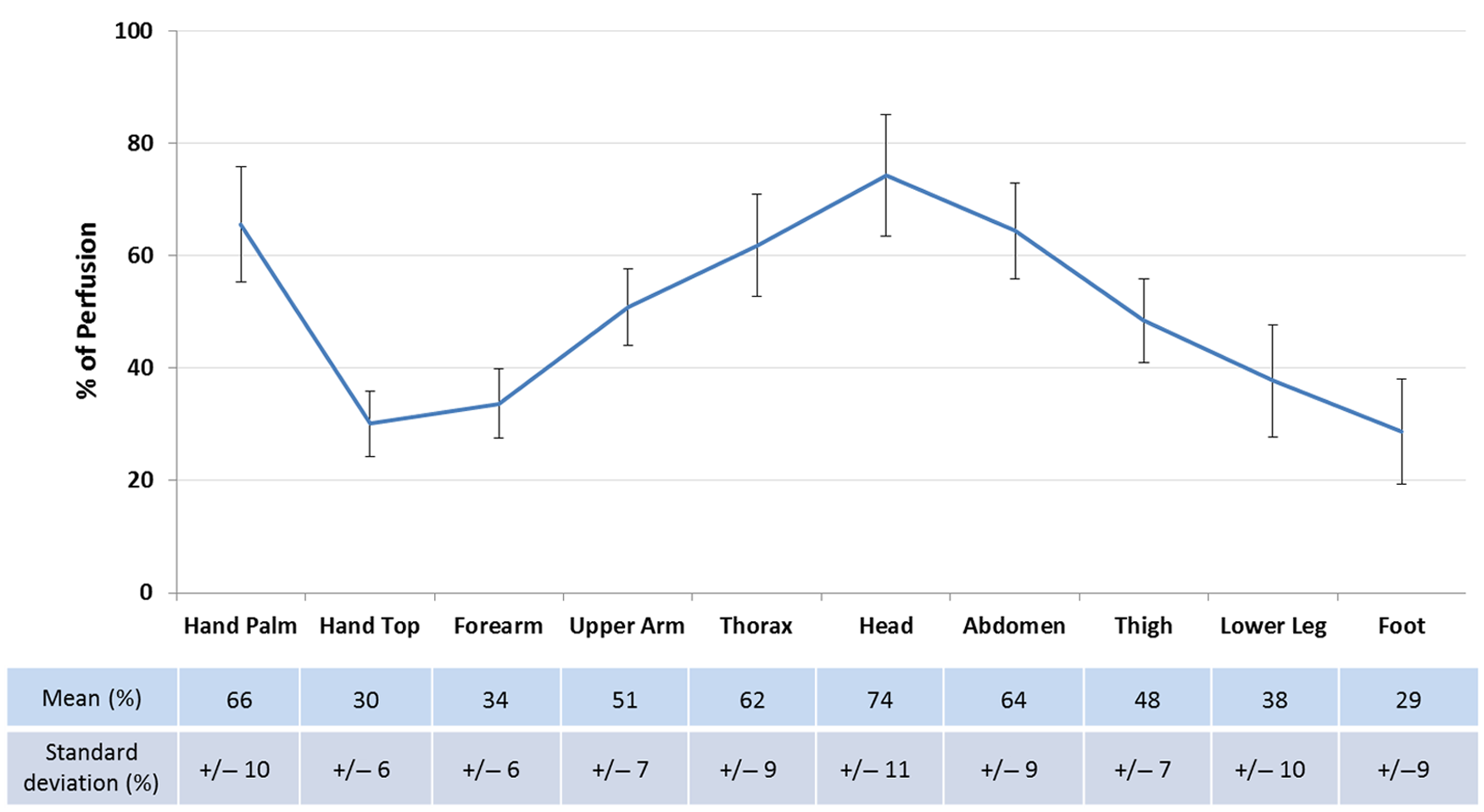
Regrouped ventral + dorsal control group data (except for hand, as indicated).
Next, ANOVA statistical analysis, followed by Tukey’s test, was performed again on the regrouped data (Figure 2) to test which data pairs have significantly different interactions. All significantly different data pairs and their corresponding mean ratios are shown in Table 1 (p < 0.01, the symbol ‘*’ indicates 0.01 < p < 0.05).
A table explaining the multiplication factors necessary to use a non-corresponding reference zone when imaging. All values of p < 0.01, the symbol ‘*’ indicates 0.01 < p < 0.05.
To use these data practically, Table 1 indicates that the average perfusion of the forearm of a healthy patient (‘reference’ axis) should be multiplied by a factor of 2.21 to predict the perfusion on the forehead of the same patient (‘site for comparison’ axis). These types of regional relations can be made at all intersections of the x- and y-axes of Table 1, with the percentage value indicating the interaction-specific correction factor.
Discussion
In the present study, we have shown that although absolute perfusion may vary among patients, intra-individual perfusion ratios between body regions are significantly distinguishable from one another. Of the 10 independent data sets analysed, there are possibilities to have 45 total independent data pair interactions. We have demonstrated that 32 of the 45 possible pairs are significantly different from one another and included the corresponding ratios of their means in Table 1.
What makes these results particularly interesting is that they indicate that although as individuals we may have varying degrees of absolute perfusion, when considering the same body regions, the relative intra-individual ratios of perfusion between body regions are in fact very similar. Thus, we have determined a way to use intra-individual relative imaging to ‘normalize’ perfusion data, minimizing variations that have plagued the use of absolute LDI perfusion imaging in the past.
This suggests that a larger study, incorporating different age groups, sex and BMI, should also show significant perfusion ratios between body regions. Understanding what Figure 2 would look like for these groups, as well as diseased populations, such as those with diabetes, rheumatic disorders and hypertension, would provide the foundation necessary to begin using real-time LDI as a reliable tool in determination of the disease extent, progression/regression and efficacy of applied treatments. Increased quantity and improved quality of data will also open the doors for more rigorous analysis methods such as investigating how the pulsation profile changes with body region (Figure 1(c)) and functional imaging integrating capillary response to physical or chemical stimuli.
Unlike other laser Doppler technologies, such as single point probes, which require contact with the patient, or scanning imagers, which need minutes to create an image, the Aïmago technology operates in real time. We hope that these significant technological improvements will open the doors for a renewed interest in the use of LDI for microvascular disease research, providing relevant and reliable perfusion data that can be utilized in a wide variety of applications. We are confident that once expanded upon, our study will be able to provide a new diagnostic vision and increased diagnostic certainty in a wide variety of surgical and non-surgical applications.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
Tyler Thacher and Pascal Harbi performed this study while under the employment of Aïmago SA, Lausanne, Switzerland, but have no financial motivation for publishing this study.