
Abstract
Objective
This study explored the perceived benefits, barriers, and recommendations of telerehabilitation for musculoskeletal disorders among physiotherapists in Malaysia.
Methods
This study employed an exploratory qualitative methodology to gather the perceptions of government-employed physiotherapists in Malaysia regarding the benefits, barriers, and recommendations for telerehabilitation in treating musculoskeletal disorders. The researchers conducted semistructured focus group discussions (FGDs) via Google Meet, which were recorded, transcribed, and analyzed using thematic analysis.
Results
Five FGDs were conducted with 24 participants, 37.5% of whom had prior experience with telerehabilitation. The data analysis returned three main themes: (1) perceived benefits, (2) barriers, and (3) recommendations. Four subthemes were derived from perceived benefits: (1a) saving time and money, (1b) convenience, (1c) clients responsible for their treatment, and (1d) alternatives for infectious diseases. Perceived barriers revealed three subthemes: (2a) technology, (2b) organization, and (2c) personal barriers. Finally, participants provided recommendations for improving telerehabilitation services, including training programs to facilitate greater acceptance of this modality.
Conclusion
The findings of this study offer crucial insights into the evolving landscape of telerehabilitation in Malaysia. These findings revealed a greater prevalence of barriers to enablers among Malaysian physiotherapists, potentially influenced by varying experience levels. Despite the prevailing lack of experience among participants, this research underscores the significance of identifying barriers and enablers in implementing telerehabilitation with participants offering recommendations for integrating telerehabilitation into their practices. This study provides clear insights and a roadmap for stakeholders aiming to shape the future of telerehabilitation among physiotherapists in Malaysia.
Introduction
Musculoskeletal disorders are among the most common disorders that contribute to the global disease burden. 1 Approximately one in three people worldwide has chronic painful musculoskeletal conditions. 2 Musculoskeletal disorders contributed to a 36% loss of productive life years in 2010 and are expected to increase to 34% by 2030. 3 In 2019, more than 66% of adults with musculoskeletal disorders benefited from rehabilitation. 4
According to the World Physiotherapy in 2022, the physiotherapist-to-population ratio in Malaysia was reported to be 0.92 per 10,000 people. This figure is considerably lower than those of Singapore and Thailand, which had ratios of 4.14 and 2.14 per 10,000 people, respectively. This suggests a noticeable shortage of physiotherapists in Malaysia compared to its neighboring countries. 5 According to the Ministry of Health Malaysia's Allied Health Science Division, there were 1632 government-employed physiotherapists in Malaysia by 2020. 6 The same report highlighted a shortage of physiotherapists in the government sector due to several factors, including the high number of patients referred for physiotherapy and increased cases of noncommunicable diseases. In addition, a previous report showed that the total number of patients seen by physiotherapists from 2017 to 2019 increased annually by up to 2%. 6
Recognizing the increasing demand for physiotherapy services and considering the challenges in timely appointments, one option to alleviate the delay in rendering or receiving a physiotherapy appointment is telerehabilitation. Telerehabilitation has gained prominence as a valuable resource in healthcare management, particularly in physiotherapy for musculoskeletal conditions, during the coronavirus disease 19 pandemic. 7 Its implementation, particularly during a pandemic, was driven by the need to provide patient care while observing social distancing measures to minimize the risk of viral transmission. 8 Telerehabilitation is defined as the provision of rehabilitation interventions carried out virtually between physiotherapists and clients at home or in a remote location through various telecommunication technologies. 9 Research has shown that physiotherapy carried out via telerehabilitation may be as effective as in-person therapy for a variety of musculoskeletal conditions, including low back pain, 10 neck pain, 11 and total knee replacement. 12 In addition, physiotherapy assessment via telerehabilitation is recognized as a valid and reliable tool for assessing the cervical spine. 13
Telerehabilitation has shown promise in enhancing physical pain associated with various musculoskeletal conditions. Its efficacy has been underscored as a practical approach for ensuring continuous rehabilitation services. Moreover, it has demonstrated cost-effectiveness while minimizing travel time for clients and money.14–16 While telerehabilitation provides convenient access to physiotherapy services for clients, 17 unpublished data suggest that only a limited number of physiotherapists in Malaysia currently utilize telerehabilitation. The growing acceptance of telerehabilitation among physiotherapists in Western countries is evident. However, the reasons for the relatively lower uptake of telerehabilitation in Malaysia, especially when compared to other allied health professions, such as speech-language therapists, remain unclear.
