
Abstract
The use of multiple drugs by patients increases the risk of medical problems. Clinical decision support could assist general practitioners with prescribing but is underused. This article aims to investigate the attitudes of general practitioners towards using decision support systems. A survey was distributed among 500 Dutch general practitioners. Virtually all 184 respondents indicated having a clinical information system, while only 21 percent indicated having a decision support plug-in; this correlated with their use of medical formularies. Only use of one of the medical formularies correlated with the number of recognized underprescription problems. General practitioners’ attitudes toward a newly proposed system aiding them with polypharmacy prescribing were mainly positive (57%); the perceived usefulness correlated with output quality (p = .000), time investment (p = .000), and financial stimuli (payability: p = .000 and reimbursement: p = .015) but not with job relevance. Dutch general practitioners are thus likely to adopt the proposed system under the conditions that it improves prescription quality and does not require extensive investments of time or money.
Keywords
Introduction
In the past decade, the development of decision support systems for the primary health-care sector has greatly increased. Whether or not integrated with electronic medical records, computerized physician order entry (CPOE) systems have provided general practitioners (GPs) with appropriate tools to facilitate their drug prescribing. By incorporating medical formularies, drug interaction databases, clinical guidelines, and best practices, decision support systems can potentially optimize prescription processes.1–4
Even though literature generally attributes prescribing quality improvement to decision support systems where applicable, their adoption by GPs is often lacking. 5 Pevnick et al. 6 report that GPs owning decision support systems use them for only one quarter of their prescribing. Additionally, McInnes et al. 7 add that while virtually all of their adopting respondents indicate using decision support tools for drug prescribing, only 20 percent of them actually employ them during consultations.
The primary care area of polypharmacy, occupied with the use of multiple medications by a patient, suffers from suboptimal prescribing. In the Netherlands alone, 17 percent of the chronically ill use more than five different drugs permanently; half of these patients are above 70 years of age. 8 This polypharmacy is associated with medical problems, including an increasing risk of adverse effects, underprescribing, overtreatment, and decreased drug adherence.9–16
Many of these problems are due to avoidable human errors GPs make during the prescribing process, including use of incomplete patient information, insufficient communication, and mistakes because of time pressure or carelessness.17,18
To counter these problems, the Prescribing Optimization Method (POM) was designed: a step-by-step method to aid GPs in optimizing drug prescribing. In tests, this method significantly improved their prescribing quality and relevance. 19 In order to fully enable the use of the method, the POM Platform (POMP) has been envisioned: a decision support knowledge system that facilitates the POM and is optimally incorporated into GPs’ systems and workflows.
Recognizing the aforementioned problems regarding technology adoption by GPs, it is essential to investigate these issues in the Dutch primary care sector, in order to incorporate the results in the realization phases. Therefore, the focus of this article is to explore these issues by assessing the current use of decision support systems and by examining GPs’ opinions toward potentially adopting an application assisting them with treating polypharmacy. The research question that will be investigated is the following: how are GPs in the Dutch primary care sector, based on their experiences with decision support systems and medical formularies, likely to respond to the introduction of a platform assisting them with optimizing polypharmacy?
Literature analysis
Clinical decision support systems
Clinical decision support systems in the primary care sector have the potential to improve the decision-making of GPs and pharmacists.1–4 In their extensive literature study, Kuperman et al. 1 conclude that in order to realize the benefits of these systems, context-specific implementation complexities have to be addressed; in their words, “there is not yet a ‘one-size-fits-all’ approach.” Other studies that have been undertaken specifically in the Dutch primary care sector show mixed results regarding the influence implemented decision support systems have. While Martens et al. 20 found no favorable effects for computerized messages reminding GPs to prescribe certain drugs, messages not to prescribe them “sometimes positively influence[d] the prescribing behaviour [sic] of GPs.” A study by Kuilboer et al. 21 showed that the system they tested “changed the manners in which the physicians monitored their patients and, to a lesser extent, their treatment behavior.”
Due to these developments, CPOE software in the primary care sector has increased in diversity in recent years. From systems that were mostly organizational in nature, they have been enhanced to facilitate consultation of electronic medical records and clinical decision support. 22
Software market diversity
Consequently, the Dutch software market of GPs’ CPOE systems is diverse. Up to 10 different systems are currently in use, all providing their own distinct features and tools in addition to the common patient record management facilities. 22 Some of these systems include their own digital prescription aids and decision support tools, while others do not. As a result, third-party developers have produced additional software that, integrated with their existing systems, assists GPs in prescribing drugs. The major plug-ins on the market are Prescriptor, which can communicate with most existing GPs’ CPOE systems, and NHGDoc, which currently has limited integration capabilities.23,24
POMP
The POMP has been envisioned as a software program that, integrated with these aforementioned CPOE systems, would add to GPs’ range of assistive tools. Through the decision support platform, GPs would be advised on how to prescribe in patient-specific cases; through a medication review structured by the Polypharmacy Optimization Method, they would determine actual use of drugs, identify superfluous ones, and detect untreated diseases. Advice provided by the system would be based on proven clinical interactions between drugs, compatibility of medicine with patients’ other diseases, and best practices extracted through knowledge management. The system would facilitate the execution of a medication review, and thus operate on-demand; it would not disturb GPs’ workflows by reacting to decisions made during general consultations.
