
Abstract
Dance is a form of exercise that engages motor, cognitive, social, and emotional skills (Charras et al., 2020). Céilí dance is a traditional Irish social dance offering physical and psychological health benefits, with the added benefit of a social element. People living with dementia and care partners have low levels of physical activity (PA) despite understanding the range of benefits (van Alphen et al., 2016). This study aimed to develop a person-centred dance - based exercise intervention for people living with dementia and care partners. The Medical Research Council Framework (MRCF) and behaviour change wheel (BCW) informed the intervention design. A literature review, focus groups and interviews with people living with dementia and care partners were completed to explore experiences and preferences of physical activity and exercise. Findings were mapped to intervention functions and further developed into intervention components using selected behaviour change techniques (BCTs). A stakeholder group and a participant advisory group (PAG) reviewed and refined the intervention. The intervention targeted increasing physical activity and exercise (PAE) in people living with dementia and care partners. Thirteen statements were generated from nine studies. Twenty-six participants, (nine people living with dementia, seventeen care partners) engaged in focus groups or interviews. Analysis identified physical and psychological capability, physical and social opportunity, as the key constructs for change. These aligned with six out of nine intervention functions, leading to the identification of twenty-one appropriate BCTs. These were reformed into six intervention components. These included: a supervised dance exercise class, an induction session, assessments of physical and psychological health, a goal setting and action planning session, daily prompts for class, and a social aspect. This Céilí dance exercise intervention is a theory-informed, systematically designed intervention tailored for people living with dementia and care partners. It has the potential to improve PAE in this population. Future research should assess its feasibility and effectiveness.
Keywords
Introduction
Dementia is a neurodegenerative syndrome characterized by the loss of two or more cognitive functions e.g. judgement, thinking, memory (Arvanitakis et al., 2019). Age is the greatest risk factor for developing dementia, with incidence increasing after the age of 65 (Guerreiro & Bras, 2015). As the global population ages, dementia prevalence is rising with over 57 million cases of dementia across the world and there is currently no cure (Livingston et al., 2024). This is predicted to increase to over 150 million by 2050 (Nichols et al., 2022). An estimated 64,000 people in Ireland are living with dementia and 90% of these individuals are over 65 (Nichols et al., 2022; O’Shea et al., 2019; Rogan et al., 2023).
The World Health Organisation (WHO) has highlighted that more research for care and treatment of dementia is needed to assist in the overall management of the disease (World Health Organization, 2017). Due to the limitations of pharmacological treatments, non-pharmacological lifestyle-based interventions are increasingly explored. They have identified a positive impact on physical function, behavioural, and emotional symptoms (Park & Cohen, 2019). However, this research is currently limited, due to low recruitment rates, and long research development times (Pickett et al., 2018). Both pharmacological and non-pharmacological approaches can help slow the decline of functional abilities including balance, reduce fall rates and support mental health such as reducing anxiety (Nimmons et al., 2024; Park & Cohen, 2019). Interventions specific to people living with dementia and care partners are required to allow us to understand improvements needed in current care practices.
Various intervention types are beneficial for people living with dementia, including art, such as painting or drawing sessions, music, including engaging and passive music sessions, behavioural therapy, validation therapy and physical activity and exercise (PAE) (Douglas et al., 2004). Physical and psychological health can improve following general exercise in people living with dementia (Cunningham et al., 2020). Maintaining physical function helps older adults preserve their independence and community living (Tornero-Quiñones et al., 2020). Physical activity and exercise improves mobility, strength and mental wellbeing, including reduced depression (Aartolahti et al., 2020; Fox et al., 2007; Gothe et al., 2020; Lewis et al., 2020; Nimmons et al., 2024). Physical activity and exercise interventions should be adaptable and allow for the inclusion of diverse populations, such as people living with dementia and care partners. Despite the numerous health benefits, many people living with dementia and care partners do not participate in adequate levels of PAE per week (Boyle et al., 2015). The WHO recommends 150–300 minutes of moderate - vigorous PAE weekly for all older adults, including those with a chronic illness (WHO Guidelines on Physical Activity and Sedentary Behaviour, 2024). The PAE should include multicomponent activities, such as balance, strength and aerobic exercise (WHO Guidelines on Physical Activity and Sedentary Behaviour, 2024). If unable to meet the guidelines, people living with dementia should engage in as much PAE as their abilities permit.
Benefits of PAE can vary depending on the specific type of activity. Dance is both an art and a form of exercise that involves motor, cognitive, social, and emotional skills and it can improve balance, QOL and cognition (Charras et al., 2020). Dancing with others can strengthen social relationships for people living with dementia and their care partner, enhancing their quality of life (QOL) (Wu et al., 2015). Group dance can positively effect mood and wellbeing of PLWD, it provides social engagement and psychological relaxation (Fong Yan et al., 2024; Wang, Liu, et al., 2022). Céilí dance is a traditional form of social Irish dance, it is a partnered dance and it involves structured group movements performed to Irish music (Foley, 2011). An Irish population will likely be familiar with this style of dance as it is a popular form of dance in Ireland (Clifford et al., 2019). When participants are familiar with the activity, it can potentially help them to reconnect with their bodies thus allowing access to past experiences and memories (Hamill et al., 2012).
There are barriers to PAE for people living with dementia and care partners, including physical abilities and low motivation (Vseteckova et al., 2020). Understanding their needs is important, as it may help overcome the barriers, and increase participation (van Alphen et al., 2016). There is currently limited exercise interventions developed for people living with dementia and care partners (Park & Cohen, 2019). A tailored intervention may allow for increased participation and effectiveness (Pitkälä et al., 2013).
Intervention development should be guided by evidence supported tools to enhance the success of the intervention. The Medical Research Council Framework (MRCF) is the gold standard for intervention development (Shahsavari et al., 2020). It outlines four steps; development, feasibility, evaluation and implementation, enabling researchers to identify the most appropriate methodology for their intervention (Shahsavari et al., 2020). Additionally, interventions targeting behaviour change are often guided by the Behaviour Change Wheel Framework (BCW) (Michie et al., 2011). The BCW incorporates 19 behaviour change frameworks (Webb et al., 2016). Changing behaviour requires three essential factors: capability, opportunity and motivation to perform the behaviour (COM-B) (Michie et al., 2011). The BCW identifies the components needed to perform the selected behaviour (Barker et al., 2016). The BCW supports the development of effective and feasible interventions across populations (Cantwell et al., 2020; Kwok et al., 2021).
Patient and public involvement (PPI) is a crucial component in developing interventions, it enhances the research quality, relevance and value (Biggane et al., 2019; Brett et al., 2014; Patient and Public Involvement in Research (PPI) - HSE Research & Development, 2021). In dementia research, patient and public involvement aids the development of an evidence base and advises on the process of future research (Howard Wilsher et al., 2017). Previous dementia research has focused on care partners and healthcare professionals, excluding people living with dementia due to assumptions about their reliability (Gove et al., 2018). People with a lived experience (people living with dementia and those who care for them), provide essential insights to ensure authenticity and relevance (Roberts et al., 2020). Patient and public involvement allows an understanding from the perspective of the target population (van Schelven et al., 2020). In this study, PLWD and care partners were involved as collaborators in co-designing the intervention content and advising on recruitment and data collection processes.