Several studies in Malaysia have demonstrated the suitability of speech-language therapy in telerehabilitation for speech therapy. These studies explored the delivery of intensive voice therapy, the development of a stuttering self-monitoring solution for stutterers, 18 the creation of mobile apps for aphasia patients, and the implementation of telerehabilitation during the coronavirus 19 pandemic. Approximately 75% of speech-language therapists in Malaysia had prior experience with telerehabilitation, even before the pandemic. Singh et al. 19 even noted its integration into the local university's coursework offered at the undergraduate level. The efficacy of telerehabilitation in speech and language services is attributed to its audio-visual nature, demonstrating its effectiveness in clinical interactions and techniques. Despite the increase in telerehabilitation, reports in the literature have consistently highlighted key barriers, including technology, such as low client technological literacy, 20 unstable internet signals,21–23 inadequate technology infrastructures, 14 the substantial expense of technology required in telerehabilitation 24 and the dearth of comprehensive training in telerehabilitation.21–23,25
Recognizing the importance of delving into the perceptions of telerehabilitation in depth, clinicians in a mixed-method study held the perception that telerehabilitation has the potential to provide appropriate support. 26 Moreover, in a qualitative study, the perceptions of physicians regarding virtual healthcares for Parkinson's disease were found to encompass both positive and negative voices, depending on technical concerns. 27 A survey of 1034 healthcare professionals revealed a positive shift in perceptions of telerehabilitation, with 44% of them considering it a feasible method for monitoring and delivering care with increased awareness and knowledge. 28 A recent quantitative study has demonstrated that young physiotherapists in Turkey hold a positive perspective on telerehabilitation for chronic conditions and exhibit a strong preference toward it. 29 Moreover, speech-language therapists in Malaysia also demonstrated favorable attitudes toward telerehabilitation, which can be attributed to their increased familiarity and training. 19 Although research teams23,30 in Western countries have identified and explored the possible factors that influence the use of telerehabilitation through qualitative approaches, little is known about perceptions of telerehabilitation in musculoskeletal disorders within Malaysia. This study aimed to explore the perceived benefits, barriers, and recommendations of telerehabilitation in musculoskeletal practice among physiotherapists in Malaysia.
Methods
Study design and setting
This study employed an exploratory qualitative design and utilized focus group discussions (FGDs) to delve into insiders’ perceptions of physiotherapists, providing an enriched understanding 31 and an added dimension to the interaction within the physiotherapy context. 32 The consolidated criteria for reporting qualitative research (COREQ) checklist was used to guide the comprehensiveness of the findings.33–35
Recruitment and sampling
Purposive sampling, a robust method in qualitative research, was employed to ensure the inclusion of all physiotherapists, irrespective of their familiarity with telerehabilitation. 36 The inclusion criterion was physiotherapists working in either the government or private sectors, with a minimum of 2 years of professional experience. This research included all physiotherapists and did not have any specific exclusion criteria. The recruitment process commenced with a list of potential participants sourced from an unpublished but recently completed survey. 37 Of the 32 physiotherapists who were contacted, eight declined to participate, citing scheduling conflicts and a lack of interest in the subject matter. The recruitment process occurred via email or phone communication by the researcher upon confirmation of their eligibility to participate. 38 The participants were informed of the FGD a day in advance through email notification. Additionally, they were provided with information on the online platform that would be used, including a participant link and a reminder of the discussion's date and time. Prior to the start of the session, written consent was obtained from each participant. 39 Data saturation, as suggested by past literature, depends on obtaining an adequate sample size. It is stated that data saturation can be achieved after five FGDs 40 or when no new themes or information are discovered. 41 In an earlier study, 4–5 participants in each online FGD discussion led to the desired outcome. 39
The focus groups were led by two physiotherapists: Lee Lee Sia (LLS) and Nurul Syuhada Mohd Rosnu (NSMR). Both LLS and NSMR are females currently pursuing a PhD in the Physiotherapy program, holding Bachelor of Science degrees. Additionally, they have completed two courses in qualitative research. LLS, a senior physiotherapist, fulfills the role of main researcher and moderator, while NSMR assists during the sessions, also working as a lecturer. The research team had no prior relationships with the participants recruited for the FGDs. Participants were informed about the researchers’ roles and the purpose of the study during the informed consent process. The moderators established rapport with participants at the beginning of each focus group to create a comfortable environment for sharing experiences and perspectives.