While the POMP will take the form of a stand-alone software program, it will be fully integrated in existing systems as far as user interaction and data exchange are concerned. Through this means, the developers seek to avoid the production of a software product that is underused or performs suboptimally.
Technology adoption
The adoption of technology by potential users has been extensively studied and has led to the development of various predictive models, including the technology adoption model (TAM), TAM2, and unified theory of technology acceptance model (UTAUT).25–27 These models have not, however, performed equally well at predicting acceptance behavior for all kinds of user groups. Subsequently, the potential influence of various different aspects has been explored, and the models extended accordingly. Physicians, in general, and GPs, in particular, have been studied extensively, and elements as diverse as financial stimuli or psychological ownership have been proposed.28,29 The deviations from elements common in most models that were found in multiple studies regarding this particular group are elaborated upon in the following.
When applied to GPs, some theoretical elements common in technology acceptance models do not seem to be supported. Notwithstanding new research by Ketikidis et al. 30 suggesting otherwise, many studies show an application’s ease-of-use is of minor or no importance to their acceptance by GPs, even though in literature, this is usually considered a core element.31,32
In contrast, time reduction is mentioned by various authors as a highly relevant and influential factor regarding GPs’ technology adoption, while this is not an element commonly found in any of the models.28,32,33 In their study, Chismar and Wiley-Patton 31 tested the TAM2 model on a group of pediatricians and found that, of the inherent constructs, only output quality and job relevance were determinant factors that influenced the respondents’ adoption.
In their study on the low acceptance rates of prescription software, Boonstra et al. 28 tested the original TAM and concluded that its factors were of hardly noticeable influence, and that adoption was mainly affected by systems’ embedding in consultation processes, financial stimuli, policy decisions, and cultural boundaries instead.
Theoretical framework
Based on the main TAMs and the deviations common in the aforementioned literature findings, a theoretical model for testing the attitudes of GPs in the Dutch primary care sector was assembled. Figure 1 shows the model. The final use behavior is largely determined by users’ behavioral intention, elements common in the TAM, TAM2, and UTAUT models. The original TAM is included, but in this study, the perceived ease-of-use was disregarded, as it was found to be of no importance in a literature study by Yarbrough and Smith. 32 This leaves the factors influencing perceived usefulness, which was defined by Davis 25 as “the degree to which a person believes that using a particular system would enhance his or her job performance.” The two constructs included in TAM2 that were found to be influential by Chismar and Wiley-Patton, 31 job relevance and output quality, were incorporated.
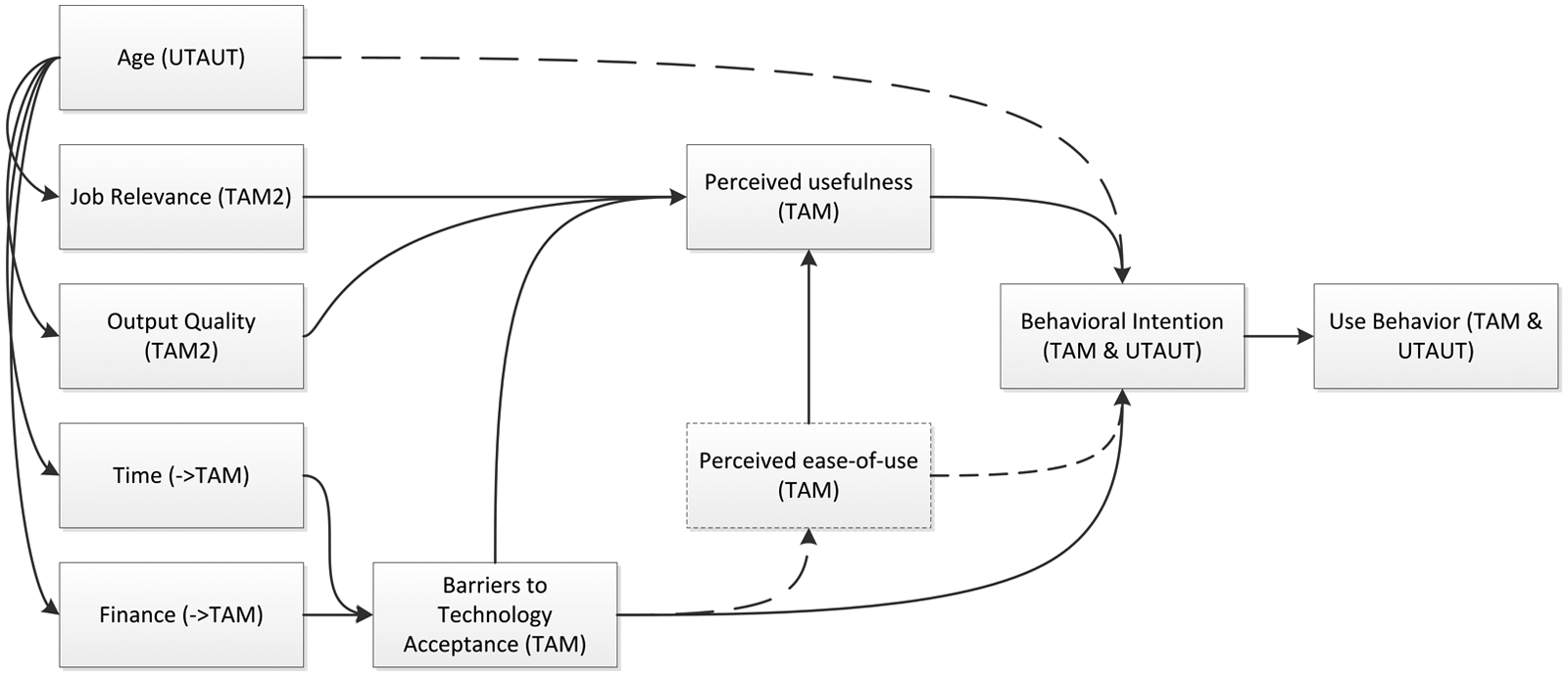
Model depicting factors influential to use behavior and their originating theories.
