
Abstract
Improving supports to enhance wellbeing of people living with dementia is a priority. Engaging people living with dementia, care partners, and other stakeholders in development of interventions increases the likelihood they will be relevant and impactful. We describe the participatory approach used to co-design the Dementia Lifestyle Intervention for Getting Healthy Together (DELIGHT) program, which aims to promote the health and wellbeing of people living with dementia and care partners. The DELIGHT project was guided by a team of researchers, people living with dementia, care partners, and an Alzheimer Society representative. The co-design team included additional people living with dementia, care partners, exercise professionals, dietitians, health care professionals, and community service providers (n = 29). The co-design was planned for in-person but was transitioned to six online, 1.5-h sessions due to COVID-19 related restrictions. We used breakout rooms for discussion, with people living with dementia in each breakout room. Co-design meetings focused on identifying target population and outcomes and developing program components and structure. Two or three guiding questions focused discussion in each meeting. The final co-design session focused on the overall structure of the DELIGHT program. Program resources were iteratively designed with the research team, co-design team, and other external stakeholders. The result of the co-design process was the DELIGHT program, an 8-week, twice weekly program designed to promote living well with dementia for people living with dementia and care partners. Each session includes 50–60 minutes of exercise and 20–30 minutes of facilitated, shared learning with an associated resource. A healthy snack may be offered. Shared learning focuses on healthy eating, sleeping well, mental well-being, social connection, and physical activity. Our vision is that the co-designed DELIGHT program will promote the health and wellbeing of people living with dementia and care partners, increasing the likelihood of living well with dementia.
Keywords
Introduction
The World Health Organization estimated that more than 55 million people lived with dementia worldwide in 2022, with 10 million new people developing dementia each year (World Health Organization, 2022). Dementia is characterized by cognitive changes that are sufficient to interfere with independence in everyday activities and can result from a variety of pathophysiologies (American Psychiatric Association, 2013). People living with dementia may also experience diverse changes affecting physical function, sensory processing, emotions, and behaviour (American Psychiatric Association, 2013). The clinical management of dementia typically focuses on limited pharmaceutical treatments for cognitive deficits alongside preparation for end-of-life (Public Health Agency of Canada, 2019). While emerging pharmaceutical treatments offer some optimism for the treatment of Alzheimer’s disease, these treatments remain well short of a cure, come with significant side effects, and do not apply to all causes of dementia (Chertkow et al., 2021). To promote the health, wellbeing, and functional independence of people living with dementia, the development and implementation of effective nonpharmacological interventions is a priority of dementia research and practice (Bethell et al., 2018).
The United Nations Convention on the Rights of Persons with Disabilities (including people living with dementia) reinforces the notion ‘nothing about us, without us’ (United Nations, 2006). Accordingly, people living with dementia have a right to be involved in designing interventions, programs, and services that target them, including nonpharmacological interventions. Participatory, co-design processes increase the likelihood that an intervention will be relevant, practical, and impactful (Dupuis, Whyte et al., 2012). Collaboration of people living with dementia, care partners, and people who provide care and services may have the additional benefit of strengthening relationships among people and groups, helping to overcome preconceptions related to stigma of dementia (Dupuis, Whyte et al., 2012; Dupuis, Gillies et al., 2012). Participatory approaches to intervention design are becoming more frequently promoted by research funding bodies and non-profit organizations (e.g., Alzheimer Society UK, Alzheimer Society of Canada, Canadian Institutes of Health Research) with the intention to improve the relevance and adoption of interventions in practice.
Multicomponent interventions—also known as a multifactorial, multimodal, or ‘cocktail’ interventions—are a common approach to reducing dementia risk (Hafdi et al., 2021). While dementia prevention and dementia treatment are often treated as two separate missions, it is reasonable to expect that a multicomponent approach would also be effective for management of dementia, improving health, function, and wellbeing, especially if enacted shortly after diagnosis (Rao et al., 2023). Physical activity and healthy eating are core features of health promotion initiatives and show promise for the management of dementia (Casas-Herrero et al., 2019; Quail et al., 2020). People with dementia who take up physical activity have better functional ability, fitness, and mobility compared to those who remain sedentary (de Souto Barreto et al., 2021). In addition, physical activity interventions are associated with improved cognitive outcomes among people living with dementia (Dominguez & Barbagallo, 2018; Morris et al., 2017). Nutrition interventions can also promote health and function, regardless of dementia severity (Volkert et al., 2015). Of note, a program of physical activity and health eating is likely to also benefit care partners, as these are both central aspects of health promotion and public health strategies (e.g., Public Health Agency of Canada, 2019; World Health Organization, 2023).
A multicomponent lifestyle intervention may be a complementary approach to other programs with shared aims (i.e., health, function, and/or wellbeing). For example, the Promoting Independence in Dementia (PRIDE) and the Valuing Active Life in Dementia (VALID) interventions include education alongside meetings with an advisor or occupational therapist to set and enact goals related to activity and/or lifestyle (Wenborn et al., 2021; Yates et al., 2019). Interventions that incorporate social engagement through a group format may yield additional benefits such as feelings of social support, companionship, and sense of community (Phinney et al., 2007, 2016).
