
Abstract
Keywords
Background and significance
The Electronic Medical Record (EMR), as well as the expanding Health Information Technology (HIT) industry, have been touted to make healthcare safer and more efficient, leading to improved health outcomes.1–3 Given the complexity of integrating HIT into a healthcare organization, many systems utilize a leader to drive such changes, often called the Chief Medical Information Officer (CMIO). 4 Additionally, other healthcare personnel have been influential in adopting healthcare information technology such as the Chief Nursing Informatics Officer (CNIO), Chief Pharmacy Informatics Officer, and Chief Dental Informatics Officer.
The title of CMIO evolved as healthcare organizations realized the value of clinical information systems in the delivery of healthcare. 5 Although it was not until the 1990s that the term “CMIO” started to become popular, 6 this leadership position has its roots dating back to the 1960s 6 and has evolved over time based on the growth of technology and healthcare needs. CMIOs were previously known as Associate Chiefs of Staff for Clinical Information Management, Medical Directors of Information Technology Services, Directors of Medical Informatics, and Directors of Clinical Information Technology. 7 They are often physicians whose primary aim is to bridge information systems and clinical medicine, a role that is complementary to the Chief Informatics Officer (CIO). 8 Their role is not only to ensure successful information technology (IT) implementations, but also have essential skills in problem-solving, quality improvement in patient care, assessing interests, engaging in informal politics, and innovation and change management. 9 And as a result, the role of a CMIO spans across multiple disciplines from administration, IT, and the clinical arena and often is seen as an interpreter between the technology and clinical worlds 10
CMIOs analyze, design, develop, implement, and evaluate information and communication systems with the intent of achieving individual and population health goals, enhancing patient care, and strengthening the clinician-patient relationships.7,11 Given the widespread functions of CMIOs, it is not unexpected that other names have been used synonymously for the CMIO which include Chief Health Informatics Officer, Chief Clinical Informatics Officer (CCIO), Medical Director of Informatics, Chief Medical Innovation Officer, Chief Innovation Officer, and Chief Health/Digital Officer.4,7,12,13
Key pieces of legislation and events that occurred since the late 2000s have further necessitated the role of the CMIO across many healthcare organizations. First, the Health Information Technology for Economic and Clinical Health Act (HITECH) was passed as part of the American Recovery and Reinvestment Act of 2009. 14 This legislation allocated 29 billion US dollars in funding to support widespread EMR adoption and tracking of quality metrics for incentive payments. 15 As a result of these new regulations, 96% of hospitals by the year 2021 (16) adopted the use of an EMR further justifying the need for CMIOs , 17. Second, the 21st Century Cures Act was passed in 2016 to promote the access, exchange, and use of electronic health information by patients via modern computing standards such as application programming interfaces (APIs). 16 This law, among other things, has encouraged the development of the patient portal which has enabled six out of every 10 patients to access their health information online. 17 Finally, the COVID-19 pandemic saw a 154% increase in telemedicine use. 18 These significant changes likely required extensive oversight by informatics leaders across the country including CMIOs, CNIOs, CCIOs, and others.
In addition to legislative initiatives, in 2011 Clinical Informatics was recognized by the American Board of Medical specialties as a subspecialty.19,20 Subsequently in 2014, the first fellowship programs were accredited by the Accreditation Council on Graduate Medical Education (ACGME). 21 The Clinical informatics fellowship can be seen as a structured pathway to a career in clinical informatics. Prior to the establishment of fellowship programs, many pioneers in the field were able to obtain board certification through the practice pathway. In addition, combined clinical informatics programs have been created to encourage clinical informatics training. 22
Given these combined factors of legislative mandates, adoption of technology, and increased educational opportunities, we hypothesized that the role of the CMIO has transitioned from EMR implementers to data analyzers and integrators of new technology for improving population health and clinical workflows. To study our hypothesis, we conducted a survey from CMIOs, Chief Health Information Officers (CHIO), and Medical Directors of Informatics which evaluated their current roles as healthcare informatics leaders. The primary objective of this study was to identify the past and current roles and responsibilities of the CMIO. The secondary outcome was to identify future trends in CMIO responsibilities and roles.
Methods
Ethics approval
This study was approved by the Institutional Review Board (IRB) (IRB ID: STUDY00005531) at the University of Buffalo. The survey questions were developed by the authors of the study. A structured survey of 13 questions pertaining to the role of healthcare informatics leaders and EMR systems was developed (Appendix A). Specifically, survey questions focused on their education, training, and years in informatics, time involved in the current role, present responsibilities, and their perspectives on future trends as healthcare informatics leaders.
Survey design
The present study had a prospective survey based observational design. It was partially blinded because the researchers could not individually link the results to any specific participant. The survey was administered prospectively and used both quantitative and qualitative methods to assess responses. For face validity, the survey instrument was reviewed by fellows and faculty physicians in the clinical informatics department at our institution. No copyright was obtained because the questionnaire was created by the authors. All survey responses were included in the analysis if the informed consent was completed. The software prompted the survey respondent to consent before beginning the survey. The software did not allow participants to begin the survey if informed consent was not obtained. Surveys were excluded if no consent was obtained. The survey questions were in a mixed-method style which included open layout questions for written responses (Appendix A). The survey questions were sent to targeted informatics groups that many health informatics leaders are members of within the United States. Using a listserv of known healthcare informatics leaders from physician informatics groups within the American Medical Informatics Association (AMIA) and Association of Medical Directors of Information Systems (AMDIS), a thirteen-question survey was emailed to all recipients and data was collected via SurveyMonkey. For additional survey outreach, contact emails were gathered manually through internet searches, research papers, downloaded from informatics organizations’ listservs, or scraped utilizing an internet browser extension that collects publicly available contact information from LinkedIn.The email invitation sent to potential respondents included a request to complete an informed consent and a link to complete the anonymous electronic version of the survey distributed via Survey Monkey. The survey was sent by the listserv moderator. The authors did not have knowledge or access to the names of the participants solicited through the listserv.
