
Abstract
Little is known about how health and social care professionals assess and respond to the caregiving needs of men who care for a family member living with dementia. This study aimed to address this research gap using a qualitative research methodology over two phases. Phase one comprised an online survey with 53 health and social care professionals. Open-ended survey responses were analysed via inductive content analysis and close-ended responses were analysed using descriptive statistics. Phase two comprised semi-structured interviews with five participants from phase one and interviews were analysed using thematic analysis. Health and social care professionals suggested that a spectrum perspective (ranging on a continuum from ‘care-manager’ to ‘care-provider’) could illustrate how people approach dementia caregiving. They suggested that socially constructed gender norms and the care partner’s kinship to their care recipient are key factors that influence where care partners stand along that continuum. For example, participants felt that men often abide by masculinity norms and tend to adopt a care-manager approach, with sons typically standing further down the care-manager end of the spectrum compared to husbands. Most participants acknowledged having adjusted their own clinical practice to match the care-manager approach used by male care partners. Participants recommended that health and social care professionals could optimise how they assess the needs of male care partners by adopting a task-focused rapport building approach; providing solution-focused advice; and proactively linking male care partners to formal and informal supports. These recommendations could inform future service developments to improve supports provided to male dementia care partners.
Worldwide, almost two-thirds of people living with dementia are women and most are cared for by a close family member, typically a spouse or an adult child (Alzheimer’s Disease International, 2015; Australian Institute of Health and Welfare, 2024; World Healthcare Organisation, 2023). Research suggests there has been an increase in the number of men as care partners since the 1990s (Brodaty & Donkin, 2009; Kramer & Thompson, 2002; Pöysti et al., 2012), presumably because more women have entered the workforce and are less readily available as care partners (Barg et al., 2014; LaManna et al., 2024; Manchester et al., 2019; Nayak, 2023; U.S. Bureau of Labor Statistics Report, 2021; Wang et al., 2013; Workplace Gender Equality Agency, 2022). For example, in the United States of America, between 1987 to 2015, the proportion of women care partners decreased from 75% to 60% (Barg et al., 2014; National Alliance for Caregiving, American Association of Retired Person, 2020) and in 2015, men made up 40% of American family care partners representing a 21% increase since 1996 (Alzheimer’s Association, 2008; Brodaty & Donkin, 2009; National Alliance for Caregiving, American Association of Retired Person, 2015). In Australia and the United Kingdom, men aged 75 and over are now more likely than women of the same age to care for their spouse (Australian Bureau of Statistics, 2022; Fee et al., 2021; Office for National Statistics, 2019).
However, men (especially older men), tend to hide their caregiving responsibilities behind a female family member (typically a daughter or sister) who is generally appointed as the official care partner, while these men keep providing care, but as an “invisible” care partner (Kokorelias et al., 2021; Kramer & Thompson, 2002; Milligan & Morbey, 2013, p. 28). As such, the number of male care partners is likely underestimated (Hutchinson, 2005; Lin-Fisher, 2025; Poisson et al., 2023; Schwartz & McInnis-Dittrich, 2015) and men are often underrepresented in dementia care partner research (Kramer & Thompson, 2002; Robinson et al., 2014; Tolhurst & Weicht, 2023).
Male care partners of people living with dementia have been reported to adopt a different caregiving approach compared to female care partners (Baker et al., 2010; McDonnell & Ryan, 2014; Poisson et al., 2023; Robinson et al., 2014; Tolhurst & Weicht, 2023). The development of a caring identity and “capacity to care”, are strongly anchored on the subjective socio-cultural meanings of gender (Bueno, 2024; Hollway, 2007, p. 1; Mahalik et al., 1998). Historically, women have been described as having an innate ability to nurture – a “maternal instinct” – because of their biological ability to give birth and to feed the infant (Shields, 1975, p. 739). This perspective of a woman’s “hardwired” natural reproductive role (Boise, 2015, p. 8) has contributed to a “paradigm of care”, which has shaped caregiving as a feminised activity and where women feel compelled to take-on caregiving (Barg et al., 2014; Hollway, 2007; Kramer & Thompson, 2002; Nayak, 2023, p. 169).
The Gender Role Conflict Theory (O’Neil, 1981), posits that socially constructed values of masculinity have led to a “devaluation” of feminine traits (p.203) and that caregiving is perceived as a feminine role (Baker et al., 2010). Men’s gender role conflict may be related to a “defense mechanism” against the shame and anxiety of performing a women’s role (Baker et al., 2010; Mahalik et al., 1998, p. 249; O’Neil, 1981). Similarly, Connell (1995) Hegemonic Masculinity Theory suggests that society has empowered men to abide by rigid patterns of masculine practices and “ways of being a man”, delineating men’s work from that of women and expecting men to maintain a distance from feminised roles (Connell & Messerschmidt, 2005, p. 837–840; Nayak, 2023). Therefore, to compensate for “non-masculine” (or “feminised”) behaviour – like caregiving – men will enact masculine traits of control, stoicism and independence (Baker & Robertson, 2008; Kramer & Thompson, 2002). For example, men are expected to have a natural ability to supress emotions and to keep their grief “secret”, because emotions are perceived as inherently feminine (Boise, 2015; Kramer & Thompson, 2002; Staudacher, 1991, p. 19).
Globally, women account for two-thirds of the health and social care workforce (World Healthcare Organisation, 2023). Literature suggests that some older men find it difficult accepting formal support from women – particularly “much younger women” (Macdonald et al., 2009, p. 17). In parallel, an implicit gender bias has been reported in clinicians’ approach towards their patients (Mahalik et al., 2012; Samulowitz et al., 2018) and some health and social care professionals reported finding it “harder to engage” with male care partners (Fee et al., 2021, p. 213). In a study which explored 59 counsellors’ insights on male and female counselling clients, the word ‘difficult’ was used 17 times to describe male clients, while only four times to describe females and these counsellors reported having more difficulty establishing a therapeutic relationship with men compared to women (Vogel et al., 2003). Research suggests that care partner support services have historically evolved to service their main client group of female care partners and are typically not “male friendly” and not designed to reach-out to men (Kaye & Crittenden, 2005, p. 100; Macdonald et al., 2009, p. 15; Mahalik et al., 2012; Malcher, 2005). Health and social care professionals should be informed of factors that may improve their clinical assessment of male care partners’ needs and consider making “male-friendly adjustments” to their practice (Mahalik et al., 2012, p. 597), which in-turn could facilitate timely care partner support interventions (Fee et al., 2021; Kaye & Crittenden, 2005).
