
Abstract
Introduction
Care partners of persons with dementia provide about 18.6 billion hours of unpaid care per year which is significantly higher compared to non-dementia care partners (Alzheimer’s Association, 2023). Prolonged periods of intense care often lead to high rates of stress-related health problems (Sörensen & Conwell, 2011). Additionally, care partners often neglect their own health to provide care for the person with dementia (Cheng, 2017; Gao et al., 2019; Richardson et al., 2013; Vara-García et al., 2019). The consequences of prolonged caregiving demands included worsened physical health (e.g., reduced sleep quality and high blood pressure) and emotional wellbeing (e.g., increased anxiety, depression, and loneliness) as compared to care partners of people with other conditions (Cheng, 2017; Gao et al., 2019; Richardson et al., 2013; Vara-García et al., 2019). As compared to non-spousal care partners of persons living with dementia, spousal care partners experience more negative effects including increased rates of depressive symptoms (Harris et al., 2021; Sallim et al., 2015), higher levels of burden (Kim et al., 2012), accelerated cognitive decline (Dassel et al., 2017), lack of social relationships (Tatangelo et al., 2018), and reduced quality of life (de Oliveira, 2015; Farina et al., 2017). As the population ages, there is an expected rise in the number of persons living with dementia and informal care partners including spousal care partners (Nordtug et al., 2021). Due to this trend and the higher intensity of care needed for persons with dementia, it is critical to provide extra support to spousal care partners in order to optimize health and emotional wellbeing.
Care partner physical activity has been shown to improve physical, emotional, and social health (Hirano et al., 2016; Hirano, Suzuki, Kuzuya, Onishi, Ban, et al., 2011; Hives et al., 2020; Prieto-Prieto et al., 2022). Increased levels of physical activity in care partners can reduce stress, levels of depression, perceived care partner burden, and improve sleep quality (Hirano et al., 2016; Hirano, Suzuki, Kuzuya, Onishi, Ban, et al., 2011; Hives et al., 2020). Barriers to physical activity in spousal care partners include their own mental and physical health (Etkin et al., 2008; Hirano, Suzuki, Kuzuya, Onishi, Ban, et al., 2011; Hirano, Suzuki, Kuzuya, Onishi, Hasegawa, et al., 2011; Marquez et al., 2012), increased burden due to caregiving (Hirano, Suzuki, Kuzuya, Onishi, Hasegawa et al., 2011), and lack of time to engage in their own self-care (Etkin et al., 2008).
A recent systematic review indicated that spousal care partners are more interested in participating in physical activity with their care recipient rather than exercising alone, resulting in more time together and increased social support (Doyle et al., 2020). However, the majority of dyadic physical activity interventions in care partners of persons with dementia and their care-recipient focused on the impact of exercise on care-recipient outcomes such as quality of life (Barnes et al., 2015), neuropsychiatric distress (Teri et al., 2003), and cognitive and physical function (Vreugdenhil et al., 2012). Some dyadic physical activity interventions focused on care partner outcomes such as care partner burden (Barnes et al., 2015; Lowery et al., 2014). Challenges associated with these trials include cost and time as the exercise strategies required travel to a medical clinic/community site for supervised exercise training (Frederiksen et al., 2014; Yu et al., 2015) or required home visits by exercise specialists (Lowery et al., 2014; Teri et al., 2003).
In recent years, there has been growing research attention on the efficacy of mobile applications (Wang et al., 2022). These mobile applications, known for their ease of use, affordability, and accessibility, have demonstrated their effectiveness in promoting physical activity among older adults (Elavsky et al., 2019; Sohaib Aslam et al., 2020; Yerrakalva et al., 2019). Systematic reviews have shown that mobile applications have been used to track steps, send personalized exercise messages, offer instructional workout videos, and set goals to boost activity in older adults (Elavsky et al., 2019; Sohaib Aslam et al., 2020). However, limited studies have examined joint activities through mobile applications, particularly involving spousal care partners of persons living with dementia and their care-recipient.