This study aimed to demonstrate the development process of a dance exercise intervention for people living with dementia and their care partners within an established medically supervised community-based exercise program for people with chronic illnesses. The MRCF and the BCW guided the interventions development to ensure a patient centred approach. The target behaviour was to increase the physical activity levels of people living with dementia and care partners.
Methodology
Overview
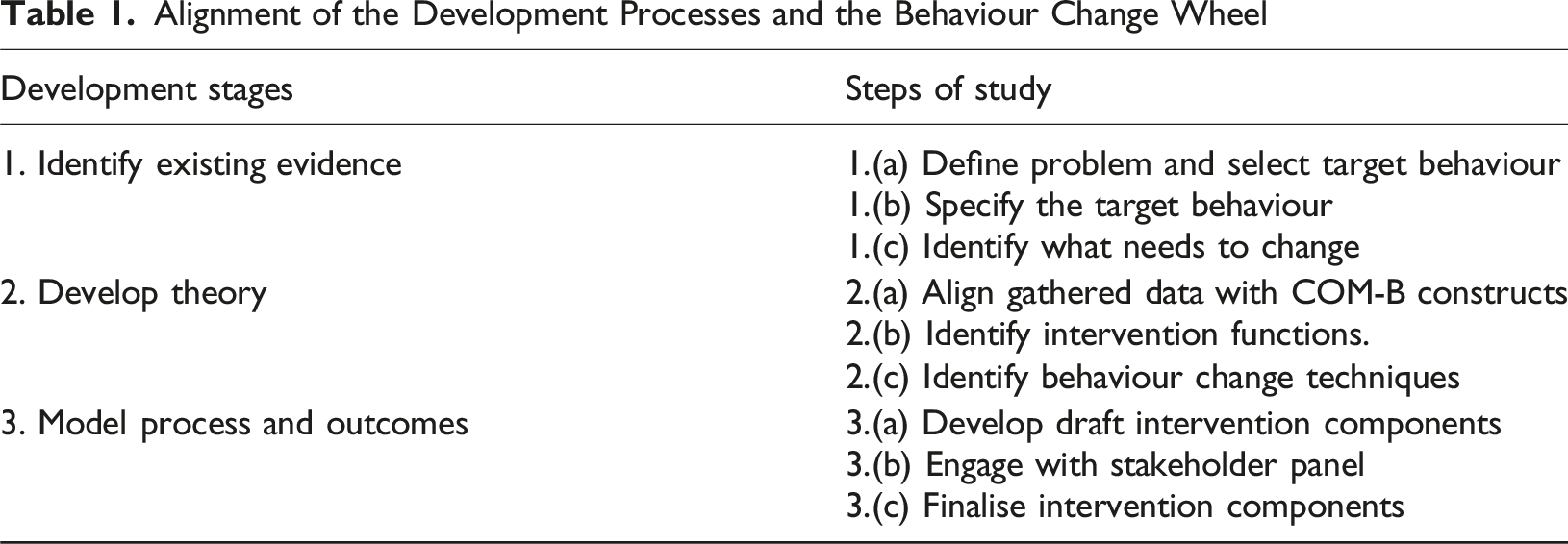
Alignment of the Development Processes and the Behaviour Change Wheel
Participant Advisory Group
A PAG was established through the Dementia Research Advisory Team in the Alzheimer’s national governing organisation (NGO) at the beginning of the study. The PAG consisted of two people living with dementia and two care partners who volunteered to participate in this research advisory team. All meetings were conducted virtually using Zoom. The PAG were involved in two specific phases of the study; (1) Reviewing the interview and focus group topic guides and (2) The final review of the intervention components. Their feedback was gathered and implemented at both stages. The PAG collaborated on the co-design of the intervention content, recruitment and data collection processes.
Procedure
Stage 1. Identify Existing Evidence
Define Problem and Select Target Behaviour
A general search of research articles, online books and grey literature within the area of PAE for people living with dementia and care partners, PAE for older adults and different forms of PA for older adults was conducted. Increasing PA in people living with dementia and care partners was identified as the primary target behaviour (Lindsay et al., 2022; van Alphen et al., 2016).
Specify the Target Behaviour
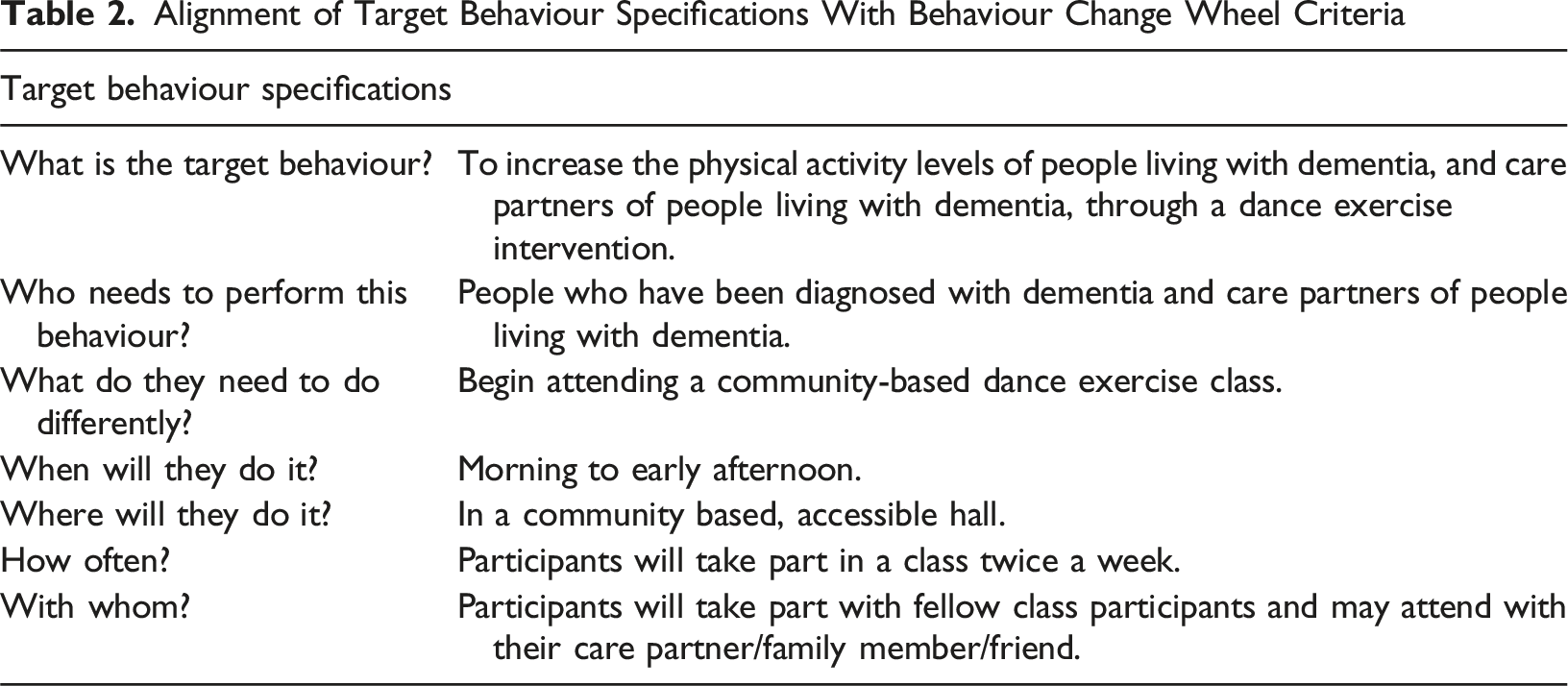
The target behaviour was further specified by using 6 questions as advised in the BCW steps (Michie et al., 2011). The questions included: (1) Who needs to perform the behaviour? (2) What does the person need to do differently to achieve the desired change? (3) When will they do it? (4) Where will they do it? (5) How often will they do it? (6) With whom will they do it? The responses were informed by the literature and qualitative findings.