Male care partners of people living with dementia have been reported to adopt a different caregiving approach compared to female care partners (Baker et al., 2010; McDonnell & Ryan, 2014; Poisson et al., 2023; Robinson et al., 2014; Tolhurst & Weicht, 2023). However, there is a gap in the literature around understanding of how health and social care professionals approach their practice and what is needed to operationalise interventions for male care partners of people living with dementia (Bueno, 2024; Fee et al., 2021; Macdonald et al., 2009; Milligan & Morbey, 2016). O’Neil's (1981) Gender Role Conflict Theory and Connell’s Hegemonic Masculinity Theory (Connell, 1995; Connell & Messerschmidt, 2005), are the theoretical frameworks that underpinned the direction of this research. This study aimed to explore health and social care professionals’ insights regarding their experience of working with male care partners of people living with dementia. The study also aimed to capture health and social care professionals’ recommendations, on how to facilitate male-friendly approaches with male care partners of people living with dementia.
Method
Study Design
We applied an exploratory qualitative research methodology because there is limited literature on this specific research topic (Liamputtong, 2020; Sandelowski, 2010). This research was conducted over two sequential phases, with a “wide-angle lens” approach, maximising the capture of both focused and rich data (Braun et al., 2021, p. 643). Phase one comprised an online survey, while phase two comprised semi-structured interviews with a sub-sample of participants from phase one.
Participants and Recruitment Strategy
Given that dementia is a syndrome that affects people of various age groups and leads to a multitude of symptom presentations (Emmady et al., 2022; National Institute on Aging, 2022), people impacted by dementia and their care partners may need to access multiple support services and are likely to be assessed by professionals across different sectors like the aged care, community care, disability care, health care and primary care sectors (Ashbourne et al., 2021; De Poli et al., 2020; King et al., 2024; Travers et al., 2025).
For researchers, there are often significant barriers to initiating contact with professionals in these sectors, especially if no “a-priori” relationship exists between the research team and the participants’ workplace (Bruneau et al., 2021; Hysong et al., 2013, p. 4; Krebs et al., 2021). To address these potential recruitment barriers and to align with the qualitative nature of this study, a targeted “snowball sampling” strategy was applied (Bruneau et al., 2021; Palinkas et al., 2015, p. 3; Stratton, 2024). The study was promoted via the social media page of an Australian dementia peak body and invited ‘health professionals’ who supported male care partners of people living with dementia to take part in the research, using an online survey. To maximise participant recruitment, the survey page remained open for one month, allowing “snowballing” of the hyperlink via the participants’ social media networks (Bruneau et al., 2021, p. 427).
The inclusion criteria for health professionals in this study were that they should be aged 18 years or older; be employed (fulltime, part-time and/or casual) in the health, aged care and/or disability sectors; and as part of their paid profession, routinely (at least weekly) provide information, advice, education and support to care partners of people living with dementia. Given the research was unfunded, no compensation was provided to participants. To better reflect the multidisciplinary group of professionals who enrolled in this study, and to align with terminology used in similar research contexts (Bergmann et al., 2022; Stephan et al., 2018), we have adopted the term ‘health and social care professionals’ (rather than ‘health professionals’) to describe participants in this paper.
Phase One: The Online Survey
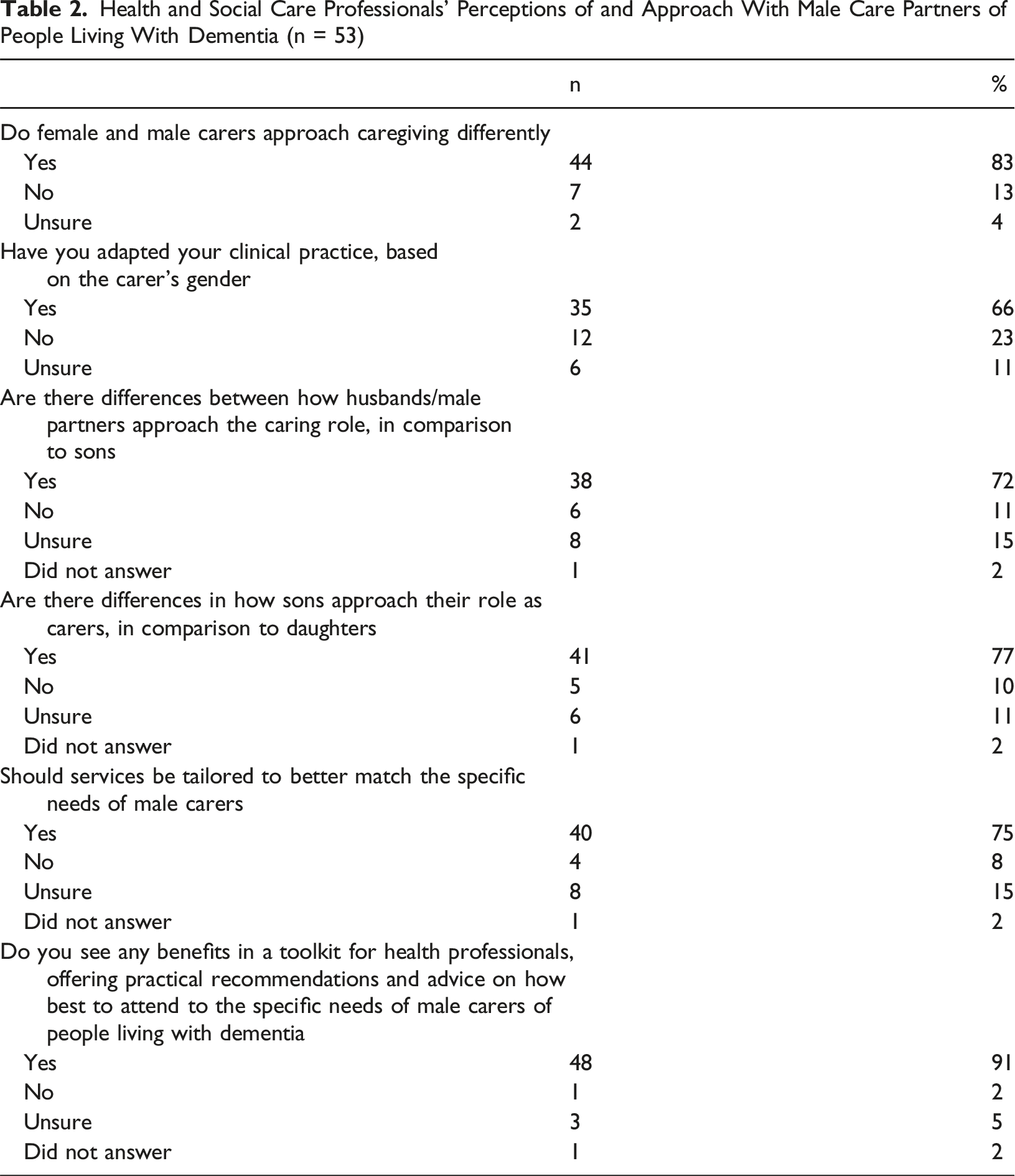
Braun et al. (2021) suggested that qualitative surveys (particularly online surveys), are compatible with qualitative values because despite being brief, they nonetheless facilitate access to data that range from people’s “material practices” to “meaning-making practices”, thus producing in-depth and nuanced insights (p. 642). In this study, each multiple-choice question included a ‘please explain’ open-ended free text option, which added richness and depth to the participants’ responses (Braun et al., 2021; Malterud et al., 2016). The questions were developed based on the research team’s dementia research and/or field experience. The questions aimed to capture whether health and social care professionals: had observed gender differences in care partners and accordingly modified their clinical approach; had observed differences between the approach of husbands/male partners and sons to caregiving; had recommendations about tailored interventions for male care partners; believed that a ‘toolkit for health and social care professionals’ would assist health and social care professionals to optimise their approach with male care partners. The survey was administered through the QualtricsXM survey platform (See Appendix A, for a copy of the survey questions).