Here, our aim is to describe and reflect on the participatory process used to co-design the DEmentia Lifestyle Intervention for Getting Healthy Together (DELIGHT) program, a multicomponent intervention that aims to improve the health and wellbeing of people living with dementia and care partners. We describe our DELIGHT co-design process within three phases: (1) engaging the DELIGHT participatory research team; (2) refining the vision and scope of DELIGHT; and (3) co-design of the DELIGHT Program.
DELIGHT Participatory Co-design Process
The DELIGHT project was conceived by the primary investigators (LEM, HK, CM) following informal discussions and interactions with people living with dementia and their families, alongside knowledge of existing research and services. Priority setting processes (Bethell et al., 2018), talks given by people living with dementia, and informal conversations identified a need for supports to promote hope, health, and well-being among people living with dementia, especially soon after diagnosis. Roger Marple, a person living with dementia and dementia advocate said, “What if we started with hope? The learning process for dementia needs to include hope for living well and practical ways to achieve this. This should be taught first.” (Marple, 2019). This challenge captures the essence of our project aims.
Programs to empower people living with dementia through hope and by teaching strategies that promote health and wellbeing were not broadly available in Canadian communities and were only minimally addressed in existing research (e.g., Barnes et al., 2015; Salvà et al., 2011; Wenborn et al., 2021; Yate et al., 2019). As such, our draft objective for the DELIGHT project was to use a participatory approach to co-design, pilot, and evaluate a program that supports the health and wellbeing of people living with dementia and their care partners. The investigators envisioned a program that included physical activity, healthy eating, and social engagement, in part because of their own disciplines (health, kinesiology, and dietetics/nutrition) and also because physical activity and healthy eating are core to most public health and health promotion initiatives due to their connection to improved health and function across ages and conditions (e.g., Public Health Agency of Canada, 2019; World Health Organization, 2023). As described below, the inclusion of these core components was further confirmed by people living with dementia and care partners. By creating a program, the researchers also envisioned participants being able to learn from strategies and resources that had been useful to other participants.
Step 1: Engaging the DELIGHT Participatory Research Team
Our first step was to engage a participatory research team to confirm and evolve the project objectives and oversee all stages of the project. Identifying people living with dementia and care partners was a priority. We started with our networks and connections. We identified two people living with dementia, a current care partner (to one of the people living with dementia), and a former care partner who had demonstrated interest and enthusiasm for exercise and healthy living through their participation in related research, workshops, and/or programs. All four were invited to be part of the research team. Only one of these people (a person living with dementia) had previously participated in participatory research teams. While some of the invited members expressed uncertainty on whether and how they could contribute, they were assured that their lived experience of dementia was of great value to the project, alongside their diverse knowledge, skills, and experiences from other life roles. We additionally reached out to the local Alzheimer’s Society, as the primary organization delivering community-based programs and services to people living with dementia in our region, for a representative on the research team. They agreed to participate. Thus, when we first convened our DELIGHT research team in January 2020, the team was composed of two people living with dementia, two care partners, one community service provider, three academic researchers, as well as research trainees and staff (one undergraduate student, one graduate student, and one research staff member at the project outset). The research staff and trainees varied most over the course of the project, with these members moving on and off the team depending on university degree status, employment status, and skills needed. However, new staff and trainees that joined the project mid-way were often familiar with members of the research team and some members of the co-design team from dementia-related programs and/or projects, which facilitated collaboration and relationships.
The participatory approach used within the DELIGHT project was guided by the principles and enablers of Authentic Partnership, which were developed over a decade of participatory action research with people living with dementia and their families (Dupuis, Whyte et al., 2012). Authentic Partnerships are guided by three principles: (1) a genuine regard for the rights, personhood, and perspectives of each member; (2) synergistic relationships grounded in respect, trust, and shared learning among members; (3) a focus on process, remaining open and flexible to change, learning from mistakes, and new possibilities. The Authentic Partnerships approach described by Dupuis, Gillies et al. (2012) further identifies five enablers of authentic partnerships (Dupuis, Whyte et al., 2012). We describe our alignment with the enablers of Authentic Partnerships (highlighted in italics) in the following sections.
Early research team meetings focused on connecting the research team (Dupuis, Gillies et al., 2012). At the first meeting, we introduced ourselves and our connection to dementia and the project. We emphasized that the diverse experiences and perspectives amongst the research team were valued and encouraged team members to share their opinions and experiences openly. We aimed to create a safe space where each person felt that they could share their perspectives and experiences openly and that these were heard and incorporated in decision-making. We discussed how we would communicate to ensure clear and open communication and how and at what frequency we would meet. The research team meetings were set to monthly, with most people meeting in-person and one person living with dementia attending by Zoom as they lived in a different area of the province from the remainder of the team. The member attending via Zoom had used the platform extensively for other committees and research projects so felt confident attending in this way. Meetings were generally facilitated by one of the study investigators, with a staff or trainee taking notes. Perspectives of all members were purposively elicited at each meeting and incorporated into decision-making.