The authors were informed by the moderator of the listserv that some of the 4000 members’ email addresses were not current and of those only 300-400 members actually participated in the listserv. Additional CMIO contact information was gathered from the internet. An informed consent statement preceded the survey instrument. Participation in the survey responses was voluntary, free, and anonymous. The responses were aggregated by survey monkey and no identifiers were linked to the survey responses.
Statistical analysis
After the survey was inactivated, the responses were downloaded into a Microsoft Excel spreadsheet for review and analysis. The participant responses and survey answers were grouped based on response categories. General descriptive statistics were used to calculate averages between groups and sub-groups. No inter-group comparisons or inferential statistics were used to compare groups. The response percentages were rounded to the nearest whole number.
Results
There were a total of 612 survey recipients and 85 responded (14% response rate). Eighty-three of the respondents identified their current title at their healthcare organization (Figure 1). Fifty-five percent reported that their current title was CMIO, while “Other” was the second most common option selected (33%). Eight out of the 27 who responded “Other” reported their role as the Associate CMIO, which combined with CMIO, represented 65% of the total participants. The least reported title was CMIO/CIO (2%). Current titles of participants in leadership roles in healthcare informatics. Abbreviations: CMIO = chief medical informatics officer, CHIO = Chief health informatics officer, CIO = Chief informatics officer.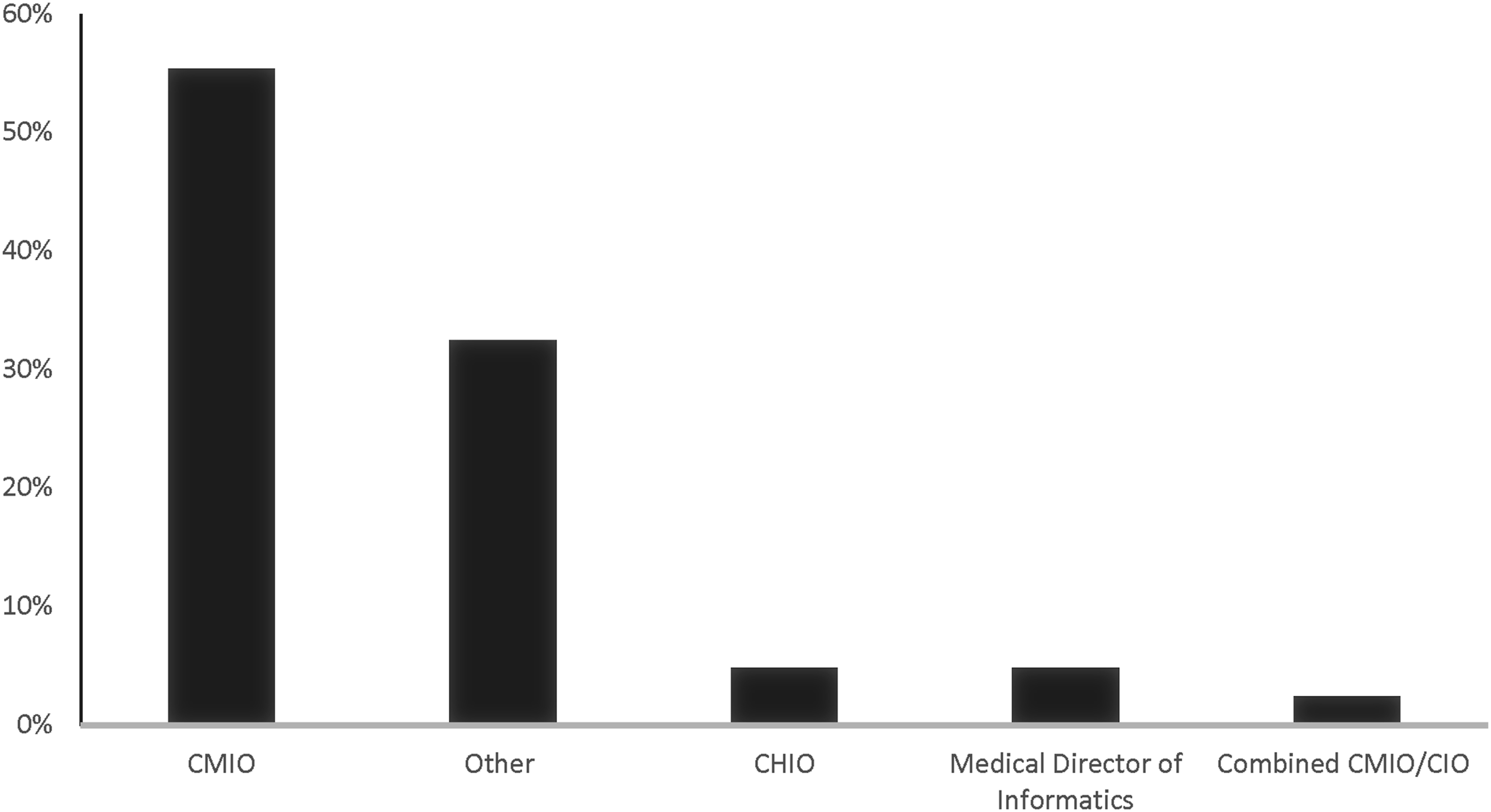
The majority of the participants had been in their current role for 0-5 years representing (41%). The participants who identified having held their leadership position for 6-10 years was the next leading response, representing 33% where 26 of the 80 participants responded to the question while the third and fourth positions were 11-15 years and 15 and more, respectively (Figure 2). Years in current position as a healthcare informatic leader.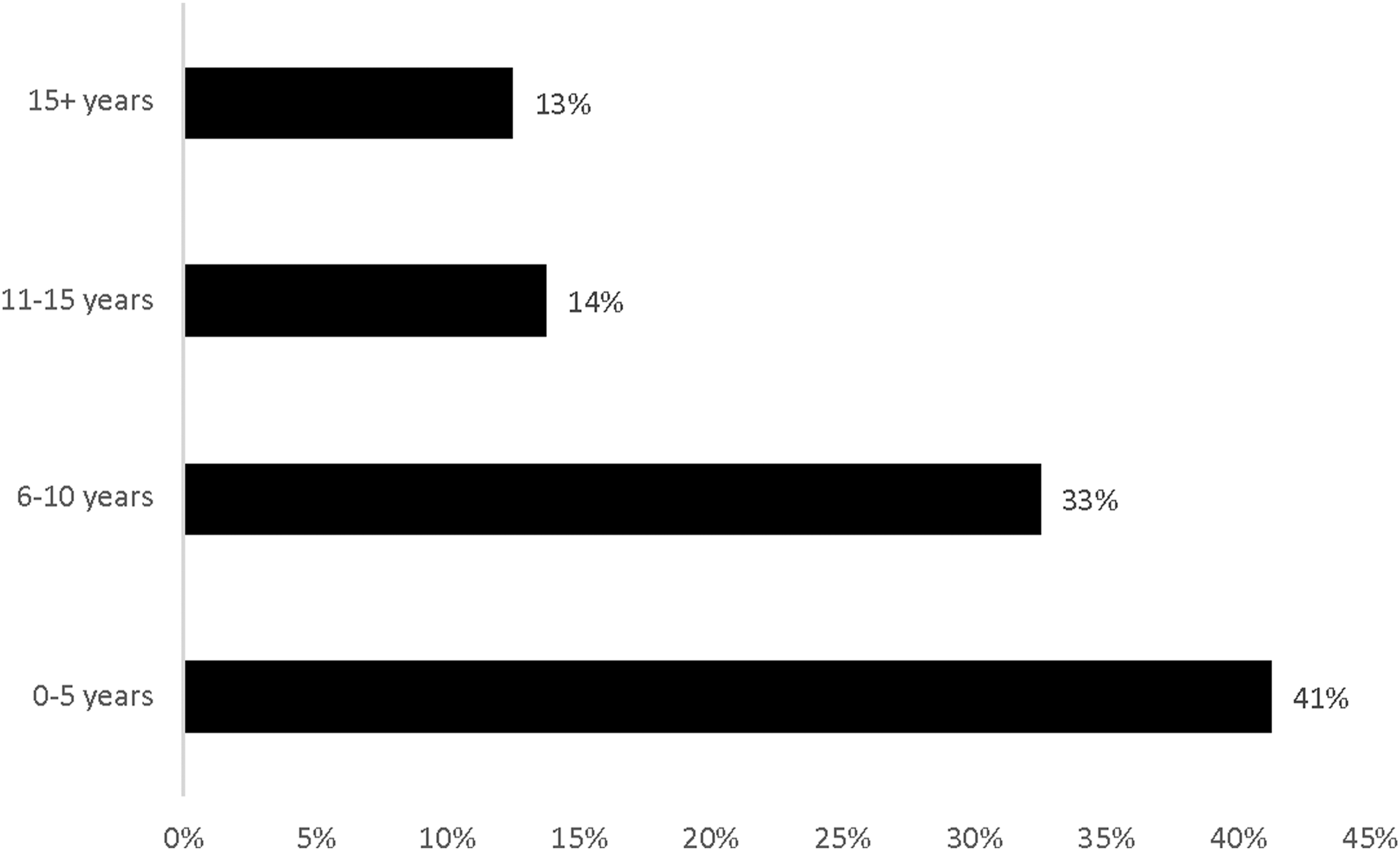
When asked about the time dedicated to health informatics leadership, the participants gave varied responses. Forty-six percent of the participants had a total of one full-time equivalent (FTE) dedicated to their leadership role in healthcare informatics. Twenty-eight percent had total time dedicated to their leadership role in informatics ranging from .25 to .75 FTE. The participants that answered “other” had a wide range of times dedicated to informatics; five out of 77 respondents reported a 0.8 FTE and another five reported 0.9 FTE for their dedicated time to informatics representing 13% of respondents.