Apart from those, the elements of time and finance, often mentioned as highly influential in literature, were added to the model as barriers to technology acceptance, as proposed by Boonstra et al. 28 and Yarbrough and Smith. 32 Finally, the only construct considered to be influential in the UTAUT study by Venkatesh et al., 34 age, was included as well. In their study, Venkatesh et al. 34 related age directly to behavioral intention but stressed that it “is not a cause but likely a symptom” and that it requires further investigation. Therefore, in this study, the authors decided to test the influence of age on the other mediating factors rather than on behavioral intention itself.
Adoption models lead to an assessment of users’ final use of software. As the POMP under study in this research project is in its preliminary stages, its actual use cannot be assessed. However, in order to gain further insight into the acceptance of decision support systems by GPs in the Netherlands, existing products with conceptually related functionality that are currently in use were evaluated.
Hypotheses
The hypotheses that were tested in this study are listed below. As will be explained in more detail in the “Research Design” section, the hypotheses were tested for correlations, and thus, they do not contain causality implications. Therefore, the survey findings are discussed in the “Results” section, whereas the meaning of the data analysis will be elaborated on separately in the “Discussion” section.
Based on the consensus in the literature concerning the benefits of clinical information systems, the following hypotheses were assumed and tested:
H1: Use of one decision support system correlates with use of another.
H2: Ownership of a decision support system correlates with use of a medical formulary.
H3: Ownership of a decision support system correlates with use of number of medical formularies.
H4: Use of a decision support system correlates with use of a medical formulary.
H5: Use of a decision support system correlates with use of number of medical formularies.
H6: Use of a medical formulary correlates with recognition of occurrences of a problem associated with polypharmacy.
H7: Use of a medical formulary correlates with number of recognized problems associated with polypharmacy.
Following the model in Figure 1 on the aspects influential on behavioral intention, these hypotheses were formulated and tested:
H8: Number of patients correlates with perceived usefulness.
H9: Recognition of occurrences of a problem associated with polypharmacy correlates with perceived usefulness.
H10: Number of recognized occurrences of a problem associated with polypharmacy correlates with perceived usefulness.
H11: Importance attributed to output quality correlates with perceived usefulness.
H12: Importance attributed to time investment correlates with perceived usefulness.
H13: Willingness of financial investment correlates with perceived usefulness.
H14: Importance attributed to financial reimbursement correlates with perceived usefulness.
Finally, also according to the model in Figure 1, the influence of age on the various aspects was investigated through the following hypotheses:
H15: Age correlates with number of patients.
H16: Age correlates with recognition of occurrences of a problem associated with polypharmacy.
H17: Age correlates with number of recognized occurrences of a problem associated with polypharmacy.
H18: Age correlates with importance attributed to output quality.
H19: Age correlates with importance attributed to time investment.
H20: Age correlates with willingness of financial investment.
H21: Age correlates with importance attributed to financial reimbursement.
Research design
Method
A survey was deemed an appropriate method to examine potential users’ attitudes toward a system assisting them with polypharmacy prescribing. The fact that many potential users could be surveyed was a decisive factor.
First, the questionnaire (Appendix I) investigated demographic information, such as respondents’ ages and potential partnerships (Appendix 1). The next section was dedicated to surveying GPs on their current use of information systems and plug-ins and included questions about formularies and common problems. The last section started with a short explanation of the features the POMP would include, and investigated their opinions toward the newly proposed system. In this last section, only a conceptual idea of the POMP was provided, without specific details regarding its implementation or user interface.
To ensure an optimal response rate, the number of questions was kept to a minimum. Consequently, only a limited number of questions on technology adoption could be included. Consistent with the theoretical framework, questions regarding perceived ease-of-use were disregarded. The oft-mentioned time constraint was surveyed, as well as the perceived influence of financial stimuli. Specific questions on usefulness and output quality were included, but job relevance was not directly surveyed; the authors considered it unfeasible to ask about both relevance and usefulness, as the subtle difference could be lost in a questionnaire. Instead, the job relevance construct was divided over two questions: one asking about the number of polypharmacy patients each GP treated (phrased as “patients using five or more drugs”) and another on the problems they encountered with these patients.