Phase Two: The Semi-Structured Interviews
Once participants completed the online survey (phase one), a pop-up message invited them to express their interest in taking part in an interview (phase two). Five participants subsequently indicated their interest via email. Once the research team had completed a preliminary analysis of phase one data, these five participants were invited (via email) to take part in the research interview (via videoconference). This invitation contained a summary of preliminary results from phase one and a draft copy of a toolkit (because the survey results showed that almost all the survey participants indicated that a toolkit would have been useful to optimise their approach with male care partners). The content of this draft toolkit was informed from two sources: first, from participant quotes extracted from phase one survey responses; and second, by drawing on the literature and the authors’ field and research experience on male dementia care partners (Poisson et al., 2023). The first author is a qualified psychotherapist and conducted all five interviews. Before commencing each interview, the first author confirmed participants had read and understood the Participant Information Statement and Consent Form, which included key information about the research process, like risk mitigation. The first author guided participants to share their first impressions of the results and to offer recommendations on the ideal content and format of a toolkit designed to facilitate health and social care professionals’ interactions with male care partners. Most interviews took approximately 45minutes.
Consent and Ethics Approval
The University of New South Wales Human Research Ethics Advisory Panel granted ethical approval of this research project (HC220247). People who visited the online survey’s landing page were directed to read the Participant Information Statement and Consent Form before proceeding to the survey questions. Survey completion and submission served as evidence of implied consent. At the end of the survey, a message popped up, inviting participants to read the Participant Information Statement and Consent Form for phase two and to express their interest in phase two via email (their email was recorded as written consent).
Data Analysis
Phase One
The raw data from the online survey responses were exported from the Qualtrics XM Software onto an Excel spreadsheet. Individual responses were labelled using the initial ‘SP’ (short for Survey Participant) and an identification number assigned using the chronological order of their survey submission date and time. Descriptive statistics in the form of percentage figures were used to demonstrate the proportion of participants who responded across the various survey questions.
Inductive content analysis was applied to the open-ended survey responses, as recommended for small scale health-related studies with text-based data (Elo & Kyngäs, 2008; Hsieh & Shannon, 2005; Vears & Gillam, 2022). Inductive content analysis of research data is generally represented as “content-categories” – broad ideas or big-picture concepts – rather than ‘themes’ (Vears & Gillam, 2022, p. 115). Data coding was built-up inductively, as data arose from reading the open-ended responses and then, content categories were created by comparing, grouping and sub-dividing groups of codes over the course of the analytic process (Vears & Gillam, 2022). Interpretation of data was aimed at creating rich narrative answers to the main research questions and then, an “abstraction process” was used to generate main categories using content-characteristic words (Elo & Kyngäs, 2008, p. 111; Liamputtong, 2020). Analysis of these content categories informed the first author’s direction and focus during the one-to-one interviews (Braun et al., 2021; Safdar et al., 2016).
Phase Two
Interview recordings were transcribed by the first author and then exported to NVivo-12. Interview participants were de-identified using the initial ‘IP’ (short for Interview Participant) and an identification number assigned using the chronological order of their interview date and time. Braun and Clarke’s (2006) six step thematic analysis guided the generation of themes. Given that we had already captured rich data from 53 survey participants (under phase one), the research team was satisfied that relevant data saturation and richness were reached to address the research aims after the fifth interview (Malterud et al., 2016, p. 1754; Morse, 2015).
