
Abstract
Background
Implementation challenges of digital health solutions (DHSs) comprise complexities of behavioural change, resource limitation, inertia in existing systems, and failure to include consumer preferences. Understanding the factors which contribute to successful implementation of DHS is essential. We report the development of an implementation strategy for Brain Tumours Online (BT Online), a digital supportive care platform for patients with brain tumours, their carers and healthcare professionals.
Aim
To develop an evidence-informed implementation strategy for BT Online, considering the specific barriers and facilitators to implementing DHS for adults with a brain tumour and their carers and healthcare professionals.
Methods
A rapid review methodology was used to summarise factors relevant to implementation of DHS for people affected by cancer. Themes from the review were supported by implementation guidelines for DHS and the combined evidence informed the implementation strategy. Each theme was matched with specific steps for implementing BT Online.
Results
The rapid review identified 10 themes, namely, awareness of the new digital platform; institutional integration and support; data security, the quality, usability and accessibility of the platform; belief in the benefit of the platform; the need for holistic and tailored features; the timing of introducing the platform; engagement of healthcare professionals; and the re-definition of roles and workload. The themes were matched with 51 concrete implementation steps.
Discussion
The purpose of the strategy was to minimise risk of implementation failure, consider the specific context of care and generate a reference framework to evaluate BT Online prior to upscaling to use outside the research context. Our method contributes a novel approach of developing an evidence-informed rigorous implementation strategy if existing implementation frameworks do not apply.
Why was the study done? We explored the best way to introduce a digital supportive care platform to patients with a brain tumour, their carers and healthcare professionals. To reach and engage all users, barriers and enablers specific to their needs must be considered when implementing such a platform into existing care pathways.
Why is the study important? In Australia, there is no digital platform that provides people affected by a brain tumour with information, self-help tools and connection with peers in one place. Our team of patients, carers, healthcare professionals, digital health researchers and digital software developers has built a digital platform that meets all these needs. It is called BT Online (https://braintumoursonline.org/). This study presents the implementation plan of BT Online.
What did the researchers do? To identify potential barriers and enablers to implement the platform we searched the research literature and published guidelines on the implementation of digital health solutions. From these resources we developed a structured implementation plan.
What did we find? The implementation plan consisted of 10 themes that guided the implementation steps when introducing BT Online to its users. For example, the timing of introducing the platform to its users is important and user data needs to be safe. Furthermore, healthcare professionals are important to engage patients and carers in platform participation. In total, we followed 51 implementation steps. Having a well-constructed implementation plan increases the chance that BT Online will be successful for patients with a brain tumour, their carers and healthcare professionals.
Keywords
Introduction
Improving the quality of life of adults with a brain tumour, and their carers, is an area of unmet need. In high-income countries, one in four brain tumour patients will live more than five years, varying with tumour type, and ranging from 88% for meningioma and 7% for glioblastoma.1,2 Irrespective of diagnosis, life with a brain tumour (including those under observation only) and after primary tumour treatment presents physical, psychological, cognitive, emotional, and social impairments3–5 and many patients need survivorship care that supports their daily activities, emotional wellbeing and social participation.6,7
Self-management interventions provide health information, enable self-management of symptoms, and address psychosocial needs and lifestyle changes inherent to living with an illness. 7 For people living with cancer, these may include initiatives to improve diet, exercise and sleep, or strategies to deal with emotions, financial difficulties, or end-of-life preparations.8–10
Self-management interventions may be delivered face-to-face, via telehealth or using digital tools. Digital health solutions (DHSs) include information provision in electronic format and electronic devices (such as websites or applications) or monitoring systems (such as wearables) to improve health. 11 DHS are attractive as they may be self-directed or practitioner-assisted and offer an accessible option to support daily needs; overcoming the geographic, physical, and social care barriers inherent in face-to-face interventions.11,12
While several systematic reviews have highlighted the potential of DHS for cancer patients, they also identified a paucity of validated DHS, particularly for those with brain tumours13–15 and for carers.15,16 There is no digital platform available to Australians with a brain tumour and their carers that provides education, validated self-management interventions or peer support.