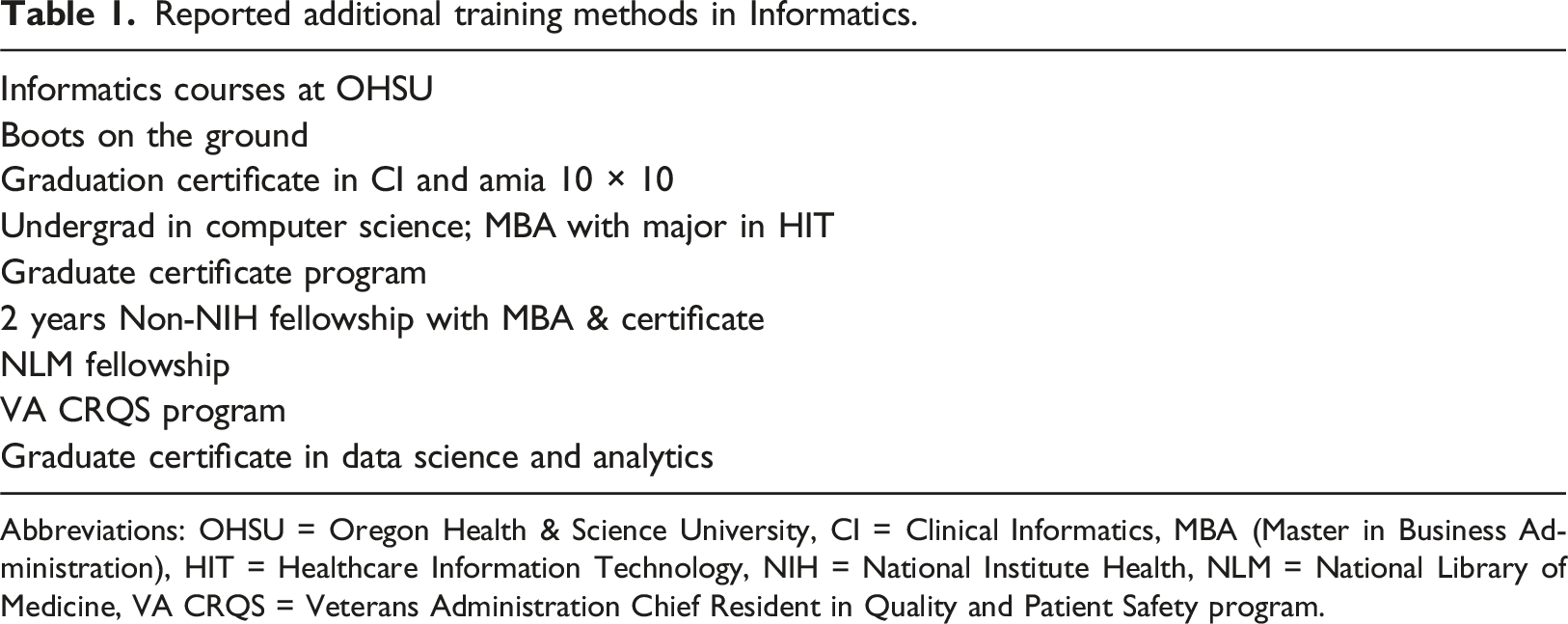
Approximately 53% of participants reported having no formal training in informatics but were board-certified in Clinical Informatics while 27% had formal training and were board-certified. Of the participants that responded yes to formal training, 30% reported completing a clinical informatics fellowship (Figure 3). Completing both a Master’s program in informatics and “Other” had an equal response rate of 27%, respectively. In the “Other” category the listed methods of obtaining training in informatics stated by the participants include informatics courses at Oregon Health & Science University (OHSU), “boots on the ground”, graduation certificate in Clinical Informatics and American Medical Informatics Association (AMIA) 10 × 10, undergrade degree in computer science, obtaining a Master in Business Administration (MBA) degree majoring in HIT, graduate certificate program, 2-years non-National Institute Health (NIH) fellowship with MBA & certificate, National Library of Medicine (NLM) fellowship, Veterans Administration Chief Resident in Quality and Patient Safety program (VA CRQS) program and a graduate certificate in data science and analytics (Table 1). The types of training participants completed in Informatics. Abbreviations: AMIA = American Medical