Findings
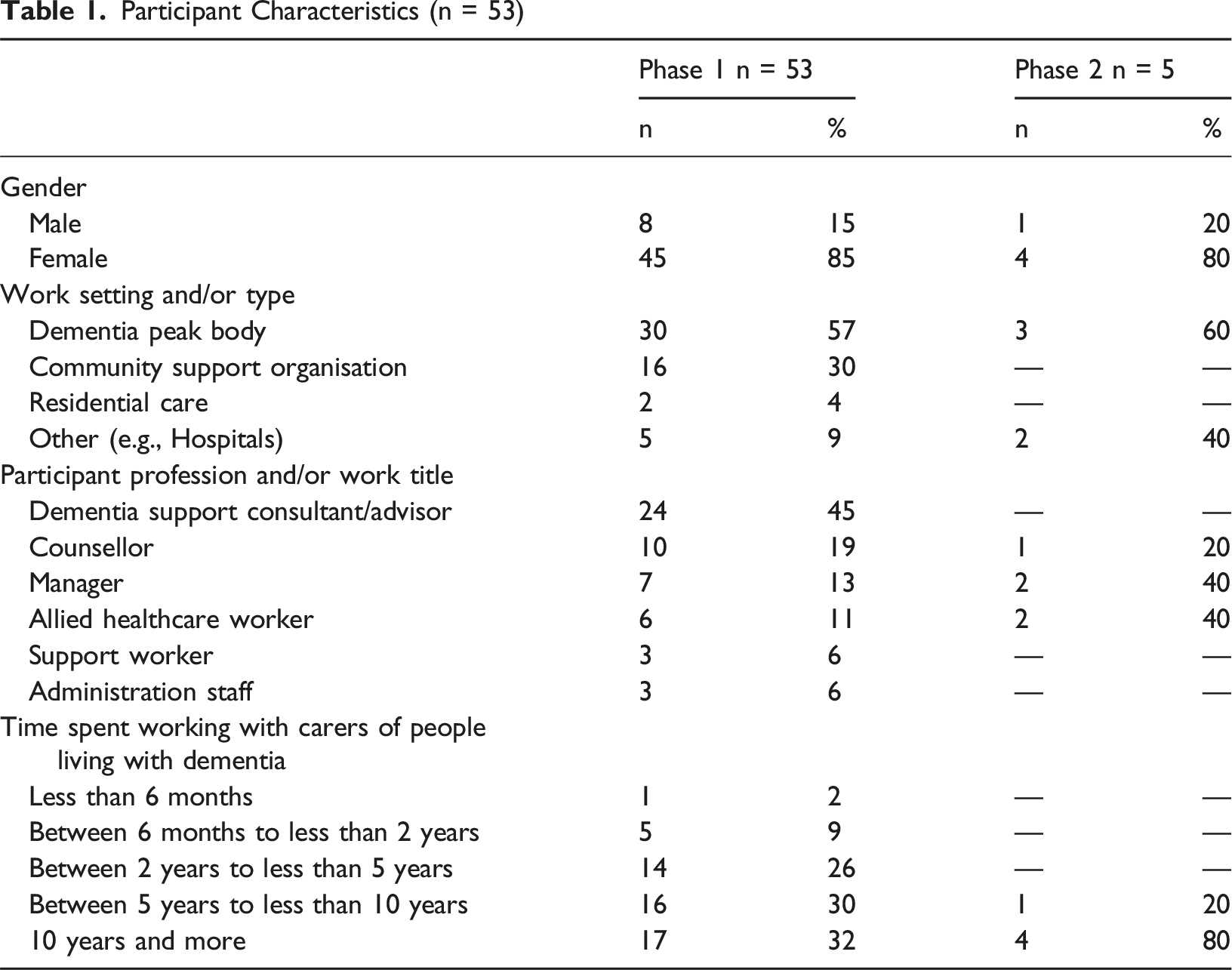
Participants’ Characteristics
Participant Characteristics (n = 53)
Descriptive Statistics of Online Survey Responses
Health and Social Care Professionals’ Perceptions of and Approach With Male Care Partners of People Living With Dementia (n = 53)
Phase 1 Qualitative Results: Inductive Analysis of Online Survey Questions
Content Categories
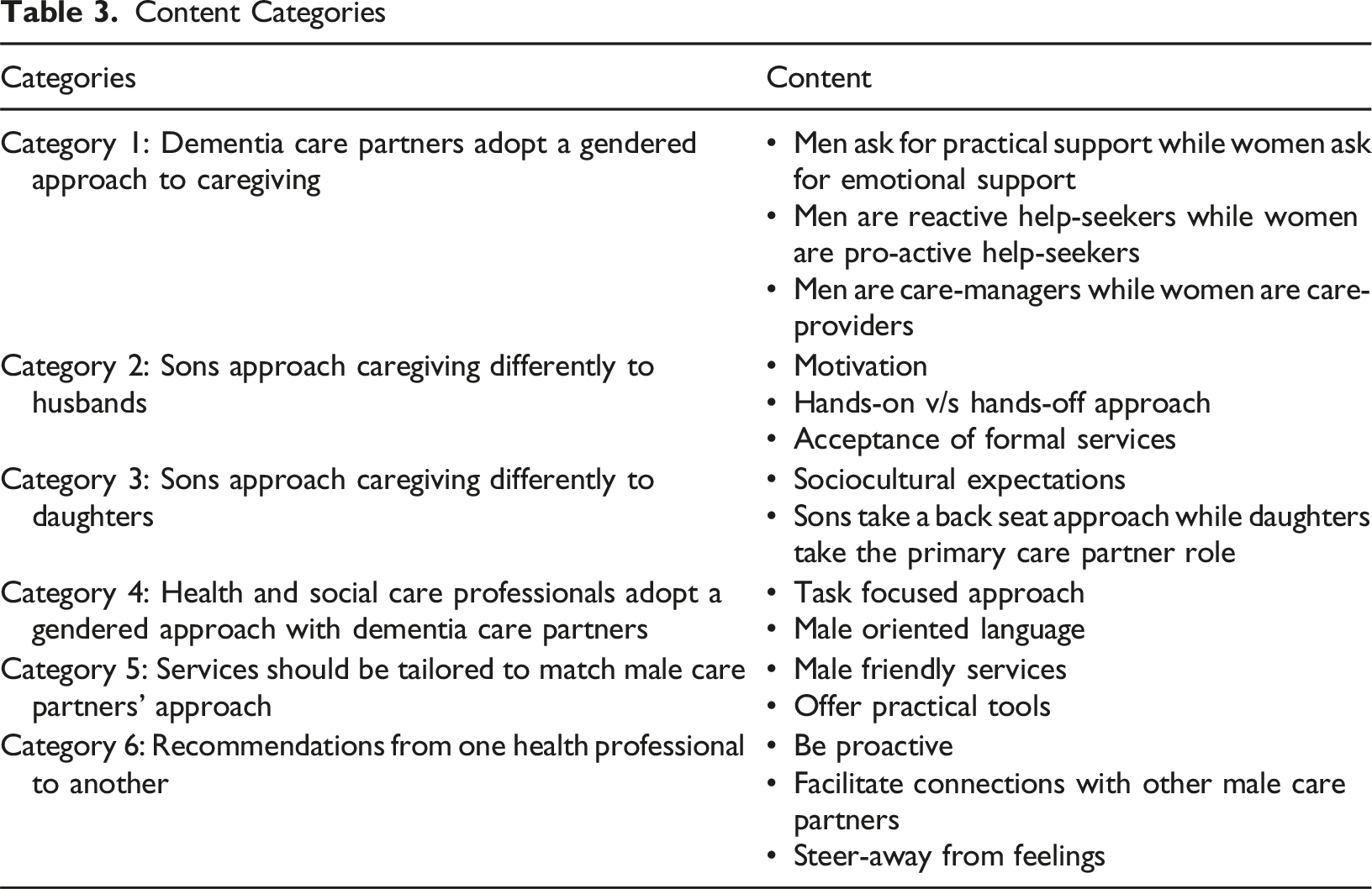
Category 1: Dementia Care Partners Adopt a Gendered Approach to Caregiving
Men Ask for Practical Support While Women Ask for Emotional Support
Participants believed that male care partners typically seek assistance for “practical support [and are] not keen to discuss feelings” (SP12), while females “would primarily focus on how they are feeling” (SP8).
Men Are Reactive Help-Seekers While Women Are Pro-Active Help-Seekers
Participants believed that “a great deal of males do not identify as ‘carers'” (SP14) and tend to “wait a long time to ask for help” (SP18). In contrast, female care partners tended to be perceived to be “proactive in seeking help” (SP39).
Men Are Care-Managers While Women Are Care-Providers
Participants suggested that in general, males tend to operate as “care-managers” (SP10) – focussed on coordinating and implementing support services – whereas females operate as “care-providers” (SP10), typically engaged in providing more personal, day-to-day care duties. For example, one participant said: “Daughters usually play the role of caring while sons have a higher possibility of managing finances” (SP43). As such, participants suggested applying a spectrum perspective to caregiving, ranging from “care-manager to care-provider” (SP10).
Category 2: Sons Approach Caregiving Differently to Husbands
Motivation
Participants believed that husbands are motivated to care, by “love and respect” (SP44) for their wife and typically “take on the job of caring” (SP19) because it forms “part of their marriage vows to care for their wife” (SP5). Participants stated that “sons struggle more with the transition from being a child to being a carer” (SP33) and tend to “care from a distance” (SP35) unless “they have to'' (SP44) because there is no one else in the family.
Hands-On v/s Hands-Off Approach
Participants said that husbands/male partners provide more “hands-on” (SP45) personal care and “will care for longer” (SP34) compared to sons, who were described as “a bit more removed and less engaged in the actual ‘caring’ requirements” (SP45).
Acceptance of Formal Services
