
Abstract
Objective
The study aimed to identify and describe the engagement strategies used in implementing electronic health records in health care settings and to ascertain why they were successful or not, using normalization process theory.
Methods
In this rapid review, we searched PubMed and CINAHL for qualitative and mixed methods primary studies published from 2010 to 2023 (June). We identified 41 studies that explored the implementation of EHRs, involving clinicians as participants. For quality appraisal, we employed the standards for reporting qualitative research (SRQR) tool. For analysis, a qualitative comparative analysis, using the normalization process theory was conducted. This was followed by a narrative synthesis to compile and analyze key findings.
Results
About 56% (n = 23) of the studies were conducted in hospitals, while the remaining were done in mental health, maternity, and ambulatory care settings. Participants included a range of clinicians such as nurses, physicians, doctors, dentists, pediatricians and other specialists. Evidence shows that prior to implementation, effective communication of the vision of EHRs and early user involvement in decision-making are useful engagement strategies in preparing users for implementation. Tailored training and on-demand technical support for users sustain system usage during the roll out. Lastly, ongoing engagement with users is essential for continuous user support and system improvements.
Conclusion
User engagement improves the chances of successful implementation, particularly if engagement strategies are effective for the specific stages of implementation. The success of these strategies is more evident when they ensure normalization process theory tenets, which include user coherence, cognitive participation, collective action and reflective monitoring.
Keywords
Introduction
Electronic health records (EHRs) are a patient-centric information resource for clinicians and a longitudinal record of patient information and service provision for managers.1,2 They enable clinicians to perform their duties more efficiently by improving diagnostic precision, coordination and delivery of care and clinical decision making,2–4 thereby acting as a tool for recording, handling and sharing health data. The World Health Organization (WHO) urges governments to invest in digital health solutions like EHRs, especially for low and middle income countries working towards universal health coverage.5,6
Despite the potential for EHRs to improve the delivery of health care, implementing EHRs is often difficult and can result in negative and unanticipated disruptions to clinician workflow. 7 Organization leaders exert greater control over the implementation processes, while end users often have a more intimate understanding of the care delivery process. 8 Where leaders fail to meaningfully engage end users, it leads to implementation failures. 9 Health care settings are dynamic networks of interactions between people and processes. 10 Introducing a new sub-system such as an EHR in health care settings has implications for end users and their workflow patterns. 11 As a result, implementing EHRs requires a synergistic approach involving a top-down and bottom-up direction, with the latter gained through user engagement.
User engagement can include activities to consult, involve or partner with end users of EHRs throughout the implementation process, thereby presenting opportunities to identify and solve implementation challenges in real time.9,12,13 Activities could be involving users in decision making processes, partnering with them to co-create solutions, conducting focus groups or feedback sessions to understand user needs. Engagement ensures that implementation is a collaborative process, ensuring that end users’ needs and workflows are accommodated, to promote ownership and acceptance of the new system. 11
Evidence on the implementation of EHRs
Evidence on the implementation of e-health systems, including EHRs, has been synthesized in two notable reviews, both of which utilized theoretical frameworks: the Consolidation Framework for Implementation Research (CFIR) 7 and the normalization process theory (NPT). 14 The CFIR focuses on the contextual determinants of implementation outcomes while the NPT explains the behaviors and thoughts underlying technology adoption by users. 15 Although these two reviews are not specific to EHRs, they elaborate on the importance of user engagement and deploy useful theoretical frameworks.
The Ross review, using the CFIR shows the importance of stakeholder engagement during the development, planning and execution of implementation processes. 7 The Mair review, using the NPT concluded that user engagement is central to successful implementation of new technology, but there are limited efforts aimed at actively involving health professionals during implementation. 14 Although both reviews underscore the importance of user engagement, they do not explore engagement strategies and factors that promote or inhibit user engagement. While the CFIR carries a wider focus on broader factors of implementation, the NPT carries more depth in explaining the mechanisms of user engagement. 7
There are several reviews on EHR implementation which report on the factors affecting implementation such as the influence of organizational, human and technological factors.16–18 While these reviews emphasize implementation strategies including user involvement, they fall short of synthesizing the strategies necessary for effective user engagement. In this rapid review, we identify and describe the engagement strategies used in implementing electronic health records in health care settings, whether they were perceived as successful and, using NPT, to ascertain the reasons why they were successful or not.