The questionnaire limitations restricted the explicit inclusion of less often investigated aspects, such as cultural biases mentioned by Boonstra et al. 28 or psychological ownership proposed by Paré et al. 29 A comment section, however, was provided where respondents could fill out any additional remarks. The survey in its final form contained 15 questions.
The number of respondents necessary to generalize results was calculated with the “proportion sample” and “finite population correction” formulas provided by Israel, 35 which showed that 95 respondents were required to fill out the questionnaire. After taking into account an expected response rate of 20 percent, the survey was sent by postal mail to 500 practicing GPs, who were selected through a process of simple random sampling (i.e. each individual was chosen randomly and entirely by chance). The addresses were geographically spread across the Netherlands; addresses included more practices in the country’s more densely populated western provinces than elsewhere, but this can be explained by the fact that more GPs work there. A prepaid return envelope was included, giving respondents the opportunity to fill it out on paper or online. Ethical concerns described by Swanwick 36 were taken into consideration in the conduction of the survey. The responses were gathered anonymously, and the respondents were assured that their results would be treated confidentially. No coercion of any kind was used to persuade potential respondents to participate nor were any incentives provided in return for their answers. Responses were gathered during a period of 3 months, from mid-February to mid-May 2011. After this period, no additional responses were received. During or after this period, no attempts to increase the response rate were made.
Validity
The internal validity of most of the survey’s questions on technology adoption followed naturally from their close relations to the theoretical constructs. In cases where the constructs were divided over multiple questions (such as those on job relevance and financial stimuli), results were not combined into single values to avoid distortion of the concepts.
As the respondents were selected through a process of simple random sampling, this study’s findings are generalizable to the whole population of 8921 practicing GPs in the Dutch primary care sector, insofar as a confidence interval of 7.15 and a confidence level of 95 percent are maintained. As it turned out, multiple questions were answered unevenly. As the frequency of answers in contingency tables was often lower than five, Fisher’s exact test (FET) was favored over Pearson’s chi square test to test the hypotheses. 37 The setup of the study required the authors to test for correlations only. As correlation by itself does not imply causality, the influences in Figure 1 were not directly tested. The implication this restriction has for the results interpretation will be further elaborated upon in the “Discussion” section.
When testing a large number of hypotheses, the potential problem of multiple comparison analysis arises. This problem states that the probability of a tested result being significant by chance increases when testing multiple hypotheses. Different approaches to cope with this problem exist, but they are disputed; in their pursuit to minimize type 1 errors, they might erroneously introduce type 2 errors, that is, falsely accepting a false hypothesis.38,39 The techniques are most widely employed when two or more different samples are used. In this single-sample study, the Bonferroni–Holm correction technique was employed to check the results’ validity whenever subgroups’ correlations were tested. In order to avoid type 2 errors, however, these corrected p-values or significance levels are not incorporated into the results reported below; applying the Bonferroni–Holm correction ensured, however, that the hypotheses from which the main conclusions were drawn remained significant after correction.
Results
Research group
The survey was sent by mail to 500 practicing GPs, accompanied by a cover letter. Potential respondents were invited to either fill out the survey online or return their copy by mail. The vast majority (98%) chose for the latter option.
A total of 184 GPs returned filled-out questionnaires, which made a response rate of 37 percent. Of these respondents, only 15 percent were younger than 40 years; 27 percent were in their 40s, while 47 percent were in their 50s. Ten percent were 60 years or older, with only one respondent being above 65 years of age. Twenty-one percent of the respondents worked alone, 37 percent shared their practice with one colleague, but the majority of 42 percent worked with several others. All but one of the surveyed GPs reported having a professional information system; one was unsure.
Software market diversity
The earlier assumption regarding the diversity of the CPOE systems market was proven to be correct by the survey results. Two of the companies dominated the market, as they were used by 58 percent of the respondents (see Figure 2). Seven smaller manufacturers each had market shares between 1 and 12 percent. Twenty-nine percent of the respondents indicated owning Prescriptor, while 25 percent were unsure of that; the remainder indicated not owning the product. Fewer respondents (13%) owned the comparable decision support system NHGDoc, with an additional 26 percent being unsure.
