
Abstract
Introduction
In response to escalating healthcare costs driven by an aging population and a rise in chronic diseases such as diabetes and COPD, governments in advanced countries are actively pursuing or have already initiated a ‘digital transformation’ of their public healthcare systems.1–4 This transformation involves significant, often disruptive, changes in the delivery of healthcare services.5–7 The primary goals of this effort are to improve population health, enhance the efficiency and effectiveness of the healthcare system, and, most importantly, improve the quality, safety, and accessibility of public healthcare services. Consequently, many of these countries have adopted and implemented large-scale national electronic health record (NEHR) systems.8–12
Electronic health records (EHRs) are digital versions of patients’ medical records, containing comprehensive and real-time information about an individual’s health status. These records typically include a patient’s medical history, medications, treatment plans, immunizations, allergies, radiology images, and laboratory test results. 13 EHRs are designed to streamline healthcare processes, improve the quality of patient care, enhance data accuracy, and facilitate secure information sharing among healthcare providers. 14 This review focuses on NEHR systems, which are most often implemented under the responsibility of national health authorities. These systems typically make a patient’s medical history accessible to health professionals across healthcare institutions and provide linkages to related services such as pharmacies, laboratories, specialists, emergency departments, and medical imaging facilities. 15
The primary role of a NEHR system is to support the wide range of healthcare operations within a health system, whether public or private. It does so by creating a dynamic and comprehensive overview that facilitates the continuous monitoring and effective management of patients’ care trajectories. 16 As such, a NEHR system serves as the central information tool for healthcare professionals, including physicians, nurses, and other healthcare practitioners, as well as healthcare managers and policymakers. It is also the primary platform through which digital health services are delivered to both patients and the general population. NEHRs typically encompass three key functional domains: (1) clinical which includes clinical information systems (IS), clinical decision support systems (DSS), laboratory IS, picture archiving and communication systems (PACS), pharmacy IS, and e-prescribing; (2) informational/communicational which encompasses hospital dashboards, big data analytics, patient portals and mobile applications, and teleconsultation platforms; and (3) managerial/administrative which includes operating room management, patient scheduling and appointment management, clinical documentation, and patient records management.
According to the ISO standard on EHRs, 17 NEHR system implementation initiatives can be characterized by two key dimensions: (1) scale, which refers to the geographical reach of the implementation and the number of public healthcare institutions involved, and (2) functional and institutional scope, which encompasses the system’s range of functionalities and the types of public healthcare institutions in which it is deployed, including secondary, tertiary, and primary care settings. Additionally, a NEHR system may incorporate a national health information exchange (HIE)—a health information infrastructure that facilitates interoperability with electronic medical records (EMRs) 18 and personal health records (PHRs) 10 at various levels, such as national, provincial, state, or regional.11,19,20 Ensuring interoperability across public health data and systems is therefore a critical requirement for the successful implementation and adoption of a NEHR system.21,22
Past NEHR implementation initiatives are often described as “wicked projects” due to their inherent complexity and multifaceted nature. These projects demand coordination and collaboration among multiple stakeholder groups, whose diverse and evolving needs must be managed from inception through implementation.23,24 For example, Cresswell et al. 1 observed that “large-scale digital transformation initiatives have typically struggled to balance national priorities with local needs” (p. 200). The complex nature of these initiatives has sometimes led to unintended consequences, such as unmet expectations, reduced clinical innovation, physician burnout, and data obfuscation. 25 Further, NEHR implementation and adoption processes involve multiple stakeholders, encompass a broad range of clinical, communicational, and managerial functions across various healthcare institutions, and often unfold over extended periods. As a result, evaluating these processes—and particularly the EHR software being implemented—requires a nuanced approach and appropriate methodologies.26–28
Despite extensive research on EHR adoption, a fragmented understanding persists regarding how large-scale NEHR initiatives unfold in practice, particularly in terms of stakeholder engagement, governance strategies, and balance between standardization and local adaptation [for example, 29–33]. Existing studies often focus on isolated case studies or specific technical aspects, leaving policymakers and practitioners without a synthesized, context-sensitive framework to guide future implementations. To bridge this gap, our review systematically examines empirical evidence from past NEHR initiatives to identify critical knowledge-practice gaps and provide actionable insights. By addressing key challenges—such as implementation barriers, decision-making complexities, and best practices—this study equips policymakers, healthcare professionals, and EHR providers with evidence-based guidance for successful large-scale NEHR deployments.