Participants said that husbands/male partners typically “decline support services until it gets to a crisis” (SP49), whereas sons are “more open to support services” (SP49). Sons were described as “often being time poor” (SP19) because they are “impacted by other life issues in regard to work, relationships, children, siblings” (SP52). Compared to husbands/male partners, sons will step-into the caring role “as a last resort” (SP44) and once they do step-in, they will more readily “acknowledge the changes” (SP2) in their parent with dementia and look for “quick fix solutions” (SP37), typically looking for ways to delegate the care duties.
Category 3: Sons Approach Caregiving Differently to Daughters
Sociocultural Expectations
Participants identified that the caring role may still be influenced by “cultural norms” (SP52) and this role “falls naturally” (SP15) to daughters who typically “take on a mothering role” (SP24) because they are “more emotionally in touch” (SP11) and “will manage everything they can” (SP20). On the other hand, sons “take-on traditional male roles” (SP10) generally adopting a “task-minded” (SP12) approach, by managing “the practical things like finances” (SP20). Participants believed that due to sociocultural norms “daughters might be praised for their caring role, while sons maybe questioned” (SP52).
Sons Take a Back Seat Approach While Daughters Are the Primary Care Partners
Participants believed that sons “seem to take more of a back seat approach” (SP45) to caregiving compared to daughters, because sons are generally reluctant to assist their parent with personal care duties – “especially mothers” (SP30) - and will “default to their female siblings in terms of providing care and making decisions” (SP34). Daughters were described as generally being the “primary supporter” (SP15) and “more willing to take on the role” (SP36) compared to sons.
Category 4: Health and Social Care Professionals Adopt a Gendered Approach With Dementia Care Partners
Task Focused
Most participants stated that male care partners “respond better to a practical” (SP31) and “task focused approach” (SP33). Participants identified that they often had to go “straight to the point with men” (SP3), be “more direct and cut to the chase” (SP50) and generally adopted a more “practical” (SP7) approach with male care partners. Additionally, they modified “the nature of information, support and advice based on where the carer sits on the care-provider to care-manager spectrum” (SP10).