Step 2: Refining Project Vision and Scope
Another major aim of early meetings was to refine and commit to a shared vision for the project, including objectives and scope. At the very first meeting, we discussed the potential scope of the DELIGHT program and how it could add to and complement existing programs and resources. A care partner suggested that integrating content regarding sleep quality was important, in addition to physical activity, healthy eating, and social engagement as envisioned by the investigators. This care partner emphasized that sleep disruptions could be very detrimental to the health and wellbeing of the person with dementia and their care partner, in line with existing research (Rose et al., 2010). Though not all team members with lived experience had experienced sleep disruptions, they agreed it was a challenge for many people living with dementia and care partners.
We also gathered, reviewed, and reflected on existing programs and resources related to our project vision. The initial meetings created a sense that there was a clear gap that a multi-component program that integrates physical activity, healthy eating, social connection, and sleep could address, with some guidelines for resource formats that could support the program. While the Alzheimer Society of Canada Minds in Motion® program provided exercise and mental and social stimulation, it did not purposefully provide learning about strategies to promote health and wellbeing. Upon review of resources, the team concluded that few existing resources were up to date with current evidence, though a few were identified as useful (e.g., an introduction to dementia and memory tips & tricks from the Alzheimer Society of Canada). The research team also identified resource formats that they liked and aspects that made resources difficult to use. For example, displaying content in resources in columns was considered more difficult to read by a member with dementia, unless there was a lot of space between each column.
Step 3: Co-Design of the DELIGHT Program
Drafting and Re-drafting the DELIGHT Co-design Process
Establishing the DELIGHT co-design team and format for their participation in the co-design process was also a major focus of the first three research team meetings (January to March 2020). Groups that were deemed important to include in the co-design process were people living with young- and late-onset dementia and care partners, dementia service providers (including Alzheimer Society and municipal program staff), community service providers who delivered healthy lifestyle programs, and health care professionals (including dietitians and registered kinesiologist or clinical exercise physiologists for exercise and healthy eating expertise). To identify invitees, we initially listed people from within our professional and personal networks. We focused on individuals and organizations local to the primary project site, in part due to restrictions in funding for travel. At the end of the recruitment process, we assembled a co-design team of 29 people, which included five people living with dementia (two with young-onset, three with late-onset), five care partners, two nurse practitioners, five exercise professionals, four dietitians, four community/dementia service providers, and six researchers. Of these, five were men and three were people of non-white racial identity. Note that some people fulfilled more than one role (e.g., dietitian and care partner). Recruitment was facilitated by the researchers’ history of community-engagement and participatory research (e.g., Dupuis et al., 2021; Middleton et al., 2023; Middleton et al., 2024) and associated relationships with people living with dementia, care partners, and health care and community service providers.
In line with prior work by investigators and co-researchers, the research team proposed a series of three or four in-person half-day workshops, as needed, to co-design the DELIGHT program. Some co-design team members would not be able to make every workshop, especially if they lived out of town. The first co-design workshop was planned for an in-person, half-day meeting in April 2020. However, the World Health Organization declared the COVID-19 pandemic on March 11, 2020 (WHO, 2020). Resultant public health restrictions meant that in-person gatherings were no longer possible, either for the research team or the co-design process. After skipping the March 2020 research team meeting, we agreed to meet virtually through the Zoom platform. We onboarded two of our research team members to Zoom for the first time and resumed meetings in April 2020.
As a research team, we reflected on the planned in-person co-design process and agreed that in-person workshops were unlikely to go ahead that summer. We also discussed the merits and challenges of a virtual co-design process, acknowledging that we may lose some members who had planned to participate. We decided that the next step would be to reach out to the DELIGHT co-design team to understand: (1) whether they were still interested in participating; (2) whether they had a device to use to connect for video conferencing; and (3) whether they felt comfortable using Zoom to try to proceed with the co-design process. We also asked whether they preferred to stay with the plan of three to four half-day meetings or a greater number of shorter meetings. Most of the co-design team supported moving ahead with a virtual co-design and had suitable devices to connect to a Zoom meeting. As a result, the research team decided to move forward with a virtual co-design process. One person living with dementia, one care partner, and one community service provider withdrew from the process. However, we identified two new people living with dementia, three new care partners and two new healthcare providers, again through our networks and connections, who could participate in the virtual co-design. Additionally, several members could attend more regularly since they were able to participate from a distance.
All co-design participants preferred shorter meetings rather than fewer half-day meetings, agreeing that having 1.5-h meetings approximately every other week was reasonable. We were able to identify a day and time that worked for all members, despite the large team, likely facilitated by the shutdown of most businesses, facilities, and in-person gatherings early in the pandemic. Many members’ schedules were more flexible than usual, apart from health care professionals.