Our study has both descriptive and prescriptive objectives. First, we aim to identify and characterize NEHR implementation initiatives in public health systems, focusing on their context, scale, scope, and key aspects of the implementation and adoption processes. Second, we seek to contextualize large-scale NEHR initiatives by distilling lessons learned from their implementation and adoption, such as barriers and facilitators. This approach enhances our understanding of how these systems have been implemented and adopted across different countries, prioritizing process insights over outcome evaluations. Guided by these objectives, our study addresses the following questions: (1) Which advanced countries have completed or are currently implementing NEHR systems? (2) What defining characteristics shape these NEHR systems in terms of scale and scope? (3) What critical elements have emerged before or during implementation and adoption? and (4) What practical recommendations and insights can be drawn from the surveyed NEHR initiatives?”
In short, this review makes several key contributions to the understanding of NEHR implementation. First, it synthesizes empirical evidence from multiple large-scale NEHR initiatives, offering a structured analysis of the sociotechnical factors that influence success. Second, it provides actionable recommendations for policymakers, healthcare managers, and IT practitioners by identifying key success factors, barriers, and strategic considerations for effective implementation. Finally, it addresses critical knowledge-practice gaps by highlighting unresolved issues and future research directions, ensuring that upcoming NEHR initiatives are better informed and contextually adapted to real-world healthcare settings.
Materials and methods
Aligned with our research objectives and questions, this review adopts an analytical framework based on the critical sociotechnical dimensions of NEHR implementation, as identified by Deutsch et al. 34 Given the complexity of these initiatives, we analyze NEHR implementation processes across key dimensions, including scale and scope, stakeholder involvement, implementation strategy, project and change management, EHR software solutions, benefits realization, success and failure factors, barriers and facilitators, and key lessons learned.
To provide actionable insights for policymakers, decision-makers, and system practitioners on NEHR implementation, we adopted a rapid review approach. Unlike systematic reviews, rapid reviews are conducted within a shorter time frame, use a streamlined search strategy, apply more restrictive inclusion criteria, and may involve a single reviewer. 35 They also simplify or omit certain quality assessments, focus on descriptive synthesis, and prioritize timely, decision-oriented evidence for health policymakers, managers, and professionals. 36 More specifically, this review was designed to inform health policymakers, health system managers, health IT project managers, and an action research team involved in an upcoming NEHR implementation initiative in Québec, Canada.
Based on our prior delineation of a full-fledged NEHR system 15 and the methodological principles of our rapid review approach,35,36 we focused on NEHR implementation initiatives in advanced countries with public health systems, excluding the United States and developing countries. The U.S. healthcare system is uniquely decentralized and fragmented, dominated by the private sector, and lacks a single NEHR system.2,3 Meanwhile, developing countries face resource constraints, infrastructural challenges, and generally low levels of digital maturity.37,38 Since rapid reviews aim to extract lessons from comparable settings,35,36 this exclusion ensures a more focused analysis of advanced countries with centralized health systems, standardized policies, and government-led NEHR initiatives. In turn, this enhances the relevance and applicability of our findings for policymakers, healthcare managers, and professionals.
Search
The Scopus, PubMed, Medline, and CINAHL bibliographical databases were initially searched on February 1, 2024, and subsequently updated on September 7, 2024, using the following query syntax: ((“large-scale electronic health record”) OR (“large-scale EHR”) OR (“nation* electronic health record”) OR (“nation* EHR”) OR (“country* electronic health record”) OR (“country* EHR”) OR (“state* electronic health record”) OR (“state* EHR”) OR (“provinc* electronic health record”) OR (“provinc* EHR”) OR (“region* electronic health record”) OR (“region* EHR”) OR (“interoperable electronic health record”) OR (“interoperable EHR”) OR (“nation* health information exchange”) OR (“nation* HIE”) OR (“large-scale health information exchange”) OR (“large-scale HIE”)) AND (“implement*” OR “adopt*” OR “use” OR “evaluat*” OR “assess*” OR “realis*” OR “realiz*” OR “benefit” OR “project” OR “Epic” OR “Cerner” OR “Meditech”)
The search initially identified 1529 English-language documents. After removing duplicates, 718 documents remained for screening.