Male Oriented Language
Many participants flagged the importance of being “mindful of the language used when discussing personal issues” (SP25) and that “knowing the background of the carer” (SP25) could help to “find a shared language” (SP52) and facilitate the rapport with the male care partners. Participants stressed the importance of “using male oriented analogies” (SP44), particularly while “normalising the emotional side of the caring role for men” (SP15), for example a participant wrote the following comment: Working with a male carer who was an engineer who was fixated on utilising a protocol which was causing distress to both him and the person living with dementia…I utilised analogies of engineering concepts which allowed a shared language which eventually enabled discussion of grief and fear. (SP52)
Category 5: Services Should be Tailored to Match Male Care Partners’ Approach
Male Friendly Services
Participants overwhelmingly identified that “male carers have very different needs” (SP34) to female care partners and flagged that “male carers often become isolated, as they are less likely to reach out for support” (SP5). As such, participants suggested the importance of advertising “clearly labelled resources for male carers” (SP2) and “male only” (SP11) workshops which “connects men with other men who are carers” (SP5). Services should offer a “safe place to share their experiences and learn from each other” (SP50), “without fear of judgement” (SP26).
Offer Practical Tools
Participants suggested that male care partners need to see purpose to “commit to a program or intervention” (SP4) and therefore an “all-male group” (SP50) should “begin with a practical focus” (SP18), offering “tangible tools” (RP50) to address the caring role.
Category 6: Recommendations From One Health Professional to Another
Be Proactive
Participants advised other health and social care professionals to “be proactive with sharing resources, instead of waiting for them [male care partners] to ask questions” (SP26) and not to “rely on being asked for help, but to be observant and to detect any additional support needed” (SP22). For example, one participant wrote: “offer practical steps, programs or services that meet the identified goals first” (SP17).
Facilitate Connections With Other Male Care Partners
Participants advised other health and social care professionals to seek opportunities to “buddy-up male carers in male-focused groups” (SP42), “where they can see themselves belonging” (SP2) and “normalise that it is okay to get support” (SP15).
Steer-Away From Feelings
Participants advised other health and social care professionals to avoid delving “into the world of feelings” (SP35) until “rapport is built” (SP18). Participants advised to “go slow with emotion talk” (SP52) or “dwelling on their emotional needs” (SP18), but instead, “learn about their strengths and assist them to see that they can, and do, bring these to their caring role” (SP8).
Phase 2 Qualitative Results: Thematic Analysis of Semi-Structured Interviews
Based on the preliminary analysis of phase one data, interview conversations focused on capturing the participants’ insights and recommendations regarding the development of a toolkit to assist health and social care professionals better meet the needs of male care partners. Five key themes (considerations) emerged from these interviews: (1) designed as a ‘cheat sheet’; (2) start with a preamble; (3) invest time in rapport building; (4) engage in solution-focused conversations; and (4) facilitate connections with other male care partners.
Designed as a Cheat Sheet
Participants suggested that a toolkit should be designed as a “quick reference” (IP2), a “one-pager” (IP5) document, like “a short cheat sheet” (IP3). Participants suggested using “guiding questions” (IP5) to provide “a rapid intervention” (IP3) in working with male care partners. One of the participants explained what they had in mind: I think of one page…just sort of the use of ‘Do’s and ‘Don’ts’… do this, maybe avoid doing that, umm yeah, just really simple… just a few pointers to sort of guide you. (IP1)
Start With a Preamble
Participants suggested that a toolkit should start with “a preamble section… an introduction” (IP3), to advise health and social care professionals that male care partners do often approach caregiving differently to female care partners. Health and social care professionals should be advised that gender norms, along with the care partner’s kinship to the person living with dementia, might influence where the care partner sits on the “care-provider to care-manager spectrum” (IP3) approach to caregiving. Participants suggested that male care partners typically sit “further down on the care manager spectrum and females sit towards the care provider spectrum” (IP3).
Invest Time in Rapport Building
Participants stressed the need to “invest in these first steps of building rapport” (IP5) and to “avoid getting into a psychological rabbit warren of how people [male care partners] are feeling at this point in time” (IP3). Participants suggested that because “men in particular don’t feel confident as carers” (IP2) it is important to identify their strengths early in the rapport building process. Providing positive affirmation and encouragement and letting male care partners know that they are doing a good job, helps them to “sort of warm-up and loosen-up and become more comfortable knowing that they are not going to be hauled over the coals” (IP4).
Participants suggested that an effective strategy to facilitate rapport building with male care partners was to find ways to normalise conversations around help-seeking and where appropriate, to “speak to them in their language… to normalise by the use of analogies” (IP2). One of the participants gave the below example: It’s just like owning a car, you can keep driving the car until the car breaks down, or you can make sure it goes to the mechanic for the regular oil changes… regular services. It is exactly the same, you keep yourself running as a carer. (IP2)
Engage in Solution Focused Conversations
Participants recommended that the toolkit should assist other health and social care professionals in “staying solution focused” (IP3) because male care partners “want the tools… the strategies… something concrete to walk away with” (IP5). A participant said: “I’ve got to give them the right tool that they are going to pick-up and use. There’s no point in giving them an embroidery kit if they want a wrench” (IP2). Participants argued that male care partners tend to expect health and social care professionals to tell them “what assistance is available” (IP3) because “they just want it fixed; they want it all better” (IP5). One of the participants gave the below example: I am actually assessing their default strategies with coping with challenges and then, understanding where the shortfalls are in relation to caring for someone with dementia, so things that worked for them all their life, they are not working now, and I can figure-out why and that’s where I can be supportive…Like to me, that’s been a game changer…to actually shift what [I] am doing, rather than trying to bring the men to how I operate. (IP2)
Facilitate Connections With Other Male Care Partners
Participants in this study commented that male care partners typically “do better in groups where there is at least one other man, or ideally a bigger group of men” (IP1), because they “value peer support” (IP1) and want “to break the isolation” (IP5). Participants highlighted that male care partners will especially value insights and advice from “other men who are further ahead on the journey” (IP1), because these “more experienced men will have nuggets of gold that they can share” (IP1). Participants suggested that a toolkit should encourage health and social care professionals to offer “referral pathways” (IP4) to help male care partners connect with other male care partners.