Identify What Needs to Change
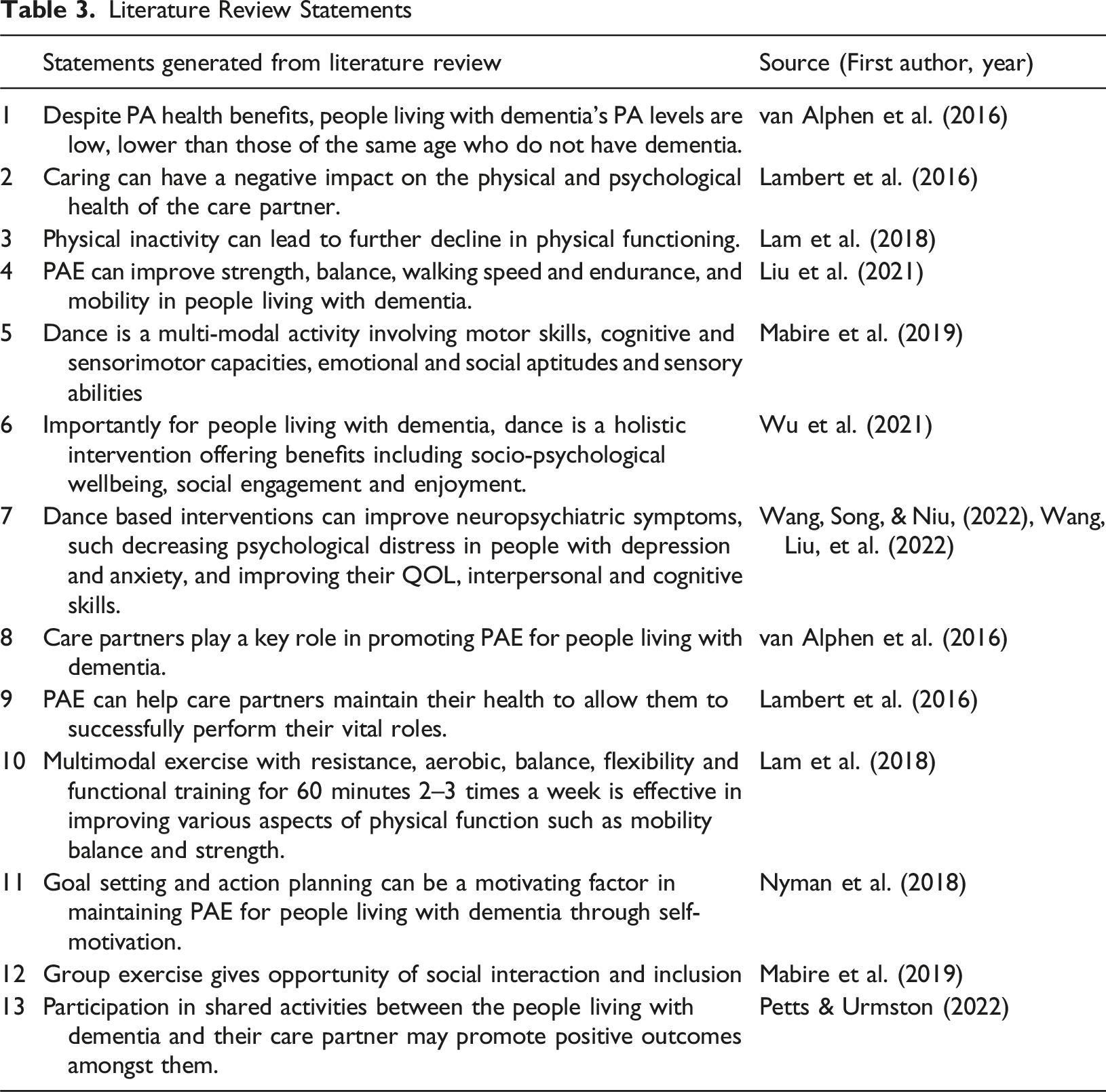
To address the target behaviour, a multi-method approach was utilized. This included a literature review, interviews and focus groups. Key statements from the literature review were generated to represent the findings of this phase.
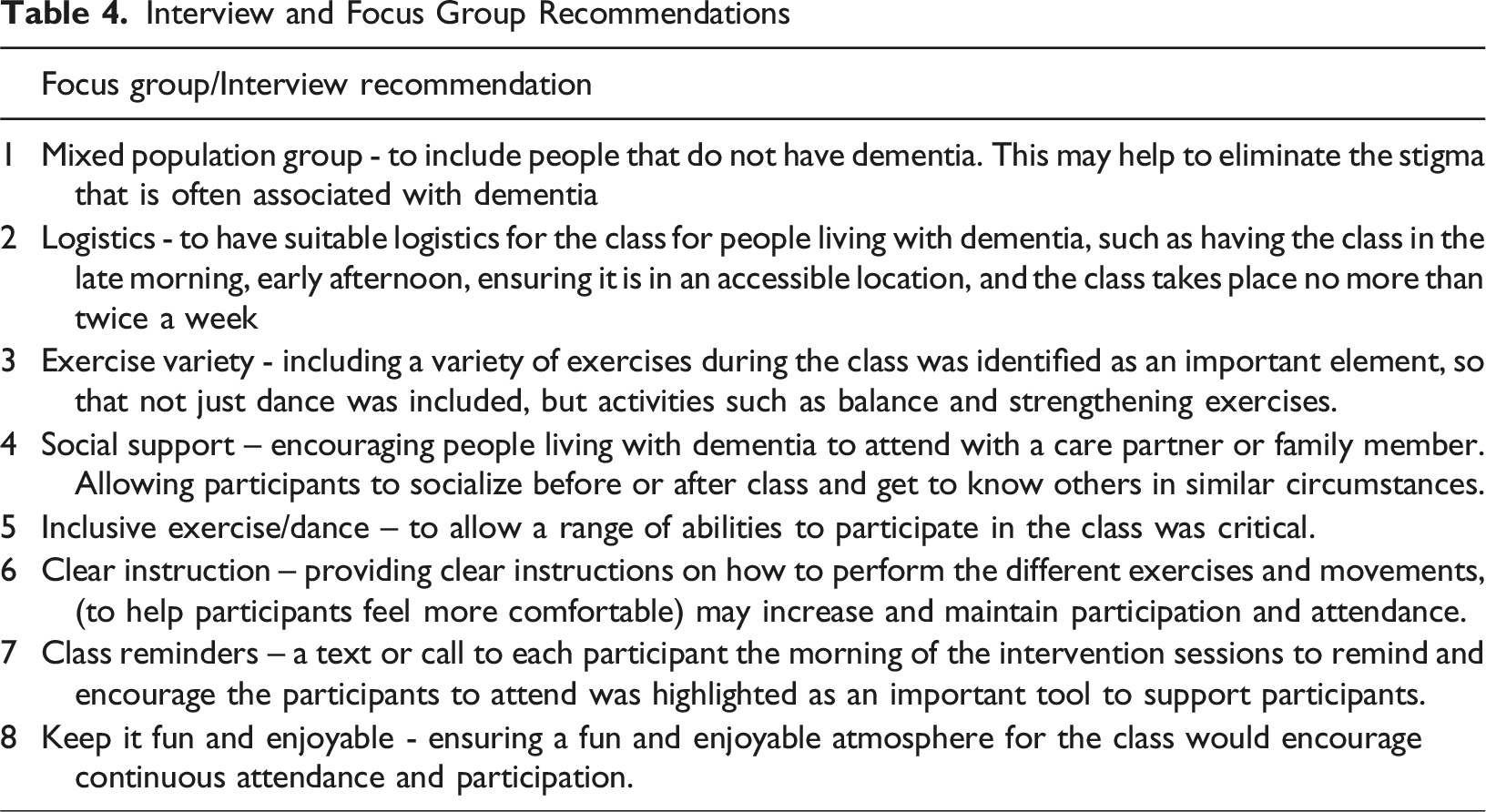
A mix of both semi – structured focus groups and individual interviews were conducted with people living with dementia and care partners where their perspectives and experiences of PAE were discussed. The focus groups and interviews followed a semi-structured topic guide, with slight variations in guides used with people living with dementia and care partners (see Supplemental File 2). Each construct of the COM-B model (Michie et al., 2011) (capability, opportunity and motivation) was addressed when developing the interview and focus group guides, to identify the constructs in most need of support. The topics included in the topic guides were, Understanding of PA, Previous and Current levels of PA, Important Factors of PA for PA interventions. The PAG reviewed the topic guides and gave their feedback on the topic guides. Their feedback was implemented to finalise the topic guides.