Screening
The research articles selected for review had to meet the following eligibility criteria: • Focus on NEHR Implementation/Adoption • Scale of the NEHR System • Functional Scope • Institutional Scope • Developed Country Context • Qualitative Empirical Data
The article selection process followed a two-stage screening approach. One reviewer initially assessed the eligibility of 718 documents based on their titles and abstracts, excluding those that did not meet the criteria. From this pool, 48 documents advanced to the full-text screening stage for further evaluation. After this second review, 24 documents were excluded, resulting in a final sample of 24 articles. The search and screening process is summarized in Figure 1. Flow diagram.
Quality assessment
The Joanna Briggs Institute Checklist for Qualitative Research 39 was used to evaluate the quality of the 24 included studies. This tool, consisting of 10 items, is designed to systematically assess a study’s conceptual, methodological, and ethical aspects, with a particular focus on evaluating its methodological quality and potential for bias. Two reviewers jointly reviewed each of the checklist’s 10 items to assess three randomly selected studies. After this initial discussion, they independently applied the checklist to evaluate the remaining 21 studies, achieving a 94.5% agreement across all assessed items. Any discrepancies were resolved through further discussion.
Data extraction and data synthesis
We employed qualitative content analysis to interpret textual data through systematic coding and the identification of themes and patterns. Specifically, we used a summative approach to content analysis, as defined by Hsieh and Shannon. 40 In this method, coding categories (e.g., NEHR systems, implementation strategies, critical success factors) were developed based on the researchers’ interests and initial research questions, with iterative refinements made before and during data extraction and analysis. Initially, one author conducted the coding, which was subsequently validated by a second author. The study’s findings were synthesized and presented as a narrative summary.
Results
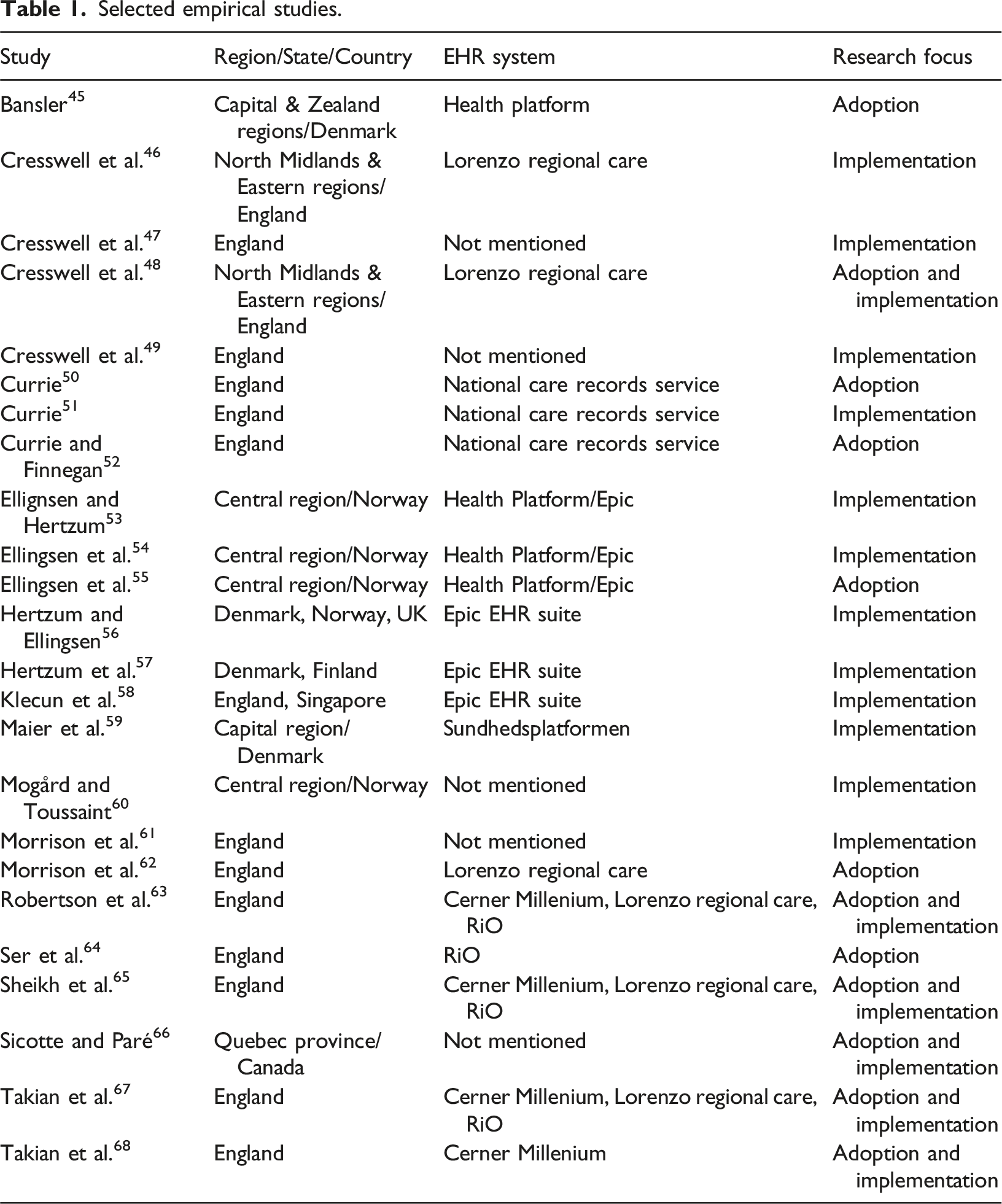
Selected empirical studies.