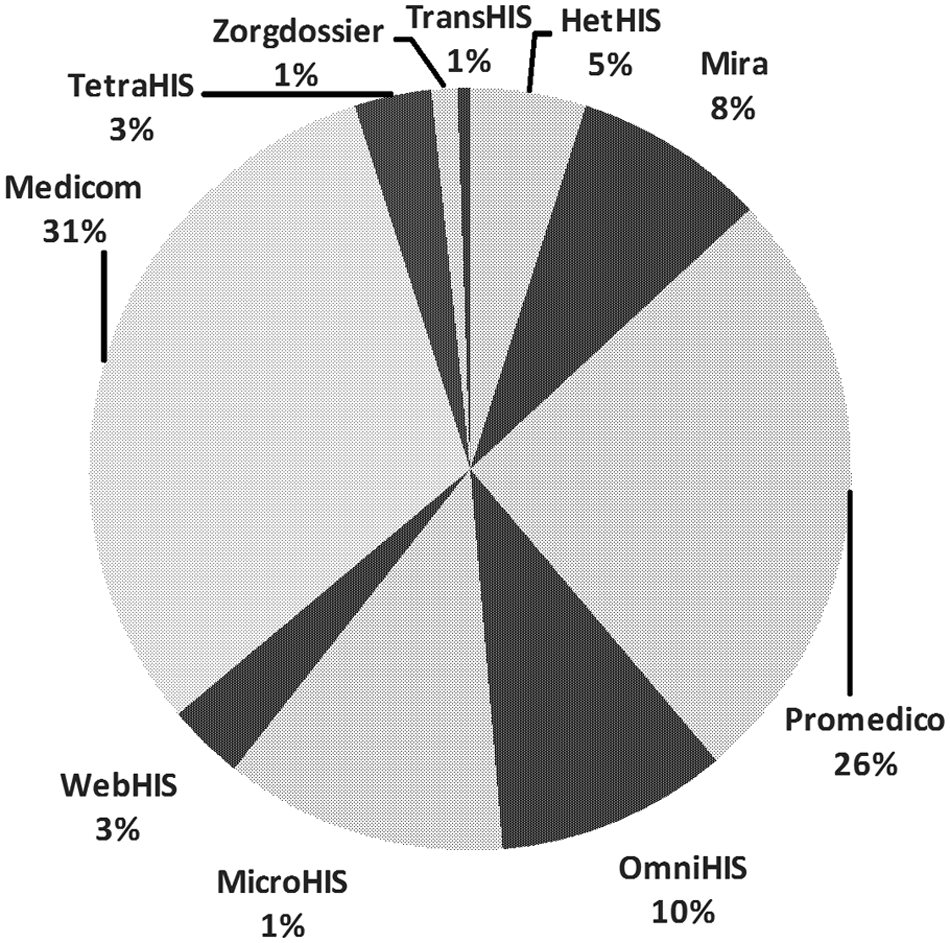
Model depicting the relative ownership of CPOE software by Dutch GPs.
Of the respondents indicating having one of these systems, the actual use differed. Of the owners of Prescriptor, the majority (55%) indicated using it never or rarely (less than once a week). Thirty-nine percent used it once or multiple times per consultation, with only 6 percent using it once per week. NHGDoc numbers were comparable: 54 percent used the software package rarely or never, 38 percent used it intensively, and 8 percent just once per week.
Decision support systems and medical formularies
Statistical analysis showed that owners using one decision support product (either Prescriptor or NHGDoc) are more likely to use the other one as well than GPs who do not (p = .002, FET); this led to acceptance of H1. The medical formularies, often integrated with GPs’ CPOE systems and facilitated by Prescriptor and NHGDoc, were widely used. Seventy-eight percent specified using the Pharmaceutical Compass, 38 percent used the guidelines by the Nederlands Huisartsen Genootschap (NHG; Dutch College of General Practitioners) and 13 and 18 percent also adhered to regional rules as established in Groningen and Nijmegen, respectively. There appeared to be some evidence that ownership and use of plug-ins was related to GPs’ use of medical formularies. Owning Prescriptor correlated with using the NHG-guidelines (p = .020, FET) and the regional guidelines from Groningen (p = .029, FET). The use of Prescriptor was correlated with the use of NHG-guidelines only (p = .006, FET). Additionally, the number of formularies used correlated with Prescriptor ownership (p = .015, FET).
Relations including ownership or use of NHGDoc did not occur in the same number; use of this plug-in correlated with use of the NHG-guidelines (p = .009, FET), but none of the other relations. These results validated H4 in the above-mentioned cases. H2 and H3 were accepted for Prescriptor but not for NHGDoc, while H5 was rejected altogether.
Problem recognition
The problems commonly associated with polypharmacy were widely recognized. Ninety-five percent of respondents recognized a higher risk of adverse effects with polypharmacy patients. Patients of 83 percent of the surveyed GPs showed signs of decreased adherence to their drug prescriptions. Forty-nine and 40 percent of the respondents recognized increased risks of under- and overmedication, respectively. Overall, after correcting for double counting due to the possible inclusion of GPs sharing the same clientele, GPs each treated 159 polypharmacy patients on average.
The sixth and seventh hypotheses were tested by checking whether the use of any of the formularies was related to the problems encountered. Especially relations including the NHG-formulary showed significant results; underprescription (p = .002, FET) and decreased adherence (p = .044, FET) were more often reported by GPs using the NHG-guidelines. Overall, GPs using the NHG-formulary reported more problems than those who did not (p = .016, FET). None of the other formularies showed any relations, except for the Nijmegen-guidelines, which showed that use of those clinical rules correlated with the recognized occurrences of underprescription (p = .036, FET). This partly validated H6 for the cases involving the NHG- and the Nijmegen-guidelines. H7 was valid only for the NHG-guidelines.