Discussion
Health and social care professionals in this study reported that in their experience, men do approach caregiving differently from women. They suggested that a spectrum perspective, ranging from care-manager to care-provider approach, could be used to better understand this divergence in caregiving approach. Health and social care professionals suggested that men tend to operate at the care-manager end of the spectrum, while women typically operate as care-providers, at the opposite end of the spectrum. Health and social care professionals reported that men may respond better to professionals who are able to adjust their practices in a way that works alongside masculine identities. Therefore, to optimise their clinical practice when supporting male dementia care partners, we propose that health and social care professionals should adopt strategies like task-focused rapport building; providing directive solution-focused advice; and facilitating connections with other more experienced male care partners.
The present findings reinforce previous research, suggesting that socially constructed gender norms and the care partner’s kinship to the person living with dementia (e.g., spouse or child), are strong factors that influence the caregiving approach (Bueno, 2024; Kokorelias et al., 2021; Pinquart & Sörensen, 2006). Based on the Gender Role Conflict Theory (O’Neil, 1981) and the Caregiver Identity Theory (Montgomery & Kosloski, 2009), one could expect that men may experience a conflict of identity as they step-into the care partner role. Therefore, men may attempt to regulate this incongruence of identity by introducing masculine behaviours to the caring role (Baker & Robertson, 2008; Brown & Chen, 2008; Bueno, 2024). For example, acting as care-managers, men are likely to focus on finding ways to delegate certain aspects of the caregiving duties, like “letting others” (generally a daughter, sister, or other female) undertake the direct personal care, while they manage the finances and medical appointments (Brown & Chen., 2008, p. 844; Grigorovich et al., 2016; LaManna et al., 2024; Milligan & Morbey, 2016; Poisson et al., 2023). In contrast, women may be more likely to feel socially pressured to operate at the care-provider end of the spectrum, providing most of the caregiving duties themselves (Bartlett et al., 2018). The above reinforces previous research suggesting that male dementia care partners may become “transparent care partners” or “invisible” to health and social care professionals, if they do not perform the personal care tasks themself (Kramer & Thompson, 2002, pp. 24-26; Milligan & Morbey, 2016). We would therefore recommend that health and social care professionals should be mindful (when performing their assessments of needs with male care partners), not to develop a blinkered perspective and fail to recognise the “jobs that men usually do” as care partners, just because they may not be performing the personal care tasks or refuse services that are more oriented to female care partners (Milligan & Morbey, 2016, p. 11).
Compared to husbands who care for a spouse living with dementia, adult sons who care for a parent living with dementia typically face more competing life responsibilities (e.g., work commitments, child rearing responsibilities, financial strain) and therefore, may face more social pressures to enact their masculinity as the breadwinner for their own family (Grigorovich et al., 2016; Kwok, 2006; Mahalik et al., 2012; McDonnell & Ryan, 2014; Sanders & McFarland, 2002). Therefore, sons may be more likely to distance themselves from the active caring duties and more readily recruit professional support services to undertake these duties compared to husbands (Grigorovich et al., 2016; Kokorelias et al., 2021). The present findings support this characterisation, suggesting that sons are likely to step-into the caring role as a last resort (if no one else in the family is available), whereas husbands may interpret this new role as being part of their marriage vows and therefore enact the role of the masculine protector who stays true to his words (Bueno, 2024; Grigorovich et al., 2016). Additionally, health and social care professionals should be mindful that compared to sons, husbands may be more likely to delay access to formal care services and be somewhat more hands-on with personal care duties (Kokorelias et al., 2021). Sons who care for a parent living with dementia might sit further along the care-manager end of the spectrum compared to husbands.
Literature suggests that in the early stages of caregiving, men are less likely to express their feelings and emotions despite experiencing a high intensity of stress related to their caregiving experiences (Kramer & Kipnis, 1995; Pillemer et al., 2018). This might be so because patriarchal narratives of the “boys don’t cry” attitude (Boise, 2015, p. 45), demand that when men are faced with an adverse or problematic situation, they should remain stoic, avoid displays of emotion, and should instead focus their efforts on finding practical solutions to the problem (Bueno, 2024; Mahalik et al., 1998). Outcomes from the present study complement the literature, suggesting that health and social care professionals should be mindful that men may not feel confident as care partners and therefore, may be somewhat on the defensive and less likely to openly divulge their vulnerabilities, especially during the early rapport building process (Fee et al., 2021; Macdonald et al., 2009; Mahalik et al., 1998; O’Neil’, 2008; Poisson et al., 2023). Health and social care professionals should guide male care partners to describe occasions when they have successfully managed caregiving tasks (rather than focusing on failures), because getting the positive reinforcement from professionals might align with their masculine identity, thus facilitating confidence building and promoting future engagement with the worker (Addis & Mahalik, 2003; Connell, 2003; Mahalik et al., 1998).
Research suggests that generally, men who step into the caring role have had little-to-no prior experience with caregiving (Bueno, 2024). The present findings suggest that while performing their initial assessments with male care partners, health and social care professionals should facilitate directive solution-focused conversations which are geared towards achieving tangible solutions. Health and social care professionals should guide male care partners to identify their main concerns and then to prioritise the issues they want to ‘fix’, one at a time. The directive advice provided by health and social care professionals might help men to integrate a sense of control over the caring role, which would fit with masculine practices (Baker & Robertson, 2008; Brown & Chen, 2008; Mahalik et al., 1998). In addition, health and social care professionals could attempt to normalise the help-seeking process by using ‘male-oriented’ language related to the care partner’s work background, because men are likely to approach caregiving as a “job”, which helps them to de-feminise the caring role and to attenuate a sense of gender role conflict (LaManna et al., 2024, p. 282; Mahalik et al., 1998).