Results of quality assessment
The quality assessment of the 24 studies revealed a consistent level of congruity across most key domains. All studies demonstrated alignment between their philosophical perspectives, research objectives, and methodologies. Similarly, 22 of the studies showed consistency between their research methodology, data collection methods, and interpretation of results. However, two studies presented unclear findings regarding data representation and analysis, indicating a potential area for improvement. A notable gap identified was the limited acknowledgment of the researcher’s cultural or theoretical positioning. Only 11 out of the 24 studies included a statement on this aspect, indicating a significant gap in researcher positionality in the remaining 13 studies. Additionally, none of the studies sufficiently addressed the impact of the researcher on the research process or vice versa, highlighting a lack of reflexivity. In terms of participant representation, 19 out of 24 studies adequately incorporated the voices of participants, while the remaining five were found lacking in this area. Ethical considerations were also a concern, as 11 out of the 24 studies either did not clearly report ethical approval or provided unclear information regarding ethical considerations. Overall, while most studies exhibited strong congruity in research design, methodology, and interpretation, there were notable deficiencies in reflexivity, researcher positionality, participant representation, and ethical transparency. Full details of the quality assessment are provided in Additional File 1.
Salient characteristics of the selected studies and NEHR systems
Salient characteristics of the selected studies and NEHR systems studied.

To thoroughly describe, understand, and ultimately explain the complex phenomenon of NEHR system implementation and adoption, all studies employed a qualitative, case-based approach, which is well-suited for process-oriented research rather than variance-oriented research. Most of these studies grounded their observations in the sociotechnical perspective, which emphasizes the interdependent relationships between social and technical factors. 69
Additionally, these studies drew upon process-oriented theories, including stakeholder theories, actor-network theories, institutional theories, organizational change and learning theories, as well as crisis management and discourse-based theories. While seven studies were relatively ‘theory-light,’ meaning that theory did not play a significant role in the paper, their contributions lay in other areas, such as presenting new arguments, facts, patterns, or relationships. 70
The aims of these studies were analytical in 14 cases, exploratory in 7, and evaluative in 3. They addressed both the NEHR implementation and adoption processes (in 10 studies) or focussed on specific sociotechnical aspects of these processes (in 14 cases) such as the engagement and experiences of specific stakeholder/user groups, including physicians. Additionally, the studies examined the organizational, work-related, and care-related changes resulting from implementation, as well as the processes and consequences of adopting large-scale EHR suites.
Referring to Table 2, we further analyzed the scale and scope of the NEHR systems under study. In terms of scale, most studies examined national health IT policies or programs aimed at deploying NEHR systems across all acute-care hospitals, including emergency care facilities, within one or more regions as a precursor to nationwide implementation. Regarding functional scope, the NEHR systems were designed to support both clinical and patient care workflows, integrating various functionalities such as specialized clinical information systems (e.g., emergency, radiology, endoscopy, pathology), laboratory information systems, e-prescribing, and PACS. Additionally, three studies explored functionalities related to patient administration workflows, while one study focused specifically on the system’s role in prescription workflows and medication management.
In terms of institutional scope, all these NEHR systems were implemented in acute care hospitals, with one exception that was implemented in mental health hospitals. Additionally, 15 NEHR systems extended to specialized institutions, including pediatric hospitals (tertiary care). Furthermore, 11 systems included networking and data-sharing functionalities that linked hospitals to primary care institutions such as outpatient, ambulatory, or community clinics.