With the testing of these hypotheses, the current situation of the use and impact of decision support systems in the Dutch primary care sector was investigated. The results are visually represented in Figure 3.
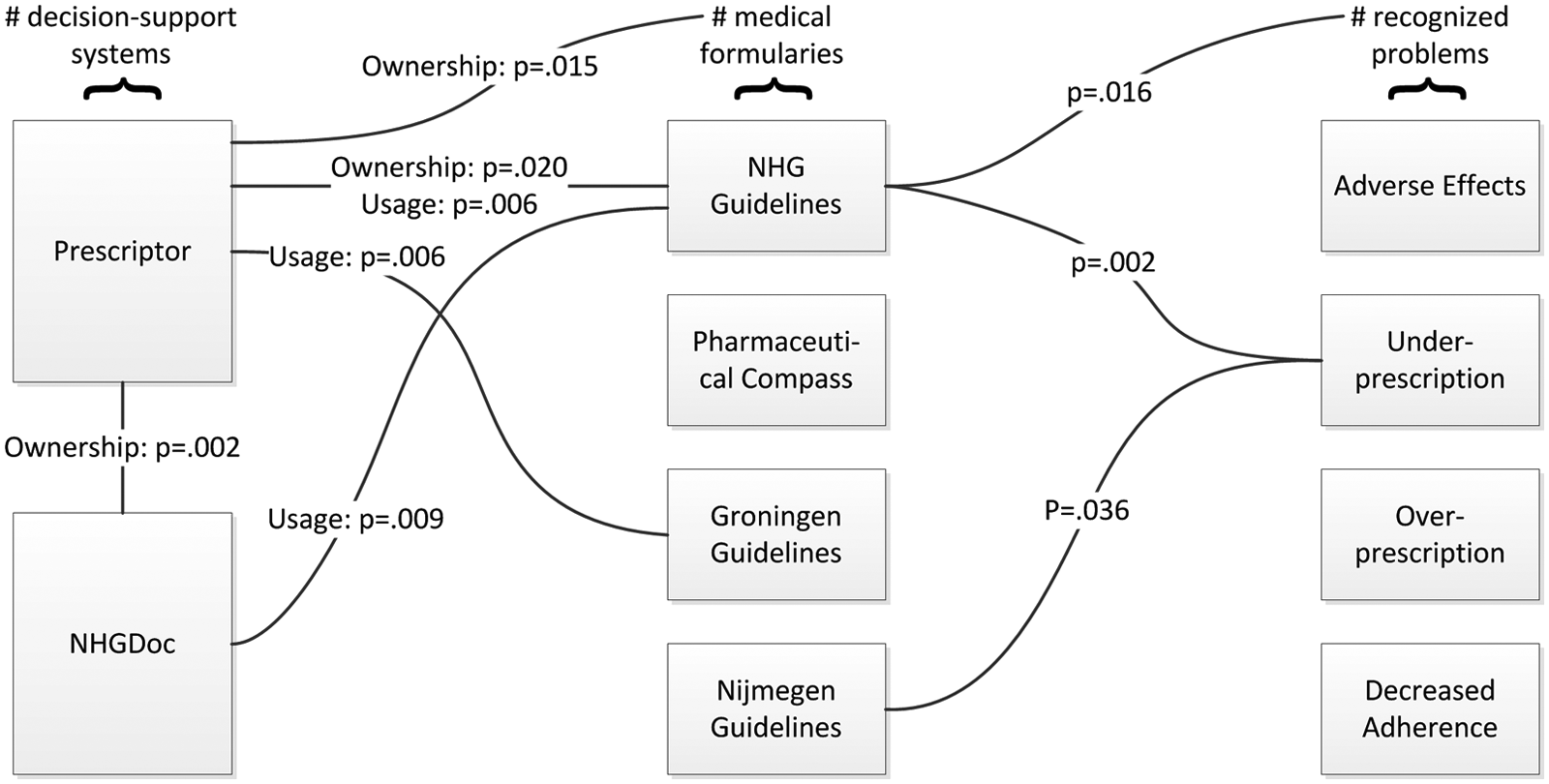
Model depicting the probability values of the statistically significant relationships between decision support systems, medical formularies, and recognized problems.
Perceived usefulness
When informed about the possible new system aiding them with treating polypharmacy, the majority (57%) of GPs responded positively; only 5 percent responded outward negatively. Subsequently, the constructs presented in the model on technology acceptance in Figure 1 were tested. The two questions on job relevance showed different results; the number of problems encountered with polypharmacy patients did not appear to have any relation with the POMP’s perceived usefulness (p = .759, FET); neither did any of the specific problems themselves appear to correlate with GPs’ attitudes (adverse effects: p = .186, FET; undertreatment: p = .676, FET; overtreatment: p = .394, FET; and adherence: p = 1.000, FET). The total number of patients using five or more different drugs that each GP reported did not significantly correlate either (p = .079, FET). The aspect of output quality, however, appeared to correlate strongly (p = .000, FET) with the POMP’s usefulness as perceived by the GPs. A similar result was found for the relation between time investment (p = .000, FET) and the system’s usefulness. The two questions used to measure the financial phenomenon, on payability and reimbursement, showed significant correlations with p = .000 (FET) and p = .015 (FET), respectively. This led to the acceptance of H11, H12, H13, and H14. H8, H9, and H10 were rejected.