Masculinity norms value the concept of fraternity, mateship and mentoring, whereby from a young age, men are encouraged to associate with and learn from more experienced male mentors (Connell, 2003; Henderson et al., 2022). This might explain why some studies reported that male care partners typically prefer support interventions and services that give them an opportunity to: connect with other men who share similar experiences; facilitate skill building; and contribute their own knowledge with other men (Macdonald et al., 2009; Poisson et al., 2023). The present findings suggest that health and social care professionals should anticipate that men may be more likely to accept help if they are encouraged to connect with other male care partners, especially more experienced care partners.
Health and social care professionals in this study voiced strong support for the development of a brief toolkit which could be used to facilitate their practice when working with male dementia care partners. To the best of the authors’ knowledge, no evidence-based toolkit existed at the time of this study. The findings from this study, in parallel with the scientific literature, suggest that a toolkit would need to highlight that men are likely to abide by masculinity norms and therefore, are likely to experience a gender role conflict, which will influence how they approach caregiving (Bueno, 2024; Kokorelias et al., 2021; Mahalik et al., 2012). A toolkit could therefore offer solution focused strategies directed at addressing male care partners’ needs. Furthermore, a toolkit could leverage masculinity norms around the process of mentorship (Connell, 2003; Henderson et al., 2022) and offer strategies about how to encourage connections between male dementia care partners.
Implications for Practice
Male care partners of people living with dementia have identified an expectation that health and social care professionals should use their professional judgement to provide proactive advice about the type of services required to address current and future caregiving tasks (Poisson et al., 2025). The present study builds on this, suggesting that services should be tailored to match how male care partners of people living with dementia approach caregiving. We would encourage health and social care professionals, especially those working in the early post-diagnostic services, to anticipate that male care partners of people living with dementia are likely to act more as care-managers (than care-providers) and to therefore engaged in solution-focused conversations (rather than emotion focused conversations) to facilitate access to formal and informal supports. A toolkit which offers practical recommendations and advice on how to best attend to the specific needs of male care partners of people living with dementia may assist health and social care professionals to optimise their approach with this unique cohort of care partners of people living with dementia.
Limitations
Given the recognised recruitment barriers with health and social care professionals (Bruneau et al., 2021; Hysong et al., 2013; Krebs et al., 2021), a small sample was obtained for the online survey in this study. The concept of “Information Power” suggests that the more a sample holds rich information relevant to the study, the fewer the number of subjects required (Malterud et al., 2016, p. 1753). In this study both samples (for the online survey and the interviews), comprised of experienced health and social care professionals in the field of dementia (information rich samples) and therefore, both sample sizes were deemed as sufficient after one month (Braun et al., 2021; Malterud et al., 2016). However, we recognise that the present findings might not be representative of all health and social care professionals and may limit the extent to which these findings can be generalised. For example, our sample comprised mostly (64%) of Dementia Consultants and Counsellors and with a minority (11%) of Allied Health professionals, suggesting that the findings might not fully reflect the perspective of clinicians who routinely support male care partners of people living with dementia. Five individual interviews were conducted to further enrich and clarify the online survey data, but it is also possible that the findings were limited to five individual views. Future research might consider focus group interviews with health and social care professionals, to facilitate a ‘group effect’ and inductively identify common ground narratives to strengthen the data (Liamputtong, 2020, p. 78). Research suggests that female workers often find it more difficult to engage with male care partners (Fee et al., 2021; Samulowitz et al., 2018). Given that approximately 85% of participants in this study were female, it is possible that the study narrative might be skewed towards insights from female health and social care professionals. Further, our results could be limited by the health and social care professionals’ own perceptions of care as a gendered role, thus future research in this field would be strengthened by an exploration of this potential bias.
Conclusion
The present findings suggest that sociocultural norms of masculinity may influence how men approach caregiving and consequently shape their caregiving needs and the expectations they have of health and social care professionals. Male care partners may benefit from health and social care professionals who adopt male-friendly approaches. The findings could inform the development of evidence-based resources – like a toolkit – to assist health and social care professionals optimise their approach with male care partners of people living with dementia.
Supplemental Material
Supplemental Material - Health Professionals’ Insights on Men as Dementia Caregivers
Supplemental Material for Health Professionals’ Insights on Men as Dementia Caregivers by Vincent O. Poisson, Roslyn G. Poulos, Adrienne L. Withall, Leanne Emerson, Kaele Stokes, Claire M. C. O’Connor in Dementia
Footnotes
Acknowledgements
The research team would like to thank all the participants who volunteered their time taking part in this research. We would also like to thank Dementia Australia for the support to advertise this research, which helped with the recruitment of research participants.
Ethical Considerations
The University of New South Wales (Sydney) Human Research Ethics Advisory Panel granted ethical approval of this research project (HC220247).
Consent to Participate
People who visited the online survey’s landing page were directed to read the Participant Information Statement and Consent Form (PISCF) before proceeding to the survey questions. Survey completion and submission served as evidence of implied consent. At the end of the survey, a message popped up, inviting participants to read the PISCF for phase two and to express their interest in phase two via email (their email was recorded as written consent).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was unfunded and conducted as part of the fulfilment of the Doctor of Public Health (DrPH) program from Dementia Centre for Research Collaboration. Participants were not reimbursed for their participation, and their participation did not incur any expenses. CMCOC is a recipient of a (DCRC) Post-doctoral Fellowship (2022-26).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first author, Vincent O. Poisson (VOP), is currently employed full-time in a management role at Dementia Australia. Research participants were recruited using the research webpage and social media page of that organisation. However, prior to starting the survey, all participants were clearly guided to read the Participant Information and Consent form (which detailed the potential conflict of interest). Dr. Claire M.C. O’Connor (CMCOC) is a recipient of a Dementia Centre for Research Collaboration (DCRC) Post-doctoral Fellowship (2022-26). The authors report there are no competing interests to declare.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author(s) upon reasonable request and pending appropriate ethical approvals. Based on the findings from this research, a toolkit for health professionals was subsequently developed by Dementia Australia and is available at ![]() .
.
Supplemental Material
Supplemental material for this article is available online.