Critical aspects of NEHR implementation and adoption processes
Critical aspects of the implementation and adoption processes of NEHR systems.

Legend. N/A: not applicable.
Key stakeholders
The most critical stakeholders, who serve as the primary users of the NEHR system, are hospital clinicians, highlighted in 20 of the 24 studies. Other hospital staff and healthcare workers are mentioned in six studies. Central, regional, and local governments, in their roles as health IT funders, policymakers, and planners, are featured in 16 studies. Hospital managers, who bear responsibility for leading the NEHR system’s implementation and adoption, constitute the third key stakeholder group, appearing in 11 studies. Other notable stakeholders include EHR solution vendors (5 studies) and the implementation project team (5 studies). Interestingly, patients, as key stakeholders, are included in only one study. As a result, all studies focus on describing and understanding the complex, mutually influential interactions among these stakeholder groups throughout the implementation and adoption processes examined.
Implementation goal and strategy
Initially, eight studies describe national governments’ objectives of implementing a centrally designed, planned, and procured NEHR system using a ‘top-down’ implementation strategy, a common approach in the public healthcare sector. However, these same governments are also portrayed in eight studies as shifting toward a more balanced approach—combining central control and standardization with local autonomy and adaptation—thus transitioning to a ‘middle-out’ implementation strategy. Other studies focus on more specific goals and the execution of the implementation strategy, including preparations for the ‘go-live’ or pilot implementation of the EHR software solution (3 studies) and evaluations of early clinical experiences following implementation (3 studies).
Project management
All studies in our sample examine the project management challenges encountered during NEHR implementation and adoption. Initially, these challenges revolve around managing contextual, structural, professional, or technological misalignments (13 studies), particularly the integration of a large EHR software vendor within the project. Additionally, five studies address project leadership, governance, learning, and risk management, with a focus on assessing and mitigating risks related to project timelines, user expectations, and resistance. A third category of challenges—navigating political and public pressures—is highlighted in three studies.
Change management and acceptance
Half of the studies primarily frame change management and user acceptance as the management of stakeholder engagement, emphasizing clinicians’ involvement in implementation and adoption while addressing coercive, mimetic, and normative institutional forces (e.g., stakeholder power dynamics and relationships). Additionally, nine studies examine change management and acceptance through structural, managerial, and organizational learning mechanisms (e.g., boundary spanners) and institutional arrangements (e.g., incentives) designed to mitigate disruptions in clinical workflows (e.g., workarounds) and patient care (e.g., coping strategies) caused by the new system. A third perspective, presented in two studies, takes a technological view, focusing on the challenges of standardization versus adaptation and the choice between an EHR software suite and an ‘ecosystem.’
EHR software solution
The NEHR system is initially evaluated based on its technical characteristics, including configurability, customizability, interoperability, functionality, and usability (11 studies). It is also analyzed as an IT artefact whose ‘meaningful use’ by clinicians and other users is shaped by institutional forces (e.g., contractual arrangements with the EHR software vendor) and influenced by contextual factors such as the healthcare organization’s IT maturity, infrastructure, and continued reliance on legacy systems (8 studies). A third perspective examines the design approach of the EHR software, whether it was developed as a monolithic, closed system (single software provider, acquired off-the-shelf) or as a modular, open system (multiple providers, assembled from an EHR software ecosystem) (4 studies).
Benefits realization
While governments and healthcare policymakers prioritize the realization of benefits from the digital transformation of public healthcare systems, this appears to be less significant for key stakeholders involved in NEHR implementation and adoption, as described in the 24 studies. Nine studies report limited or absent early benefits for clinicians and hospital staff, including post-implementation productivity, quality of patient interactions, clinical multidisciplinary practices, information sharing, and learning. Additionally, five studies highlight concerns about the benefits realization process, focusing on issues of responsibility, accountability, and legitimacy from the perspective of various stakeholders.
Key prescriptions and lessons emerging from large-scale NEHR initiatives
The fourth research question explores the practical recommendations and insights that can be drawn from past NEHR initiatives. To address this, Additional File two summarizes the key insights and lessons learned from the 24 reviewed studies. The following paragraphs provide a synthesis of our findings.
Key success/failure factors
In all studies, the objective was not simply to identify the key factors in the NEHR deployment process but to understand why and how these factors significantly influenced the process outcomes. This approach moved beyond merely checklisting the presence or absence of factors that caused the implementation to succeed or fail. Instead, each key factor was identified in a context-sensitive manner, recognizing its evolution as part of a combination with other key factors throughout the implementation process. The following key influential factors were identified:
User participation
Notably, user participation, with a particular focus on clinicians, was the most frequently identified key factor (9 studies), often examined in conjunction with system user-friendliness, usability, and customizability (5 studies).