Normalization process theory (NPT)
We use NPT for this review, a framework developed to fill the gap in addressing the work of individuals and groups during implementation.14,19 The NPT explores the factors influencing the routine embedding of complex interventions into everyday practice. 20 Thus, the theory holds practical value by offering a means to assess implementation from a user's perspective.21,22
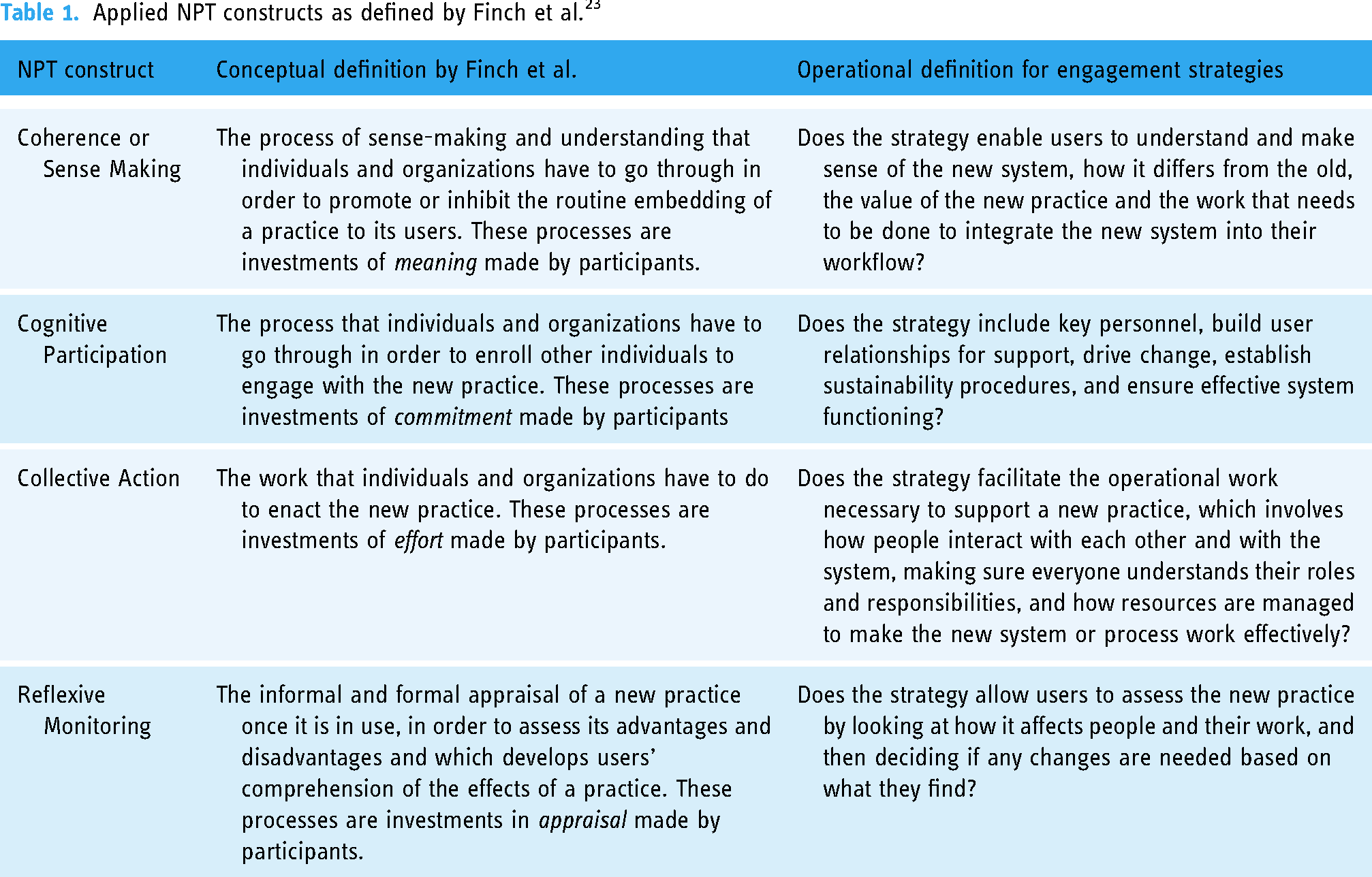
The theory incorporates four constructs, used in this review to evaluate engagement strategies: coherence (or sense-making), cognitive participation, collective action and reflexive monitoring.20,23 These constructs interact and influence one another. Table 1 below shows the definitions of the NPT's constructs and the operational definitions used for this review.