The DELIGHT Program Virtual Co-design
Like the research team, the co-design process was designed to align with the principles and enablers of Authentic Partnership. The importance of respecting, valuing, and integrating diverse perspectives into co-design decisions was emphasized in our first meeting. The aim was to create a space where each person felt confident to share their unique knowledge, experiences, and perspectives, which were valued within discussions and the co-design process. We also emphasized that engagement was flexible and adaptive. We acknowledged that members may not be able to attend each session and that we may need to adapt the process as we proceeded. We reinforced dementia-friendly language and communication strategies. All communications and materials were in simple language and large, accessible font (Arial 14pt in emails, Arial 24pt+ in presentations) with adequate white space.
Co-design meetings and guiding questions.
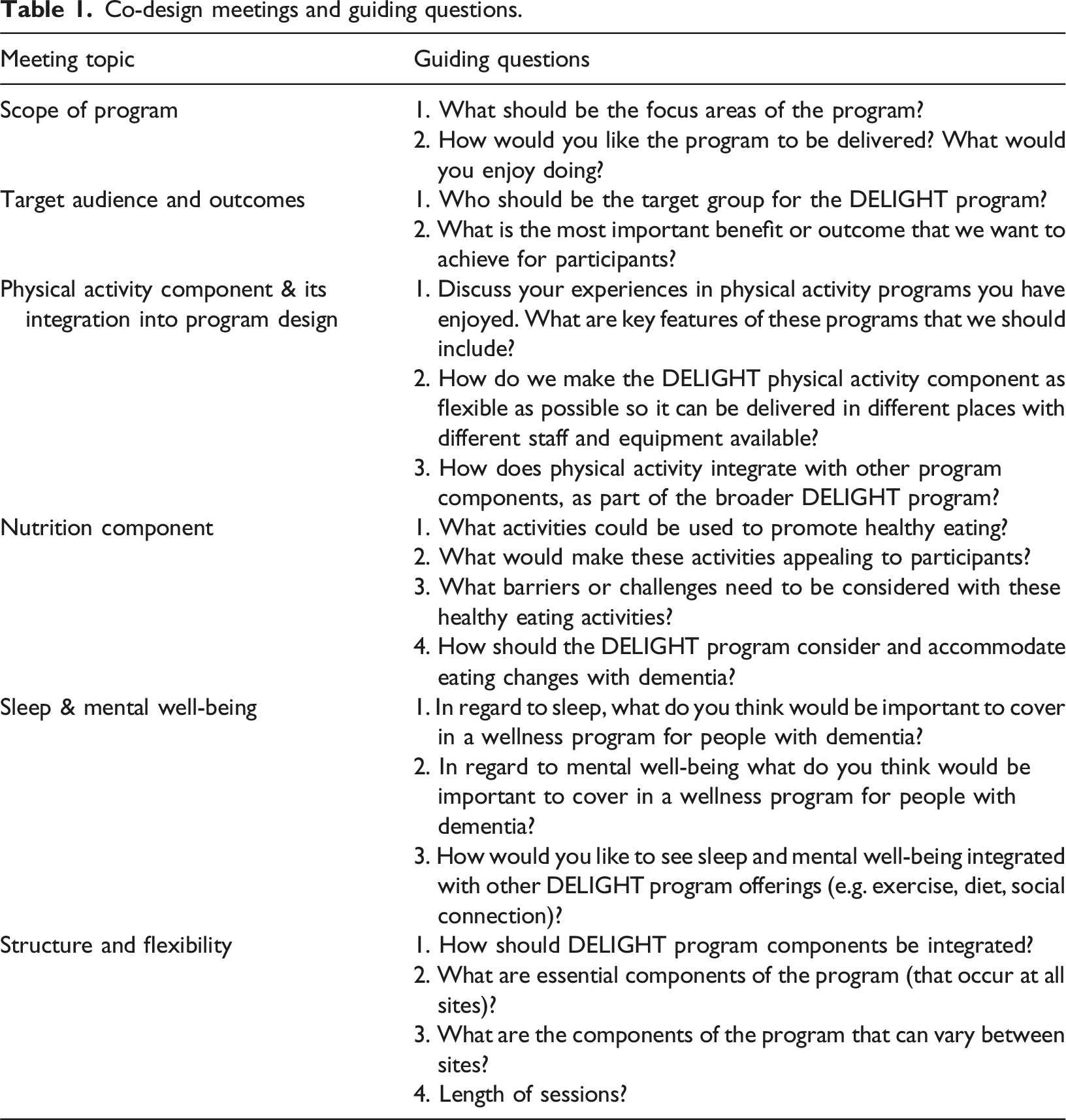
Each meeting opened with participants being individually welcomed and some time for casual conversation and social connection among members. Many people were isolated at home with little outside contact, so personal connection and conversation was valuable beyond the co-design process. The formal part of the meetings started with a presentation by an investigator, which reviewed the overarching aim of the co-design process, the objective of that meeting, related research evidence, and guiding questions for the discussion. Participants were given an opportunity for questions prior to splitting into breakout rooms of five to seven people, where guiding questions were discussed in detail. Of note, none of the investigators had previously used Zoom breakout rooms. A brief practice with students and staff prior to the first co-design meeting suggested that the technical process was relatively simple. The investigators agreed to try breakout rooms for the first co-design meeting and adjust if needed.