Therefore, the purpose of this study was to explore the perceptions of spousal care partners of persons with dementia and their care-recipient on the design and content of a mobile application intended to promote physical activity. This study will provide a deeper understanding into what elements of a mobile application could encourage physical activity engagement among spousal care partners of persons with dementia their care-recipient.
Methods
Design
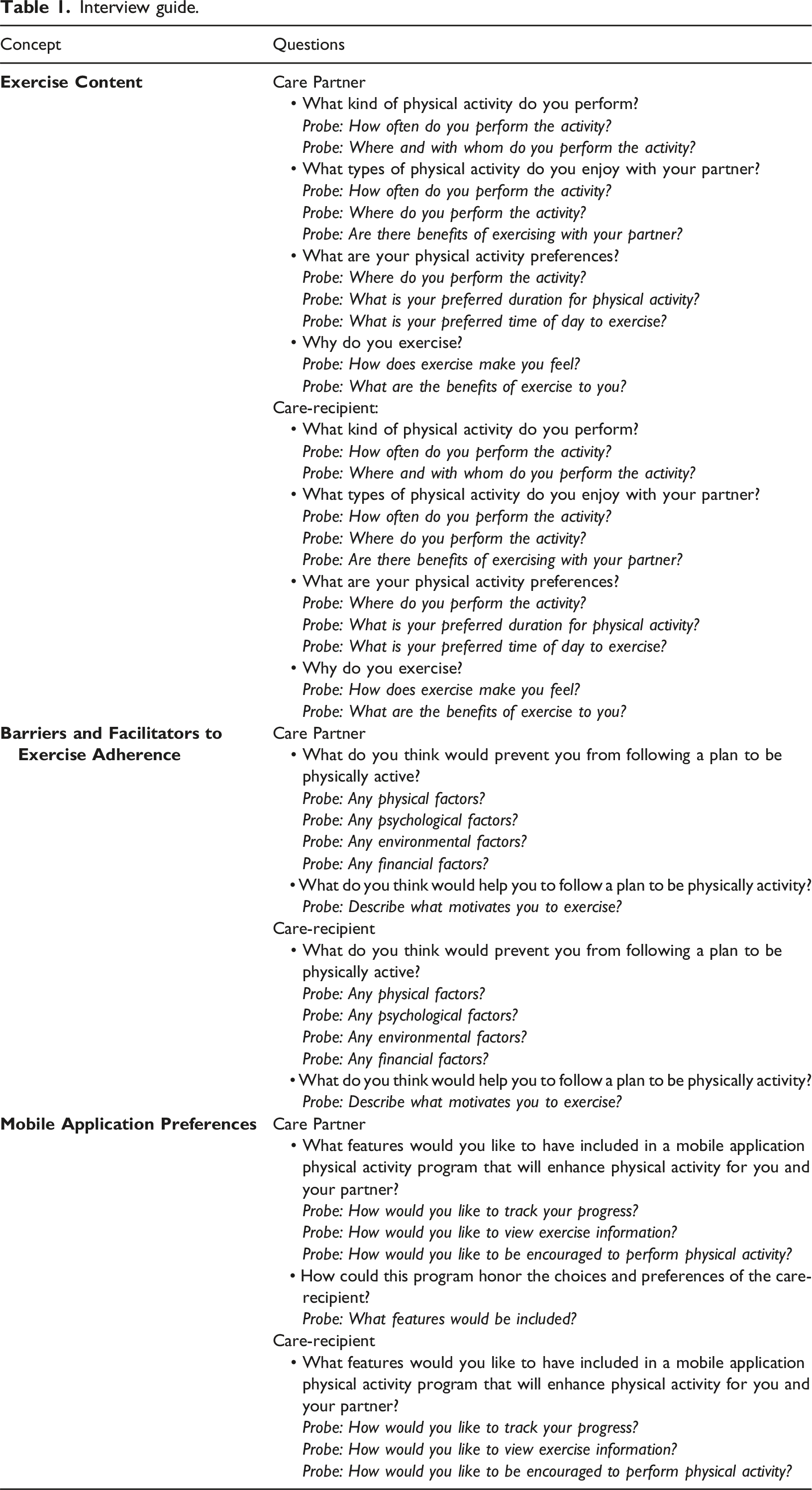
Interview guide.