Age
Finally, the hypotheses regarding the impact of respondents’ ages on the constructs were tested. As it appeared, age correlated significantly with the constructs of time (p = .016, FET) and payability (p = .022, FET). The aspects of output quality (p = .066, FET) and reimbursement (p = .098) were not related. Age appeared to significantly correlate neither with the number of encountered problems (p = .725, FET) nor with the number of patients (p = .963, FET); no evidence was found to assume any relations between age and the recognition of specific problems (adverse effects: p = .960, FET; undertreatment: p = .827, FET; overtreatment: p = .191, FET; and adherence: p = .203, FET). This validated H19 and H21 but led to the rejection of H15; H16; and H17, H18, and H20. All probabilities found with FET that are part of the model in Figure 1 are depicted in Figure 4.
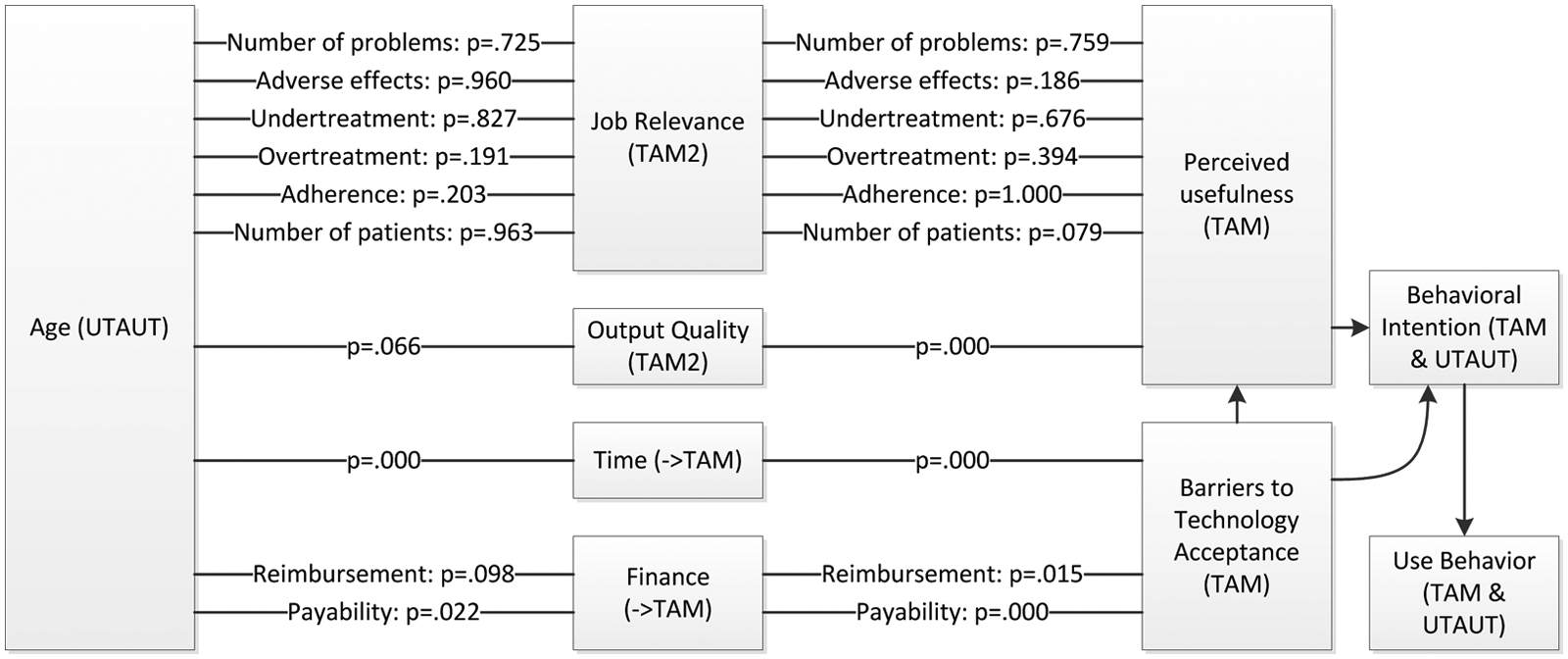
Model depicting the probability values of all tested relationships between the factors relating to use behavior, according to Figure 1.
Discussion
With this article, the authors aimed at exploring the motivations of GPs to adopt decision support systems. This study being part of a greater project involving polypharmacy complications, the data collection focused on GPs’ experiences with polypharmacy prescribing, treatment, and assistive software.
The questionnaire’s results showed that the Dutch market of GPs’ CPOE systems is very diverse, even though the two largest providers control half of the market. Assistive plug-ins for these products are roughly distributed among a fourth of the GPs; their functionality, however, is seriously underused. The majority of the owners of this assistive software indicate never or rarely ever using it, with just below 40 percent employing it regularly during consultations.