Breakout rooms were set ahead of time in Zoom, purposely balanced with at least one person living with dementia, care partner, researcher, and health care or community service provider in each room. Each breakout room had a facilitator (investigator or senior trainee) and a notetaker (trainee or research staff). Like the main meeting, breakout room discussions started with a few minutes of social connection. The conversations were then run in a semi-structured format, generally following the guiding questions but allowing conversation to evolve based on the discussion and priorities of participants. The facilitator elicited the perspectives of quieter participants when needed. Most participants who lived with dementia were onscreen and participated fully in discussions. One participant with more advanced dementia was nearby but not onscreen. This person’s opinion was elicited through their care partner at key points in the discussion, with the care partner repeating responses back to the group. In this way, the care partner acted as a communication aid but did not generate responses on behalf of the person living with dementia. After about 40 minutes of discussion in breakout rooms, all participants returned to the main Zoom meeting where the notetaker shared a summary of their breakout room discussion. Opportunity for breakout room members to clarify or add points was provided. The technical process of moving people in and out of breakout rooms went smoothly, as did the opportunity to connect and discuss in small groups.
Within two days following each co-design meeting, the investigators, trainees, and staff met to summarize the results of the session, determine whether there was a consensus path forward, and decide the next steps, including any follow-up questions needed and selecting guiding questions for the next co-design session. The full research team met midway through the co-design process to reflect on our approach and progress and identify whether any changes were needed to the plan moving forward. No substantial changes were made. The co-design process occurred over six virtual meetings between May and July 2020.
Output of the DELIGHT Co-design: The DELIGHT program
The co-designed DELIGHT program is outlined in Figure 1. Key reflections that informed our decisions are described here. Team members agreed with the initial proposal of the research team that the DELIGHT program should include physical activity, healthy eating and nutrition, sleep, and social engagement, as each was considered valuable to the health, wellbeing and function of people living with dementia. The co-design team also emphasized that an explicit focus on supporting mental wellbeing of people living with dementia and care partners was needed, while recognizing that mental wellbeing can also be influenced by other components of the program. Co-design team members also recommended that the program should connect participants to other programs and supports in their community as system navigation can be challenging for people living with dementia and their families. DELIGHT program.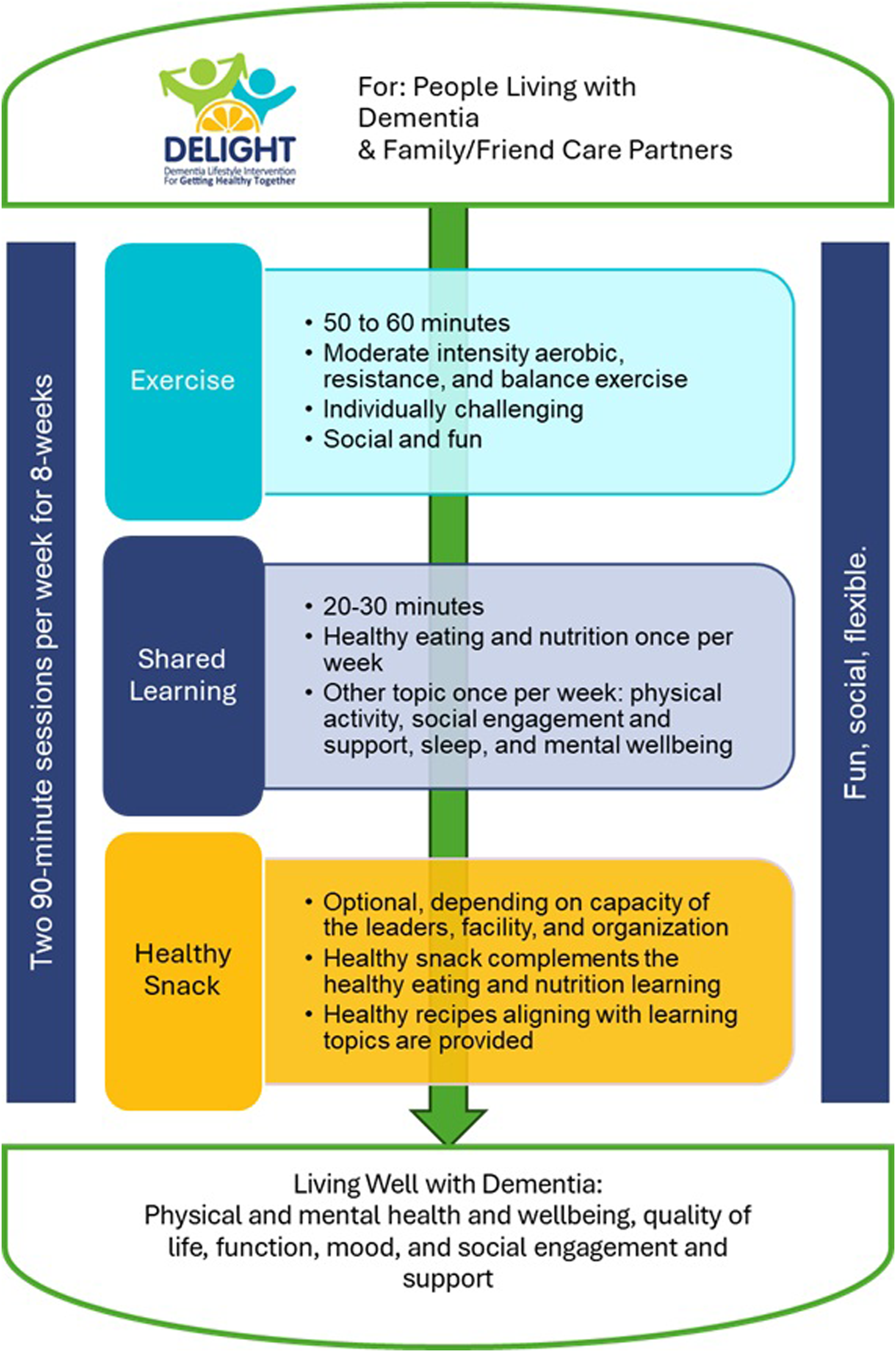
The co-design team decided that the DELIGHT program should target people in the early- to mid-stages of dementia (including those with mild cognitive impairment) who were living in the community, with particular emphasis on those who recently received a dementia diagnosis. Welcoming people at different times in their dementia journey would provide mentorship opportunities, where those with more experience could share strategies and supports that had been helpful. Team members strongly advocated to include an option for care partners to enrol as full participants alongside people living with dementia (i.e., not just as supporters). Care partners could also benefit from the health promotion and social engagement inherent to the program. However, people living with dementia who did not have a care partner available should still be able to participate.