Participants for the focus groups and interviews were recruited though several avenues. A recruitment email and flyer were circulated to relevant organisations and individuals (e.g. relevant NGO, Exercise groups, Memory Clinics). The flyer was shared on social media. In-person visits to relevant groups were made by the researcher (Dementia Cafes, community-based exercise classes, social clubs,). Engagement with healthcare professionals, where the researcher provided details of the study, were conducted as part of the recruitment strategy. All interested persons were asked to complete an expression of interest form on Microsoft Forms or to contact the researcher whose details were provided. Prior to taking part all interested individuals were provided with a participant information sheet and completed an informed consent form or informed assent with a proxy informed consent if required.
Semi – structured focus groups (n = 3) and interviews (n = 14) took place online and in person. Each focus group consisted of four care partners. The focus groups and interviews were between 20–90 minutes (average = 34 minutes, standard deviation ±16 minutes). All were audio recorded via zoom or using a mobile recording device and transcribed verbatim. The transcripts were analysed using content analysis, via the analysis software NVivo 12. Content analysis provided the researcher with a process to identify patterns and key points within the gathered information (Vears & Gillam, 2022).
Stage 2. Develop Theory
Align Gathered Data with COM-B Constructs
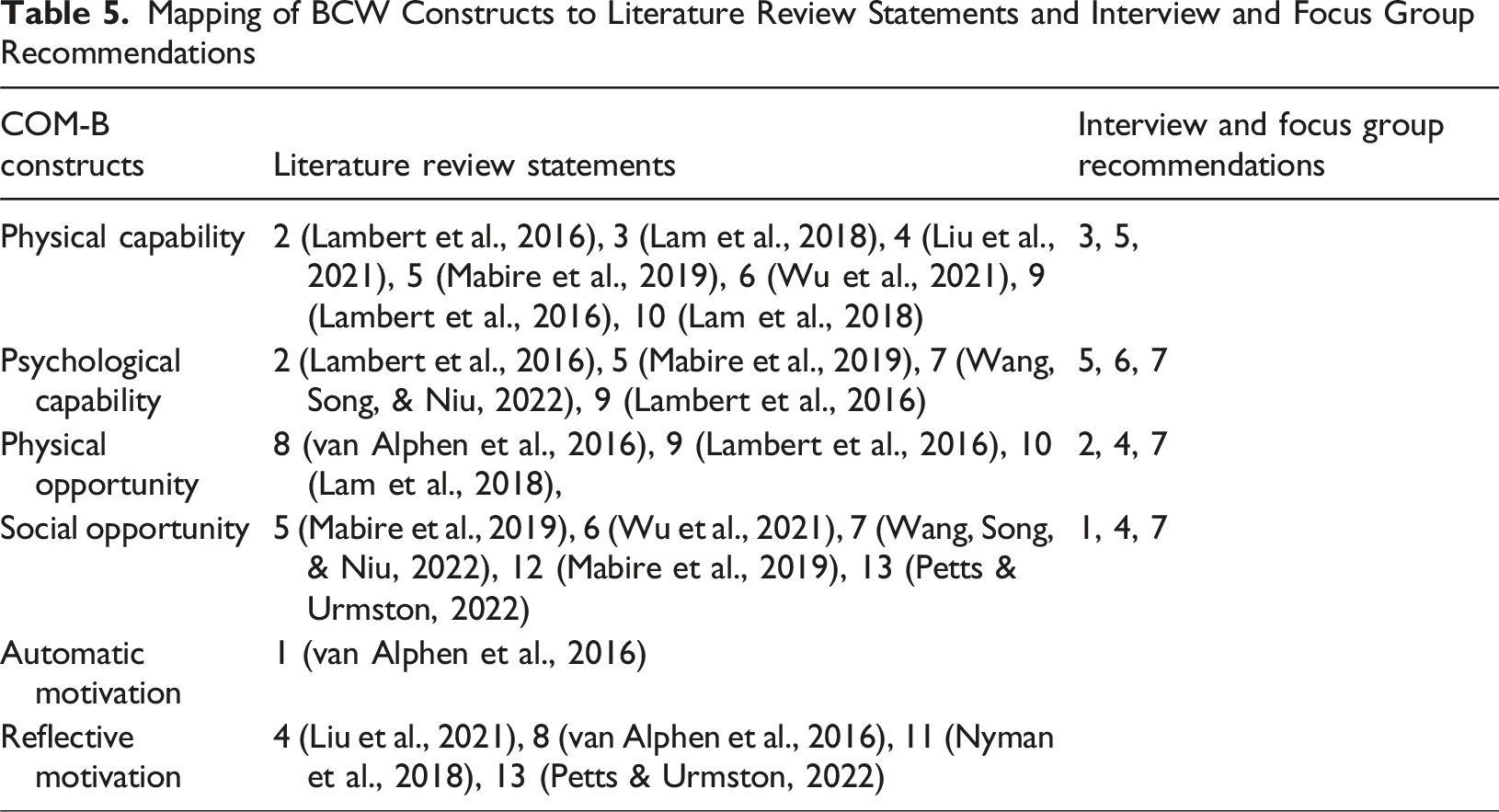
Key findings and recommendations from the literature and qualitative data were summarised and were aligned with the COM-B model to identify which COM-B constructs should be targeted. The COM-B constructs include: physical capability, psychological capability, physical opportunity, social opportunity, automatic motivation and reflective motivation.
Identify Intervention Functions
This phase involved identifying which intervention functions were relevant to support the selected COM-B model constructs. The BCW framework describes nine intervention functions, training, modelling, incentivisation, environmental restructuring, education, persuasion, coercion, enablement and restrictions, to guide intervention development (Michie et al., 2011).