Informatics Association. Reported additional training methods in Informatics. Abbreviations: OHSU = Oregon Health & Science University, CI = Clinical Informatics, MBA (Master in Business Administration), HIT = Healthcare Information Technology, NIH = National Institute Health, NLM = National Library of Medicine, VA CRQS = Veterans Administration Chief Resident in Quality and Patient Safety program.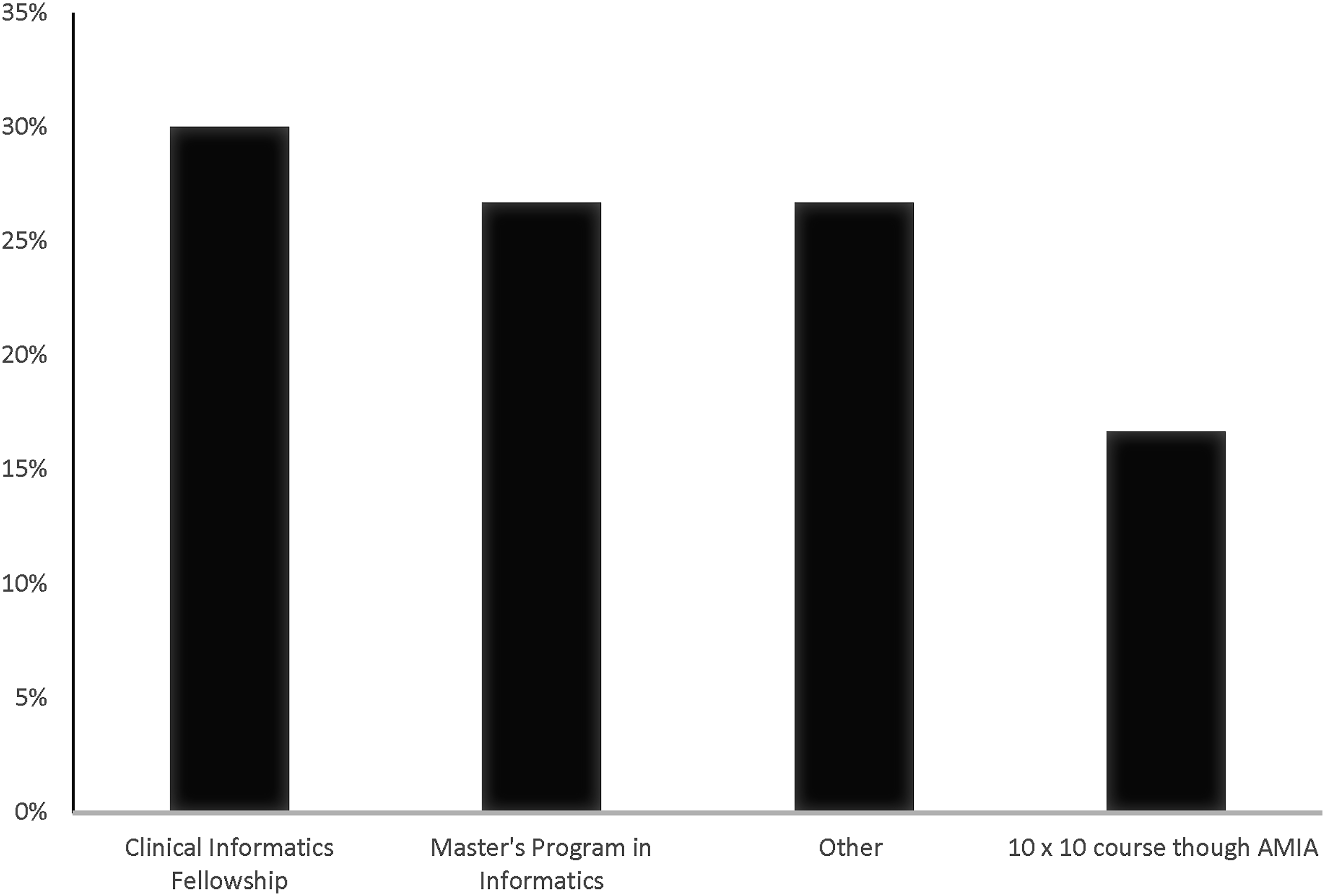
Of the medical specialties that responded to the survey as healthcare informatics leaders, Internal Medicine represented 47% and other as 42%. The additional medical specialties represented included Neurology, Psychiatry, Neurology, Otolaryngology, Emergency medicine, Internal Medicine, and Pediatrics Allergy/Immunology. The type of facility where the participants worked was more likely to be not-for-profit (63%), large hospital centers with more than 500 beds (48%), and a teaching hospital (64%).
When questioned on how their job roles have changed since assuming an informatics leadership position, the following responsibilities were mentioned in decreasing order: use of EMR to improve patient outcome and efficiency (62%), overseeing compliance with federal and state regulations regarding the hospital’s EMR (53%), design and customization of information technology