Stakeholder interaction
Strategic decisions
The choices and changes made by stakeholders concerning NEHR implementation (e.g., top-down vs middle-out), procurement (central vs local), and adoption strategies (standardization vs adaptation) were also found to exert strong influences on process outcomes (6 studies).
Implementation scale and maturity
The scale and scope of NEHR implementation and the maturity of EHR technology played influential roles in two studies, while one study emphasized the project team’s use of a sociotechnical approach and the mitigation of implementation risks.
Key barriers and facilitators
The approach used in the reviewed studies to identify key barriers and facilitators in NEHR implementation closely mirrors the method for determining success and failure factors. Notably, some barriers or facilitators may overlap with specific success or failure factors. Given the diversity and idiosyncrasies across the 24 case studies, barriers and facilitators are categorized at a higher level of abstraction than success and failure factors. They can be grouped as follows: • User participation • Stakeholder cooperation and conflict resolution • Institutional, organizational, and professional culture • Stakeholder resources and competencies
Deriving key lessons
All 24 studies in our sample derived key lessons from their case findings on the implementation and adoption of large-scale NEHR systems. These lessons were framed as critical insights, considerations, recommendations, or implications for various stakeholders, including governments, health IT policymakers, clinicians, hospital managers, project managers, consultants, EHR software vendors and integrators, and health IT researchers. Aligned with the key issues identified earlier, these lessons were categorized based on whether they addressed unresolved or resolved concerns related to unfavorable or favorable NEHR implementation and adoption outcomes. The lessons learned were classified as follows:
Engagement of clinicians and healthcare workers
These lessons address the challenge of securing clinician and healthcare worker participation. Key insights include identifying the right point of engagement, balancing encouragement with mandates, and, in the early stages, emphasizing benefits related to patient care quality rather than economy and efficiency (9 studies).
Navigating conflicting stakeholder and institutional forces
This issue involves managing competing interests and institutional logics. Considerations include establishing legitimacy across the medical profession, resolving conflicts between public and private sector logics, and facilitating translation between technical/managerial and clinical/practitioner discourses (9 studies).
EHR software procurement and design
These lessons focus on addressing NEHR design limitations and recognizing the significant impact of vendor-provided software on implementation steps and activities (6 studies).
Defining NEHR system functional scope and standardization
Considerations include limiting standardization to essential elements and prioritizing user and organizational needs over national requirements (3 studies).
Change and risk management
Recommendations highlight the need for flexibility in responding to policy shifts, viewing NEHR implementation as an ongoing process that adapts to evolving local, regional, and national needs, as well as political changes (3 studies).
EHR software maturity
This issue underscores that configuration and adaptation do not end at ‘go-live.’ A hybrid approach, combining standardized core solutions with customized modules tailored to specific users and workflows, is recommended (2 studies).
Discussion
Principal findings
This rapid review has helped unravel the complexities of NEHR initiatives, effectively unlocking their ‘black box’. By confirming that these projects are inherently wicked problems, our findings underscore how process outcomes — and ultimately project success or failure — are shaped by the intricate, interdependent and often conflicting interactions among stakeholders, and by the distribution of power and influence within the institutional landscape. As a result, the central component of NEHR initiatives, the EHR software solution, gains significance primarily from a stakeholder or institutional perspective, aligning with the sociotechnical view prevalent in most reviewed studies. For example, system interoperability is frequently framed not as a purely technical issue but as an institutional or organizational challenge. In summarizing these findings, we identify a set of partially unresolved issues and outstanding questions that warrant further investigation by action researchers, practitioners, and policymakers. These concerns are presented below as three nexuses and three conundrums.
Health IT policy-practice nexus
As several NEHR case studies highlight, the translation of national governments’ digital transformation goals, strategies, and policies into NEHR systems was met with diverse interpretations and varying levels of stakeholder acceptance or resistance. This, in turn, led to unforeseen shifts in national health IT policies, often driven by stakeholders themselves. These shifts were further complicated by political, institutional, and public pressures, creating significant challenges for NEHR implementation and adoption. Consequently, there is a pressing need for a deeper understanding of how national health IT policies can be effectively formulated, promoted, and translated into widely adopted NEHR systems.