Applied NPT constructs as defined by Finch et al. 23
Methods
We conducted a qualitative evidence synthesis using a rapid review approach. Rapid reviews use an accelerated process compared to standard reviews, allowing researchers to draw insights from scientific evidence in a timely and resource efficient way. 24 This rapid review's protocol was registered on the PROSPERO database: CRD42021275000, and is reported following the enhancing transparency in reporting the synthesis of qualitative research (ENTREQ) statement. 25 No amendments were made to the information provided at registration or in the protocol.
Search strategy
The search strategy (see Appendix A) was adapted from the reviews conducted by Ross and Mair on the factors affecting the implementation of E-Health systems.7,14 For this review, the strategy was narrowed to search for studies on the implementation of EHRs only. Using the rapid review approach, we limited our search to only two electronic databases as more databases would increase the number of hits while diminishing the number of included papers. A systematic Boolean search method was employed on the 23rd of June 2023 using key operators (such as OR and AND) truncated to find relevant literature. The search utilized two categories of keywords (see Appendix A), using Medical Subject Headings (MeSH) terms related to “Electronic health records” and terms related to “Implementation.” The search was initially conducted in PubMed and then adapted for CINAHL, using different indexing methods to suit each database and maintain the consistency of results. Both searches were limited to January 1st, 2010. The search strategy was refined through team discussions and the final search syntax is provided in Appendix A.
Eligibility criteria
Inclusion criteria
Included studies were primary studies published between January 1, 2010 and June 23, 2023, of qualitative or mixed methods design, reporting on the implementation of EHRs in any health care setting, with end users of as study participants. Studies were included if they provided descriptions of engagement strategies used during implementation. Only studies in English were considered.
Exclusion criteria
Studies were excluded if their participants were only non-end users, or if they were reviews, meta-analyses, literature reviews or quantitative studies. By non-end users we mean individuals who do not directly use or interact with EHRs in their healthcare roles, which may include policy makers and managers. At final screening studies were excluded if they did not describe any engagement strategies used at any point during EHR implementation; there was no description of user involvement undertaken or attempted.
Study selection
All identified studies (n = 1034) were checked for duplicates using the Zotero software. The remaining studies (n = 963) were double screened by title and abstract using the Covidence software by three members of the review team (CZ, SA and SM), guided by the inclusion criteria. Full text screening was conducted by the lead reviewer (CZ), screening the first 20 studies, while FG and JG independently screened the same batches to ensure consistency of screening decisions. Beyond this point, CZ conducted full text screening of the remaining studies and discussed the screening decisions with the senior co-authors (FG and JG) to ensure consistency and accuracy of this process. This led to the final sample of included papers (n = 41).
Quality assessment
The standards for reporting qualitative research (SRQR) was used as a quality appraisal tool, the lead reviewer (CZ) assessed the quality of the articles with the input of senior co-authors (FG and JG). The SRQR consists of 21 items which provide SRQR. 26 To adapt the SRQR for quality appraisal, we assigned a scoring system for each of the 21 items, scoring points for fully addressed items (1 point), partly addressed (0.5 point) and not addressed (0 point) (see Appendix B). For mixed methods studies, we focused exclusively on the qualitative parts of the findings and applied the SRQR accordingly. We used the total score as an indicator of the quality of the paper. Thus, from a possible maximum score of 21 (see Table 2), studies that had a score lower than 15 out of 21 were regarded as low quality. They were retained if they met the inclusion criteria but we were cautious in use of evidence from lower quality papers. As this is a novel use of the SRQR, we additionally assessed the quality of papers using CASP checklist (see Appendix C). The CASP ratings provided similar quality ratings but with a narrower range of scores, limiting differentiation between studies.
Description of studies.

Data extraction
The lead author (CZ) extracted data from eligible studies (n = 41) into an Excel spreadsheet and word document. The details from each study were recorded and these include the names of authors, year of publication, participants, design, study setting/context, intervention characteristics, description of engagement strategies used and user perceptions on engagement strategies (see Tables 2 and 4). After this stage, JG and FG met with CZ to review the consistency of the extraction. All included studies featured engagement strategies, but only those providing detailed insights were incorporated into Table 4. These offer rich information on strategy implementation and user perceptions. Studies with less depth are only included in the results section text (See next section for how this was managed during analysis).
Data analysis
The results of all studies were inductively coded using descriptive themes in NVivo. Themes were grouped by type of engagement strategy (see Table 3). The coded data from richer studies was interrogated to create Table 4 which reports on the context of implementation (setting and scale of implementation), engagement strategies that were used at each stage of implementation (before, during and after implementation) and the success or failure of the strategies as reported in the paper. Papers reported success/failure as perceived by their research participants. We used the NPT constructs (coherence, cognitive participation, collective action and reflexive monitoring) to identify the reasons for the success or failure of each engagement strategy.