Participants
The sample in this study included 14 dyads residing in Pennsylvania who were recruited through social media (i.e., Twitter, LinkedIn, and Facebook) and community outreach (i.e., senior centers). Inclusion criteria for the care partners were: 1) 55 years of age or older, 2) English speaking, 3) lived in the community, 4) spouse or partner to the care-recipient, 5) lived at home with the care-recipient, and 6) primary care partner of care-recipient.
Inclusion criteria for the care-recipients were: 1) 55 years of age or older, 2) English speaking, 3) screened positive for dementia with a score of two or higher on the AD8 Dementia Screening Interview (Galvin et al., 2006), and 3) had mild to moderate dementia (score of 0.5–2.0) based on the Clinical Dementia Rating Scale (Morris, 1997). Care-recipients were excluded if they: 1) planned to transition to residential care (e.g., assisted living or nursing home) in three months or less, 2) had end-stage disease (e.g., bed-bound, noncommunicative, or on hospice), 3) had history of major psychiatric and or/personality disorder, and 4) had history of major surgery in the past three months.
Procedure
A trained doctoral student, proficient in qualitative research, conducted each of the semi-structured interviews in this study. Interviews took place over the telephone with both members of the dyad together, with each interview lasting about 45 minutes. The interviews were recorded, and a professional transcript service transcribed the audio recordings verbatim. The principal investigator checked each transcript for accuracy. We continued interviews until we determined that data saturation had been achieved, indicating that no new data or themes were emerging (Johnson & Christensen, 2014). Each couple received a $50 gift card for completing the interview. Data was collected between December 2022 to May 2023.
Data analysis
We performed a thematic analysis following the approach outlined by Clarke and Braun (2017), which encompassed coding the data, categorizing codes into themes, and exploring the connections between these themes. We also analyzed descriptive statistics for both care partners and care-recipients. Analysis occurred after the transcription of each interview. We used MAXQDA 2022 (VERBI Software, 2022) to code and analyze the qualitative data.