To address these gaps, our team of patients, carers and healthcare professionals (HCPs), digital health researchers and digital product developers have co-designed Brain Tumours Online (BT Online), a digital platform to support patients with a brain tumour, their carers and HCP (https://braintumoursonline.org/). The platform comprises three pillars: (1) ‘Learn’ – a curated database of information (2) ‘Connect’ – an online peer support community, through which users can connect, share stories and access online webinars and (3) ‘Toolbox’ – a directory of evidence-based, self-management interventions. The co-design of the platform prototype comprised interviews and workshops with patients, carers and HCP, as well as regular key investigator and design reference group meetings. Once completed, the platform prototype underwent usability testing in one-on-one sessions between users and the digital development team (Figure 1). The co-design process occurred parallel to the development of an implementation strategy for the second phase of this project, during which the platform will be tested with patients, carers and HCP. Note, we use the term ‘patients’ for ease of reading but acknowledge that this term does not adequately describe those who live with a brain tumour diagnosis outside of the clinical context. There was no consensus amongst our consumers – we considered patients, survivors (particularly disliked) and people living with a brain tumour, but ‘patients’ seemed acceptable to all.
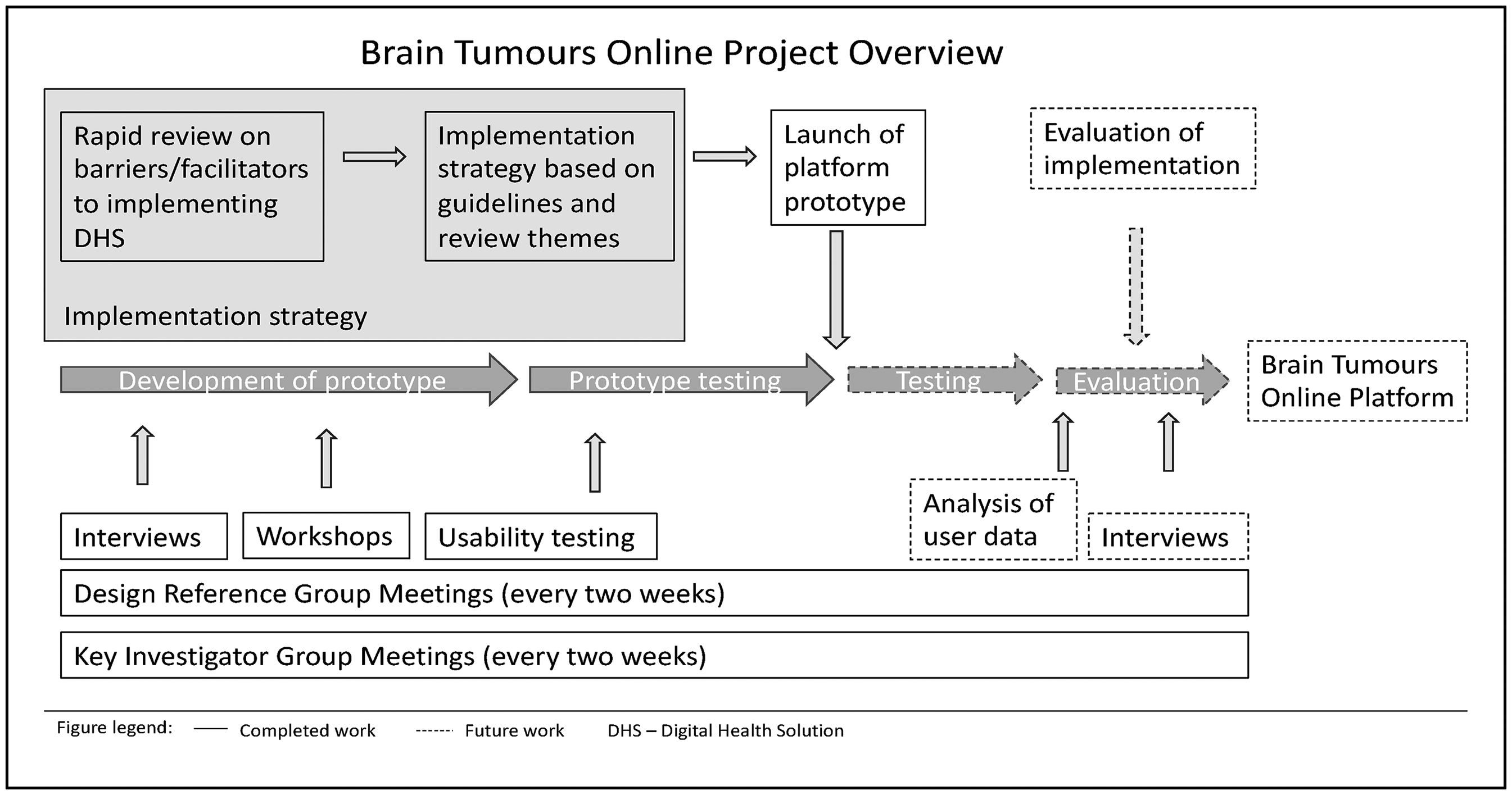
Project overview.