Description of engagement strategies.

Evidence synthesis of results from 16 studies.

Through a qualitative comparative analysis (QCA) process, we compared the studies to identify what combination of context and engagement strategies resulted in successful engagement (see Table 4). The QCA is a method for identifying the configurations of conditions that lead to specific outcomes. 27 A narrative synthesis was then written, drawing in data from the papers beyond Table 4 to provide diverse examples and avoid overlooking disconfirming results.
Findings
Description and overview of studies
The search yielded 1034 results, reducing to 963 after removing duplicates. From these, 108 were remaining after title and abstract screening, reducing to 41 after full text screening (see Figure 1), with 36 qualitative and 5 are mixed methods studies. Quality assessment resulted in 21 high-quality (18–21/21) studies, 17 average-quality (16–17.5/21) studies, and 3 below-average studies (<16/21). We included all studies but found higher quality papers had richer and more useful data for our review.

PRISMA flow diagram.
Of the 41 studies, 38 were from high-income countries, 2 from middle income and 1 from a low-income country (see Table 2). Additionally, 13 studies were conducted in single units/facilities, 18 were multi-site or regional implementations, 7 were national implementations, and 3 were multi-national implementations. 23 studies were conducted in hospital settings, while the remaining 18 were spread across mental health, maternity, long-term care, nursing homes, ambulatory, teaching clinics and HIV care facilities. Among the 41 studies, 22 primarily involved nurses as participant users, while the other 19 had participants from various professions, including physicians, doctors, dentists, pediatricians, pharmacists, administrators, data capturers, and mental health practitioners. Of the 41 studies, 22 involved non-user participants: managers, software developers, engineers, heads of departments, case managers, quality improvement specialists, policy makers, researchers, software vendors, business and process analysts, safety officers, information officers and process architects.
Table 3 gives a list of the all the identified engagement strategies, descriptions of each strategy, and references to studies reporting these strategies.
Before implementation
Engagement strategies used at this stage aimed to prepare facilities and end users for implementation beforehand.
Communication of policy and vision
Policies at national level were perceived as an effective way of communicating intention across multiple facilities and to foster buy in and collective action for stakeholders at various levels as one study reports: “You need upper-management buy-in and buy-in from all department heads, including HIM director or materials management, not just top administration. Clinical and operational leadership must be engaged fully in the process.” 28 In most cases of national and multi-site implementation, policies and visions were generated at national level but facility leaders proactively made policy changes and provided support to users.29–31 Several studies show facility leaders playing this role in preparing and engaging users at this stage.30–34 Local facility managers should be able to engage end users according to their own managerial insights and organizational needs to ensure that users can make sense of the new system. Communicating the vision requires leaders to manage expectations for users as one study highlights: “This is an organizational change project not an IT implementation project, and it will rise and fall on how much the leaders—all the leaders not just the CEO—understand and set and guide expectations.” 28
However, in some cases policy and vision were communicated from the top but lacked engagement with local leaders leading to poor communication with end-users.32,34–39 For instance, where implementation was led by national structures without engaging users and leaders from local organizations, the vision was perceived as poorly communicated. 34 In such cases, communication was in the form of a directive, which limited facility managers’ autonomy to tailor implementation for their organizations. One study shows how this led to poor coherence and cognitive participation, as users perceived the EHRs as imposed: “It's getting the users to understand and the hospital to understand that the system is theirs and they own it…The danger is they feel it's thrust on them and they have to use it.” 32 Thus, local management struggled to communicate the policy and vision when national bodies used a top-down engagement approach. In another study, national bodies later tried to address this issue after users showed resistance: “I think it's about what are we communicating, how we communicate that, what are we saying our expectations are to staff about what are the benefits of this system to patients and to staff.” 34 This was done through communication strategies, emphasizing anticipated benefits, training, appointing clinical leads, and seeking user input in system design.