Two researchers independently coded the data for each interview, and the initial codes were shared with the rest of the research team for discussion. The coding process consisted of iterative stages, involving repeated cycles of refining the codebook until a consensus was attained by the research team. The primary coders then categorized the codes into themes and subthemes. The research team participated in validating these themes and subthemes. To ensure trustworthiness of the data, we followed the guidelines of Lincolin and Guba (1985) by maintaining a comprehensive codebook that documented initial categories, definitions, and ongoing analysis decisions (audit trail). Investigator triangulation was achieved through coding audits, thorough reviews, and collaborative team consensus on findings and themes.
Results
Care partner and care-recipient characteristics (N = 14).
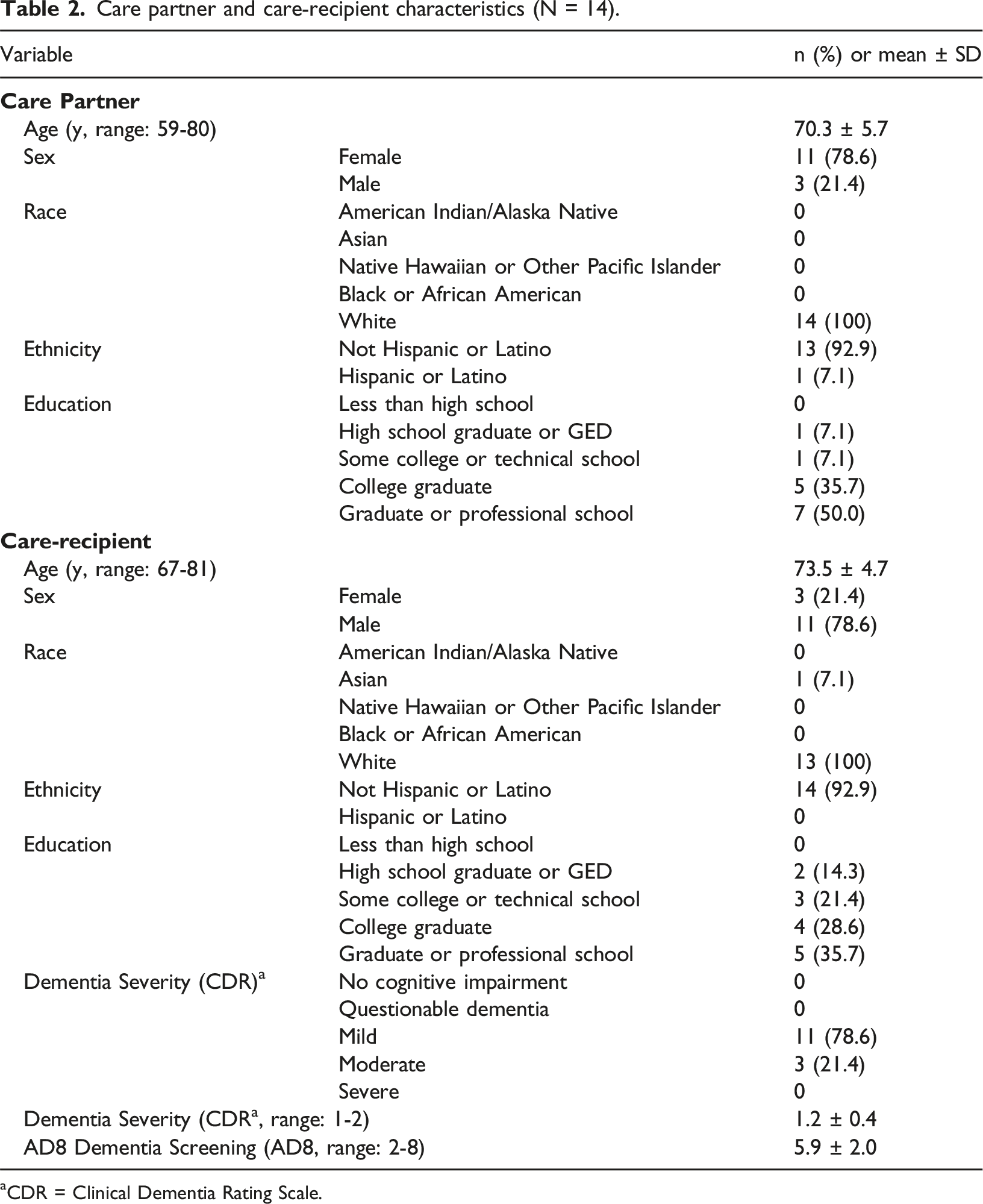
aCDR = Clinical Dementia Rating Scale.
Theme 1: Exercise preferences and habits
The first theme from the interviews was related to the participants’ exercise preferences and habits. This theme includes three subthemes: personal preferences and activities, frequency and routine, and partner involvement.
Personal preferences and activities
Care partners and care-recipients shared a range of exercise preferences that give insight into their individual choices. The most common choices were “walking” and engaging in “yard work” for both the care partner and care-recipient. These activities offer accessibility and the chance to incorporate physical activity into daily life. Beyond the most common choices, the participants’ interests span a wide range of activities, showcasing their diverse preferences. One care partner (#3), for instance, expressed a passion for both “basketball and softball,” highlighting their interests in team sports, and their desire for a more dynamic and interactive exercise routine. Examples of other individual activities the participants reported were: “I'm an avid cyclist, both riding roads, trails, and indoor cycling as well. I do a good bit of hiking and walking as well.” (Care partner, #1) “I really enjoy swimming and water aerobics, especially in the summer.” (Person with dementia, #12) “If I could choose an exercise that I really liked, I like dancing.” (Person with dementia, #7)
Frequency and routine
The insights gathered from the participants shed light on the frequency and timing of their physical activity engagement, revealing a range of routines. Some participants prioritize exercise “a few times a week,” emphasizing consistency over intensity. Other participants have adopted a structured approach, aiming to exercise “twice a week” as a manageable goal. For example, one care partner enthusiastically shared, “We love to do that [walking at community park] twice a week” (Dyad, #14).