“Living well” was designated as the primary outcome of the program. This concept incorporates (physical and mental) health and wellbeing as well as quality of life, function, mood, and social engagement and support. The co-design team also deemed important changes in physical activity and eating habits as well as connection to community services.
The DELIGHT program should be fun and socially engaging for participants. The program needed to be flexible within a core format and principles so that it could be delivered by staff or volunteer teams in diverse settings with different equipment and resources available. Anticipated settings included community centres, gyms, places of worship, cultural organizations, and more. In-person and virtual formats should be supported for broader reach to rural communities, though the initial focus was the development of the in-person format.
The co-design team arrived on a program structure of twice weekly sessions that were each 90 minutes. Each session would include 50–60 minutes of physical activity followed by 20–30 minutes of shared learning, with a short transition period in between. Social engagement should be integrated in all elements of the program. Program frequences of once to three-times a week were suggested, discussed, and considered. People living with dementia and care partners suggested that two weekly sessions would allow relationships to develop more quickly and was sufficiently pragmatic for community organizations. Shared learning at each session would allow for purposeful dialogue and connection between members. Moreover, physical activity twice weekly for 45–60 minutes aligned closely with practice guidelines for people with cognitive impairment (Ginis et al., 2017; Petersen et al., 2018).
Co-design participants recognized that physical activity could contribute to most goals of the program, including increased health, function, appetite, social engagement, mental wellbeing, and sleep. The physical activity should include moderate intensity aerobic, strength, and balance training, aligning with best evidence for improving physical and cognitive function (López-Ortiz et al., 2023). How these elements are delivered can be flexible – for example, though walking groups, strength training, dance, and more. Choice of activities should align with the equipment available and the preferences of the group. There should be at least two difficulty levels available to ensure that the program is individually challenging. Having a knowledgeable instructor was seen as important to provide a safe but challenging program. Low instructor/volunteer to participant ratios were seen as desirable.
The physical activity component would be followed by shared learning, which would focus on healthy eating, physical activity, social engagement and support, sleep, and mental wellbeing in relation to dementia. The learning should not be didactic but an open discussion around a resource related to one of these topics. A series of learning resources were developed for each topic. These resources were used to prompt discussion and sharing. Having an open discussion was seen as a strategy to recognize experience, expertise, and capacity of participants and normalize asking for help and supports. Participants could share their own knowledge and strategies in relation to the topic as well as programs and resources that had been helpful to them. In this way, participants could learn from each other. Healthy eating would be the focus once per week, with one of the other four topics in the other weekly session. In addition to a resource, simple recipes were provided that highlighted the healthy eating theme of the week and could be served as a snack after the exercise. Preparing and eating the health recipe (or another food complementary to the topic) was designated an ‘optional’ component as not all facilities or organizations would have capacity to prepare or offer food.