Preparation for implementation
Engaging end users prior to implementation was deemed important, with local leaders playing a crucial role in translating the implementation vision into practical tasks.30,40 This enables sense-making, helping users understand the coming changes and their roles in it. One study reports how multiple sites minimized workflow disruption by conducting a “readiness to change” assessment at facility and individual levels. 29 This involved assessing issues such as current user IT usage in facilities and computer literacy to inform implementation plans. One study reports how preparation for implementation should involve collective action: “Assembling the right team—usually the practice manager, a clinician, and staff members—to plan and implement this work was essential. We have put a team together that involves every area of the practice.” 41
As shown in Table 4, early preparation involves leaders proactively engaging users early, and involving them in vendor selection, planning and decision making stages.29,30,34,42–44 This secures cognitive participation, fostering collective work towards a goal as one study reports: “Across sites, informants emphasized the importance of early physician buy-in, with several sites noting that, ideally, the physicians themselves should drive the EHR adoption decision as opposed to the health system. Early and strong physician buy-in was deemed critical in order to ensure successful implementation and minimize resistance.” 29 Another study showed how early user involvement generates buy-in: “participatory process in selecting the EMR system represents a distinctive way to generate and improve commitment to the project within the organization. Conversely, if this process is imposed, it can generate user frustration and have a negative impact on the implementation process and on the overall use of the system.” 43 Several studies showed that the overall benefit of early user participation is that users can select a system that meets their needs.29,30,38,45 One study suggests that learning from facilities with similar systems can further inform user choices: “Take a group of staff to visit another hospital that has the system you’re considering; observe how the system works, and ask to hear their stories about system build and use.” 28
In cases of poor preparation, poor user cognitive participation was also noted. For instance, when national bodies imposed EHRs on users, local management struggled to prepare their facilities because they perceived it as an attempt to promote software that was not chosen by intended users. 34 Such engagement allows early feedback from users, through reflexive monitoring. In one study, users tested the system but their feedback was largely ignored leading to a rollout of a system that malfunctioned. 45 Similarly, in one facility, extensive user preparation included awareness road shows, on-site demos, training and e-learning before going live, but the system malfunctioned poorly as users could not communicate with developers for intelligent problem-solving. 46
During implementation
Engagement strategies used at this stage were aimed at supporting end users and managing challenges during the implementation process.
Training and education
Training and education were frequently reported in the findings. Studies shared user insights on training methods, timing, frequency, content and the delivery of training.37,47–49 Training that was reportedly successful was delivered a few weeks before going live, 29 with one study cautioning against delaying EHR rollout after training as it may lead to users forgetting what they learnt. 32 Training that came too early or too late after the rollout was reportedly unsuccessful.36,50 While timing was important for initial training, users felt that refresher training was particularly helpful following system upgrades.42,51,52
Studies report various training methods: formal course training, simulations and practice, providing user manuals and leveraging highly trained users to train colleagues.40,46,53,54 Hands on and simulation training were favored by users because they allowed users direct interaction with systems.29,54,55 Users describe its usefulness in real-work situations: “[The training should be] more applied by focusing on a patient scenario, to facilitate learning how to use the system safely and efficiently during a patient visit.” 56 In cases where users had varying levels of computer literacy, training started with basic computer education.54,57 In a nursing home study, users found it beneficial to supplement theoretical training sessions with manuals as they provided a convenient and quick reference: “it is reassuring to know that you can always fall back on it [manual] when you have doubts about putting things in the right screen,” while another stated: “a manual is necessary, especially in the weekends, when it is hard to contact someone.” 58 In other cases, training was supplemented by emails on lessons learnt and guidance for complex tasks.36,59
Some users, did not favor formal training, and found it too generic to just sit and receive information on how to use the system from a trainer.54,60,61 In Table 4, formal training was successful when supplemented with peer support and learning.43,47,48,57 Users also preferred hands on training and learning from peers more: “[Training with technical support] was pretty useful [but] experimentation is number one and then being taught by colleagues.” 62 In such cases, proficient users who were peers and colleagues facilitated training tailored for their context for non-proficient users. 29 This eliminated the need for users to leave their wards for more training or support. 43 In one study, physician champions through reflexive monitoring noted that the training was too generic and developed a tailored simulated training environment for users before going live, which was well received. 47 However, in two studies, training was only offered to advanced users, neglecting the broader user base and leading to poor training outcomes among users.46,63
Users preferred tailored training because it catered to their unique roles and workflows. 33 Conversely, where training was not tailored, users found it irrelevant: ‘‘If you were an admin person, you’ve got a certain type of training…And so, you had people sitting in training session where maybe 50% of what was being trained was not really applicable to their job.” 32 Thus, failed training efforts were typically attributed to generic and untailored training approaches,32,63 which discouraged cognitive participation. Other challenges in training included inconsistent and insufficient training, 44 as one study reports: “Participants found EHR training to be superficial and of insufficient duration. Some obtained training for a few hours before using EHR for clinical activities. Some were trained as they performed clinical activities, and others got trained over the phone.” 49 Users noted that training was poor when delivered by individuals unfamiliar with the workflow or the specific work of users as they perceived that such trainers could not effectively bring coherence and cognitive participation among users. 30 Users felt that training was also unsuccessful when imposed on them. In some facilities, users were reluctant to take time to learn until necessary, as some managers mandated training, requiring users to demonstrate competency before EHR use.29,30,46 However, this approach was perceived to be too intrusive and less effective in aiding users to make sense of EHRs.