Data collection
Five virtual FGDs were conducted between November and December 2022 using Google Meets with a total of 24 participants. Each FGD consisted of four to five participants. A semistructured interview guide with open-ended questions was developed based on a literature review and expert opinions. The FGDs were conducted by LLS and NSMR. LLS moderated the discussion, while NSMR provided technical assistance to the participants and was responsible for taking field notes. 38 During the FGDs, the moderator (LLS) posed suitable probing and follow-up questions to elicit an in-depth description of the participants’ perceptions and took steps to ensure that all participants in the study participated actively and openly. Each session lasted until the moderator felt that the discussion had already reached data saturation as the discussions started to repeat similar ideas. Each FGD session lasted 45–60 min and was audio- and video-recorded. The important points are summarized at the end of the discussion. 42
Data coding and analysis
Six thematic analysis steps were performed to identify and report themes within the transcripts. 43 The researcher read the transcripts several times for familiarization purposes. The initial codes were systematically generated using a semistructured question guide. The codes were compiled when potential themes were identified. Reviewing and recoding these potential themes helped create the thematic “map” of the analysis, which was then enhanced by naming each theme with a clear definition. Finally, a report was written using appropriate examples.43–45 The researchers verified and discussed each theme, and all disagreements were resolved through discussion. All transcripts were returned to the participants via email for member checking to ensure the trustworthiness of the results. The research team thoroughly examined and evaluated the feedback obtained from participants via email. 46 NVivo 12 was used for comprehensive qualitative data analysis. The purpose of utilizing NVivo 12 was to ensure rigorous data synthesis and promote transparency throughout the study. 47
Results
Twenty-four physiotherapists (75% women and 25% men) consented to participate in the study, and more than half of the participants were aged 30 to 39 years. Fifty percent of the participants worked with a musculoskeletal clinical population. Table 1 provides information on the demographic characteristics of the physiotherapists included in this study. An overview of the themes and subthemes is presented in Figure 1.
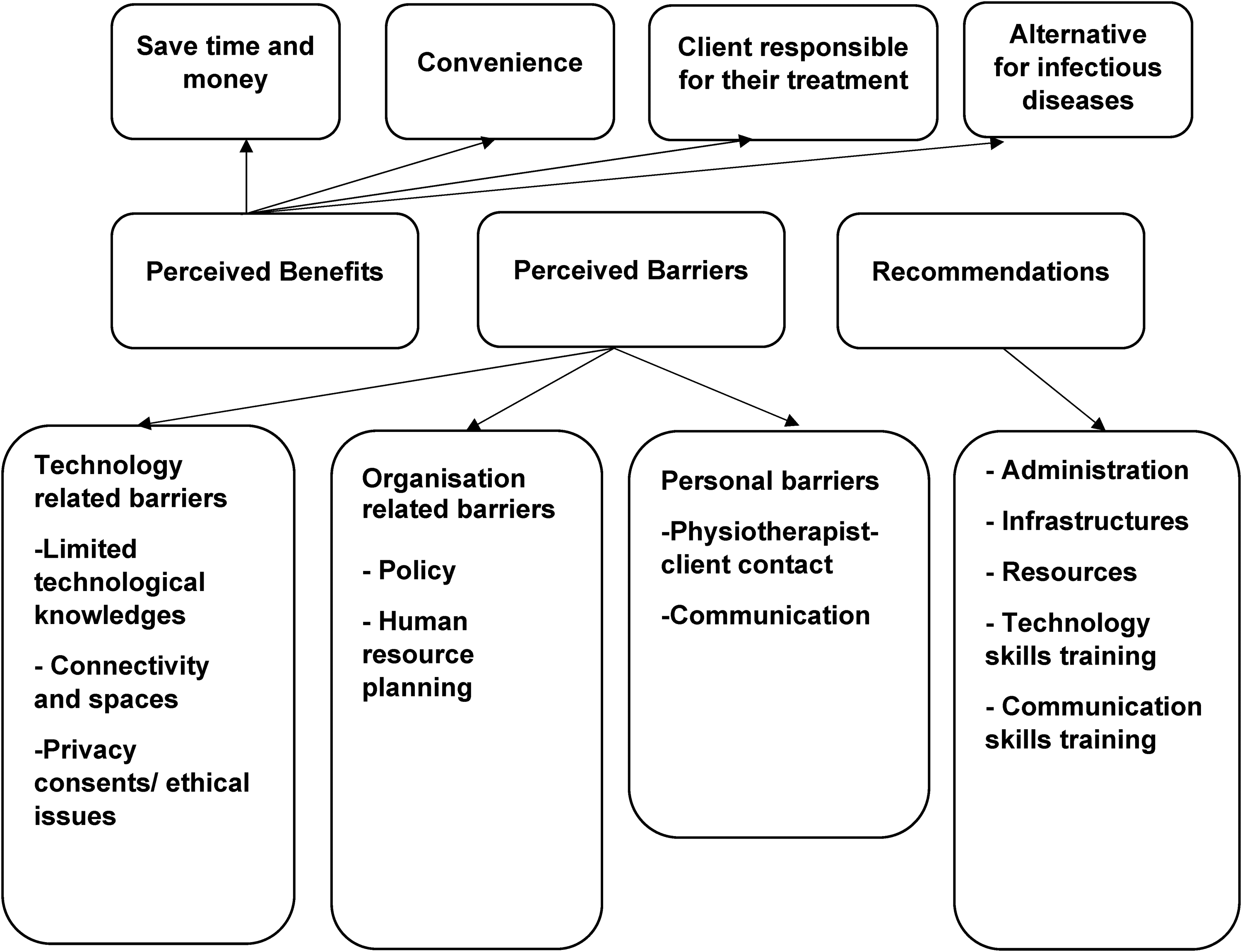
Thematic network for main themes and subthemes.
Demographic information of participants.

Perceived benefits of telerehabilitation
In this study, both experienced and inexperienced participants expressed their expected benefits in several domains, including time savings for clients and physiotherapists, cost savings for clients on travel and transportation, alternative modalities for infectious diseases, and greater client responsibility for their care.
Saves time and money