Conversely, some participants embrace a daily exercise routine as a cornerstone of their lifestyle. As one care partner highlighted, “We try to do it [walking] every day. We try to take one, at least a 20-minute walk with the dog” (Dyad, #5). Furthermore, the diversity of activity timing was apparent among the participants, with engagement spread across the morning, afternoon, and evening.
Partner Involvement
Several of the participants highlighted their preference for exercising alongside their partner. This shared activity brought them closer and made the exercise experience more “enjoyable.” Some of their responses are as follows: “We love to work in the garden together.” (Dyad, #13) “Probably the only thing we do together is walk.” (Dyad, #1) “We bicycle on trails, do yard work.” (Dyad, #9)
The recurring message from the participants is that engaging with their partner in exercise is a “meaningful” aspect of their routines. This connection not only strengthens their bond but also adds to the “motivation” for staying active.
Theme 2: Barriers to exercise
The second theme from the interviews was related to barriers to exercise. The subthemes described were physical and mental health, weather, and lack of time.
Physical and mental health
Care partners and care-recipients revealed how physical health challenges significantly impact their exercise routines. These challenges, including chronic pain, fatigue, arthritis, allergies, and asthma, play a crucial role in shaping participants’ ability to stay active. Moreover, participants acknowledged the interplay between their mental health and exercise engagement, highlighting how emotional wellbeing is closely tied to staying active. For example, a care partner (#7) stated, “He doesn’t want to do them [exercise]. He gets to the point where he gets depressed, and he don’t want to do them.”
Weather
The influence of weather on participants’ exercise decisions and routines emerged as a unanimous subtheme throughout the interviews. For example, one care partner (#6) noted, “If the weather is dreary and it’s not inspiring or it’s drizzling, it’s cloudy. We don’t get to exercise. We got so much of that here.”
Lack of time
The concept of a “lack of time” as a hindrance to physical activity was a prevalent and relatable subtheme raised by multiple participants. Their insights provide a deeper understanding of how busy schedules can directly impact their exercise routines. For instance, one care partner (#11) expressed, “I get busy with other things and then it [exercise] falls by the wayside.” This underscores the challenges of juggling that many individuals, especially care partners, face in balancing various responsibilities. Similarly, another care partner’s (#10) perspective: “I’m busy, so I’d rather if I could take something off my schedule, it would be exercise.” This statement reflects the competing demands that exist within care partners’ daily lives and how exercise might be perceived as expendable when faced with numerous commitments.
Theme 3: Motivations for exercise
The interviews revealed a third theme that was related to factors that motivate exercise. The subthemes identified include physical and mental wellbeing, and social interaction.
Physical and mental wellbeing
Physical and mental wellbeing were highlighted by participants as reasons for exercising. One participant noted, “Because I know that it's [exercise] good for my physical health and for my brain health” (Care partner, #9). This insight resonated with another participant who shared, “I think it [exercise] helps my mind as well as my body. It makes me feel better and more alert” (Person with dementia, #7). These responses collectively reflect a recognition of the integral link between physical and cognitive wellbeing, reinforcing their motivation to engage in regular exercise.
Social interaction
Several dyads expressed that they exercise because it gives them an opportunity to socialize with others. For example, one care partner (#2) stated, “I enjoy doing things with people, so there’s a social element to what motivates me.” Additionally, participants highlighted their enjoyment of being with others while taking walks. As one care partner (#5) pointed out, “Socializing with neighbors during walks also contributes to our motivation.”
Theme 4: Mobile application preferences and supportive features
The interviews revealed a fourth theme related to participants’ mobile application preferences and the supportive attributes they seek in the development of a mobile application to promote physical activity. This theme encompassed several subthemes: reminder and tracking, customization and accessibility, motivational features, and personalized features.
Reminder and tracking
Some participants expressed their desire for mobile application features that serve as a virtual journal. This feature would help them track their exercise progress, including health data like heart rate and step counts. For instance, a care partner (#14) mentioned, “I guess something like a journal part of it where you can keep track of what you’ve done, your progress, and I guess the health aspects, like heart rate and how many steps you’ve taken.”