The co-design team also created several additional optional program elements. These included a “happiness” check-in midway through the program to see how participants were feeling, particularly in relation to their mental wellbeing. Special events could also be integrated, including expert speakers, off-site activities, and novel activities such as a nature walk, yoga, or a visit to a community program. These options may promote awareness of other community resources and programs that could support living well with dementia, beyond what was known and brought up by participants.
Iterative development of DELIGHT program & materials
Following the six DELIGHT co-design sessions, each participant indicated how they would like to be engaged in the development of program materials moving forward. Many expressed willingness to review resources as they were developed, or to be consulted in their area of expertise. Research team members, in particular, reviewed resource formats and content as they were created. Various options for font, colours, and layout were reviewed for accessibility and attractiveness by the research team, with focus on accessibility to the members who were living with dementia. Large font size (14pt or more) and a single (rather than multiple) columns were identified as important by research team members who were living with dementia. Bright colours and joyful images were preferred. An illustrator created drawings of people that aligned with content, with an effort towards inclusivity across ethno-racial groups and images that showed joyful engagement. The research team reviewed, reflected on, and discussed draft illustrations and selected six drawings, with each used in one or more resources.
The content was evidence-based. The research team included expertise in physical activity, healthy eating and nutrition, social engagement and support, and mental wellbeing in relation to dementia. Where needed (e.g., for sleep resources), additional experts were engaged to ensure the resource content aligned with best evidence. A manual for program leaders and 32 learning resources were developed. The program manual detailed staff/volunteer training requirements, program onboarding processes, and both required and optional program requirements. The learning resources included 12 healthy eating resources, 10 physical activity resources, three resources on mental wellbeing, three resources on sleep, and three resources on social connection and support (see Supplemental Material for topics).
In the winter of 2021, it became clear that it would not be possible to pilot the in-person DELIGHT program in the near future due to the ongoing COVID-19 pandemic. As a result, the development of the virtual program became a priority. Members of the co-design team with experience delivering or attending virtual exercise sessions were engaged in one additional co-design meeting focused on virtual adaptations. While the program format (90 mins twice per week) remained the same, it was to be completed on Zoom. Furthermore, exercise duration was slightly shortened (40–50 minutes) with a break before the shared learning. “Bite-sized but not superficial” social breaks were recommended to be interspersed within the exercise portion. No specialized fitness equipment was required but could be used if available. Exercise bands were suggested as an easy to share equipment that would enable a more diverse range of strength training. Rather than providing healthy snacks in-person, recipes for snacks were to be shared with participants a week or more in advance so they could prepare the snack if desired. The shared learning component remained unchanged.
Reflections & discussion
In this paper, we described the participatory approach used to co-design the DELIGHT program (in-person and virtual formats), including a virtual co-design process that occurred in early stages of the COVID-19 pandemic via web-conferencing (Zoom). The research team of people with lived experience, as well as the extended group of people with lived experience, health care, and community providers, were essential to ensure that the created program and materials were addressing DELIGHT goals in a practical way.
Integrating the diverse voices within our co-design process created a DELIGHT program that has the potential to promote the health and wellbeing of people living with dementia and care partners and increase their ability to live well with dementia. The perspectives and experiences of people living with dementia, care partners, and health care and community service providers resulted in meaningful changes to the program design. For example, we added content about sleep and mental wellbeing to our shared learning resources in response to people living with dementia and care partners highlighting these as important factors for their wellbeing. Indeed, altered sleep and poor mental wellbeing are common among people living with dementia (Wennberg et al., 2017). One rural-dwelling person living with dementia also highlighted a need for a DELIGHT program model that could be delivered both in-person and virtually. Keeping this in mind throughout the co-design meant that we could quickly shift to a virtual pilot of the program when in-person programming remained impossible with the continuation of the pandemic. Perhaps most importantly, our members with lived experience emphasized that the program needed to have joy and connection at its core. The result is a program that integrates all interventions identified as important to promoting ‘living well with dementia’ by the IDEAL program (a study of 1537 people with cognitive impairment and 1277 care partners): promoting physical fitness, positively supporting people living with dementia, enabling functional abilities and independence, and reducing isolation and increasing participation.
The DELIGHT co-design was initially planned for in-person but was transitioned to virtual in response to public health restrictions early in the COVID-19 pandemic. Guidance for virtual co-design emphasizes that accessibility for all stakeholders is an important consideration (Mallakin et al., 2023). While older adults have lower rates of technology use (Government of Canada, 2019), COVID-19 public health restrictions prompted a rapid increase in technology use and skill development among older adults (AGE-WELL, 2020) as well as increased availability of virtual programming and services, including those for people living with dementia (e.g., Alzheimer Society programs) (Neudorf et al., 2024). This created new opportunities to engage people living with dementia and care partners virtually. Among our co-design participants, only two research team members (a person living with dementia and a care partner) had never used Zoom before. Using Zoom for this and future co-design enables involvement of people who might not otherwise participate due to distance or travel times. Indeed, we had participants from locations ∼18 hours apart. Recognizing differences in capacity with technology and taking the time to support team members individually was necessary for this virtual co-design. While most of the DELIGHT research team had used Zoom previously, none had used Zoom breakout rooms prior to the co-design process. Given this limited experience, it was surprising to the investigators (and perhaps others) how smoothly the co-design process proceeded. A brief practice session enabled us to smoothly transition participants to breakout rooms even in the first meeting. Setting up the consistent composition of breakout rooms allowed transitions to breakout rooms to occur smoothly and created connections and comfort in the smaller groups.