Challenges to successful implementation of DHS include the complexities of changing human behaviour, financial or other resource limitations, disruption of existing systems, and failure to include consumer preferences.17–21 Application of a rigorous implementation strategy has been shown to minimise implementation and user-acceptance failure when introducing new health interventions to existing health services.22,23
Considerations for the implementation strategy
After considering well-established implementation frameworks24–29 in preparation for the implementation plan for BT Online, we decided to develop a bespoke strategy specific to the needs of our study for two reasons. Firstly, few implementation strategies have been reported for brain tumour populations, with unique challenges of poor prognosis, multiple symptoms, physical and cognitive impairments, and complex psychosocial challenges due to social function changes.5,7 Secondly, many implementation strategies assume the new intervention will be disruptive to existing (healthcare) systems. 30 However, BT Online was developed to be additive to existing services. Little is known of the applicability of existing implementation frameworks to DHS that are introduced to contexts that sit ‘outside’ hospital-based models of care.
Thus, we aimed to develop an evidence-informed implementation strategy for BT Online, using a rapid review of literature considering the specific barriers and facilitators to implementing DHS for brain tumour patients, their carers and HCP. We present a novel approach to develop a bespoke implementation strategy when existing implementation frameworks do not match the purpose.
Methods
In preparation for this study, published guidelines and checklists specific to the implementation of DHS were identified by searching the PubMed version of the Medline database in October 2022. However, none of these guidelines were specific to people with brain tumours. Therefore, a rapid review was conducted to summarise barriers and facilitators to implementing DHS specific to a brain tumour population.
Rapid review methodology
A rapid review is a form of knowledge synthesis that accelerates a traditional systematic review by streamlining or omitting specific methods to produce evidence for stakeholders in a resource-efficient manner. 31 Findings from such reviews can inform the development of evidence-based implementation strategies to improve the success of any new DHS.32,33 An a priori understanding of the factors that can impact implementation of DHS was important for our project. 30
We adopted a rapid review thematic synthesis approach to enable a transparent yet expedient process compatible with our project timeline (Thomas & Harden, 2008). For reporting we used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (where applicable) 34 and the PRISMA extension for rapid reviews. 35 The rapid review was not registered with PROSPERO.
Search strategy
An information specialist experienced in digital health resources (CG) developed the search strategy based on the terms for population, context, phenomena of interest, study design and time frame (Supplemental File 1). The search was conducted in six electronic databases: Cumulative Index of Nursing and Allied Health Literature (CINAHL), Cochrane Library, Embase, Engineering Village, the PubMed version of Medline, and Web of Science for the time period January 2015 to December 2022. In contrast to a full systematic review, we did not search unpublished literature or reference lists and we limited the databases to six and kept the search period short. No relevant literature for the brain tumour population was identified, so the search strategy was adapted to cover all types of cancer. Titles and abstracts of retrieved articles were exported into Covidence 36 and duplicates removed.
Screening and quality appraisal
Titles and abstracts were screened against pre-defined inclusion and exclusion criteria (Supplemental File 2). We obtained full-text articles that met the inclusion criteria and each was screened by one member of the research team (VS, TO, MaK) and discussed if eligibility was unclear.
In line with our rapid review synthesis approach, we included original research as well as literature reviews to achieve conceptual saturation faster.
37
Articles reporting barriers or facilitators to implementing patient-facing self-management web- and mobile-based health technologies for the following psychosocial challenges in adult cancer patients were included:
Those including children or incorporating additional wearables or sensors, virtual or augmented reality add-ons, or for general health promotion, were excluded as out of scope for BT Online.
No formal quality appraisal was conducted in the rapid review. However, we used appraisal prompts to identify fatally flawed papers, a process used by Dixon-Woods et al. 38 Five appraisal prompts considered clearly reported aims, accurate design of the research, appropriate methodology, appropriate data analysis and sufficient data display to support the conclusions. These prompts were applied to all study types and reviews and allowed a judgement of research quality. No papers with fatal flaws were identified, however some methodologically weaker papers were included as judged to be informative.