systems (49%), quality improvement management (47%), healthcare data analytics (machine learning and artificial intelligence (47%), population health management (43%) (Figure 4). Participants were asked to select responsibilities that they are currently performing but were not part of their original job duties. Described changes in responsibilities and roles by Health Informatics Leader since starting in current position. Abbreviations: IT = Information Technology.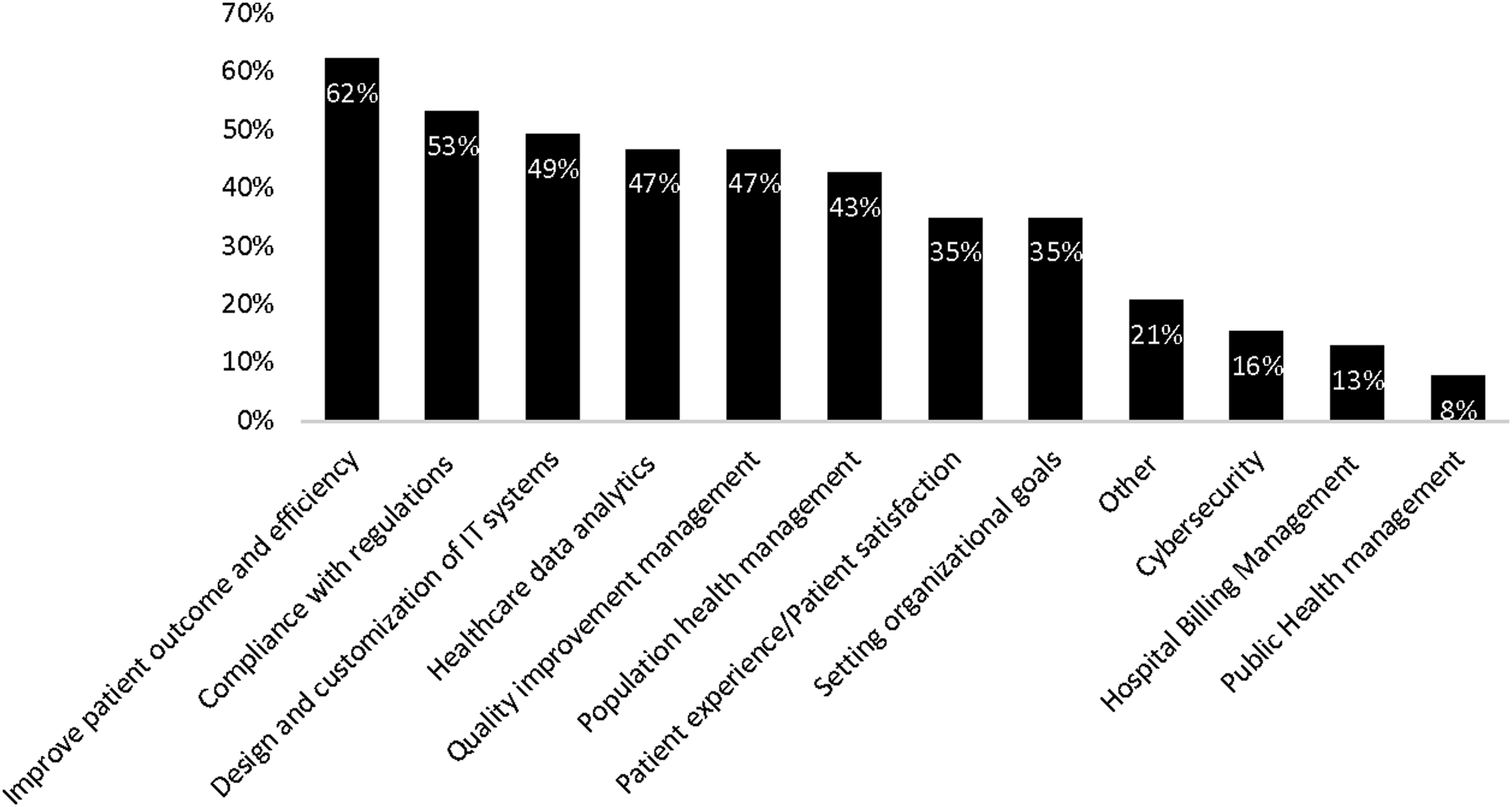
In regards to how they foresee their role changing in the future, increased healthcare data analytics responsibility was 67%, increased use of EMR to improve patient outcome and efficiency responsibility was 62%, increased population health management responsibility was 47%, increased quality improvement management responsibility 43%, and increased responsibility for setting organizational goals was 39% (Figure 5). Participants’ anticipated changes of their healthcare informatics responsibilities.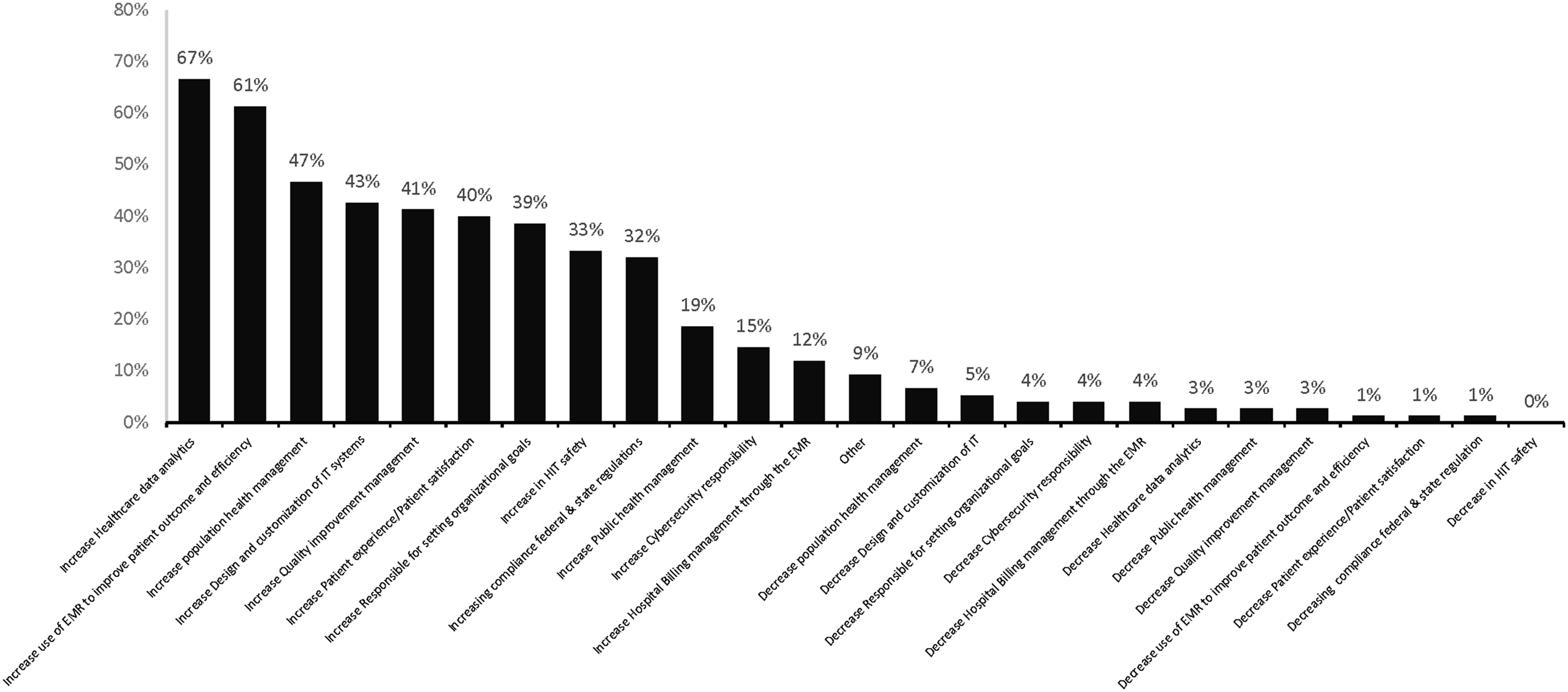
During the COVID-19 pandemic, participants reported the addition of the following roles and responsibilities: implementation of telehealth applications (54%), increased operational responsibilities (35%), and increased reporting to state and federal agencies (32%) (Figure 6). The participants that responded as other, reported the increased use of clinical data for research, development of COVID-19 pandemic charting for nursing, and increased reporting to their local public health authority. Participants’ experiences on how COVID-19 influenced their responsibilities.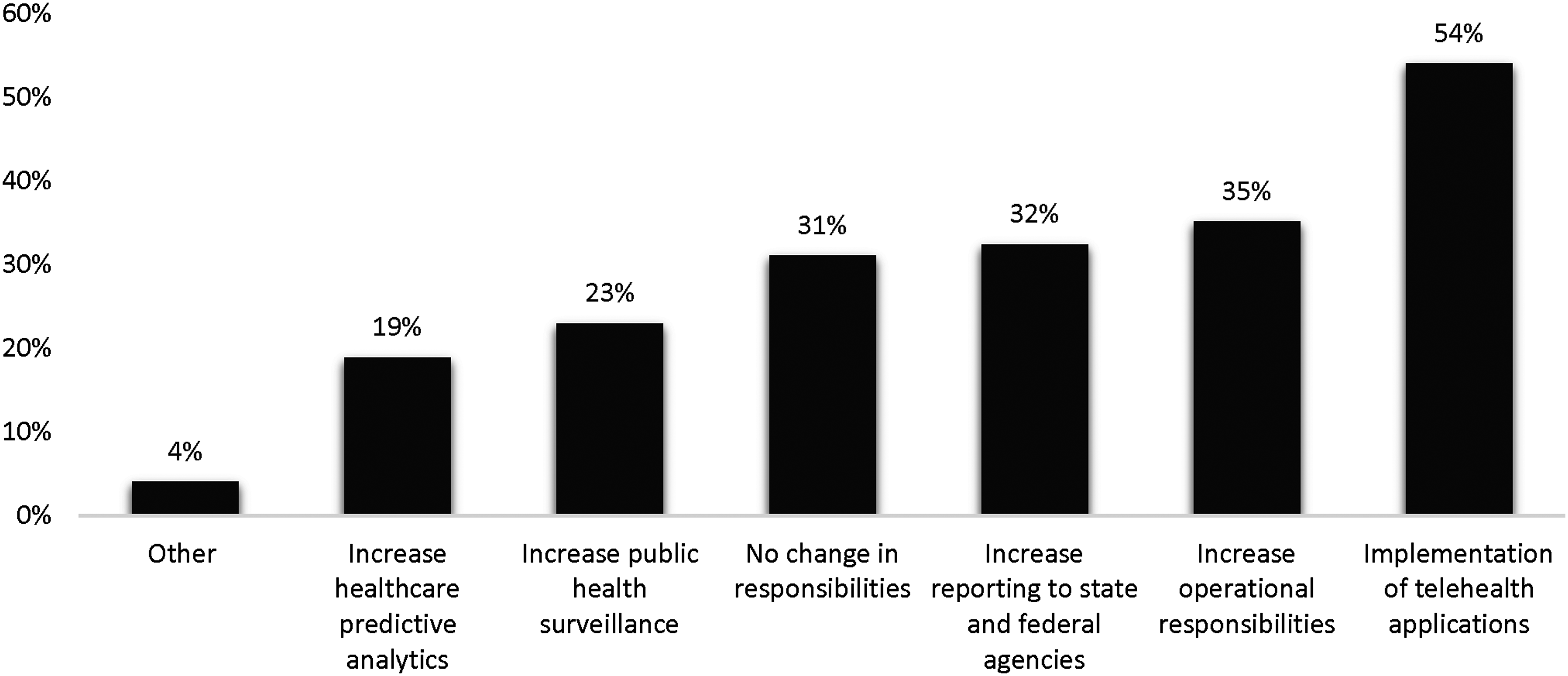
Discussion
The objective of this study was to assess the current role and responsibilities of healthcare informatics leaders and to gain insight into what their potential future responsibilities and roles could be. The participants in the survey did anticipate changes to their role and responsibilities. The survey responses from participants indicated the following additional changes were foreseen to have an impact on their future responsibilities: quality improvement management responsibilities, patient experience/patient satisfaction responsibilities, and responsible for setting organizational goals. Of the participants surveyed, it was noted that they had varied responsibilities and roles and different training background in clinical informatics. With the advent of accredited fellowship programs in clinical informatics, it is very likely that this varied and broad training will become more standardized in future healthcare informatics physician leaders.