Few prior studies have used virtual co-design or participatory research with people living with dementia (Middleton et al., 2023; Nomura et al., 2009). Most prior virtual co-design processes used interviews with people living with dementia as input into virtual co-design meetings, which were attended only by other stakeholder groups (e.g., care partners, health care professionals) (Thodis et al., 2023). In our co-design, people living with dementia attended the virtual meetings and were supported to engage in a way that suited their needs and preferences. Three of five people living with dementia attended with a care partner, while one only had the support of their care partner to connect to Zoom and the other attended independently. Flexible approaches allowed individuals with a range of cognitive and communication abilities to participate and contribute to decision-making. When the person living with dementia had more significant communication challenges (two participants), the care partner facilitated discussion some or all of the time. Importantly, however, the care partners relayed questions and responses but did not generate responses for the person living with dementia, reducing misrepresentation of the perspectives of people living with more advanced dementia. Guidance for virtual co-design processes also emphasizes the importance of connection, collaboration, and facilitation (Mallakin et al., 2023). In both research team and co-design meetings, actions were intentionally taken to reinforce connection and relationships among the team. We made time for social connection in the main meeting and breakout rooms. Consistent, small breakout rooms likely allowed deeper relationships to develop, where developing trusting relationships is a core part of the Authentic Partnerships approach (Dupuis, Whyte et al., 2012).
While we aimed to engage voices from diverse ethno-cultural and racial groups in our co-design process, we needed more time for relationship building and only three of 29 co-design participants were of ethno-racial minority identity. Time and effort are needed to develop strong relationships, resolve differences, and identify shared priorities (Freeman et al., 2021), especially among those who experience stigma due to their identity or in relation to dementia (Di Lorito et al., 2024). It also needs to be recognized that invited participants of ethno-racial minority identities may have had other priorities during the pandemic, such as high demands on cultural organizations to support their community with income, food, and service access (Beringer et al., 2023). Equity differences, such as internet access, need to be recognized when attempting a co-design process with diverse groups. Being flexible with frequency and how team members participate is an important learning. In-person meetings, more difficult early in the pandemic, are important to building relationships (Freeman et al., 2021). Future work by our team must engage people from different ethno- racial identities to reflect on the relevance of DELIGHT and adapt the program to suit the needs and preferences of diverse communities.
Conclusion
To co-design the DELIGHT program, we engaged people with diverse roles in a virtual co-design process based on the Authentic Partnership approach (Dupuis, Gillies et al., 2012). Valuing and integrating each person’s perspectives within this approach led to the development of a unique, evidence-based, multi-component program called DELIGHT. The virtual engagement evolved the DELIGHT project from a high-level vision to a fully developed program with a program manual and 32 accompanying resources. Our co-design process increases the likelihood that the DELIGHT program will be relevant to people living with dementia and care partners and feasible for implementation in the community. Our end goal is that people living with dementia and care partners have access to a relevant and effective program to increasing their health and wellbeing and ability to live well with dementia.
Supplemental Material
Supplemental Material - The Co-design of the Dementia Lifestyle Intervention to get healthy together (DELIGHT) program: An authentic partnership approach
Supplemental Material for The Co-design of the Dementia Lifestyle Intervention to get healthy together (DELIGHT) program: An authentic partnership approach by Laura E Middleton, Lauren Bechard, Bill Heibein, Lloyd Schneider, Marg Shoemaker, Gail Roth, Cindy Wei, Melissa Koch, Heather Keller, and Carrie McAiney in Dementia
Footnotes
Acknowledgements
David Shoemaker was a member of the DELIGHT research team whose input was foundational for the development of the DELIGHT processes and co-design decisions. He passed away in late 2021 and his presence continues to be missed.
Author contributions
L.M., H.K., and C.M. conceived of the project and M.S., L.S., W.H., and G.R provided foundational input into the more fulsome development of the concept into process. L.M., H.K., C.M., M.S., L.S., W.H., and G.R, and the DELIGHT Co-design Steering Team members collaboratively decided on project processes described herein. This includes patient partner (W.H., D.S. [acknowledgements]), care partner (L.S., M.S.), and a community partner (G.R.). All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Canadian Consortium on Neurodegeneration in Aging. The Canadian Consortium on Neurodegeneration in Aging is supported by a grant from the Canadian Institutes of Health Research with funding from several partners, including the Alzheimer Society of Canada. The Canadian Institute of Health Research grant number is (CNA-163902).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.