On-demand technical support
Users appreciated real time, hands on, in person and on demand support during actual care situations. 30 Some multi-site studies highlighted the effectiveness of real-time support,51,54,64 with one study emphasized the value of on-site developer assistance due to the convenience of developers’ prompt availability. 51 In this case, the on-site developer was available for user support throughout their work shifts. 51 Another study achieved this by establishing direct contact with off-site developers who could remotely assist users: “staff could write notes and feedback any problems directly to the developer, who also had remote access and could look into any issues quickly.” 54 However, slow responses could led to frustration, especially during urgent situations as reported in one large organization: “Essentially, anyone can submit a ticket but as far as the response, I guess there are thousands of tickets so the ability of the organization to respond personally, you always get an automated response.” 64 As a workaround, some users submitted their requests to their immediate supervisors, who escalated it up the “chain of command.” One nursing home required nurses to sequentially contact the administrator, head nurse, and IT manager to address problems 58 and issues were resolved on the same day.
On-demand support was also provided by super users, physician champions, and nurse informaticians.36,39,64,65 Physician champions were perceived to be effective in providing localized support during critical periods, a month or two after the system's implementation. Similarly, another study made use of nurse coordinators for this task: “Our nurse coordinators who served as super users…really knew the system and were adept at helping their colleagues and physicians.” 47 In this study, external people were also hired to provide extra support on a part time basis. 47 Where nurse informaticians (NIs) were used, they initially facilitated implementation and continued to provide user support after, with some NIs directly embedded with the IT team, and others in the nursing department. 64 Although NIs were understaffed, users found them useful in promoting system use. In other cases, similar roles were fulfilled without specific titles, where a team of proficient clinicians acted as knowledge resources and were strategically positioned in wards.34,39,43
On-demand technical support was perceived as more effective when provided by peers as they leveraged existing relationships and were often influential enough to garner the trust of other users. However, when these roles were imposed or incompatible with user workflow, there was limited success. 34 Several studies underscore the importance of providing well trained support personnel.29,53,66 In one case, IT support personnel were slow in responding to problems causing delays and user frustration: “IT personnel need to quickly assist us in resolving problems… If the problem remains the same, how can you expect us not to have negative emotions toward this system?.” 67 Poor support led to users disengaging: “In fact, we are not uncooperative with the hospital's policy to use technology. We only hope for more support during the adaptation period. Our workloads remain the same, and adapting to the new system is an additional task, which is exhausting.” 67
After implementation
Strategies implemented at this stage were aimed at sustaining user involvement by addressing ongoing needs and improving the system.
Ongoing user engagement
Ongoing engagement ensures continued use and improvement of EHRs through reflexive monitoring, especially when introducing system upgrades, changes and adding new features as users need to be informed about these changes.
Users perceived that channels for continuous user feedback are useful for making informed improvements, with effective channels involving bi-directional feedback. 28 In one study, sites used different engagement approaches for bi-directional feedback, with some through staff meetings, emails, an open-door policy, and by allowing direct communication with the Director of Nursing (DON). 30 Users from this study found this to be an effective way of engaging as leaders would relay back the outcomes of their input back to them. Another study showed that effective ongoing engagement was through regular meetings of physicians from various specialties in EHR-focused committees. 57 This approach, through the collective action of various users, ensured the input of diverse perspectives for planned upgrades and changes.