Data extraction and synthesis
The full texts of the included publications were imported into NVivo (Version 12). 39 First, study location, aim, cancer type, intervention, design and participants were extracted and organised in a summary table (Supplemental File 3). Second, qualitative data reporting implementation barriers and facilitators were extracted from the results and discussion sections of the articles. Extracted data included direct quotations from participants, as well as key concepts or themes developed by the authors through an interpretive process. 37
Findings were synthesised in accordance with Thomas and Harden's 37 thematic synthesis approach. The process involved: (a) three researchers (MaK, VS, TO) independently double coding the results and discussion sections line by line for all included studies for inter-coder reliability; (b) one researcher (MaK) grouping the codes into overarching themes; (c) the key investigator group commenting on the emergent thematic structure after presentation with subsequent refinement.
Rapid review search results
The search identified 435 papers with an additional three identified in an updated search. After the removal of duplicates, 235 titles and abstracts were screened for relevance, followed by full-text review of 52 papers, with 11 papers included in the final review (Figure 2).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart.
Implementation strategy methods
The themes from the rapid review identified factors important to DHS implementation for people with cancer. These were checked against the determinants from the general population DHS implementation guidelines for additional facilitators or barriers to be considered but not identified in the rapid review. All themes were expressed as facilitators and entered into an Excel spreadsheet. The determinants from the guidelines were mapped to each theme and entered into an adjacent column. Additional rows were created for determinants that were not identified in the rapid review themes. The themes and DHS determinants combined provided the overarching framework to develop an implementation strategy for BT Online. Two authors (MaK, VS) systematically matched the facilitators with measures to be taken to ensure a successful implementation of the digital platform. In a third column, the specific steps that addressed the facilitator for implementation of BT Online were recorded. For better visual representation a table was created for each theme in a Word document, listing the theme, the determinants and the implementation steps. In columns next to the implementation steps, it was recorded by whom and when the step would be completed. The tables were used in two team meetings to discuss and refine the implementation steps. We also used information from prior co-design interviews and workshops with patients, carers and HCP when this information was relevant to the implementation.
Results
Digital health implementation guidelines
The preparatory screening of Pubmed identified three ehealth service implementation guidelines. Cremers et al. 40 published a checklist based on a literature review and two Delphi panels with ehealth experts. Similarly, Schreiweiss et al. 41 produced a list of 77 barriers and 292 facilitators based on a literature review and workshops with medical and health informatics experts. Finally, a systematic review of systematic reviews by Ross et al. 20 presented important factors for the implementation of DHS, based on categories from the Consolidated Framework for Implementation Research. 42
Rapid review findings
The rapid review identified 11 research papers reporting DHS with varying aims including physical symptom management (tumour-related fatigue) and psychotherapeutic support (Supplemental File 3). Six evaluated studies with specific interventions, while five were literature reviews or evidence syntheses. No research papers included DHS to manage return to work or study. Most included all cancer types, some only specific cancers and none were specific for brain tumours. Two research papers included management of both cancers and other chronic diseases.21,43 The ten themes developed from the rapid review are presented in Table 1.
Themes, their content description and illustrative quotes.

Implementation strategy
The implementation strategy for BT Online included 51 steps and was developed to implement the platform prototype as part of the research study. The implementation steps will be reviewed during the platform evaluation phase and adapted for long-term implementation and sustainability aiming for public availability. The implementation steps for each of the themes outlined in Table 1 are listed in ten theme-specific tables (Supplemental File 4).
Awareness of the availability of the platform Institutional integration, support, planning and user training
To use the platform, the target audience must be aware of it and its features
20
(Table 2). HCP distributed flyers and business cards during clinical appointments, which explained BT Online and provided a web link and QR access code. Information was also sent via email by HCP directly to their patients. BT Online was also promoted via networks of partner organisations and cancer support organisations, including via social media posts, print newsletters, and information sessions, including some held online. An introductory video was created in which HCPs and a carer provided an overview of the platform features and instructions to navigate the site.
Example of implementation steps for theme 1.

HCP: healthcare professional; BT Online: brain tumours online.