Identify Behaviour Change Techniques
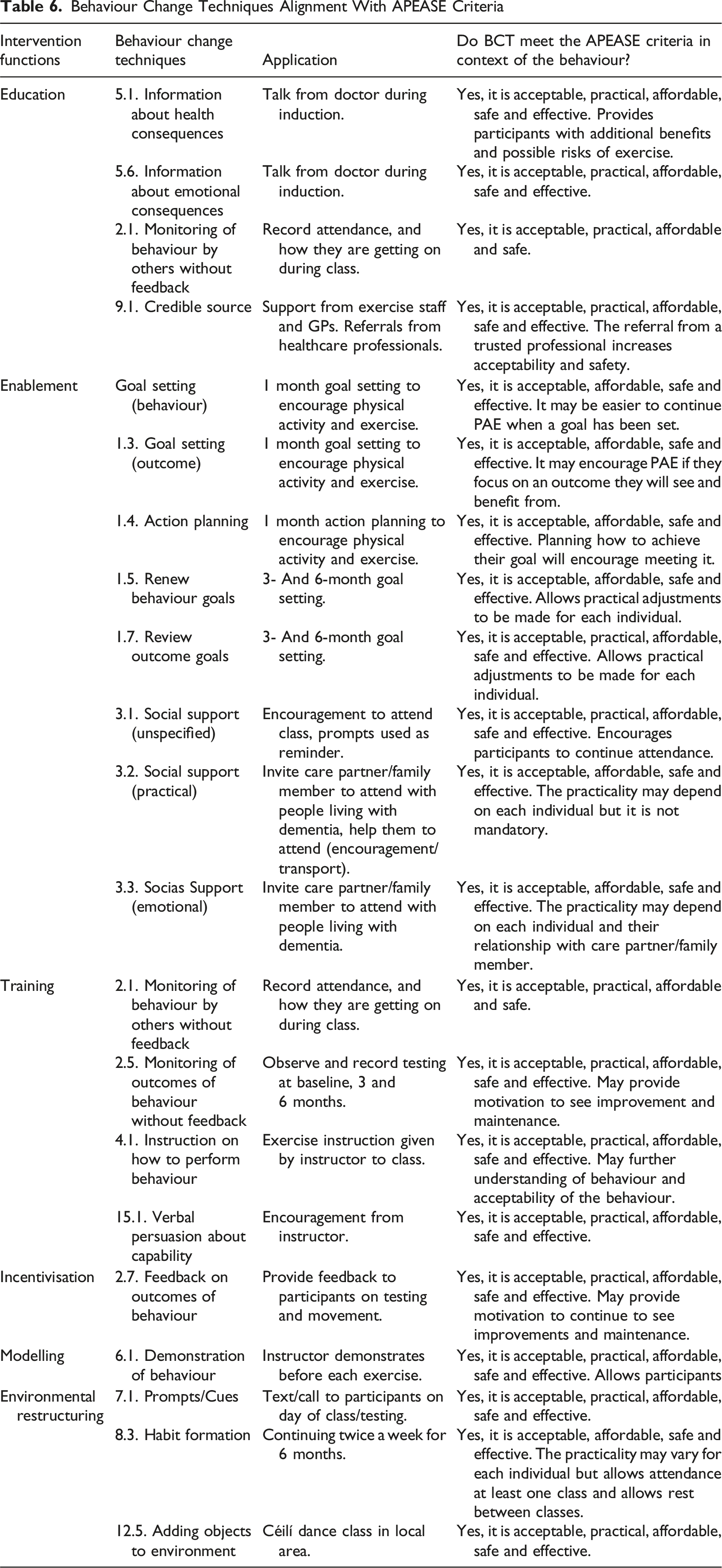
There are ninety - three behaviour change techniques (BCTs) in the behaviour change technique taxonomy. All the BCTs were reviewed. The most applicable BCTs were selected based on their alignment with the intervention functions. The affordability, practicability, effectiveness, acceptability, safety and equity (APEASE) criteria was used to evaluate each BCT (Michie et al., 2011).
Stage 3. Modelling Process and Outcomes
Develop Draft Intervention Components
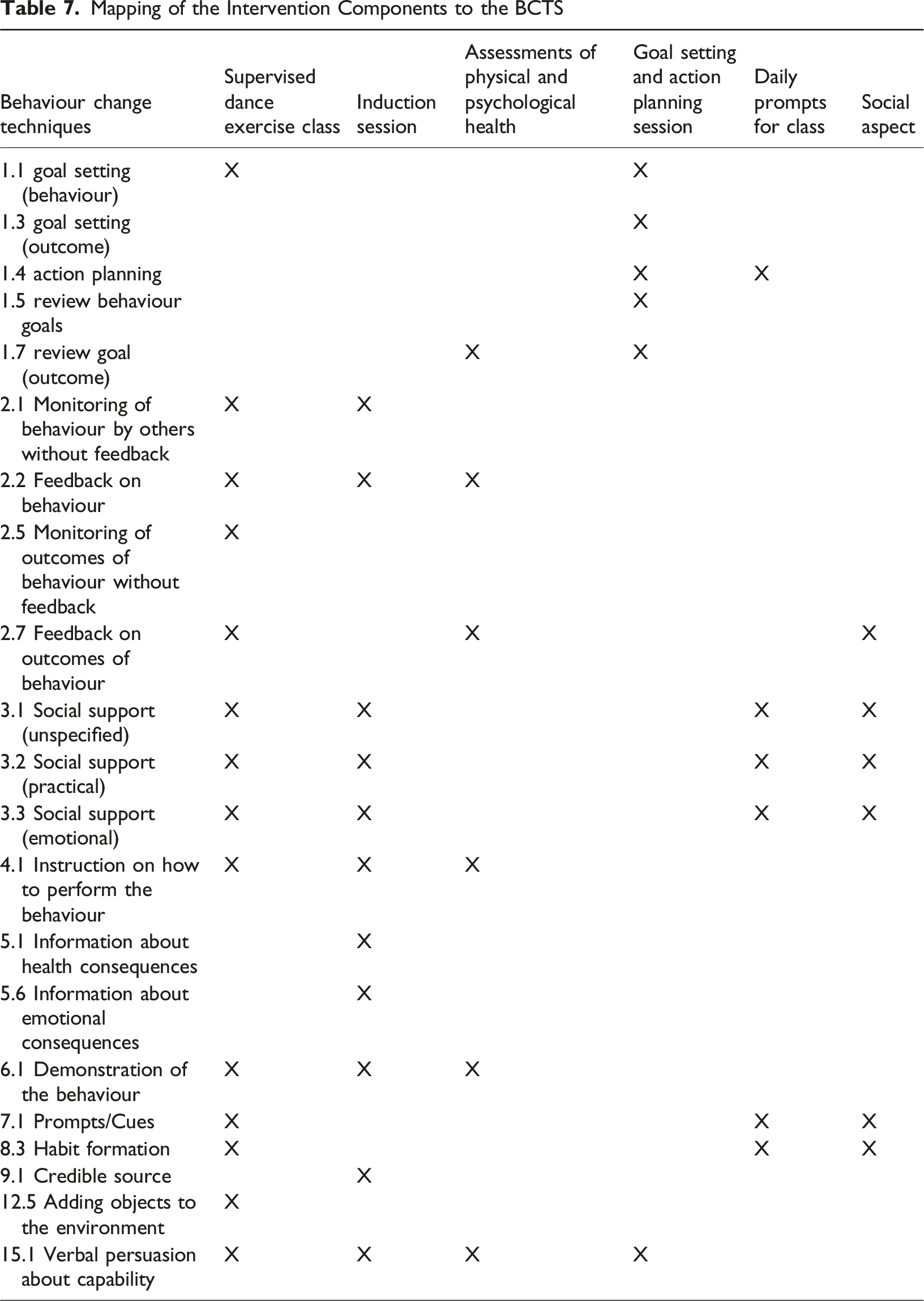
The initial draft of the intervention components was created by translating the selected BCTs into practical, deliverable content.