Facility leaders played an important role in establishing communication channels, and users reported favorably towards positive communication: “Leadership communication strategies about implementation were mostly positive and supportive to the user…All groups reported a range of communication strategies, including education manuals, direct communication, e-mails, cheat sheets, and auditing.” 30 In another study, nurses who were intermediaries during implementation also facilitated this communication: “We have frequent updates [EHR system], guided by nurses who have become part of the program. Our system therefore has become close to exactly what we need…I contact one of those nurses who usually make [sic] it happen.” 50
Although updates were appreciated, users preferred receiving periodic updates, communicated through regular staff meetings with developers: “What I think would be really helpful is sort of periodic updates in various forms. If there's going to be a massive change or update…if they could come to our division meeting, department meetings, probably division meeting, or even our clinics.” 57 Some users preferred less frequent email updates and admitted to ignoring non-urgent emails due to email fatigue: “I hate to say it that way, because we get, there's email fatigue, too…A lot of times I don’t even open’em. I delete a lot of stuff. You just gotta’ focus on stuff that seems relevant for the moment to get you through the day.” 57
However, users in large organizations faced challenges with complex organizational layers to provide feedback: “Now that we are part of a larger system, making those changes, just go into layers and layers of people to get those changes.” 64 Thus, ongoing engagement can be complicated by organizational size and can lead to user frustration. 68
Use of engagement strategies
Table 4 shows that successful implementation requires the use of multiple strategies concurrently. A contrast can be made between the Cucciniello 43 study, which used 4 strategies and can be seen as more successful, against the Bristol 50 study, which used 2 strategies with less success. In the Cucciniello study, 43 implementation was more successful because users were involved and prepared early, offered training and support through peers, and a phased implementation approach was used to allow for real time adjustments during rollout. This ensured user coherence and cognitive participation through early involvement, followed by collective action and reflexive monitoring through peer led training and support. In contrast, the Bristol study 50 reports only training and ongoing engagement after rollout, leading to a poor implementation due to poor coherence and late training, rendering it ineffective.
Users perceived that another important success factor for engagement strategies is the capacity for reflexive monitoring. Studies that were reportedly successful were able to revise, and adapt where necessary due to feedback from user groups such as super users and champions,43,47 representative groups, 57 online platforms 64 and direct engagement with users. 30 The constant monitoring and dynamic responsiveness led to a more successful use of engagement strategies and a more resilient implementation.
Discussion
Our findings show that effective communication of policy and vision is crucial for user buy-in as a top-down approach without user participation may result in poor outcomes. Preparation for implementation and early user involvement in decision-making processes are effective engagement strategies prior to implementation. This involves assembling a diverse and representative team to facilitate implementation. Tailored training, especially through simulated practices, accommodates diverse user roles, workflows, and user literacy. However, critical factors for training effectiveness include timing, content and methods used. During rollout, on-demand support from technical personnel and proficient peers is crucial engagement to promoting EHR adoption. After implementation, ongoing engagement sustains a successful EHR adoption and optimization process through user feedback and active participation.
Similar to our findings, reviews emphasize the importance of user involvement for user readiness and better adoption. 69 Reviews report on the effectiveness of individual or clusters of engagement strategy reported in our study. Policies are crucial in fostering user readiness. One review shows that in developed and developing countries, policies were key determinants of readiness for EHR implementation. 70 Involving users early in the co-design of EHR systems has proven effective in improving implementation by ensuring the system caters for user needs, minimizing workflow disruption. 71 Another review demonstrated how tailored training, before, during and after EHR implementation is effective, especially when it includes super users, peer to peer and a mix of different training methods. 72 Successful adoption of digital technologies in clinical settings often hinges on organizational support, including that of personnel such as physician champions. 73 Ongoing formal programs of peer support groups, and online tools was reported to be an effective way of continuing to engage users. 74
WHO resolutions on digital health implementation encourage governments to develop strategies that guide implementation. 6 While global EHR adoption is rising, 75 many studies in this review focus on high-income countries (see Table 2). Several middle-income countries such as China, Brazil, India, and Mexico have initiated their EHR adoption, but most of them are still in early stages primarily due to financial and technological challenges.5,76 This review draws insights from counties that have implemented EHRs to aid those in early stages. Low- and middle-income countries face challenges when implementing an EHR challenges including financial constraints. 77 This review synthesizes learning that can contribute to implementation success and the avoidance of costly failures of implementation such as that in England in the 2000s. 78
Successful implementation is important because of the stress caused to health-workers during implementation due to heightened uncertainty. 79 Effective engagement strategies can reduce this stress. 80 Evidence suggests that user stress can be reduced through tailoring EHRs to clinicians’ needs, conducting usability testing and providing ongoing support. 81 High levels of EHR related stress have been linked to an increased intent among clinicians to leave their clinical practice. 82 Low- and middle-income countries already face challenges in retaining their clinical workforce. 83 User engagement during implementation of an EHR can help retain the clinical workforce. Engagement strategies remain necessary even after implementation to keep clinicians motivated and promote mature use of EHRs. 84
Implications for policy and practice
This study underscores the importance of user engagement in implementing EHRs and identifies the effective strategies along with the underlying reasons for their success. Inclusion of user engagement within policy can enable implementers to give priority to user engagement during implementation. This evidence review can inform implementers’ decisions on how to engage users, when and why. This is particularly important for low- and middle-income countries now considering the roll out of EHRs to support universal health coverage, where costly failure needs to be avoided.