This theme covers several crucial sub-themes. First, planning the implementation strategy is essential, and ideally should be evidence-based and with the guidance of frameworks.20,40 We also took this approach and added discussions during team meetings. Second, key stakeholders must be involved and partnerships built with organisations with a shared vision.20,40,41 We used a multidisciplinary team of HCPs across four health institutions and several advocacy groups. Collaborations with national advocacy groups allowed inclusion of their resources to support navigating government and other social support systems. Third, institutional support and integration of the digital platform into existing systems is essential.20,41 We used key HCP such as cancer care coordinators or nurse navigators as champions to facilitate this integration. While the rapid review did not specifically identify champions or local opinion leaders, we considered them essential clinical partners to promote the platform to their colleagues, answer questions and refer patients and carers.
20
Fourth, for maximum usability, guidelines recommend that users are trained and educated to use the DHS.20,40 Our literature review emphasised that instructions and training material in various formats improve user benefits and equity of access. BT Online presents information in a range of formats, including text, video, and user-generated stories. Summaries of resources provide context to the information and help with navigation. Trained HCP moderators are available for questions within the online community.
Data security, legal requirements, and liability
A major concern for DHS is misuse of personal data. DHS implementation will be jeopardised, if users are reluctant to join because they doubt data security. Therefore, legal requirements must be met and ownership of IP and liability clarified.20,40,41 At present, BT Online can only be accessed as part of a research study, which requires participants to meet eligibility criteria and provide consent. They must provide an email address when registering for the platform for data analysis and evaluation purposes. BT Online also offers a social networking space through Mighty Networks, which is a closed community and requires an additional login and verification of the study participant by a moderator of the community. For additional data safety, users may use a pseudonym within the community if they prefer.
BT Online adheres to the Australian Privacy Principles. 49 Thus, all communication between users and servers is via encrypted connections and data is encrypted at rest so data compromise is unlikely. An expert digital product development team built the platform.
Consultations with institutional Human Research Ethics Committee and the legal teams also enhanced cybersecurity. BT Online links to overseas third-party software, subject to differing legislation, therefore users are informed in the Participant Information and Consent Form, as well as the terms and conditions section, that the usage of their data is outside our control if they decide to use third-party providers. Some of these implementation steps must be reviewed and modified once the research has concluded and the platform is publicly available. Table 3 provides an example of the implementation strategy for this theme.
Platform quality, relevance and usability, including technical challenges
Example of implementation steps for theme 3.

Usability of the platform is a key feature for successful implementation, highlighted in our rapid review and existing guidelines.20,40,41 It encompasses platform quality, its design and elimination of technical issues. BT Online has been co-designed with high levels of consumer engagement to include end-user preferences. Patients, carers and HCP expressed their preferences and provided feedback on the design, ease of use, language and functionality at regular team meetings, during interviews and workshops and at usability testing, which was incorporated by the digital product development team. Our rapid review identified time commitment to the DHS as important to use, which is likely not relevant to BT Online as use can be episodic, irregular and has no time constraints.
Technical malfunctions and other issues can be reported via the website and rectified.
Accessibility Belief in the benefit of and positive attitude towards the platform Holistic and tailored
Accessibility refers to user ease of access to and navigation of the platform, considering illness constraints and digital or health literacy.40,41 Based on end-user feedback, we added video content on some features and topics of the platform. A read-aloud option was also discussed but not added at this stage due to insufficient resources. BT Online is accessible on computers, tablets and mobile phones to provide portability of access. The platform is self-paced allowing users any pace and to take breaks when suffering illness or caring related fatigue.
Belief in the benefit of a DHS and a positive attitude towards it are facilitators to implementation, with negative attitudes a barrier that could result in resistance to use.20,41 In addition, our rapid review highlighted that social proof of others’ benefit from the platform may encourage users. Our strategy includes to seek feedback on perceived benefits during usability testing and to provide a ‘welcome video’, in which patients, carers and HCP give testimony to the potential benefits of the platform. BT Online features regular Q&A webinars during which presenters (patients, carers and HCP) also highlight benefits of the platform. Posting user product reviews on the platform itself is another strategy by which users can express their positive experience with the platform and to engage others.
A DHS adapted to user needs and preferences is more likely to be accepted and utilised.20,40 Our rapid review emphasised the importance of addressing the holistic needs of users, offering a wellbeing focus, providing user-specific content, with control over the amount and timing of data access.
Strategies for implementation success include specific and customised content for brain tumour patients, their carers and HCP, with the ability to choose the time, place and type of content they access and with control of the amount of personal information they want to provide. As an exception in the research evaluation phase of BT Online, users are required to provide an email address for data linking purposes when registering for the platform. Following advice from users, content warnings were added to the platform to highlight material that covers death and dying, self-harm and suicide, adult themes, confronting medical images and Aboriginal and Torres Strait Islander cultural sensitivities. Filters and search capabilities assist to prioritise content by illness stage, tumour-type, location and age.