Participants generally perceived that telerehabilitation could reduce client time. They believed that using telerehabilitation, clients could save time compared to the time spent in hospitals and clinics, especially with traffic jams and poor geography. The participants in the study also highlighted that client, particularly those from rural areas, may have to pay high transportation costs. Hence, they believed that clients might be more willing to receive telerehabilitation.
“…they have to pay to visit the clinic, they’ll be more willing to stay at home, at that point we can phone them…” (Participant 16, clinic, experienced)
“… could help those in urban areas to save time and money…” (018, clinic, experienced) “… maybe can save clients’ money as some of my clients stay in rural areas… they need to use a boat and change to a four-wheel drive vehicle…they need to spend hundreds of ringgits just to come to hospital treatment…” (Participant 3, hospital, inexperienced) “… for some clients, the cost of taxi, which ranges from RM50 to RM60 every hospital visit, is a financial burden…” (Participant 7, hospital, inexperienced)
Convenience
Participants with experience in telerehabilitation who participated in this study explained that they perceived telerehabilitation as convenient and easy to observe for clients who frequently visited. Furthermore, they emphasized that telerehabilitation could be a convenient option for clients who use public transport to the hospital or who need to take it off to attend physiotherapy sessions. “… clients do not need to spend their time searching for limited parking spaces…” (Participant 18, clinic, experienced) “… clients do not need to take time off to seek treatment, as this is easy to approach…” (Participant 23, clinic, experienced)
Clients responsible for their treatment
The participants observed that telerehabilitation require clients to participate more actively in their physiotherapy session. The participants believed that telerehabilitation could encourage active participation by offering self-management tools and allowing exercise in their home environment. “… they will be responsible for their own progression via telerehabilitation; they will need to take action to ensure their progression…” (Participant 16, clinic, experienced)
Alternative for infectious diseases
Participants who experienced telerehabilitation during the pandemic stated that telerehabilitation was an adjunct delivery mode for infectious disorders, particularly during the pandemic. “… Clients were unable to visit the department during the pandemic. Thus, this is a good attempt to manage and treat clients on a virtual platform…” (Participant 1, hospital, experienced) “…Thus far in my clinic, previously during the pandemic, our clinic was one of the clinics assigned for BookDoc sessions, so we used to BookDoc and then physiotherapist or also one of the professions that we used telerehabilitation. For me, er… Telerehabilitation using BookDoc is very convenient and easy to use for the consultation for the client…” (Participant 2, clinic, experienced)
Perceived barriers in telerehabilitation
Although the participants generally agreed that telerehabilitation has several benefits, they identified some potential barriers to its adoption. Three themes and related subthemes emerged prominently in the discussion. These include concerns about technology, organization, and individuals.