Engage with Stakeholder Panel
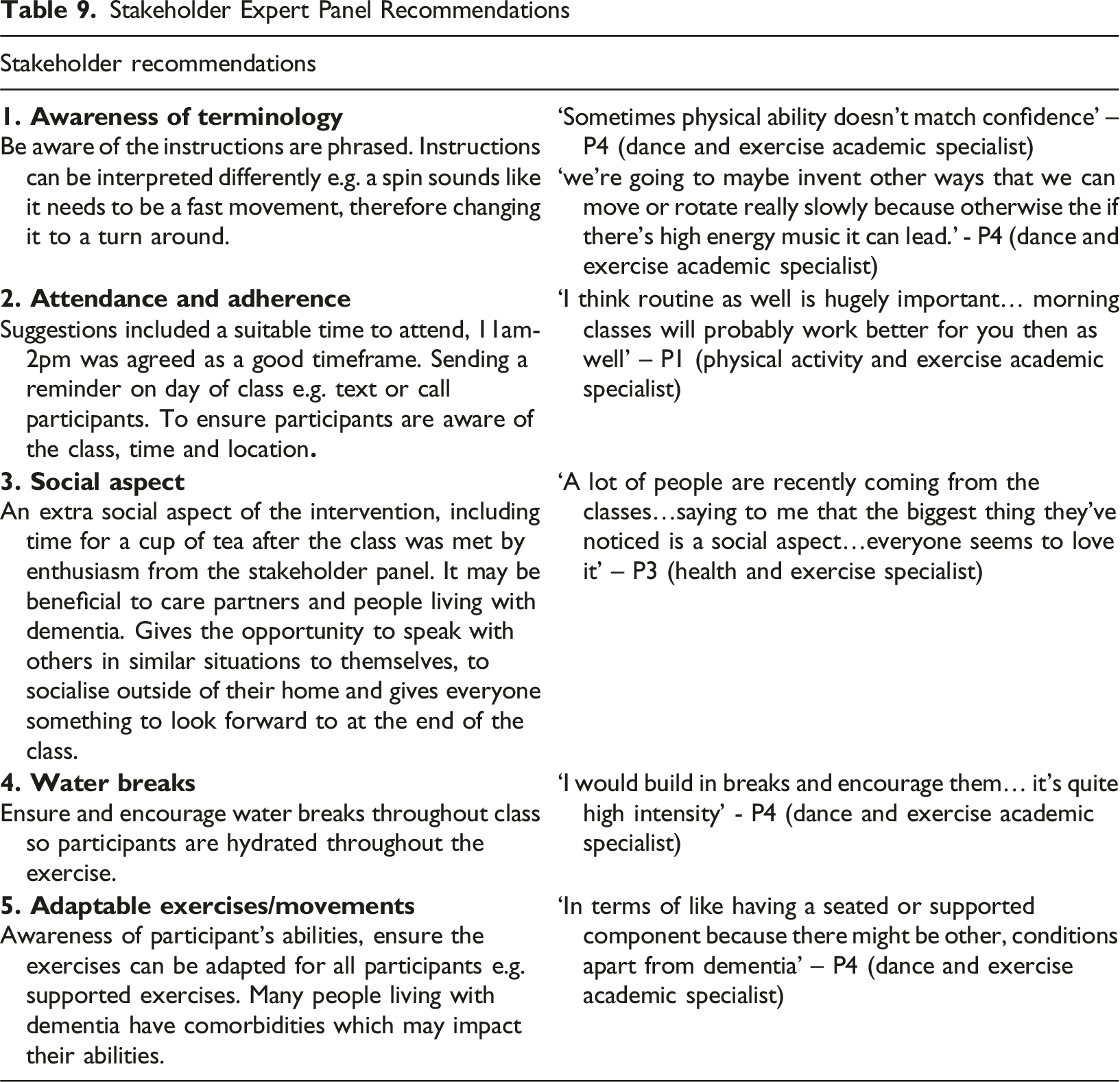
The final stage involved engagement with an expert stakeholder panel, including healthcare professionals and exercise professionals who worked with people living with dementia or who worked in the exercise and dance industry (n = 8). All stakeholders were recruited via email. The stakeholder panel discussion was held online via Zoom and lasted 1 hour and 16 minutes. The developed intervention components were presented and facilitated a group discussion based on their experiences. The discussion was transcribed. Stakeholder feedback was summarized into additional comments and recommendations incorporated into the intervention components.
Finalise Intervention Components
An updated version of the intervention components was presented to the PAG. The PAG discussed their thoughts on the practicality, accessibility and relevance of the developed intervention. Conclusive changes were made to the components based on their input, and the intervention was finalised.
Results
Stage 1. Identify Existing Evidence
Define Problem and Select Target Behaviour
The researchers identified the problem as follows: people living with dementia and their care partners face a high risk of low PA levels (Lindsay et al., 2022; van Alphen et al., 2016). Despite understanding the physical and psychological benefits of PAE, people living with dementia and care partners have low PA levels (Lambert et al., 2016; van Alphen et al., 2016). Evidence supports dance in particular as a form of PAE as it can benefit people living with dementia’s physical functioning, their mood and their social engagement, all of which positively influence their quality of life (Mabire et al., 2019; Wang, Song, & Niu, 2022; Wu et al., 2021). As a result, the target behaviour was to increase physical activity levels via a dance exercise intervention for people living with dementia and their care partners. Further evidence is provided in Supplemental File 3.
Specify the Target Behaviour
Alignment of Target Behaviour Specifications With Behaviour Change Wheel Criteria
Identify What Needs to Change
Literature Review Statements
Interview and Focus Group Recommendations
Stage 2. Develop Theory and Intervention Functions
The development of the intervention components followed a process of identifying COM-B constructs (2 (a)), which were mapped to BCW functions (2 (b)) and finally suitable BCTs to embed into the intervention were identified (2 (c)).