Timing of introduction to the platform HCP interface encourages use
While none of the guidelines specifically addressed the ideal moment to introduce the platform to the user, our rapid review identified this as an important consideration for DHS users with cancer. The illness trajectory varies considerably with tumour type, and may influence timing of user introduction to a platform. After discussion in our team meetings, it was considered that this is not likely to be a major implementation barrier as BT Online offers support and resources across tumour types and disease trajectories. Compared to DHS that commence at a particular time of an illness,44,48 our platform offers flexible and self-paced access. However, HCP suggested in workshops that information about the platform may need to be provided repeatedly to patients and carers, depending on their ability to concentrate, remember or engage.
Cremer's guidelines highlight that ‘the presence of key-users [can…] stimulate people to be involved and use the program’.
40
One such strategy to engage users in BT Online was utilisation of HCP and researcher moderators within the online social media community, Mighty Networks. Moderators were assisted by volunteer carers and patients with experience in managing social media groups. Moderators were trained by the project manager and received moderation guidelines. Users also engaged with the platform through interactive monthly Q&A webinars with HCP or people with lived experience hosted on BT Online.
The rapid review also identified that an ‘active’ introduction of the platform, such as during a consultation with an HCP, was a facilitator to implementation and engagement. While time constraints may not allow demonstration of the platform during the appointment, the personal HCP recommendation may encourage users to engage with the platform.
Job roles, workload and disruptions to existing systems
Concerns about increased workload and disruptions to existing systems such as alterations of clinical processes, incorporation of new technology or job redesign were identified in our rapid review and highlighted in all three guidelines.20,40,41
We expect that BT Online will have minimal impact on routine care as it provides an additional and parallel service to patients, carers and HCP rather than disrupting routine care. However, HCP workload may be affected if they face additional questions related to specific BT Online features during a consultation. In interviews and workshops, patients expressed a wish for symptom monitoring through the platform with direct feedback to an HCP, however, HCP considered this an item for future platform iterations due to limited resources.
Discussion
To address the specific needs and challenges of brain tumour patients and their carers and HCP, we have generated an evidence-informed implementation strategy for a DHS, BT Online. In contrast to prior work, which focussed on adapting existing implementation frameworks, we embarked on a novel approach to develop our implementation strategy, guided by rigorous research processes. These were, first, the rapid review, which identified specific challenges and needs of the cancer community. Second, we used research-generated guidelines of implementation determinants of DHS to strengthen the themes of the rapid review. Third, the strategy was informed by interviews, workshops and team meetings conducted during the prototype development phase of the overall project, adding an additional source of information from target end-users, specifically brain tumour patients, their carers and HCP. Fourth, the implementation strategy was presented to key investigators of this project who provided feedback, thus gaining input from digital health experts, HCP, patients, carers and researchers. Our process resulted in 51 concrete steps to guide the implementation of BT Online. This list provided a reference for discussions in key investigator meetings around particular implementation steps that were or were not possible within the project resources.
Many of the determinants laid out in the guidelines matched the themes from the rapid review, even though the breadth of the themes necessitated the allocation of multiple determinants to each theme. For example, the determinants of costs, resources, financing, planning, strategy, organisational support, involvement of stakeholders and leadership engagement were all reflected in the theme on institutional integration, support, planning and user training. The guidelines used in developing the implementation strategy focused on ehealth services, a much broader spectrum of electronic health services, devices, programmes and digital interventions than needed for the development of our DHS. Hence, determinants irrelevant to our project were not considered in the implementation strategy. For example, automatic data transfer to electronic medical records or connection with wearable devices 40 were out of scope but may be future expansions.
All three guidelines20,40,41 outline the importance of sufficient funding and resources for the implementation of DHS. Our rapid review touched on this within some themes, but it was not a prominent factor. This is most likely due to the nature of the included literature, which mainly reports user opinions and lacks reports from researchers and resource managers accompanying the implementation process. Our implementation strategy included steps possible within the existing research budget but had to relinquish effective strategies, such as providing more video resources or paying a carer, patient, or HCP to spend exclusive hours as a moderator in the online community. Consequently, volunteer moderators were recruited. A systematic review identified that engagement from HCP and peers contributes to a feeling of social connectedness, known to be an important factor to keep DHS users engaged. 50 While that review focused on a mental health population, people with brain tumours and their carers have also reported a need for social connectedness to overcome social, physical and geographic isolation.51,52 The future evaluation of our implementation strategy will determine if the voluntary engagement of moderators is sustainable, particularly once the platform is publicly available, or if future funding will need to be secured to facilitate this important determinant of DHS use.