NEHR implementation-adoption nexus
Initially conceptualized as distinct and sequential processes—implementation preceding ‘go-live’ and adoption following it—several studies reveal that these processes are intertwined and mutually influencing. As implementation extended beyond ‘go-live’ and adoption began even before it, attributing specific descriptive or prescriptive findings to either process became challenging. Instead, these findings suggest an integrated NEHR introduction process, where implementation and adoption evolve concurrently. This underscores the need for a deeper understanding and more refined modeling of health IT implementation, adoption, and assimilation within large-scale NEHR initiatives.
Secondary-primary care / acute-chronic care nexus
As noted earlier, public health systems in advanced countries face mounting challenges due to aging populations and the rising prevalence of chronic diseases, necessitating significant improvements in primary care delivery, particularly in chronic care management. This includes diagnosis, treatment, and follow-up by general practitioners (GPs) and nurse practitioners (NPs). However, the large-scale NEHR programs examined in this study primarily targeted secondary and tertiary care, focusing on acute and specialized services provided by hospital-based clinicians. While some studies included regional hospital systems that incorporated ambulatory or outpatient clinics, GPs and NPs were rarely considered key users of the NEHR system and were seldom regarded as primary stakeholders in its implementation and adoption. For the digital transformation of public health systems to be truly effective, action researchers, practitioners, and policymakers must prioritize the integration of primary care institutions and clinicians within NEHR and HIE strategies, policies, and practices. In some cases, primary care should be given greater emphasis to ensure a more comprehensive and inclusive approach.
Centralized-decentralized / coercive-normative / national-local conundrum
In most reviewed studies, the translation of national policies and programs for NEHR system implementation—which included centrally procured EHR software solutions—faced significant challenges at the local level. These difficulties stemmed from the autonomy and responsibility granted to public hospitals and healthcare institutions by national governments. They stemmed as well from the substantial influence of local stakeholders, particularly physicians, in contrast to national decision-makers. As a result, national policies often encountered strong resistance, requiring rapid adaptation toward greater decentralization and a more persuasive implementation approach. Finding the right balance between centrally and locally planned, procured, and implemented NEHR systems remains a major point of contention among national and local stakeholders. This conundrum highlights the need for context-sensitive, actionable insights from action researchers, practitioners, and policymakers to navigate these complex dynamics effectively.
Interoperability-customisability / standardization-adaptation conundrum
The tension between integration and flexibility in systems theory is evident in large-scale NEHR systems as a trade-off between interoperability and customizability of the EHR software solution. This reflects a fundamental conflict between national and local stakeholders: the former prioritizes interoperability, while the latter advocate for customizability. Achieving interoperability requires standardizing clinical workflows in public hospitals to align with the EHR software. In contrast, ensuring customizability demands adapting the EHR system to fit existing hospital workflows. As observed in the case studies, this trade-off is dynamic and follows a pattern of punctuated equilibrium, with national NEHR policies, programs, and implementation strategies frequently shifting. Striking the right balance between interoperability and customizability—and the corresponding standardization and adaptation of clinical workflows—remains a critical challenge. This conundrum warrants further exploration by action researchers, managers, and policymakers to develop sustainable, context-sensitive solutions.
EHR software suite-ecosystem conundrum
Several reviewed studies emphasize the significant role of the chosen EHR system and vendor in shaping NEHR implementation and adoption outcomes. Large-scale EHR suites from major vendors such as Epic and Cerner reinforce the importance of the IT artefact within the sociotechnical perspective of NEHR adoption, positioning these vendors as key institutional stakeholders. Aligned with the standardization–adaptation conundrum, the studies highlight challenges related to monolithic, single-provider, closed software procurement models (e.g., large-scale EHR suites) versus modular, multi-provider, open approaches (e.g., EHR software ecosystems). Further context-sensitive research is needed to assess the suitability of these approaches for large-scale NEHR implementation. Additionally, a deeper understanding of their relative advantages and disadvantages from stakeholder and institutional perspectives is essential for informed decision-making.
Implications for practice and research
The major implications of this rapid review for NEHR implementation practice are largely drawn from the key insights and lessons summarized in Additional File 2. It is crucial to recognize that these prescriptions and lessons are highly context-sensitive, meaning they cannot be applied in a straightforward checklist manner in future NEHR implementations. Indeed, key prescriptive concepts such as ‘user engagement’ and ‘top-management support’ were observed in these studies as evolving conditions rather than static factors. These elements are dynamic, subject to variation, and their impact on project success or failure differs across various contexts. For instance, the level of engagement among hospital physicians was found to fluctuate, often intertwined with other evolving conditions like the quality of user training.