Aligning Gathered Data with COM-B Constructs
Mapping of BCW Constructs to Literature Review Statements and Interview and Focus Group Recommendations
Identify Intervention Functions
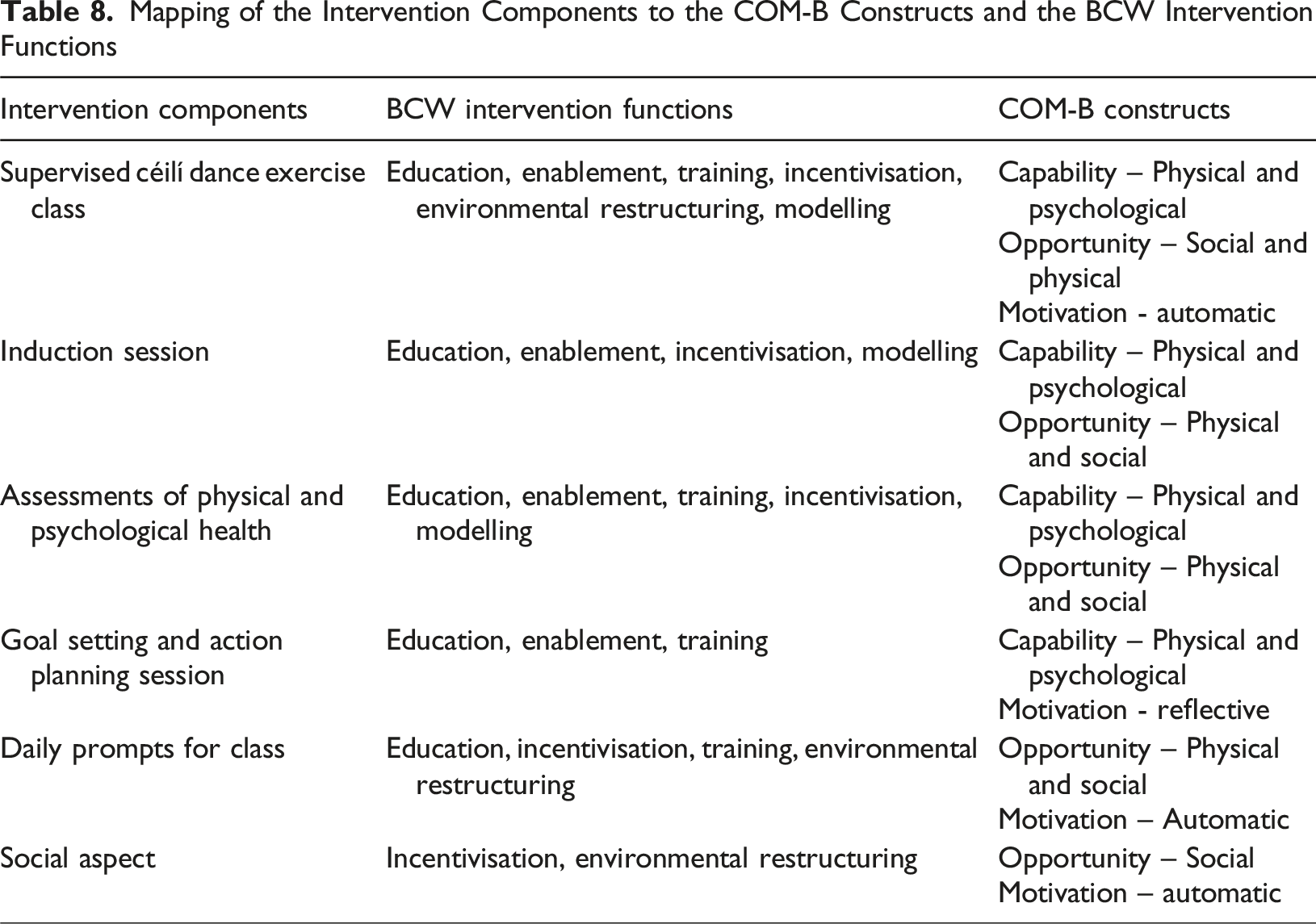
Six of nine possible intervention functions were selected based on the BCW framework guidelines, to support the selected COM-B constructs (Michie et al., 2011). These included education, enablement, training, incentivisation, modelling and environmental restructuring. The three intervention functions excluded—persuasion, coercion, and restriction—were deemed inappropriate for this intervention.
Identify Behaviour Change Techniques
Behaviour Change Techniques Alignment With APEASE Criteria
Stage 3. Modelling Process and Outcomes
Developed Draft Intervention Components
Mapping of the Intervention Components to the BCTS
Mapping of the Intervention Components to the COM-B Constructs and the BCW Intervention Functions
Engagement with Stakeholder Expert Panel
Stakeholder Expert Panel Recommendations
Finalise Intervention Components
The proposed intervention was presented to the PAG. Final recommendations were provided on each intervention component and the intervention in its entirety.
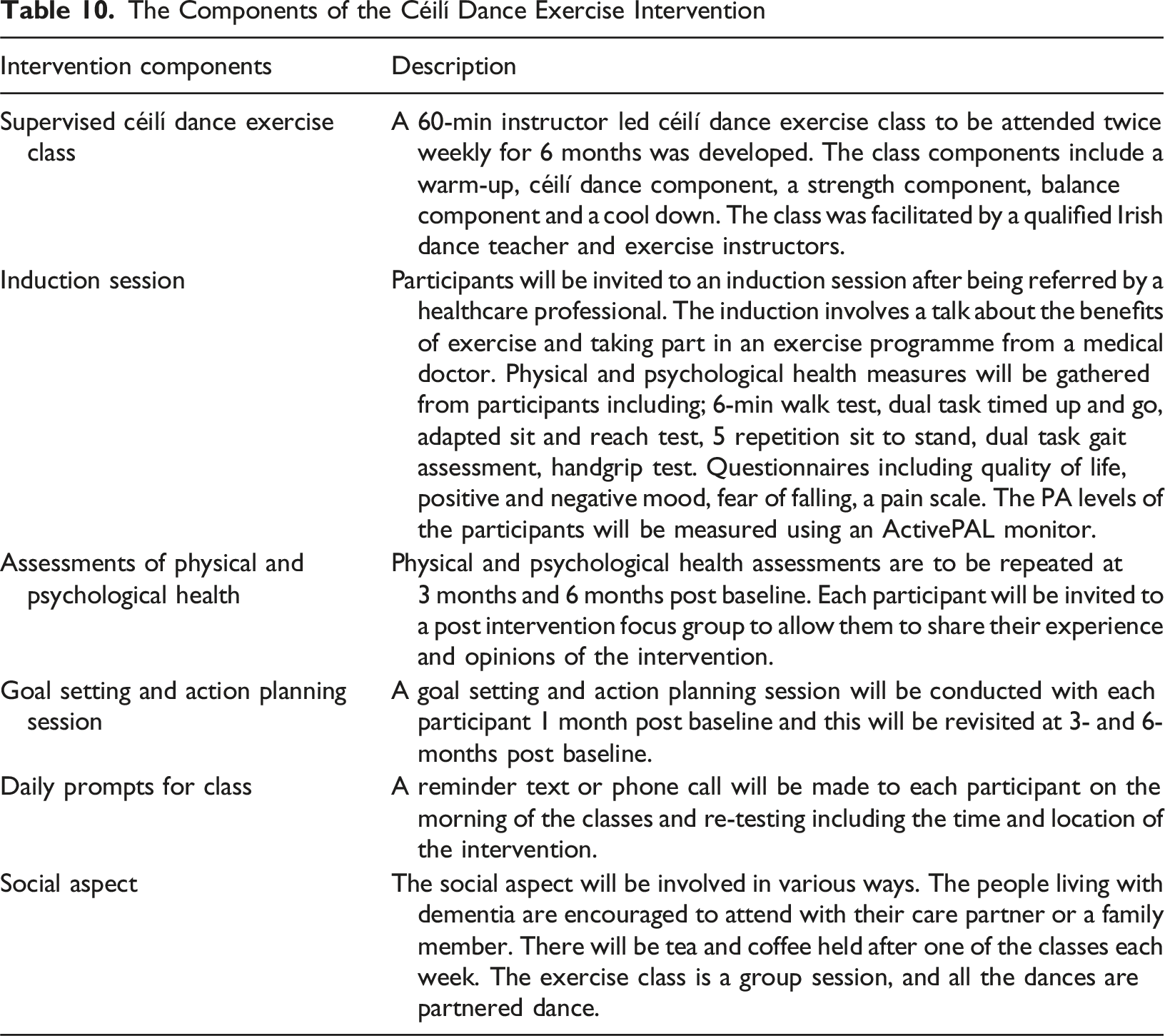
The Components of the Céilí Dance Exercise Intervention
Discussion
This study outlines the methodology used to develop a patient-centred dance exercise intervention for people living with dementia and their care partners. The aim of the intervention was to increase or maintain levels of PAE for this population. Interventions focused on PAE have significant potential to benefit people living with dementia and care partners through their physical and mental health including their ADL and QOL (Lambert et al., 2016; Liu et al., 2021; Petts & Urmston, 2022). The study employed the MRCF and the BCW to guide the development of an appropriate dance exercise intervention for the selected population. Based on the evidence from the literature review and the qualitative investigation, an intervention composed of six components was developed and linked to the COM-B constructs and BCW intervention functions. The intervention components include; a supervised dance exercise class, an induction session, assessments of physical and psychological health, a goal setting and action planning session, daily prompts for class and the social aspect.