Simultaneously, the results indicate that—in several cases—use of decision support systems is related to the use of medical formularies. Furthermore, in the case of the NHG-guidelines, the adherence to these clinical rules is related to GPs’ recognition of polypharmacy problems.
As mentioned earlier, the data analysis only revealed correlations between hypotheses; causality could not be inferred from the statistical results. However, since the hypotheses were based on the influential relations between the variables in Figure 1, which in turn were based on consensus in literature, causality may be assumed when interpreting these results. Thus, in the discussion below, these aspects are interpreted in the light of this justifiable causality.
When exploring GPs’ attitudes toward using an assistive software program aiding them with polypharmacy treatment, subjects generally responded positively to the idea of such a decision support system. Some, however, uttered doubts as to its added value; several respondents questioned the proposed application’s form as a separate product, suggesting to “improve existing systems rather than introducing new methods.” The generally positive response to clinical decision support systems corresponds with the findings of a study among Irish physicians by Hor et al. 40
The theoretical framework in Figure 1 includes two constructs that are commonly included in TAMs; job relevance and output quality. Of these, the only one that appears to be strongly valued by GPs is that of output quality. The other construct, job relevance, seems to be of lesser importance; neither the number of patients suffering from polypharmacy a GP treats seems to positively influence his or her opinion toward the proposed system, nor does the (number of) recognized problems. This finding does not concur with GPs’ answers regarding the system’s usefulness, nor does it reflect views in literature that specifically mention job relevance as vital to GPs’ attitudes. 31 Reasons for this discrepancy may be found in the methodical approach to this aspect, which will be further elaborated upon in the section on limitations.
An aspect not included in any of the common TAMs by default, time, appears to have a very strong influence on GPs’ motivations. This finding concurs with several other studies investigating this aspect.28,32,33 Due to their high workload, GPs may be unwilling to adhere to new guidelines requiring time investment but welcome aids reducing consultation time per patient. 41
Another aspect explored in literature as possibly influential is that of financial stimuli. Just as time, it is supposedly a barrier against adoption of new technology. 32 The survey results show that payability and, to a lesser extent, reimbursement influence GPs’ attitudes toward the newly proposed system. One of the respondents, for example, indicated that he would be willing to consider purchasing the finished product “only if reimbursement is guaranteed in writing.” The importance of financial stimuli found in this study mirrors the findings of Boonstra et al. 28 who mentioned it as one of the four influential factors in their research.
Age, finally, has a moderate influence on the importance GPs attribute to time and financial stimuli. No effect on output quality or job relevance was discovered. As an aspect commonly investigated in technology adoption literature, its discovered influence corresponds with the scientific consensus, most notably with the work of Venkatesh et al., 34 who found that age was the only construct common in adoption models that appeared to be influential to GPs’ attitudes.
Conclusion
While GPs’ CPOE systems are widely in use, the use of decision support systems during patient consultations is lacking. When being proposed as a conceptual decision support system aimed at assisting polypharmacy treatment, however, GPs indicate expecting such a system to be valuable. Specifically, they indicate output quality, time investment, and financial stimuli as important determinants in their attitudes toward acceptance. Job relevance seems not to have as strong an influence as is commonly assumed in literature. 31
The original research question that the authors attempted to answer through this study was: how are GPs in the Dutch primary care sector, based on their experiences with decision support systems and medical formularies, likely to respond to the introduction of a platform assisting them with treating polypharmacy? Following the result that the vast majority of respondents judged the perceived usefulness of the proposed system as high, GPs working in the Dutch primary care sector are likely to adopt such a system, under the conditions that it improves prescription quality and does not require extensive investments of time or money.
Limitations
Even though utmost care was taken in the conduct of this study in order to ensure its reliability and validity, some considerations should be taken into account when applying its findings. The survey employed in the study contained some questions that did not directly represent theoretical constructs, most notably the one on job relevance. This choice was made because of the possible ambiguity respondents may perceive between that concept and usefulness, but ultimately, it hinders generalizability. The large differences between the rough estimates given by the respondents may explain the lack of significance in the relations measured. Considering that this study’s outcomes on job relevance do not concur with scientific consensus, the authors suggest that these specific findings should be generalized outside of this study with caution.
Additionally, given that respondents voluntarily participated in the study, they may be more interested in, and thus hold more positive attitudes toward clinical decision support systems than nonparticipants.
Further research
This study has investigated factors of influence on GPs’ attitudes toward adopting decision support systems. Factors commonly not included in TAMs, such as time or financial investments, have been proven to be influential in shaping GPs’ attitudes toward such systems.
Further research should focus on investigating the wider generalizability of these claims. Additionally, the salient beliefs held by health-care professionals should be explored, as proposed by Holden and Karsh, 42 in order to find out whether indeed some fundamental concepts of technology adoption, most notably perceived ease-of-use, do not influence this group’s attitudes, while other aspects generally not included in such models do.
Footnotes
Appendix 1
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.