Technology-related barriers
Limited technological knowledge
The participants raised concerns about the challenges faced by clients with limited technological skills. In particular, the participants in this study found that some clients in rural areas had difficulty using electronic devices, such as computers and handphones. They also noted that clients in rural areas may lack familiarity with social media platforms such as WhatsApp. “… clients are not good at using computers and handphones…” (Participant 13, clinic, experienced) “… Some clients remained alone. Family members work during the day. Therefore, they're alone at home, so it is difficult for them to use tele rehabilitation…” (020, hospital, inexperienced) “… most of my clients are not even familiar with WhatsApp's…” (Participant 22, clinic, inexperienced) “… is extremely challenging for seniors. Not all older people know how to use smartphones, and some also don’t know how to operate laptops or computers…” (Participant 3, hospital, inexperienced)
One participant mentioned that some physiotherapists had inadequate technological literacy. I believe that some senior physiotherapists found it challenging to conduct Zoom meetings. I’m talking about seniors who are at least fifty years old” (Participant 22, clinic, inexperienced)
Connectivity and space challenges
Participants identified poor internet access, insufficient space for telerehabilitation and inadequate technology equipment at government facilities as barriers. Some worried about inconsistent Internet network coverage in certain regions. They were concerned that the telerehabilitation sessions would be disrupted. In addition, the experienced participants in the sample were concerned about telerehabilitation sessions being interrupted by weak networks, particularly in remote locations. Most participants reported the limited availability or unavailability of technological devices. Some of them raised other barriers, such as the lack of a convenient place for telerehabilitation. Some of those with previous telerehabilitation experience indicated that they felt uncomfortable conducting telerehabilitation in public. “… internet access only available at my counter, where I must compete for the crying of children who's come together with their parents…” (Participant 1, hospital, experienced) “… people are walking by and there is noise from the equipment while I am conducting telerehabilitation…” (Participant 1, hospital, experienced) “… My unit has four computers, but none have webcams…” (Participant 24, hospital, inexperienced) “…webcam also considered a limitation, and we must plan when we will use the computer because we only have a limited number of computers…” (Participant 8, clinic, inexperienced)
Privacy concerns/ethical issues
According to the participants in the study, privacy and confidentiality issues were identified as potential barriers to telerehabilitation. One participant specifically raised the concern that clients may misuse their privacy by contacting them outside of regular office hours. “…I found that clients might suggest their relatives to you as well and that they sometimes contact me on weekends, which violates my privacy…” (Participant 22, clinic, inexperienced)
Furthermore, another participant mentioned the confidentiality of the clients’ profiles and records. They raised concerns that telerehabilitation may expose client information, particularly under sensitive conditions. Confidentiality concerns may arise in telerehabilitation as a result of the digital nature of records. Data can be vulnerable to hackers or unauthorized access. “…In terms of therapist safety, for example, the therapist can record the session using BookDoc; if the therapist uses an application that cannot record and the client complains, we do not have enough proof…” (002, clinic, experienced) “…internet is unsafe; we do not know if some hacker is spying on our conversation during the therapy session…” (008, clinic, inexperienced)
Organization-related barriers
Policy
The participants in the study conveyed that the implementation of telerehabilitation lacked an evident policy framework. They emphasized the need for robust policies to safeguard their interests and enhance their confidence. “…we have no policy regarding this; thus, anyone can potentially generate electronic records and use them as proof…” (Participant 17, hospital, experienced)
Human resource planning
The participants in the study emphasized the importance of human resource planning. According to most participants in the study, if staffing levels were not increased, there would not be sufficient manpower for success. Several participants in the FGD mentioned that they conducted physiotherapy alone in their units. “… In our hospital, we have enough physical therapists to cover the ward and outpatients. Therefore, if one of the physiotherapists is not available, it will be tough for the rest of us…” (Participant 24, hospital, inexperienced) “… I agree with the issue of manpower I am currently working alone in the unit, and it is quite difficult for me to manage telerehabilitation…” (Participant 23, clinic, inexperienced)
Personal barriers
Physiotherapist–client contact
In general, all participants agreed that physical contact between physiotherapists and clients is necessary for assessment, evaluation, diagnosis, and treatment because of the nature of physiotherapy care. A participant with experience in telerehabilitation expressed dissatisfaction with the lack of physical contact during the assessments and interventions. Another participant with telerehabilitation experience who participated in the study highlighted concerns about the possibility of parents being unable to perform the taught techniques, as demonstrated. “… I was dissatisfied because I could not do physical observation and assessment in person…” (Participant 18, clinic, experienced) “… We were unable to measure our clients’ physical performance, which made it difficult to assist them. This may be because we lack a comprehensive view of them…” (Participant 10, clinic, experienced) “…although we conduct hands-on skills on our pediatric patients and teach their carers how to perform them at home, their handling techniques may differ from those that we teach…” (Participant 19, clinic, inexperienced) “… even during in-person sessions, clients might carry out the exercises incorrectly; however, if the session is conducted virtually, I believe they will make much more mistakes…” (Participant 14, hospital, inexperienced)