Sufficient funding is a key facilitator to sustainable use and upscaling of DHS.20,40 While working within the study budget for prototype implementation, we prospectively designed an economic evaluation alongside the prototype implementation to understand if there is an economic impact for users or on the healthcare services, as a result of access to BT Online, which will guide our long-term implementation strategy.
While not an implementation step for the testing phase of the platform, evaluation is an important facilitator for successful and sustained implementation in the guidelines20,40 to ensure constant monitoring, feedback and adaptation of the DHS. 53 Assessing the success of our implementation strategy is crucial due to its novel development approach, but more importantly, to provide evidence to potential funders and users for the broader distribution and expansion of BT Online. Evaluation of the platform itself will identify user perceptions and necessary future features. As such, the implementation strategy is a fluid framework that requires adaptation as BT Online progresses.
Limitations
Rapid reviews have been used to inform DHS implementation processes or digital health policies previously.32,33 Using rapid methodologies in reviews and for thematic analysis are well-accepted methods to generate evidence in time- and resource-limited settings.31,54 While they offer valuable insights within tight timeframes, they may not cover all relevant literature due to time constraints. These were mitigated through searching across multiple databases and inclusion of a quality judgement of the studies incorporated in our analysis. 55
The terminology around DHS is varied and inconsistent. 56 Over recent years, ehealth has developed from the simple use of telehealth and digital data in the health sector 57 to the use of wearable devices and more recently to sophisticated self-managed digital interventions (with or without input from HCP) and complex integrated systems that link individuals and treatment teams with electronic medical records. 58 More commonly the term digital health is now used for ehealth and mhealth. 58 Despite clear search and eligibility criteria, it was not always possible to limit the literature to that most similar to our digital platform as DHS are reported with varying terminology. We, therefore, included literature with DHS that contained various aspects of digitally supporting users and selected those implementation determinants that were relevant to our digital platform.
Implications
Our novel approach to developing an implementation strategy may inform researchers who find that traditional implementation frameworks do not entirely match their project purpose. Our approach can provide a guiding framework to facilitate rapid insights from a literature review combined with research-based guidelines that complemented and enhanced the rapid review findings. The input of a multidisciplinary team in the development of concrete implementation steps strengthened this approach.
A well-structured and evidence-informed implementation strategy will facilitate the preparatory work and launch of our platform for brain tumour patients, their carers and HCP. Furthermore, it may enable user-acceptance and uptake of the supportive care provided through BT Online. It will function as an evaluation framework of our own implementation strategy to measure its success or failure and the individual steps can be adapted accordingly. Our concrete implementation steps may be useful for other researchers or organisations who are developing, implementing, and evaluating other DHS for a brain tumour community.