The physician healthcare informatics leader positions are relatively new, but beneficial, to healthcare organizations to ensure clinical information technology is successfully implemented. The role and responsibilities have changed since its inception requiring the informatics leaders to expand their knowledge and skill set. For this survey, most of the positions were held by CMIOs and Associate CMIOs (66%). AMDIS and WittKieffer have conducted similar surveys in 2014, 2018, and 2021 where they investigated the CMIO role and compensation. 12 Specifically, Chief Medical Information Officer and Physician IT Executives at AMDIS were surveyed. In the 2021 survey, 42% of respondents reported being in their current position for less than 3 years 38% between four-seven years, and 20% over 8 years. 12 In our study, 74% of respondents reported having been in their position between 0 and 10 years. Healthcare informatics leadership positions have been established for over 20 years, however, currently 13% of the individuals surveyed have held their position for over 15 years. A significant portion of the participants responded that their position was 1.0 FTE (47%), while the “other” response was the next most common in which these participants spent 0.8-0.9 FTE on informatics (13%). This indicates that a significant majority (60%) spend at least 80% of their time overseeing healthcare informatics at their organization. The AMDIS and WittKieffer survey respondents reported they spent 55% or less on clinical work while 28% reported currently not active in clinical work which sums to 82% of respondents dedicating majority of their time to informatics. 12 This is similar to our results where 80% reported their time was dedicated to overseeing healthcare informatics.
Many of the participants that were surveyed were board certified (79%). The board certification process began in 2013 and allows for a physician to be certified without a fellowship via a “practice pathway”. 23 Despite this career development opportunity, some have not become board certified (21%). The practice pathway requires 3 years in clinical informatics practice with a minimum of at least 0.25 of FTE in healthcare informatics. 24 In the AMDIS and WittKieffer survey, 72% of participants responded as no formal informatics training which is greater than our study where the participants responded 53% had no formal training. Our survey differs from the AMDIS and WittKieffer survey since it focused on compensation trends and not the evolution of their responsibilities.
Currently, there is sparse literature on the CMIO and healthcare informatics leaders evolving responsibilities which have been influenced by emerging new healthcare information technology. From technology changing at a rapid pace to patients having more access to their health records and growing use of health information technology, the role of health informatics leaders will most likely continue to evolve. It is highly likely that as artificial intelligence continues to flourish and make inwards into the healthcare sector, this evolution of healthcare informatics physicians will concomitantly and exponentially flourish l and morph into more of digital healthcare leaders.
The role of CMIO emerged as healthcare information technology began to integrate into the healthcare organization. The current roles and responsibilities align with the diversity of responsibilities that different healthcare informatics leaders have at a healthcare organization. Many respondents indicated they foresee their future job responsibilities to include analyzing healthcare data, increasing the use of EMR to improve patient outcomes and efficiency, and increasing responsibility in population health.
Limitations
We acknowledge that there are some limitations to our survey. Our survey was limited by the inability to assess the exact sample size. No precise method could be used to assess the scope of how many surveys reached participants. The listserv utilized could not provide an exact number of recipients who received the email invite. They only provided an approximate number of active members part of their listserv. In addition, many of the emails sent to known healthcare leaders in informatics were invalid and received an undeliverable response. Despite efforts to create a survey to ensure all questions were answered within the survey platform, many participants were able to skip questions. Because the number of respondents who chose to respond to questions differed from those who chose not to respond, this could potentially create bias in the data. The questions on roles and duties were in multiple choice format which may have swayed the respondent to answer in a certain way. Additionally, more questions could have focused on data analytics and artificial intelligence as this is a growing field. The survey we created targeted a specific sector of healthcare informatics leaders which may decrease its generalizability and not represent all the changes that other healthcare informatics leaders have experienced. A descriptive non-validated survey was created by the authors of present study, also the survey was not piloted. Using a non-piloted non-validated survey our study could have a measurement error and any conclusions drawn from it should be interpreted within that context. 25 Finally, participants may have interpreted the survey questions and answers differently leading to unclear data results.
Conclusion
The role of CMIO and healthcare informatics leaders have begun to be distinctly delineated, and their positions have had a tremendous impact on the integration of health information technology in healthcare. The role of CMIO will continue to evolve as technology changes. The positions have migrated from an implementation and change management of HIT into a diverse set of skills which includes being a clinical strategist and optimizer of HIT, and a critical contributor to the strategic planning of HIT initiatives. These skills will be fundamental for assessing new HIT, improving healthcare data exchange, improving patient care and outcomes, and improving physician efficiency and workflow through HIT. Healthcare informatics leaders will be the steward of progress concerning HIT in the healthcare settings. The requirement to understand healthcare data within EHRs will continue to mature. Additionally, different leadership roles within healthcare informatics have expanded outside of CMIO such as the new roles of Chief Nursing Informatics Officer and Chief Digital Officer. As more healthcare informatics leaders complete advanced training in clinical informatics, programs must adapt to the expanding skills these future leaders must understand. These leaders will need to be fluent not only in technology and healthcare but also be versed in healthcare data analytics, change management, population health, and quality improvement as many of the survey respondents have indicated. These roles will require strategic adoption of healthcare IT to ensure the new technology aligns with the needs of their healthcare organization. As technology changes and advances, how it will be used in healthcare will need to be evaluated and planned by physician Healthcare Informatics Leaders.
Supplemental Material
Supplemental Material - Evolutionary role of physician leaders in healthcare informatics and health technology
Supplemental Material for Evolutionary role of physician leaders in healthcare informatics and health technology by Kendria Hall, Geoffrey Bocobo, Randeep Badwal and Mandip Panesar in Health Informatics Journal
Footnotes
Acknowledgements
We would like to express our gratitude to the staff of the Erie County Medical Center and the Department of Biomedical Informatics at the State University of New York at the University for all their support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the IRB at the State University of New York at the University at Buffalo. The study is registered as STUDY00005531 with University at Buffalo’s IRB. All study participants completed a required consent form before completing the survey. Given the nature of the utilized data, there is no cause for concern regarding ethical considerations in this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.