Communication-related barriers
The participants who participated in the study expressed worries about potential obstacles in communication that may have emerged during the implementation of telerehabilitation. Their main concern was that clients might misunderstand the instructions provided by physiotherapists when using virtual platforms. Furthermore, they also noted the possibility of clients becoming less engaged and having more trouble remembering their appointments in the context of telerehabilitation. “…I'm worried that they will misinterpret our messages…” (Participant 5, hospital, inexperienced) “…my clients are mostly old, so communicating over the phone will be challenging…” (Participant 19, clinic, inexperienced) “…we scheduled an appointment with the client, and then they said they were still outside and could not make it, so we wasted our time sitting in front of the computer…” (Participant 12, hospital, inexperienced)
Recommendations for future telerehabilitation
Several suggestions have been proposed to improve the effectiveness of potential telerehabilitation initiatives. The participants also underscored the necessity for increased administrative support, ensuring sufficient infrastructure, and allocating appropriate resources such as computers equipped with video conferencing capabilities and dedicated spaces for telerehabilitation. Furthermore, they strongly advocated the development and implementation of comprehensive telerehabilitation policies to ensure security and wellbeing. "…the organization must provide space…” (Participant 11, hospital, experienced) “… we need a policy to protect us. If something bad happens to a client, who will hold the responsibility? …” (Participant 23, clinic, experienced) “…we require extra dedicated physiotherapists to focus on telerehabilitation so that the physiotherapist is not distracted by other activities during telerehabilitation…” (Participant 4, hospital, inexperienced)
Proper training was deemed crucial for physiotherapists using telerehabilitation. They recognized the direct connection between suitable training and the success of telerehabilitation sessions. The participants in the study were keenly aware that physiotherapists varied in technological proficiency and training requirements when working with unfamiliar technical tools. Furthermore, they emphasized the necessity for training in technology skills, including setting up technology devices and addressing technical issues. “…perhaps a training in camera basics, lighting setup, and audio setup before telerehabilitation…” (Participant 10, clinic, experienced) “…because we cannot ask for assistance while conducting telerehabilitation, the physiotherapist should have a basic knowledge of how to operate the computer on their own…” (Participant 6, hospital, inexperienced) I agree that ICT (Information and Communications Technology) training is needed. For example, Google Meet is difficult for me when I first use it…” (Participant 7, hospital, inexperienced)
Some participants also expressed the need for training related to communication skills related to telerehabilitation. Compared to in-person sessions, they believed that they would need more effective communication skills to conduct telerehabilitation, including body gestures and effective and interesting techniques for communicating and demonstrating treatments. “…I would say effective communication is very important, as I am a Chinese person, and I need to convey messages effectively to clients of all races through screens…” (Participant 24, hospital, inexperienced) “…I agreed that effective communication should be considered as well since we have to know how actually to draw their attention because it is not face to face…” (Participant 8, clinic, inexperienced)
Conversely, some participants maintained that communication skills are closely tied to personal growth acquired through their professional experiences, regardless of any modifications to the treatment platform. “…the communication skill is more to personal development because it may be enhanced with more working experience…” (Participant 18, clinic, experienced)
The significance of clinical skills training was emphasized by the participants, as they recognized that patients who are well versed in technology may challenge their physiotherapists with information they have gathered online, making it imperative for healthcare professionals to stay current with the latest developments. “… at least we need to improve our knowledge about the condition. For example, if a client has knee osteoarthritis, we should be able to gain more knowledge about how to manage the pain so that the client will become satisfied…” (Participant 2, clinic, experienced)
However, a dissenting voice also exists. “… We already have musculoskeletal skills from college. We probably do not need any additional training…” (Participant 6, hospital, inexperienced)
Discussion
For telerehabilitation to achieve its full potential as an effective treatment option for musculoskeletal disorders, it is essential to understand its benefits, barriers, and recommendations from the perspective of physiotherapists. An earlier research explored the potential of telerehabilitation among musculoskeletal physiotherapists during the coronavirus pandemic in 2019, and discussed opportunities, barriers, and future directions of telerehabilitation. 7 Although the use of telerehabilitation for musculoskeletal disorders began in Australia in 2003, 48 research in Southeast Asia is limited and mostly quantitative.49–51 As a result, there is a knowledge gap in firsthand accounts from users’ (physiotherapists’) perspectives on telerehabilitation.