Customization and accessibility
Participants emphasized the importance of the mobile application being easily readable, reflecting their need to clear and legible text within the mobile application. For example, one care partner (#1) said, “Well, I would like it to, if I have to read it, I’d like it to be large enough text that I can actually read it.”
Motivational features
Participants expressed interest in incorporating motivational features within the mobile application. One participant emphasized the value of seeing their accomplishments in a tangible way, stating, “Then when you look at it [the app] and you say, ‘Oh, look what I did. I did five days of exercise, five days' worth of exercise this week.’ And it inspires you” (Care partner, #9).
Participants also pointed out the psychological benefits of progress tracking. For example, participants highlighted the positive reinforcement aspect that can boost motivation by acknowledging and celebrating users’ achievements through the mobile application’s interface. For example, a care partner (#10) commented, “I do like to see the chart of my progress [regarding exercise], so I can think, oh, I was successful, so sometimes the app rewards me and says, ‘You’re good. You did it.’”
Further, several participants recognized the potential of the mobile application to positively impact people living with dementia. For instance, one care partner (#13) noted, “Well, I think that the app should encourage him to go outside and exercise, because when people with dementia are with other people, they don’t feel as depressed, because they’re out there with others.”
The perspectives underline the role of the mobile application not only promoting physical activity but also enhancing the emotional wellbeing of individuals.
Personalized features
Participants highlighted the significance of personalized features that cater to individual characteristics. One participant explained, “Catering it [the app] to what the person is physically able to do…so not making a one size fit all for everyone” (Care partner, #2).
Participants also expressed their desire for features that offer gently reminders or prompts, demonstrating their preference for personalized and adaptable interactions with the mobile application. For instance, a care partner (#8) highlighted a specific example of a personalized feature they would find useful, saying, “Just a text or something, or a message that says… Like my smartwatch, it says it’s time to stand up.”
These examples underscore the participants’ strong desire for mobile application features that consider and adapt to each person’s unique abilities and needs, rather than adopting a generic approach.
Discussion
This study explored the perceptions of spousal care partners of persons with dementia and their care-recipient on the design and content of a mobile application aimed at improving physical activity. The interviews revealed four primary themes: exercise preferences and habits, barriers to exercise, motivations for exercise, and mobile application preferences and support features.
In the exploration of the first theme, it is evident that participants presented a wide array of solo performed exercise preferences and routines. Among both care partners and care-recipients, walking and yard work emerged as common choices, indicating accessibility and practicality in daily life. These results are consistent with other research where walking and gardening ranked as the most common activities among older adults without cognitive impairment (Kuzmik et al., 2023). Yet, within this overarching similarity (i.e., walking and yard work), our findings also found notable variations in participants’ exercise choices (e.g., team sports, cycling, and dancing). This divergence is indicative of the diverse nature of exercise preferences and interests between care partners and care-recipients.
Interestingly, where individual preferences diverge, there are also opportunities for joint activities that can bridge these differences. The subtheme of “Partner Involvement” revealed that several participants expressed a strong inclination toward engaging in exercise alongside their partner. This shared experience not only brought them closer but also enhanced the enjoyment of the activity, a finding also supported by previous research (Doyle et al., 2020). Thus, this aspect holds potential implications for mobile application content development, suggesting that while individual preferences may diverge, the motivation to exercise could be bolstered by creating opportunities for joint participation in activities that align with diverse preferences.
The second theme highlighted crucial challenges that care partners face in maintaining regular physical activity. Aligning with previous studies involving informal care partners or care-recipients in various settings (Farina et al., 2021; Gebhard & Mir, 2021; Telenius et al., 2022), the participants identified physical and mental health, weather, and lack of time as barriers to exercise. Our findings emphasize the significance of incorporating flexibility and adaptability into the features of a mobile application. This would allow users to adapt their routines according to varying health circumstances and external influences. To illustrate, a future mobile application could offer a range of workout options in its library, catering to different levels of health conditions, thereby ensuring inclusiveness and safety for both care partners and care-recipients. Furthermore, a mobile application could include adaptive routines that accommodate weather-related constraints and time limitations. For instance, indoor exercises might be suggested on rainy days, and quick workout options could be provided for users with busy schedules.