Similarly, the key lessons from each study should not be blindly applied or treated as ‘one-size-fits-all’ solutions in future NEHR policymaking, programs, and implementations. Instead, they should serve as guiding principles for stakeholder actions, interactions, and preparations throughout the NEHR implementation and adoption processes. For instance, while opposing stakeholder visions and conflicting institutional logics consistently emerged as critical challenges, the mechanisms used to mitigate tensions—such as engaging boundary-spanning clinicians—were introduced at different stages and had varying effects on process outcomes. This dynamic nature underscores the need to contextualize these lessons, carefully considering specific circumstances when applying them to future initiatives.
The major implications of this review for future research focus on identifying the unresolved issues and unanswered questions highlighted in the reviewed studies. These issues, organized into three nexuses and three conundrums, underscore areas that require further exploration by scholars. Researchers should recognize that the concepts of scale and scope are critical for understanding the complexity of implementing a NEHR and guiding stakeholder interactions. These concepts also help reduce terminological ambiguity by providing a clear definition of what constitutes a NEHR system. Additionally, future studies would benefit from adopting stakeholder and institutional theories as overarching theoretical frameworks to better contextualize and refine IT implementation, adoption, and evaluation models derived from information systems research. This approach would facilitate the integration and synthesis of various models, such as digital transformation process models, IT maturity models, and information systems success models.
Study limitations and future research
While this study adhered to most PRISMA guidelines for systematic reviews—such as defining clear objectives, predefining eligibility criteria, assessing validity, and systematically synthesizing results—a key limitation of our rapid review approach is the higher risk of bias. Specifically, empirical study selection was conducted by a single reviewer, rather than following the commonly recommended double-screening procedure.
71
This approach was justified by the primary goal of rapid reviews: providing timely insights for practitioners and policymakers by streamlining certain elements of the systematic review process.
72
Future research could adopt a systematic rather than rapid review approach to expand on our findings and offer comprehensive, high-quality evidence synthesis on critical aspects of NEHR implementation. Key areas for deeper exploration include: • Managing scale and scope: Balancing national priorities with local needs in NEHR initiatives.
1
• Implementation strategy selection: Identifying the most effective approaches for guiding NEHR implementation.
73
• Project management: Addressing key challenges such as cost management, training requirements, and data security and privacy. • Emerging technologies: Exploring the role of AI, connected devices, and blockchain in the evolution of EHR software solutions.
Finally, while this study focused on large-scale EHR implementations in a developed country context, our findings may nonetheless have implications for developing countries. Generally characterized by an underdeveloped public health system and a poor HIE infrastructure, these countries face specific sociotechnical barriers and managerial challenges as they strive to implement EHR systems, be it at the local, regional or national level. 74 Hence, future research on such implementations could first ascertain the extent to which and the manner by which this study’s implications may be adapted and applied to a developing country context.
Conclusions
Given a country’s goal to enhance healthcare effectiveness and efficiency while improving population health through digital transformation, the findings of this rapid review underscore the complexity of implementing and adopting large-scale NEHR systems. This process unfolds over an extended period and involves multiple stakeholders with diverse interests. The reviewed studies employed theoretical frameworks and qualitative methods well-suited for analyzing such multifaceted processes. By conducting a context-sensitive analysis of key findings and recommendations, we have provided a practical overview of NEHR implementation and adoption. In doing so, we have identified critical challenges to be prioritized by researchers and addressed by practitioners in future initiatives. These insights serve as valuable guidance for those involved in shaping the future of NEHR systems, ultimately contributing to improved healthcare services and the well-being of individuals and communities.
Supplemental Material
Supplemental Material - Navigating large-scale EHR implementations in public health systems: Lessons learned and recommendations from a rapid review
Supplemental Material for Navigating large-scale EHR implementations in public health systems: Lessons learned and recommendations from a rapid review by Louis Raymond, Aude Motulsky, Gregory Vial, Mickaël Ringeval and Guy Paré
Footnotes
Author contributions
All authors contributed to the design of the study. The search and screening were performed by LR. Quality assessment was performed by GP and MR. Data analysis was performed by LR. All authors contributed to the writing of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Quebec Ministry of Health and Social Services (#11979).
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data are within the manuscript and its supplemental material files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.