According to the FGDs, participants expressed the belief that telerehabilitation could positively impact both saving clients’ time and reducing costs. This finding aligns with a survey conducted among physiotherapists in Sri Lanka, wherein telerehabilitation could save time and costs for clients with knee osteoarthritis. 15 These findings are consistent with those of an earlier quantitative study, which also revealed that most speech-language therapists in the survey agreed that telerehabilitation could save clients time and money on travel. 16 The participants also expressed another benefit: that clients would perceive telerehabilitation as a convenient option. A qualitative study examining a home-based stroke telerehabilitation system reported unanimous agreement among participants that telerehabilitation was more convenient than traveling to health facilities. 52
In light of these positive perceptions, concerns regarding technical obstacles to telerehabilitation are universal. Participants discussed instances in which their telerehabilitation sessions were interrupted by unstable Internet connections. Similar to the research conducted,21–23 the present study echoed these concerns, with participants emphasizing limited technological resources, such as webcams and insufficient space. These findings are consistent with those of previous research, highlighting the lack of available space, inadequate technological infrastructure, and limited access to technical support within healthcare facilities owing to resource constraints. 14
Furthermore, the participants in this study identified poor technological literacy as a barrier, which aligns with the findings of previous research, 20 and researchers highlighted computer literacy as the primary obstacle to virtual healthcare delivery. Despite some participants having prior experience with telerehabilitation in the study, concerns were raised regarding old people facing challenges in adapting to telerehabilitation. A qualitative study revealed that veterans’ acceptance of telerehabilitation was closely linked to their regular smartphone use. 53 Furthermore, the research team reported that participants in their study who had little to no experience with technology displayed high acceptability and enthusiasm in mastering telerehabilitation, 54 indicating that age is not the primary factor determining poor technological literacy. A study conducted in Italy reported that technological literacy is related to age. However, participants found that the technology was easy and comfortable after training. 55 Participants in the study, irrespective of their experience with telerehabilitation, expressed concerns about communication challenges that may arise during telerehabilitation. Communication plays a vital role in healthcare. We find this point to be very important because many studies have argued that telerehabilitation may lead to communication challenges. 56 Consistent with previous research involving seven nurses working in telerehabilitation in Brazil, difficulties in perceiving clients’ nonverbal signals have been cited as reasons for stricter interactions. 57 In contrast, a group of healthcare providers with telerehabilitation experience emphasized that communication skills developed after they gained experience in the field. 58 Participants were satisfied with the video calls and messaging apps for communication, indicating that telerehabilitation could be promoted in the public health system and expanded. 56 Through the implementation of telerehabilitation, healthcare providers will shift their focus toward utilizing visual cues to compensate for the absence of nonverbal cues, such as physical touch. This shift in focus has the potential to foster the development of a strong clinician–patient relationship. 59 Musculoskeletal care relies not only on physical contact during client visits but also on the use of signs and nonverbal communication. This in turn has been found to enhance the quality of telerehabilitation by conveying a sense of care and attention. 7 However, the reliance on visual cues in telerehabilitation may not fully address the need for nonverbal communication and physical interaction between healthcare providers and patients. It is crucial to recognize these barriers identified by participants in the study, which include the inability of telerehabilitation to offer hands-on intervention. This finding aligns with previous findings, such as clinicians perceiving the inability to physically assess muscle strength as a barrier. 60 A survey conducted among psychiatrists in the Philippines revealed that 98.1% expressed concerns about the limited examination capabilities of telerehabilitation. 61 Similarly, more than 40% of occupational therapists identified a lack of physical contact as a primary barrier in telerehabilitation, posing safety concerns for clients. 62 Concerns related to limited physical touch extend across multiple disciplines and are not confined to the field of physiotherapy.