The third theme reflected participants’ motivations for exercise, encompassing physical and mental wellbeing as well as social interaction. Our findings align with existing literature which also found factors like physical health (e.g., maintaining function), mental wellbeing (e.g., reducing stress) and social connectedness can serve as motivators for physical activity among older adults with dementia or their family care partners (Farina et al., 2021). Participants’ recognition of the interconnectedness of physical activity and mental health indicates that a mobile application should emphasize the holistic benefits of exercise. Thus, alongside conventional fitness metrics (e.g., weight, heart rate, and body mass index [BMI]), a mobile application could incorporate holistic wellbeing indices, measuring factors like mood, energy, and cognitive function. As users witness improvements in both physical and mental aspects, their motivation to engage in regular exercise could be reinforced. Further, the participants’ desire for social interaction suggests that a mobile application could potentially include-building elements, such as virtual group activities or challenges, to facilitate engagement and foster a sense of friendship among users.
The fourth theme, which focused on mobile application preferences and supportive features, provided insights into the participants’ expectations for designing a mobile application to promote physical activity. In general, the participants emphasized the importance of prioritizing personalization and a user-centric approach in the development of a mobile application to encourage physical activity. Specifically, customization and accessibility emerged as important considerations, indicating the need for clear and legible text as well as personalized settings to accommodate users with varying needs. Some participant’s also expressed a desire for a virtual journal feature, reflecting the growing trend of using technology to track health data and progress (Peng et al., 2016).
In addition, motivational features were highly valued by participants, suggesting that a mobile application could effectively serve as a source of inspiration and reinforcement. Particularly noteworthy was a mobile applications potential to positively impact emotional wellbeing, especially for individuals with dementia, thus underlining a mobile applications potential to enhance overall quality of life. Lastly, the emphasis on personalized features underscores the importance of tailoring mobile application interactions to individual capabilities and preferences. The incorporation of gentle reminders and prompts align with theory-based behavior change techniques, which serve as the essential components of mobile interventions designed to modify the underlying processes that regulate behaviors (Michie et al., 2013).
Implications for future directions
The findings provide actionable insights that can guide the design, development, and refinement of a mobile application to promote physical activity in spousal care partners of persons with dementia and their care-recipient. Overall, to address diverse preferences in exercises, a mobile application should offer a wide range of activities and prioritize joint engagement, recognizing the value of shared experiences. Adaptable features are also essential to help users over barriers such as health concerns and weather limitations. Additionally, a mobile application’s potential to enhance holistic wellbeing can be leveraged to motivate users and reinforce the benefits of exercise. Finally, emphasizing personalization and user-centric design, while integrating motivational elements like reminders, can create a user-friendly mobile application that effectively supports spousal care partners of persons with dementia and their care-recipient in maintaining regular physical activity and improving their quality of life.
Strengths and limitations
A strength of this study was the rigorous approach to data collection and analysis, involving two coders, purposive recruitment, member checking, and data triangulation (Creswell & Creswell, 2017).
Our study had limitations. Spousal care partners and care-recipients were recruited from a single state, and our sample was predominantly White, limiting generalizability. Additionally, the study only focused on individuals with mild-moderate dementia, thus excluding persons with severe dementia and their care partners. Future research should include racial and ethnic diversity in participants, and spousal care partners of persons with more advanced dementia and their care-recipient to capture diverse needs and perspectives. Additionally, given that the interviews involved both members of the dyad, it is possible that some participants may have restrained their viewpoints to avoid upsetting their family members.
Conclusion
The themes that emerged from the participants’ responses offer preliminary understanding of the factors influencing exercise behaviors and mobile application preferences. These insights lay the foundation for designing an effective user-friendly mobile application to promote physical activity that caters to the diverse needs, preferences, and challenges among spousal care partners and their care-recipient. Future research is warranted to further explore the perceptions of spousal care partners and their care-recipient on the design and content of a mobile application to promote physical activity across diverse cultural and geographical contexts.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research funds from the Pennsylvania State University, Ross and Carol Nese College of Nursing, Tressa Nese and Helen Diskevich Center of Geriatric Nursing Excellence.