Recommendations
The table below outlines recommendations drawn from the study findings on effective engagement strategies for EHR implementation, offering guidance on when and how to apply engagement strategies (Table 5).
Recommendations

Strengths and limitations
A notable strength of the study is that it builds on two existing reviews by Mair and Ross,7,14 which enhances their relevance and amplifies some of the findings from earlier reviews. However, the rapid review's limited search on PubMed and CINAHL only may have constrained our findings, potentially missing other information that may be captured by a more extensive search. The lead author (CZ), carried out the data extraction alone, however, the lack of cross checking at this stage was mitigated by supervisors, who checked for accuracy and consistency in the process and methodology.
Conclusion
In conclusion, this study highlights the importance of user engagement for a successful EHR implementation. These strategies include a communication of policy and vision, preparation for implementation, training and education, on-demand technical support and ongoing user engagement. The strategies are effective at different stages of implementation and need to be aligned with user coherence, cognitive participation, collective action and reflexive monitoring.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241291286 - Supplemental material for What engagement strategies are useful in facilitating the implementation of electronic health records in health care settings? A rapid review of qualitative evidence synthesis using the normalization process theory
Supplemental material, sj-docx-1-dhj-10.1177_20552076241291286 for What engagement strategies are useful in facilitating the implementation of electronic health records in health care settings? A rapid review of qualitative evidence synthesis using the normalization process theory by Campion Zharima, Samantha Mhlanga, Saira Abdulla, Jane Goudge and Frances Griffiths in DIGITAL HEALTH
Supplemental Material
sj-xlsx-2-dhj-10.1177_20552076241291286 - Supplemental material for What engagement strategies are useful in facilitating the implementation of electronic health records in health care settings? A rapid review of qualitative evidence synthesis using the normalization process theory
Supplemental material, sj-xlsx-2-dhj-10.1177_20552076241291286 for What engagement strategies are useful in facilitating the implementation of electronic health records in health care settings? A rapid review of qualitative evidence synthesis using the normalization process theory by Campion Zharima, Samantha Mhlanga, Saira Abdulla, Jane Goudge and Frances Griffiths in DIGITAL HEALTH
Supplemental Material
sj-xlsx-3-dhj-10.1177_20552076241291286 - Supplemental material for What engagement strategies are useful in facilitating the implementation of electronic health records in health care settings? A rapid review of qualitative evidence synthesis using the normalization process theory
Supplemental material, sj-xlsx-3-dhj-10.1177_20552076241291286 for What engagement strategies are useful in facilitating the implementation of electronic health records in health care settings? A rapid review of qualitative evidence synthesis using the normalization process theory by Campion Zharima, Samantha Mhlanga, Saira Abdulla, Jane Goudge and Frances Griffiths in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076241291286 - Supplemental material for What engagement strategies are useful in facilitating the implementation of electronic health records in health care settings? A rapid review of qualitative evidence synthesis using the normalization process theory
Supplemental material, sj-docx-4-dhj-10.1177_20552076241291286 for What engagement strategies are useful in facilitating the implementation of electronic health records in health care settings? A rapid review of qualitative evidence synthesis using the normalization process theory by Campion Zharima, Samantha Mhlanga, Saira Abdulla, Jane Goudge and Frances Griffiths in DIGITAL HEALTH
Footnotes
Contributorship
CZ led the search, screening, data extraction, quality appraisal, analysis, and drafting of the review manuscript. SM and SA were involved in title and abstract screening, reading, and refining the screening tool. JG and FG contributed to the design of the research protocol design, provided supervision, and guidance throughout the review process. All authors read, reviewed, and approved the final version of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is part of a PhD study funded by the South African National Research Foundation (NRF) through the SARChI programme for health systems and policy research at the Centre for Health Policy, School of Public Health, University of the Witwatersrand. Scholarship number: PMDS2205046516. The funders were not involved in writing this review.
Guarantor
CZ.
Informed consent
As a review, patient consent for this study was not required as no patients were included in this study. Our review conducts a secondary analysis of already existing and published studies.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.