Conclusion
This research is one component of many to make BT Online a valuable and easy-to-use online resource for patients with a brain tumour and their carers and HCP. To develop this implementation strategy, we combined two components important to a tailored implementation strategy for our digital platform: (1) specific barriers and facilitators to introducing DHS to people affected by cancer and (2) specific barriers and facilitators to implementing DHS. This resulted in a rigorous evidence-informed implementation strategy matched with 51 practical steps to efficiently introduce BT Online to its users. This specific and evidence-informed implementation strategy increases the likelihood of BT Online's success and sustainability. The future evaluation of BT Online will include an evaluation of this implementation strategy to identify its strength and weakness.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251316713 - Supplemental material for Development of an evidence-informed implementation strategy for a digital supportive care platform for brain tumour patients, their carers and healthcare professionals
Supplemental material, sj-docx-1-dhj-10.1177_20552076251316713 for Development of an evidence-informed implementation strategy for a digital supportive care platform for brain tumour patients, their carers and healthcare professionals by Verena Schadewaldt, Teresa O’Brien, Mahima Kalla, Meinir Krishnasamy, Kara Burns, Sarah CE Bray, Cecily Gilbert, Richard De Abreu Lourenco, Joseph Thomas, Daniel Capurro, Wendy Chapman, Ann Borda, Rana S Dhillon, James R Whittle and Katharine J Drummond in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251316713 - Supplemental material for Development of an evidence-informed implementation strategy for a digital supportive care platform for brain tumour patients, their carers and healthcare professionals
Supplemental material, sj-docx-2-dhj-10.1177_20552076251316713 for Development of an evidence-informed implementation strategy for a digital supportive care platform for brain tumour patients, their carers and healthcare professionals by Verena Schadewaldt, Teresa O’Brien, Mahima Kalla, Meinir Krishnasamy, Kara Burns, Sarah CE Bray, Cecily Gilbert, Richard De Abreu Lourenco, Joseph Thomas, Daniel Capurro, Wendy Chapman, Ann Borda, Rana S Dhillon, James R Whittle and Katharine J Drummond in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251316713 - Supplemental material for Development of an evidence-informed implementation strategy for a digital supportive care platform for brain tumour patients, their carers and healthcare professionals
Supplemental material, sj-docx-3-dhj-10.1177_20552076251316713 for Development of an evidence-informed implementation strategy for a digital supportive care platform for brain tumour patients, their carers and healthcare professionals by Verena Schadewaldt, Teresa O’Brien, Mahima Kalla, Meinir Krishnasamy, Kara Burns, Sarah CE Bray, Cecily Gilbert, Richard De Abreu Lourenco, Joseph Thomas, Daniel Capurro, Wendy Chapman, Ann Borda, Rana S Dhillon, James R Whittle and Katharine J Drummond in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076251316713 - Supplemental material for Development of an evidence-informed implementation strategy for a digital supportive care platform for brain tumour patients, their carers and healthcare professionals
Supplemental material, sj-docx-4-dhj-10.1177_20552076251316713 for Development of an evidence-informed implementation strategy for a digital supportive care platform for brain tumour patients, their carers and healthcare professionals by Verena Schadewaldt, Teresa O’Brien, Mahima Kalla, Meinir Krishnasamy, Kara Burns, Sarah CE Bray, Cecily Gilbert, Richard De Abreu Lourenco, Joseph Thomas, Daniel Capurro, Wendy Chapman, Ann Borda, Rana S Dhillon, James R Whittle and Katharine J Drummond in DIGITAL HEALTH
Supplemental Material
sj-docx-5-dhj-10.1177_20552076251316713 - Supplemental material for Development of an evidence-informed implementation strategy for a digital supportive care platform for brain tumour patients, their carers and healthcare professionals
Supplemental material, sj-docx-5-dhj-10.1177_20552076251316713 for Development of an evidence-informed implementation strategy for a digital supportive care platform for brain tumour patients, their carers and healthcare professionals by Verena Schadewaldt, Teresa O’Brien, Mahima Kalla, Meinir Krishnasamy, Kara Burns, Sarah CE Bray, Cecily Gilbert, Richard De Abreu Lourenco, Joseph Thomas, Daniel Capurro, Wendy Chapman, Ann Borda, Rana S Dhillon, James R Whittle and Katharine J Drummond in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors thank the patients, carers, consumer advocates, healthcare professionals and researchers who have shaped this implementation strategy through their input in meetings, workshops and interviews. We appreciate their valuable time spent on this study.
Author contributions
VS, MaK, MeK, KB, SB, CG, RDAL, JT, DC, WC, AB, RD, JW, and KD conceptualised the overall project. MaK developed the methodology for the rapid review, VS developed the methodology for the implementation strategy. MaK, VS, TO, MeK, KB and CG conducted the literature review. VS and MaK developed the steps for the implementation strategy. VS, MeK, RDAL, JT, DC, AB, WC, RD, JW, and KD contributed to the funding acquisition by successful application for the MRFF grant. SB, MaK, VS, MeK, and KD were responsible for the management and coordination of the research activities for the project and provided supervision. VS, MaK, and TO wrote the original draft of the manuscript. All authors participated in data validation through feedback on themes of the rapid review and components of the implementation strategy and reviewed the manuscript, edited for important intellectual content and approved the final version.
Data availability
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Melbourne Health Human Research Ethics Committee HREC/77238/MH-2021 on 19 August 2021 for phase 1 and (HREC/89522/MH-2022) on 22 December 2022 for phase 2.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medical Research Future Fund (MRFF) 2020 Brain Cancer Survivorship Grant [MRFBCII000014].
Informed consent
Participants who took part in an interview signed a consent form.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.