Comprehensive and tailored training play a crucial role in maximizing the potential for successful implementation.63, 64 This research highlights the urgent need for training in communication skills and digital health proficiency, particularly focusing on developing competencies in general digital technology use and addressing health problems from electronic sources. 65 To enhance the successful implementation of telerehabilitation, undergraduate programs should incorporate the training process into their curriculum. 66 Previous literature suggests that a massive open online course could effectively meet the needs of both physiotherapists 67 and students. 68 Additionally, the need for specific training and practice in providing telerehabilitation care has been emphasized, indicating that healthcare providers, including physical therapists, may require tailored training to effectively deliver telerehabilitation services. 69 Concerns have also been raised regarding the adoption of telerehabilitation models, including changes in work roles, hidden work practices, and fears of insufficient support with technology, which all underscore the need for comprehensive training programs to address these challenges. 64
Strengths and limitations
The strength of this study is that it employed a qualitative approach. FGDs provide a diverse spectrum of perceptions by incorporating physiotherapists with prior experience with telerehabilitation and those who are inexperienced with the concept, as well as from individuals at different stages of their careers. In comparison to face-to-face FGDs, FGD researchers have circumvented geographical limitations that increase the diversity and quality of the data obtained. Another strength of the study is methodological rigor, in which all transcripts were shared with the participants for review and correction. Thus, selection bias may have been introduced. Individuals who are more comfortable with technology may be overrepresented, potentially excluding those facing technological barriers. This limitation raises concerns regarding the generalizability of the findings. Another limitation of the study is the potential for certain participants to exhibit a bias toward providing more input to a particular question, while others have a lower level of participation. This may have resulted in an uneven contribution to the findings.
Conclusion
This research contributes crucial knowledge to an emerging area of interest in Malaysia telerehabilitation. The findings revealed a greater prevalence of barriers to enablers among Malaysian physiotherapists, potentially influenced by varying levels of experience. Despite the prevailing inexperience in telerehabilitation observed in this participant pool, this research underscores the importance of understanding the barriers and enablers identified by physiotherapists. This research revealed that there are some recommendations from physiotherapists for establishing telerehabilitation practices. By confirming the key themes in the research, comprehensive insights gathered from this research can provide physiotherapists with direction when implementing telerehabilitation. The findings suggest that future telerehabilitation implementation should consider active involvement and engagement across stakeholders, encompassing diverse sectors such as information technology, healthcare policy, and administration and clients. The interplay between stakeholders in various sectors is valuable.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241248916 - Supplemental material for Exploring physiotherapists’ perceptions of telerehabilitation for musculoskeletal disorders: Insights from focus groups
Supplemental material, sj-docx-1-dhj-10.1177_20552076241248916 for Exploring physiotherapists’ perceptions of telerehabilitation for musculoskeletal disorders: Insights from focus groups by Lee Lee Sia, Shobha Sharma, Saravana Kumar and Devinder Kaur Ajit Singh in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241248916 - Supplemental material for Exploring physiotherapists’ perceptions of telerehabilitation for musculoskeletal disorders: Insights from focus groups
Supplemental material, sj-docx-2-dhj-10.1177_20552076241248916 for Exploring physiotherapists’ perceptions of telerehabilitation for musculoskeletal disorders: Insights from focus groups by Lee Lee Sia, Shobha Sharma, Saravana Kumar and Devinder Kaur Ajit Singh in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors wish to thank Nurul Syuhada Mohd Rosnu for assisting in FGDs as well as all participating physiotherapists who shared their perceptions of during the discussion.
Contributorship
LLS, SS, and DKAS conceptualized the project. The study was designed by the LLS, SS, and DKAS. The data were collected by LLS. Formal analyses were performed by LLS, SS, and DKAS. The draft of the manuscript was prepared by LLS. SS, DKAS, and SK reviewed the manuscript. All authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Research Ethics Committee of Universiti Kebangsaan Malaysia (UKM PPl/111/8/JEP-2021–830) and NMRR (NMRR ID-21-01970-Q2S (IIR).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
SS.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.