Theoretically informed interventions may increase the efficacy of exercise-based behaviour change interventions (Charras et al., 2020). This intervention was developed by applying steps from the MRCF and the BCW framework (Michie et al., 2011; Shahsavari et al., 2020). The resulting intervention programme was evidence-based and specific to the needs of people living with dementia and care partners. The evidence base was gathered via a literature review. Focus groups and interviews with people living with dementia and care partners were conducted to understand the PAE perspectives and experiences of people living with dementia and care partners. Communicating with the target population was the best way to consciously involve their perspective and experiences with the hope of increasing attendance and adherence to this intervention (Bielinska et al., 2022). The BCW has previously supported the development of multiple PAE for various populations with specific requirements (Cantwell et al., 2020; Chen et al., 2022).
Studies for people living with dementia have not consistently engaged with people living with dementia in the development stages of research (Brooks et al., 2017). This study involved interviews and focus groups with people living with dementia and care partners, to understand their perspectives and what they want and require from a PAE intervention. Previously, care partners and healthcare professionals have been asked to give their opinions on behalf of this population. They have been asked to give proxy answers rather than involving people living with dementia (Ho et al., 2018). This emphasises the importance of involving people living with dementia, care partners and healthcare professionals at various points of the development to ensure different viewpoints are included. Combining methods qualitative data collection and PPI allows the intervention to be developed with insight into behaviour and this increases the quality and acceptability of the intervention (Biggane et al., 2019).
This study enlisted the expertise of a PAG, comprised of people living with dementia and care partners. The PAG gave their opinions on the research being conducted and implemented for the intervention development. Involving people living with dementia and care partners as part of the development process through PPI, assured the lived experience was included throughout the project. Establishing a PAG is becoming standard practice when engaging with diverse populations (Koskinas et al., 2022). The PAG in this study worked with the researchers to finalise the topic guides for the focus groups and interviews. This established all questions were appropriate in terms of content and language when engaging with people living with dementia and care partners. They discussed the developed intervention components with the researchers. Each component was considered in terms of practicality and reasoning. Possible barriers to attending the intervention were debated and potential feasible solutions were determined. This approach is increasingly valued because involving PPI has been shown to enhance both the research process and its outcomes. It further enhances the creditability and relevance of the research (Gove et al., 2018).
The qualitative data from this study highlighted the request from the people living with dementia and the care partners for a community-based, mixed population class. The social element of PAE is of particular importance for people living with dementia, as staying social and active within their community is imperative for good social and mental health (Pakstis et al., 2018). The social aspect of exercising in a group has been reported to add enjoyment to PAE for the participants (Fox et al., 2007). This shows there is a recognized need for interventions that incorporate social engagement to support individuals with dementia. Good social health positively influences both physical and psychological well-being (Joyce et al., 2022). Older adults with high participation in social activities in community groups, including PAE and non PAE based, experienced better QOL, higher self-esteem and stronger emotional and psychological support, along with greater muscle mass, better balance and improved cognition than those with low social participation (Sepúlveda-Loyola et al., 2020).
Previous evidence has stated despite the benefits, people living with dementia and care partners have low levels of PAE engagement (van Alphen et al., 2016). This is due to insufficient suitable support systems for this population in both rural and urban areas (Hobson et al., 2019). The results from the qualitative data in this study show people living with dementia, care partners and healthcare professionals understand the of importance of PAE for their health. One of the primary barriers to their PAE is the lack of tailored services. This emphasises the importance of developing a person-centred PAE intervention for people living with dementia and care partners.
Exercise and dance interventions have previously demonstrated increases in positive mood, improvements in agitation, anxiety and overall wellbeing (Bennett et al., 2021; Koh et al., 2020). The developed intervention from this study has the potential to positively effect people living with dementia and their care partners due to its patient-centred approach. The intervention is community based, it includes a social aspect and focuses on dance which is a social form of exercise. These points may motivate and support other psychological factors of the participants. This social element is vital for people living with dementia within their community as it reduces isolation and fosters social interaction with others (Cooper & Thomas, 2002). There is a need for PAE intervention for people living with dementia and care partners as they can have a positive impact on their life.
Strengths and Limitations
This study utilized the effective and feasible methodologies of intervention design by implementing the use of the MRCF and the BCW framework (Michie et al., 2011; Shahsavari et al., 2020). These frameworks use a structured evidence-based approach while allowing adaptation and flexibility for different populations and styles of interventions. The sample of participants involved in the focus groups and interviews were previously involved in PAE throughout their lives and therefore may have had focused on a more positive outlook on PAE than the wider population. This may be because this sample of people were more willing to speak about their previous PAE experiences due to their positive nature. The recruitment timeline was long for the number of participants recruited. The recruitment of people living with dementia for the interviews and focus groups resulted in lower numbers than expected for the qualitative analysis.
Conclusion
This study aimed to develop a relevant, effective, person-centred dance exercise intervention for people living with dementia and care partners by integrating developmental theory and practice. The intervention included six intervention components: a supervised dance exercise class, an induction session, assessments of physical and psychological health, a goal setting and action planning session, daily prompts for class, and a social aspect. These components structure a dance exercise intervention intending to increase the physical activity levels of people living with dementia and care partners. The next step involves implementing and evaluating this intervention in a practical setting. Future research should assess the feasibility and effectiveness of implementing this type of intervention with people living with dementia and care partners.
Supplemental Material
Supplemental Material - The Development of the Dance Smart Intervention: A Céilí Dance Exercise Intervention for People Living With Dementia and Their Care Partners (Dance Smart Intervention)
Supplemental Material for The Development of the Dance Smart Intervention: A Céilí Dance Exercise Intervention for People Living With Dementia and Their Care Partners (Dance Smart Intervention) by Niamh Kelly, Fiona Skelly, Kieran Dowd, Desmond O’Neill, Noel McCaffery, Clare McDermott in Dementia.
Footnotes
Ethical Considerations
This research ethics was approved by The Technological University of the Shannon Research Committee. All respondents gave either written or verbal consent before participating in this research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Technological University of the Shannon President’s Doctoral Scholarship.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset generated during the current study is not publicly available due to the involvement of a vulnerable population. Access of the data is restricted to safeguard the wellbeing of the participants.
Supplemental Material
Supplemental material for this article is available online.